
Abstract
Background
Depression and anxiety have been found prevalent during all phases of the COVID-19 pandemic. In late December 2022, almost all COVID-19 control measures were lifted in China, leading to a surge in COVID-19 infections. The public’s perceived risk and fear of COVID-19 would be increased. This study aims to examine the prevalence of depression and anxiety in the Chinese general population and explores the mediating role of fear of COVID-19 between COVID-19 perceived risk and depression/anxiety and the moderating role of resilience between fear of COVID-19 and depression/anxiety.
Methods
A cross-sectional online survey was conducted in Wenzhou, China, immediately following almost all COVID-19 control measures lifted. The 9-item Patient Health Questionnaire (PHQ-9), Generalized Anxiety Disorder-7 (GAD-7), the COVID-19 Risk Perception Scale, the Fear of COVID-19 Scale, and the Connor-Davidson Resilience Scale (CD-RISC) were used to evaluate depression, anxiety, COVID-19 perceived risk, fear of COVID-19, and resilience, respectively. Structural Equation Modeling (SEM) with Maximum Likelihood (ML) estimator and adjusted for significant background factors was performed to test the moderated mediation. Data obtained from 935 participants were analyzed.
Results
The prevalence of moderate to severe depression and anxiety was 23.7% and 9.5%, respectively. The present study revealed positive associations among COVID-19 perceived risk, fear of COVID-19 and depression/anxiety, and negative associations between resilience and fear of COVID-19/depression/anxiety. Fear of COVID-19 partially mediated the association between COVID-19 perceived risk and depression/anxiety. Furthermore, resilience significantly moderated the association between fear of COVID-19 and depression/anxiety. Two moderated mediation models were constructed.
Conclusion
Depression and anxiety were prevalent among Chinese adults during the final phase of the pandemic in China. The significant mediation role of fear of COVID-19 implies that reducing fear of COVID-19 may effectively alleviate depression and anxiety symptoms. Moreover, enhancing public resilience during an epidemic crisis is crucial for promoting mental health.
Similar content being viewed by others


Introduction
Depression and anxiety are prevalent mental distress that individuals commonly experience during the pandemic and the levels of distress may be dramatically elevated [1,2,3,4]. At all phase of COVID-19, a surge in mental health problems (e.g., depression and anxiety) were observed among various population such as infected people, healthcare workers, and the general population [5,6,7,8,9,10,11,12,13,14]. For instance, a meta-analysis including 66 studies indicated that during the COVID-19 pandemic, the pooled prevalence of depression among infected individuals, healthcare workers, and the general population was 41.7%, 31.0%, and 31.5%, respectively; the pooled prevalence of anxiety among these population was 42.3%, 29.8%, and 29.0%, respectively [8]. Another meta-analysis involving 31 studies demonstrated that the pooled prevalence of depression and anxiety among COVID-19 infected people was 45% and 47%, respectively [15]. Examples of factors associated with depression and anxiety among general population included worry about infection [16], uncertainties [17, 18], and negative perceptions toward the pandemic [19]. There are reasons to believe that the prevalence of depression and anxiety would be high in the end phase of COVID-19 pandemic in China.
Perceived risk and depression/anxiety
The perception of potential threats and risks may affect individual’s emotional response such as depression and anxiety. Perceived risk, i.e., individual’s perception and awareness of objective risks existing in the outside world [20], emphasizes the influence of the individual’s experience gained from intuitive judgment and subjective perception on the individual’s cognition [20, 21]. Individual’s subjective interpretations of risk could affect their behavior and emotional responses when facing new, unobservable, and unpredictable hazard such as COVID-19 [22]. Li & Lyu reported that higher perceived risk was associated with poorer mental health outcomes during the acute phase of COVID-19 pandemic [21]. Perceived COVID-19 infection risk was positively associated with depressive symptoms in young adults in quarantine [23] and in healthcare workers [24]. Additionally, Alsolais et al. reported that higher level of self-reported perceived risk was associated with greater depressive symptoms and anxiety in their longitudinal study [25]. Similar results have been found in other infectious diseases, such as SARS and Ebola virus [26, 27].
Potential mediating role of fear of COVID-19
It is well-established that cognition and emotion regarding a specific disease are associated with mental distress [28]. Fear, characterized as an unpleasant emotion [29], could be harmful to mental health [30]. Previous study revealed that fears of COVID-19 was positively associated with perceived risk during the pandemic [31], and also with depression and anxiety [32]. A recent study suggested that fear of COVID-19 could potentially mediate the relationship between perceived risk and mental distress among healthcare workers [33]. The associations can be explained by emotional illness representation of a disease, i.e., how people feel about the disease [34, 35]. Thus, it is plausible that COVID-19 perceived risk would increase fear of COVID-19, which would in turn increase depression and anxiety, i.e., fear of COVID-19 may be a mediator between COVID-19 perceived risk and depression/anxiety. The potential associations imply that reducing fear of COVID-19 may lessen the high prevalence or reduce severity of mental distress among the public.
Potential moderating role of resilience
Resilience is a dynamic process by which individuals adapt well to stressful events [36]. In this process, individuals make full use of their personal and psychological resources to effectively cope with negative life events such as stress, frustration and trauma as well as to survive adversity [36, 37]. The importance of resilience stems from its ability to help individuals actively adapt to severe adversity, maintain mental health, recover from disasters [38] and protect individuals from depression [39] and anxiety [40]. Thus, individuals who experienced depressive symptoms and anxiety could benefit from a high level of resilience [40, 41]. The importance of resilience is also highlighted at various phases of the pandemic [42, 43]. For example, that the higher COVID-19-related resilience, the less severe depressive symptoms was observed in a group of healthcare workers [44]. Therefore, it is plausible to hypothesize that resilience might reduce the negative consequences of fear of COVID-19 on depression/anxiety, i.e., resilience may weaken the associations between fear of COVID-19 and depression/anxiety.
Objective of the present study
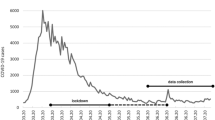
The present study was conducted among the general population in Wenzhou, China from January 11, 2023 to January 29, 2023, right after the lifting of almost all control measures. COVID-19 prevention and control measures in China changed so suddenly from extremely high to none in a very short time so that most people were unprepared. Given that background, this study investigated (1) the prevalence of depression and anxiety; (2) the associations among COVID-19 perceived risk, fear of COVID-19, resilience, depression, and anxiety; (3) the mediating role of fear of COVID-19 between COVID-19 perceived risk and depression/anxiety; (4) the moderating role of resilience between fear of COVID-19 and depression/anxiety (See Supplementary Fig. 1).
Methods
Participants and data collection
Data were collected through an online survey among a convenient sample of 947 participants aged 18–60 in Wenzhou, China from January 11 to 29, 2023, via Wenjuanxing which is a widely used professional online survey platform in China. Participants were informed that participation in the survey was voluntary and anonymous and they were not required to provide any personal information. All information collected would be used for research only and kept strictly confidential. Once informed of the above, participants could choose to participate in or withdraw from the survey. The time required to complete the survey was approximately 10 min.
To ensure timeliness of the study, convenience sampling was used as people’ s mental distress, fear, and perceived risk may change quickly as the pandemic moved through its stages. Data from 947 participants were collected, of which 12 were excluded because they either took less than 4 min (mean completion time = 11.57 min, SD = 7.50 min) to complete the survey or showed response set in the answer. Finally, data obtained from 935 was analyzed.
Measurements
Background factors
Background information was collected including sex, age, educational level, religious belief status, family economic status, whether having medical background, marriage status, and physical status.
Depression
The 9-item Patient Health Questionnaire (PHQ-9) was used to evaluate depression [45]. It was rated on four-point Likert scales (0 = not at all to 3 = nearly every day), with total scores ranging from 0 to 27. Summative scores of 0–4, 5–9, 10–14,15–19, 20–27 indicate no depression, mild depression, moderate depression, moderately severe depression, and severe depression, respectively. Its Chinese version has been validated and showed excellent psychometric properties in previous studies [5, 46]. The Cronbach’s alpha of the scale was 0.92 in this study.
Anxiety
Generalized Anxiety Disorder-7 (GAD-7) was used to evaluate anxiety [47]. It is a seven-item scale rated on four-point Likert scales (0 = not at all to 3 = near every day), with total scores ranging from 0 to 21. The summative scores of 0–4, 5–9, 10–14,15–21 reflect no anxiety, mild anxiety, moderate anxiety, and severe anxiety. Its Chinese version has been validated and showed excellent psychometric properties in previous studies [7, 46]. The Cronbach’s alpha of the scale was 0.95 in this study.
COVID-19 perceived risk
The COVID-19 Risk Perception Scale was developed to assess COVID-19 perceived risk in Chinese population [48]. It consists of 9 items including three dimensions (perceived susceptibility, severity, and controllability of COVID-19) rated on a 5-point Likert scale (1 = negligible to 5 = very large), with a total score ranging from 9 to 45. The Cronbach’s alpha of the scale was 0.90 in this study.
Fear of COVID-19
The fear of COVID-19 was evaluated by using the fear of COVID-19 Scale, which is reliable and validated in assessing the fear of COVID-19 among the general population [49]. It consists of 7 items rated on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree), with a summative score ranging from 7 to 35. Its effectiveness and superiority for assessing fear of COVID-19 were indicated in Chinese population [50,51,52,53,54]. The Cronbach’s alpha of the scale was 0.93 in this study.
Resilience
Resilience was assessed using a short version of the Connor-Davidson Resilience Scale (CD-RISC). It reflects the ability to tolerate experiences, such as change, personal problems, illness, pressure, failure, and painful feeling [55]. Its Chinese version was demonstrated good reliability and validity [56, 57]. It is a 10-item scale rated on a 5-point Likert scale (0 = not true at all to 4 = true nearly all of the time), with total scores ranging from 0 to 40. The Cronbach’s alpha of the scale was 0.97 in this study.
Statistical analysis
Descriptive analyses were conducted for background factors and the prevalence of depression and anxiety. Simple linear regression analyses were performed to test the associations between background factors and depression (PHQ-9 score)/anxiety (GAD-7 score). Pearson correlation coefficients were derived to test associations between variables, i.e., COVID-19 perceived risk, fear of COVID-19, resilience, PHQ-9 for depression, and GAD-7 for anxiety. Structural Equation Modeling (SEM) with Maximum Likelihood (ML) estimator and adjusted for significant background factors was performed to test the moderated mediation. COVID-19 perceived risk was constructed as a latent variable, while other variables were observed variables. Satisfactory model fit indices included Comparative Fit Index (CFI ≥ 0.90), Tucker-Lewis Index (TLI ≥ 0.90), Root Mean Square Error of Approximation (RMSEA ≤ 0.08), and Standardized Root Mean Square Residual (SRMR ≤ 0.08) [58]. Moderated mediation was tested using Mplus 7.3 and other analyses were done with SPSS 23.0. Statistical significance was defined as two-tailed p-value < 0.05.
Results
Descriptive statistics
As shown in Table 1, the majority of the sample were female (79.3%), aged over 40 (52.1%), currently married (90.3%), had a college or above degree (42.2%), had no religious belief (66.5%), had very poor/poor family economic status (58.4%), had no medical background (88.2%), or had healthy physical status (92.1%). Of all participants, 23.7% exhibited moderate to severe depression (PHQ-9 ≥ 10) and 9.5% with moderate to severe anxiety (GAD-7 ≥ 10).
The mean [standard deviation (SD)] values were 6.77 (SD = 5.66) for PHQ-9, 4.00 (SD = 4.54) for GAD-7, 26.73 (SD = 6.40) for COVID-19 perceived risk, 19.15 (SD = 5.77) for fear of COVID-19, and 24.75 (SD = 9.36) for resilience (Table 2).
Background factors of depression and anxiety
Participants aged over 40, or were currently married, or were healthy were less likely to have depression or anxiety. Those who had medical background were more likely to have depression but not anxiety. Depression and anxiety was higher among those with a college or above degree. No significant differences were found across sex, religious belief status, and family economic status groups (Table 1).
Pearson correlation analysis
As shown in Table 2, COVID-19 perceived risk, fear of COVID-19, depression, and anxiety were significantly and positively associated with each other (r between 0.32 and 0.82). Depression (r = -0.10), anxiety (r = -0.09) and fear of COVID-19 (r = -0.14) were significantly and negatively associated with resilience. The correlation between COVID-19 perceived risk and resilience was statistically non-significant.
Results of moderated mediation
Depression and anxiety were used as two outcome variables. Thus, two models were generated (Model 1: depression and Model 2: anxiety), which were adjusted by significant background factors (Table 3, Fig. 1and Fig. 2). Significant background factors associated with depression were age, educational level, medical background, marriage status, and physical status, while significant background factors associated with anxiety were age, educational level, marriage status, and physical status (Table 1). Both models showed satisfactory fit indices (Model 1: χ2/df = 2.33, CFI = 0.97, TLI = 0.96, SRMR = 0.04, RMSEA = 0.04; Model 2: χ2/df = 2.40, CFI = 0.96, TLI = 0.95, SRMR = 0.04, RMSEA = 0.05).

Structual equation modeling for Model 1. Standardized coefficients were reported. **p < 0.01; ***p < 0.001. The model was adjusted for age, educational level, medical background, marriage status, and physical status

Structual equation modeling for Model 2. Standardized coefficients were reported. **p < 0.01; ***p < 0.001. The model was adjusted for age, educational level, marriage status, and physical status
In Model 1, fear of COVID-19 significantly mediated the relationship between COVID-19 perceived risk and depression. COVID-19 perceived risk was positively associated with fear of COVID-19 (β = 0.48, SE = 0.03, p < 0.001), which was in turn positively associated with depression (β = 0.26, SE = 0.03, p < 0.001). As the direct effect of COVID-19 perceived risk on depression was statistically significant (β = 0.23, SE = 0.03, p < 0.001), a partial mediation effect was observed with a mediation effect size of 35.17% (p < 0.001). In Model 2, fear of COVID-19 significantly mediated the association between COVID-19 perceived risk and anxiety, i.e., COVID-19 perceived risk was positively associated with fear of COVID-19 (β = 0.48, SE = 0.03, p < 0.001) which in turn was positively associated with anxiety (β = 0.38, SE = 0.03, p < 0.001). The direct effect of COVID-19 perceived risk on anxiety was also statistically significant (β = 0.13, SE = 0.03, p < 0.001) and the partial mediation effect with a mediation effect size was 14.10% (p < 0.001).
Moderating effect of resilience on the relationship between fear of COVID-19 and depression/anxiety was supported in that the relationships become weaker when resilience was high. Variables were centralized prior to creating their product terms and standardized score of depression or anxiety was applied. The results showed that the interaction term of resilience and fear of COVID-19 was negatively related to depression (β = -0.09, SE = 0.03, p < 0.01; Model 1). Simple slopes analysis was conducted to further interpret the results. The interaction plot in Fig. 3 showed that the positive association between fear of COVID-19 and depression was stronger in participants with low resilience (1 SD below the mean, simple slope: βLow = 0.35, SE = 0.04, p < 0.001) than that in participants with high resilience (1 SD above the mean, simple slope βHigh = 0.17, SE = 0.05, p < 0.001). It is also indicated that interaction term of resilience and fear of COVID-19 was negatively related to anxiety (β = -0.07, SE = 0.02, p < 0.01; Model 2). The interaction plot in Fig. 4 showed that the association between fear of COVID-19 and anxiety was stronger in participants with low resilience (1 SD below the mean, simple slope: βLow = 0.45, SE = 0.03, p < 0.001) than that in participants with high resilience (1 SD above the mean, simple slope βHigh = 0.31, SE = 0.04, p < 0.001).

Interactive effect of resilience and fear of COVID-19 on depression (standardized)

Interactive effect of resilience and fear of COVID-19 on anxiety (standardized)
Discussion
This timely study was conducted during the end phase of the COVID-19 pandemic in China from January 11 to 29, 2023. At the end of 2022, almost all measures were lifted in mainland China. Before lifting all the measures, China’s infection rate was less than 1% [59], indicating very low exposure of the public to COVID-19 infection. The abrupt relaxation of prevention and control policies exposed a majority of Chinese population to the infection [60]. Rapid policy shifts and exposure to infections might challenge public trust in the health care system and authorities, which may in turn affect their mental health and increase depression and anxiety [61]. Furthermore, the public was unprepared for the sudden changes and China also faced a shortage of medical resources. In such situations, unpreparedness and increasing demand for medical supplies made obtaining treatment difficult, which subsequently contributed to the rise of mental distress [60]. It reminded us that public trust and preparedness are important to maintain mental health [61]. Trust fostered a sense of security, which helped to reduce mental distress. Preparedness empowered individuals to cope with challenges and mitigated the psychological toll of unexpected circumstances.
Our study found high prevalence of moderate to severe depression (PHQ-9 ≥ 10 = 23.7%) and prevalence of moderate to severe anxiety (GAD-7 ≥ 10 = 9.5%) in Chinese adult general population. This finding was consistent with previous research conducted during the acute phase of the COVID-19 pandemic in Wuhan, with 20.3% depression rate using the same instruments and cut-off value [46]. However, the prevalence of moderate to severe anxiety in our study was much lower than the reported anxiety rate of 18.9% in Wuhan [46]. Variations may be explained by numerous factors such as the differences in the features of the different pandemic phases and participants’ characteristics [62]. Despite variations, our results indicated that people at the end phase of COVID-19 still had high levels of mental distress.
In line with published literature, those aged over 40 or unmarried, divorced or separated, or with chronic disease, pregnancy, serious illness were more likely to have depression and anxiety [63, 64]. Interestingly, sex and religious belief status were not significant factors. Consistent with finding of a meta-analysis [15], no significant sex differences was found in the prevalence of depression and anxiety. Possible reason was that during such special period, males and females were equally mentally-distressed. Religious belief was found as a protective factor against mental health problems in COVID-19 pandemic in previous study [65, 66], but not in the current study. Some of the background factors seemed non-significant in affecting depression and anxiety in the Chinese general population.
The present study revealed significantly positive associations among COVID-19 perceived risk, fear of COVID-19, depression and anxiety. This suggested that public’s risk perception towards COVID-19 and the fear of COVID-19 deserved more attention on account of their roles in mitigating depression and anxiety. Similar positive associations were found among Saudi nursing students during the COVID-19 pandemic [25]. The results showed that COVID-19 perceived risk had positive direct effect on depression and anxiety, which was consistent with previous findings on epidemic risk perception and mental health [21, 24]. The emergence of epidemic created lots of uncertainty, posed threats to individuals and sharply increased individuals’ perceived risks, which resulted in anxiety and depression [67]. People also experienced loss of control and powerlessness during great pandemic and felt that they could only wait passively through the development of the epidemic, which brought to them higher levels of depression and anxiety [21].
One of the key findings was that fear of COVID-19 partially mediated the associations between COVID-19 perceived risk and depression/anxiety. It supported the hypotheses that fear of COVID-19 was both associated with COVID-19 perceived risk and depression/anxiety, which was partially in line with the Common Sense Model (CSM), i.e. an illness determines emotional responses that further affects mental health [34, 35]. Also, Beck’s cognitive theory proposed that cognitive content (including individuals’ belief systems, expectations, assumptions, and evaluations) is activated by events and driven by subjective meaning that interacts with their affective systems [68]. Therefore, exaggerated interpretations of threats, including fear of COVID-19 [69], may lead to inappropriate or excessive anxiety and depression [70]. Yıldırım et al.’s finding supported the mediation role of coronavirus fear between coronavirus risk and parental coronavirus anxiety among healthcare workers [71]. Notably, in the current study, the mediation effect size was 35.17% for depression and 14.10% for anxiety. It suggested that the decrease in COVID-19 fear could reduce depression and anxiety. As individual’s COVID-19 perceived risk and fear of COVID-19 could change over time, future longitudinal studies would provide valuable insights to the dynamics among perceived risk and fear and mental distress and also discover other potential mediators.
Another key finding was that resilience weakened the impact of fear of COVID-19 on depression/anxiety. Consistent with previous findings, high resilience was a protective factor against depression and anxiety [72]. Individuals with higher resilience may be more positive and more likely to use active coping strategies which help reduce the impact of fear on how much depression/anxiety they develop [73]. More resilient people may also possess more effective emotion regulation skills to weaken the effect of fear on depression and anxiety, despite the existence of subjective fear of COVID-19 [74]. Zhou et al. showed that resilience moderated the association between fear and depression among middle school students after earthquake [73]. Besides resilience, which has been widely studied as a positive psychological resource, research could also examine other potential moderators such as self-compassion, which is a caring, nonjudgmental lens in the face of personal suffering [75] and is another resistance factor for mental health problems [76].
In sum, the present study supported the hypotheses and had great implications. Firstly, it facilitated a better understanding of how COVID-19 perceived risk resulted in depression and anxiety. It thus provided theoretical guidance for future epidemic intervention [21]. Secondly, an important reminder is that fear of COVID-19 has emotional components. Partially according to CSM, emotional components would affect mental health [34, 35]. To reduce depression and anxiety among the public, interventions are needed for such components. Fear of COVID-19 was an important mediation mechanism by which the perceived risk of unexpected epidemic affected individuals’ mental health. Coping with the fear of COVID-19 was an important means to reduce mental distress during such crisis. It is well-known that fear stems from uncertainties and the unknown. Thus, intervention and measures need to focus on helping individuals gain more knowledge about COVID-19 and increase availability of drug and treatment. Thirdly, the mediation and moderation relationship found in the current study allow us to explore various ways to attenuate mental distress in pandemics, rather than taking a single approach. For example, as resilience is a resistance factor to mental health problems, especially in pandemics, efforts could be directed to increase public’s resilience, through actions via well-suited online resilience-based interventions or adding psychological counseling and mental health services [77, 78].
Despite its strengths, this study has some limitations. Firstly, social desirability bias could exist. For instance, fear of COVID-19, depression and anxiety may be underreported due to potential stigma and discrimination [79]. Secondly, this study failed to calculate the participation rate. Thirdly, given the feature of cross-sectional design, no causal inferences can be made. Future longitudinal studies are needed to verify the such associations as COVID-19 perceived risk and fear of COVID-19 would change over time. Fourthly, the distribution of participants characteristics was not representative of the Chinese population as convenience sampling was used. For instance, the majority of our participants was female (79.3%). Cautions are warranted to generalize the results to the entire Chinese population and to other countries. However, through adjusting the models with demographic variables the current study aimed to maximize its generalizability.
Conclusion
The present study detected high prevalence of moderated to severe depression (23.7%) and relatively low prevalence of moderate to severe anxiety (9.5%) among Chinese adult population after lifting all measures. The associations between COVID-19 perceived risk and depression/anxiety were partially mediated via fear of COVID-19. Resilience moderated the relationships between fear of COVID-19 and depression/anxiety. Due to vaccination uptake and less virulent variants, it seemed that the COVID virus became weaker and more controllable, caused fewer and less severe symptoms, and induced fewer emotional responses over the last three years till the end of 2022. Yet with sudden lifting all measures in January, 2023, panic and mental distress surged. Depression and anxiety caused by fear of COVID-19 needs to be highlighted. It is important to reduce people’s perceived risk towards COVID-19 to decrease the fear of COVID-19, which in turn reduces depression and anxiety. Interventions and efforts are necessary to enhance resilience of the public when epidemic crisis emerged.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding authors on reasonable request.
Abbreviations
- COVID-19:
-
Corona Virus Disease 2019
- SARS:
-
Severe acute respiratory syndrome
- CSM:
-
Common Sense Model
- PHQ-9:
-
The 9-item Patient Health Questionnaire
- GAD-7:
-
Generalized Anxiety Disorder-7
- SEM:
-
Structural Equation Modeling
- CFI:
-
Comparative Fit Index
- TLI:
-
Tucker-Lewis Index
- RMSEA:
-
Root Mean Square Error of Approximation
- SRMR:
-
Standardized Root Mean Square Residual
- SPSS:
-
Statistical package for social sciences
- SD:
-
Standard deviation
- SE:
-
Standard error
References
Banerjee D. The COVID-19 outbreak: crucial role the psychiatrists can play. Asian J Psychiatry. 2020;50:102014.
Nayan MIH, Uddin MSG, Hossain MI, Alam MM, Zinnia MA, Haq I, et al. Comparison of the performance of machine learning-based algorithms for predicting depression and anxiety among University students in Bangladesh: a result of the first wave of the COVID-19 pandemic. Asian J Social Health Behav. 2022;5:75.
Tsai C-S, Wang L-J, Hsiao RC, Yen C-F, Lin C-Y. Psychological distress and related factors among caregivers of children with attention-deficit/hyperactivity disorder during the COVID-19 pandemic. Eur Child Adoles Psy. 2023. https://doi.org/10.1007/s00787-023-02220-w.
Vicerra PMM. Mental stress and well-being among low-income older adults during COVID-19 pandemic. Asian J Social Health Behav. 2022;5:101.
Guo Q, Zheng Y, Shi J, Wang J, Li G, Li C, et al. Immediate psychological distress in quarantined patients with COVID-19 and its association with peripheral inflammation: a mixed-method study. Brain Behav Immun. 2020;88:17–27.
Krishnamoorthy Y, Nagarajan R, Saya GK, Menon V. Prevalence of psychological morbidities among general population, healthcare workers and COVID-19 patients amidst the COVID-19 pandemic: a systematic review and meta-analysis. Psychiatry Res. 2020;293:113382.
Li J, Yang Z, Qiu H, Wang Y, Jian L, Ji J, et al. Anxiety and depression among general population in China at the peak of the COVID-19 epidemic. World Psychiatry. 2020;19:249–50.
Wu T, Jia X, Shi H, Niu J, Yin X, Xie J, et al. Prevalence of mental health problems during the COVID-19 pandemic: a systematic review and meta-analysis. J Affect Disord. 2021;281:91–8.
Lin Y-H, Chen J-S, Huang P-C, Lu M-Y, Strong C, Lin C-Y, et al. Factors associated with insomnia and suicidal thoughts among outpatients, healthcare workers, and the general population in Taiwan during COVID-19 pandemic: a cross-sectional study. BMC Public Health. 2022;22:2135.
Liu C, Chen Y-J, Chen J-S, Fan C-W, Hsieh M-T, Lin C-Y, et al. Burdens on caregivers of patients with stroke during a pandemic: relationships with support satisfaction, psychological distress, and fear of COVID-19. Bmc Geriatr. 2022;22:958.
Kukreti S, Strong C, Chen J-S, Chen Y-J, Griffiths MD, Hsieh M-T, et al. The association of care burden with motivation of vaccine acceptance among caregivers of stroke patients during the COVID-19 pandemic: mediating roles of problematic social media use, worry, and fear. Bmc Psychol. 2023;11:157.
Al-Mamun F, Hussain N, Sakib N, Hosen I, Rayhan I, Abdullah AH, et al. Sleep duration during the COVID-19 pandemic in Bangladesh: a GIS-based large sample survey study. Sci Rep. 2023;13:3368.
Sandya PD, Shetty KV, Jaise J, Manikappa SK, Pai NB. Stress and burden among caregivers of persons with bipolar affective disorder during the COVID-19 pandemic in India. Asian J Social Health Behav. 2022;5:51.
Huang P-C, Hung C-H, Chen G-W, Cashin C, Griffiths MD, Yang W-C, et al. COVID-19-Related Self-Stigma, post-traumatic stress disorder, Insomnia, and Smartphone Addiction among Frontline Government Workers with COVID-19 pandemic control duties. Psychol Res Behav Ma. 2022;15:3069–80.
Deng J, Zhou F, Hou W, Silver Z, Wong CY, Chang O, et al. The prevalence of depression, anxiety, and sleep disturbances in COVID-19 patients: a meta-analysis. Ann N Y Acad Sci. 2021;1486:90–111.
Asmundson GJG, Taylor S. Coronaphobia: fear and the 2019-nCoV outbreak. J Anxiety Disord. 2020;70:102196.
Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. The Lancet. 2020;395:912–20.
Carvalho PM, de Moreira M, de Oliveira MM, Landim MNA, Neto JMM. The psychiatric impact of the novel coronavirus outbreak. Psychiatry Res. 2020;286:112902.
Hazumi M, Okazaki E, Usuda K, Kataoka M, Nishi D. Relationship between cognition and emotions caused by the COVID-19 infection, and depression and anxiety. Preprint. In Review; 2022.
Cho J, Lee J. An integrated model of risk and risk-reducing strategies. J Bus Res. 2006;59:112–20.
Li X, Lyu H. Epidemic risk perception, perceived stress, and Mental Health during COVID-19 pandemic: a Moderated Mediating Model. Front Psychol. 2021;11.
Yıldırım M, Güler A. Factor analysis of the COVID-19 perceived risk scale: a preliminary study. Death Stud. 2022;46:1065–72.
Hou J, Yu Q, Lan X. COVID-19 infection risk and depressive symptoms among young adults during Quarantine: the moderating role of grit and social support. Front Psychol. 2021;11.
Lam SC, Arora T, Grey I, Suen LKP, Huang EY, Li D et al. Perceived risk and Protection from infection and depressive symptoms among Healthcare workers in Mainland China and Hong Kong during COVID-19. Front Psychiatry. 2020;11.
Alsolais A, Alquwez N, Alotaibi KA, Alqarni AS, Almalki M, Alsolami F, et al. Risk perceptions, fear, depression, anxiety, stress and coping among Saudi nursing students during the COVID-19 pandemic. J Mental Health. 2021;30:194–201.
Cheng SKW, Chong GHC, Chang SSY, Wong CW, Wong CSY, Wong MTP, et al. Adjustment to severe acute respiratory syndrome (SARS): roles of appraisal and post-traumatic growth. Psychol Health. 2006;21:301–17.
Yang JZ, Chu H. Who is afraid of the Ebola outbreak? The influence of discrete emotions on risk perception. J Risk Res. 2018;21:834–53.
Min J-A, Yu JJ, Lee C-U, Chae J-H. Cognitive emotion regulation strategies contributing to resilience in patients with depression and/or anxiety disorders. Compr Psychiatr. 2013;54:1190–7.
Mobbs D, Adolphs R, Fanselow MS, Barrett LF, LeDoux JE, Ressler K, et al. Viewpoints: approaches to defining and investigating fear. Nat Neurosci. 2019;22:1205–16.
Mertens G, Gerritsen L, Duijndam S, Salemink E, Engelhard IM. Fear of the coronavirus (COVID-19): predictors in an online study conducted in March 2020. J Anxiety Disord. 2020;74:102258.
Serpas DG, Ignacio DA. COVID-19 fear mediates the relationship between perceived risk and preventive behaviors: the moderating role of perceived effectiveness. Psychol Health. 2022;37:1457–70.
Montano RL, Acebes K. COVID stress predicts Depression, anxiety and stress symptoms of Filipino respondents. 2020;9:78–103.
Yıldırım M, Arslan G, Özaslan A. Perceived risk and Mental Health problems among Healthcare professionals during COVID-19 pandemic: exploring the Mediating effects of Resilience and Coronavirus Fear. Int J Ment Health Addiction. 2022;20:1035–45.
Leventhal H, Leventhal EA, Contrada RJ. Self-regulation, health, and behavior: a perceptual-cognitive approach. Psychol Health. 1998;13:717–33.
Leventhal H, Phillips LA, Burns E. The common-sense model of self-regulation (CSM): a dynamic framework for understanding illness self-management. J Behav Med. 2016;39:935–46.
Connor KM, Davidson JRT. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depress Anxiety. 2003;18:76–82.
Fayyad J, Cordahi-Tabet C, Yeretzian J, Salamoun M, Najm C, Karam EG. Resilience-promoting factors in war-exposed adolescents: an epidemiologic study. Eur Child Adolesc Psychiatry. 2017;26:191–200.
Southwick SM, Charney DS. The Science of Resilience: implications for the Prevention and Treatment of Depression. Science. 2012;338:79–82.
Smith PR. Resilience: resistance factor for depressive symptom. J Psychiatr Ment Health Nurs. 2009;16:829–37.
Ran L, Wang W, Ai M, Kong Y, Chen J, Kuang L. Psychological resilience, depression, anxiety, and somatization symptoms in response to COVID-19: a study of the general population in China at the peak of its epidemic. Soc Sci Med. 2020;262:113261.
Cheng C, Dong D, He J, Zhong X, Yao S. Psychometric properties of the 10-item Connor–Davidson Resilience Scale (CD-RISC-10) in Chinese undergraduates and depressive patients. J Affect Disord. 2020;261:211–20.
Haldane V, De Foo C, Abdalla SM, Jung A-S, Tan M, Wu S, et al. Health systems resilience in managing the COVID-19 pandemic: lessons from 28 countries. Nat Med. 2021;27:964–80.
Prime H, Wade M, Browne DT. Risk and resilience in family well-being during the COVID-19 pandemic. Am Psychol. 2020;75:631–43.
Hwang S, Lee J. The influence of COVID-19-related resilience on depression, job stress, sleep quality, and burnout among intensive care unit nurses. Front Psychol. 2023;14.
Kroenke K, Spitzer RL, Williams JBW. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606–13.
Wang M, Zhao Q, Hu C, Wang Y, Cao J, Huang S, et al. Prevalence of psychological disorders in the COVID-19 epidemic in China: a real world cross-sectional study. J Affect Disord. 2021;281:312–20.
Löwe B, Decker O, Müller S, Brähler E, Schellberg D, Herzog W, et al. Validation and standardization of the generalized anxiety disorder screener (GAD-7) in the General Population. Med Care. 2008;46:266–74.
Cui X, Hao Y, Tang S. Reliability and validity of a self-designed COVID-19 risk perception scale– a large online empirical study. Chin J Public Health. 2021;37:1086–9.
Ahorsu DK, Lin C-Y, Imani V, Saffari M, Griffiths MD, Pakpour AH. The fear of COVID-19 scale: development and initial validation. Int J Ment Health Addiction. 2022;20:1537–45.
Chi X, Chen S, Chen Y, Chen D, Yu Q, Guo T, et al. Psychometric evaluation of the fear of COVID-19 Scale among Chinese Population. Int J Ment Health Addiction. 2022;20:1273–88.
Chen I-H, Chen C-Y, Zhao K-Y, Gamble JH, Lin C-Y, Griffiths MD, et al. Psychometric evaluation of fear of COVID-19 scale (FCV-19S) among Chinese primary and middle schoolteachers, and their students. Curr Psychol. 2023;42:12557–73.
Chang K-C, Hou W-L, Pakpour AH, Lin C-Y, Griffiths MD. Psychometric testing of three COVID-19-Related scales among people with Mental Illness. Int J Ment Health Ad. 2022;20:324–36.
Lin C-Y, Hou W-L, Mamun MA, Aparecido da Silva J, Broche-Pérez Y, Ullah I, et al. Fear of COVID-19 scale (FCV-19S) across countries: measurement invariance issues. Nurs Open. 2021;8:1892–908.
Alimoradi Z, Lin C-Y, Ullah I, Griffiths MD, Pakpour AH. Item response theory analysis of the fear of COVID-19 scale (FCV-19S): a systematic review. Psychol Res Behav Ma. 2022;15:581–96.
Campbell-Sills L, Stein MB. Psychometric analysis and refinement of the connor–davidson resilience scale (CD-RISC): validation of a 10-item measure of resilience. J Traum Stress. 2007;20:1019–28.
Wang L, Shi Z, Zhang Y, Zhang Z. Psychometric properties of the 10-item Connor-Davidson Resilience Scale in Chinese earthquake victims: Chinese version of the 10-item CD-RISC. J Neuropsychiatry Clin Neurosci. 2010;64:499–504.
Ye ZJ, Qiu HZ, Li PF, Chen P, Liang MZ, Liu ML, et al. Validation and application of the Chinese version of the 10-item Connor-Davidson Resilience Scale (CD-RISC-10) among parents of children with cancer diagnosis. Eur J Oncol Nurs. 2017;27:36–44.
McDonald RP, Ho M-HR. Principles and practice in reporting structural equation analyses. Psychol Methods. 2002;7:64–82.
Leung K, Lau EHY, Wong CKH, Leung GM, Wu JT. Estimating the transmission dynamics of SARS-CoV-2 omicron BF.7 in Beijing after adjustment of the zero-COVID policy in November–December 2022. Nat Med. 2023;:1–4.
Qin T, Li X, Gu M, Wang Y, Yang Y, Bai X, et al. Cross-sectional online survey on depression and anxiety among the Population infected or non-infected with COVID-19 — China, December 2022. China CDC Weekly. 2023;5:235–40.
Khankeh H, Pourebrahimi M, Karibozorg M, Hosseinabadi-Farahani M, Ranjbar M, Ghods M, et al. Public trust, preparedness, and the influencing factors regarding COVID-19 pandemic situation in Iran: a population-based cross-sectional study. Asian J Soc Health Behav. 2022;5:154.
Jia Z, Du X, Du J, Xia S, Guo L, Su X, et al. Prevalence and factors associated with depressive and anxiety symptoms in a Chinese population with and without cardiovascular diseases. J Affect Disorders. 2021;286:241–7.
Shi L, Lu Z-A, Que J-Y, Huang X-L, Liu L, Ran M-S, et al. Prevalence of and risk factors Associated with Mental Health symptoms among the General Population in China during the Coronavirus Disease 2019 Pandemic. JAMA Netw Open. 2020;3:e2014053.
Yuan K, Zheng Y-B, Wang Y-J, Sun Y-K, Gong Y-M, Huang Y-T, et al. A systematic review and meta-analysis on prevalence of and risk factors associated with depression, anxiety and insomnia in infectious diseases, including COVID-19: a call to action. Mol Psychiatry. 2022;27:3214–22.
Iswanto AH, Gustina ZA, Murodov A, A BE-EY, Sattarova DG. Studying the role of islamic religious beliefs on depression during COVID-19 in Malaysia. HTS: Theological Studies. 2022;78:7567.
Kimhi S, Eshel Y, Marciano H, Adini B, Bonanno GA. Trajectories of depression and anxiety during COVID-19 associations with religion, income, and economic difficulties. J Psychiatr Res. 2021;144:389–96.
Zhao G-Q, Yong-Guang W, Yi-Qiang W, Ri-Fang C. a. O, Su-Fen < BR > FU. Psychological Crisis intervention in disasters: comment on Psychiatric View. Adv Psychol Sci. 2009;17:489.
Beck AT. Cognitive therapy of Depression. Guilford press; 1979.
Fitzpatrick KM, Drawve G, Harris C. Facing new fears during the COVID-19 pandemic: the state of America’s mental health. J Anxiety Disord. 2020;75:102291.
Clark DA, Beck AT. The Anxiety and Worry Workbook. 2011.
Yıldırım M, Özaslan A, Arslan G. Perceived risk and parental coronavirus anxiety in healthcare workers: a moderated mediation role of coronavirus fear and mental well-being. Psychol Health Med. 2022;27:1095–106.
Hjemdal O, Vogel PA, Solem S, Hagen K, Stiles TC. The relationship between resilience and levels of anxiety, depression, and obsessive-compulsive symptoms in adolescents. Clin Psychol Psychother. 2011;18:314–21.
Zhou X, Wu X, An Y. Understanding the relationship between Trauma exposure and depression among adolescents after earthquake: the roles of fear and resilience. Front Psychol. 2016;7.
Catalano D, Chan F, Wilson L, Chiu C-Y, Muller VR. The buffering effect of resilience on depression among individuals with spinal cord injury: a structural equation model. Rehabil Psychol. 2011;56:200–11.
Neff KD. The Development and Validation of a scale to measure Self-Compassion. Self and Identity. 2003;2:223–50.
Kotera Y, Tsuda-McCaie F, Edwards A-M, Bhandari D, Williams D, Neary S. Mental Health shame, Caregiver Identity, and Self-Compassion in UK Education Students. Healthc (Basel). 2022;10:584.
Chen Q, Liang M, Li Y, Guo J, Fei D, Wang L, et al. Mental health care for medical staff in China during the COVID-19 outbreak. Lancet Psychiatry. 2020;7:e15–6.
Pfefferbaum B, North CS. Mental Health and the Covid-19 pandemic. N Engl J Med. 2020;383:510–2.
Ye J, Chen TF, Paul D, McCahon R, Shankar S, Rosen A, et al. Stigma and discrimination experienced by people living with severe and persistent mental illness in assertive community treatment settings. Int J Soc Psychiatry. 2016;62:532–41.
Acknowledgements
We sincerely appreciate every participant in this study.
Funding
No funding.
Author information
Authors and Affiliations
Contributions
HL, DW, and YW conceived and designed the study. JY, KZ, ZJ, XW, NH, HY, ZS, and HC collected data and analyzed the data. HL, YH, DW, and YW wrote and revised the manuscript. All authors reviewed and approved the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee of The Affiliated Kangning Hospital of Wenzhou Medical University (Approval number: YJ-2023-16-01). The objectives of the study were explained to the study participants. And informed consent was obtained from them. They could withdraw anytime, and both refusal and incompletion would bear no consequences. Any personal information disclosed during the data collection was considered confidential and the data was secured anonymously. All methods were carried out in accordance with the declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lu, H., Yang, J., Zhao, K. et al. Perceived risk of COVID-19 hurts mental health: the mediating role of fear of COVID-19 and the moderating role of resilience. BMC Psychiatry 24, 58 (2024). https://doi.org/10.1186/s12888-024-05511-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-024-05511-x