
Abstract
Background
Suicidal ideation and attempts usually occur during adolescence time, and living in war- affected area make the problem more predominate and severe. To the best of our knowledge, there were no studies done among high school students who live in war affected areas in Ethiopia.
Objective
We assessed the prevalence and factors associated with suicide ideation and suicide attempts among high school students of war- affected area at Woldia town, Northeast, Ethiopia.
Methods
School based cross-sectional study was conducted from May 23 to June 08, 2022.Data were collected from high school students in Woldia town, Ethiopia. Pretested, self-administered Amharic-language questionnaire was used to collect the data. Bivariable and multivariable logistic regression was used to identify the independent factors associated with suicide ideation and attempt.
Results
A total of 668 of the 707 sampled students participated in the study (94.5% response rate). The prevalence of suicidal ideation and attempts among high school students in Woldia town was 16.29% and 12.87%, respectively. In the multivariable analysis, poor social support(AOR = 2.86, 95% CI:1.49, 5.46), posttraumatic stress disorder (AOR = 2.15, 95% CI:1.20, 3.85), family history of suicide(AOR = 3.94, 95% CI:2.21, 7.04), anxiety(AOR = 3.45, 95% CI:1.72, 6.89), and depression (AOR = 2.31, 95% CI:1.24, 4.33) were factors significantly associated with suicide ideation, and poor social support(AOR = 2.75, 95% CI:1.38, 5.47), depression (AOR = 4.27, 95% CI:2.10, 8.67) and being a female sex (AOR = 2.12, 95% CI:1.22, 3.69) were factors significantly associated with suicidal attempt.
Conclusions and recommendations
This study revealed that at least one in six and one in eight of the students had suicidal ideation and attempt, respectively. Therefore, we recommend that Ministry of Education shall work with Ministry of Health to extend and implement mental health services in high schools and provide social support to those students who need the services in order for the prevention of suicidal ideation and attempts.
Similar content being viewed by others

Introduction
Suicide is defined as deliberately trying of killing oneself. It is described as a death caused by self-inflicted injury, poisoning, or suffocation in which the person planned to commit suicide and the injury was towards the self. Suicidal ideation (SI) is defined as any self-reported desire to harm oneself that is not accompanied by any preparatory behavior. Suicidal attempt(SA) is a nonfatal outcome that is instigated and perpetrated by the person in question and culminates in self-harm [1].
Suicide is among the top 20 causes of death for all ages worldwide. Every 40 s, one person commits suicide in the world [2]. Suicidal ideation and suicidal attempts usually occur during adolescence time [3]. In adolescence, young people frequently go through significant changes, learn new abilities, and encounter difficulties that can lead to suicide [4]. About 67,000 adolescents worldwide die by suicide each year [5]. Of this, over 79% of global adolescent suicides occur in low- and middle-income countries (LMICs) [6]. Even though the majority of suicide research is conducted in high-income countries, the data suggests that low- and middle-income countries have also this health threat. A study using Global School-Based Health Survey (GSHS) from 46 LMIC showed that the pooled 12-month prevalence of suicidal ideation and attempt were 14.5% and 12.7%, respectively [7]. A study high school students in 40 low- and middle-income countries (LMICs) reported a pooled mean 12-month prevalence rate for suicide attempt of 17.2% [8]. In Asia, suicide accounts for about 60% of World suicides, with China, India, and Japan accounting for about 40% of the World’s suicides [9]. A study from sub-Saharan countries using GSHS survey reported that suicidal ideation ranges from 11.2 -31.9% [10].
Living in war affected areas in which people directly or indirectly faced traumatic events, made suicidal ideation and attempts more predominate and severe. According to the Diagnostic and Statistical Manual 5 (DSM-5), a traumatic event includes exposure to actual or threatened death, serious injury or sexual violation [11]. Exposure to such an event is followed by psychological distress such as re-experiencing the event, avoiding associations with the event, negative cognitions, and mood, arousal, and the traumatic event eliciting emotional responses such as shock, denial, flashbacks and memory loss [11]. Studies have documented the prevalence of various traumatic experiences, their effects on people's physical and mental health, and how these effects might lead to suicidal ideation an attempt [12]. According to studies conducted in Lebanon, Afghanistan, and South Africa, between 50 and 70 percent of the population has experienced at least one traumatic event as a result of conflicts [13,14,15]. In Ethiopia there are also areas affected by traumatic events, for example, Woldia town, which is found in North Wollo in Northeast of Ethiopia, is one of the recently war-affected area in the last one year. High school students in this town were one of the demographic groups affected by the conflict's aftereffects. Most of the studies focusing on trauma and suicidality have been done in developed countries until now. Researches done in Bangladesh and Lebanon indicate that students who had traumatic experiences are more likely to have suicidal ideation [16, 17]. Increased suicidalities were discovered in African studies, for example, those conducted with students from war-affected places of South Africa and Uganda [18, 19].
Suicide and attempted suicide have detrimental emotional, physical, and financial effects. Suicidal attempt survivors may sustain severe trauma to themselves that have a long-term negative impact on their beings. Additionally, they could struggle with depression and other mental health problems and friends, relatives, coworkers of them, and the communities as a whole are affected. When someone commits suicide, their remaining relatives and friends may feel shock, angry, guilty, and show symptoms of depression and anxiety, or even have suicidal ideation of themselves [20]. Suicide costs society a lot of money as well. In terms of medical expenses, lost wages from employment, loss of statistical life, and quality of life expenditures, suicide, and nonfatal self-harm cost the country almost $490 billion in 2019 [21].
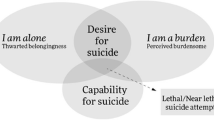
According to the studies, a number of factors affect high school students' suicidal ideation and attempts. Among these factors are PTSD, which has been shown to affect suicidal ideation in high school students in studies conducted in the United States and the United Kingdom [22,23,24], the interpersonal psychological theory of suicide stated that a combination of three interpersonal constructs such as thwarted belongingness (TB), perceived burdensomeness (PB) associated with sense of hopelessness about the possibility of change in these state and the third construct, acquired capability for suicide (AC) which is required condition before acting on the desire for suicide, are an important risk factors for suicide [25,26,27,28]. Other factors include female gender, lack of social support, loneliness, anxiety, being physically harmed, and the use of alcohol and other drugs [7, 29,30,31,32,33,34] and, school absenteeism were reported as a factor affecting suicidal ideation and attempt among high school students [31, 35, 36], disappointing with school results were also a factor that affect suicidal ideation and attempt among high school students [31, 37, 38]. In order to halt the threat of suicidal ideation and attempt, it is advisable to work on reducing risk factors and increasing protective factors and resilience among those students who live in war-affected areas. In these regards, different studies were done especially among developed countries, studies done in Ethiopia showed suicidal attempts of 12.5% and 16.2% in their life time respectively [31, 39], but these studies were not done in war affected areas, the current study assessed the prevalence and factors associated with suicidal ideation and attempt among high school students in the last 12 months after war affect in the area of Woldia.
Methods and materials
Study area and populations
An institutional-based cross-sectional study was conducted in May 2022 at four Secondary and High Schools of war-affected area in Northeast Ethiopia. The Schools are Woldia Comprehensive and Secondary school, Millennium Comprehensive and Secondary School, Genetie Comprehensive and Secondary School, and Mesenado Comprehensive and Secondary School.
The study area is situated in North Wollo Zone in the Amhara National Regional State with a distance of 521 km from Addis Ababa, the capital city of Ethiopia. A total of 46,139 people lived in the study area with 23,000 men and 23,139 women. Among the total population, 80.49% of the people were followers of Ethiopian Orthodox Christians religion, while 18.46% were followers of Muslim religion.
All high school students who attended their class during data collection time were included in this study. Whereas students who lived in the study area for less than one year and students who were unable to communicate due to acute illness during data collection time were excluded from this study.
Sample size determination and procedures
The sample size was determined by assuming a single population proportion formula with the assumptions. The prevalence of suicidal ideation and attempt were 17.7% and 18.5% respectively [40], with 95% confidence interval (CI) and margin of error 2%, and 10% non-response rate. And then the final sample size for suicidal ideation was 683 and for suicidal attempt was 707, we have used 707 since it is higher than 668.
Before the actual data collection time, students were first stratified by their grade level as grade nine, grade ten, grade eleven, and grade twelve, considering each grade level as strata. The data we get from Education be rue of the study region showed that there were a total of 5100 high school students. Among these, grade nine accounts 1606, grade ten accounts 1230, grade eleven acounts1179, and grade twelve accounts 1085 of the students from the total high school students. Then, we made a proportional allocation for each stratum (grade levels) and as a result, 223 students from grade nine, 171 students from grade ten, 163 students from grade eleven, and 150 students from grade twelve were drawn. Finally, a computer generated lottery method using student’s identification number was applied to select study participants from each stratum. At the end, the selected students in each stratum were taken to one hall, and then the questioners were administered after orientation.
Data were collected using a structured self-administered questionnaire which includes: an outcome variable, suicidal ideation and attempt, which was assessed by using Composite international diagnostic interview (CIDI) with yes/no questions. Socio-demographic characteristics such as age, sex, and grade level were collected by using structured socio-demographic questionnaires. Clinical factors like family history of suicide, mental illness, and history of chronic medical illness were assessed using a structured yes/no questionnaire, history of anxiety, depression, and PTSD were assessed using GAD-7, PHQ-9, and PCL-5 respectively. Substance related factors, including Khat, tobacco, and alcohol which were assessed using a yes/no questionnaires adapted from the ASSIST (Alcohol,Smoking, and Substance Involvement Screening Test) [41, 42]. Finally, psychosocial factors including social support level, which was assessed using OSLO 3-items social support scale with scores ranging between 3 and 8 were classified as poor social support, a score between 9 and 11 as intermediate social support, and a score between 12 and 14 as strong social support level, and disappointed with school results, school absenteeism, having physical harm, were assessed using structured yes /no questions [43].
To control the quality of data, the questionnaire was translated appropriately into the local Amharic language. The training was given to data collectors and supervisors and each completed questionnaire was checked and the necessary feedback was also offered to data collectors following each morning. The questionnaire was pretested one week before the actual data collection time on 5% (n = 36) of the study participants who were not included in the main study.
The dependent variable assessment tool (PCL-5) had Cronbach alpha of 0.81. Based on the feedback obtained from the pretest, an appropriate modification was made to the questionnaire. The collected data were coded, edited, entered, and checked into the computer using EPI data version 4.6.02 and imported to STATA version 14.0 to generate descriptive statistics like means, standard deviation, frequency, and percentages. To determine an association between dependent and independent variables, adjusted odds ratios were used using logistic regression and the significance level was determined using a confidence interval of 95%. Bivariable and multivariable logistic regression was used to identify the independent predictors of PTSD. Each independent variable was separately entered in the bivariable analysis. Then variables with a p-value < 0.2 on bivariable analysis were entered into multivariate analysis. Then variables that showed a statistically significant association with a p-value < 0.05 on logistic regression were considered predictors of PTSD.
Results
Socio demographic characteristics of participants
Data were obtained from 668 high school students with a response rate of 94.5%. The mean age of the participants was 17.85 ± 1.658, ranging from 14 to 25 years old, and the majority of participants aged for 44.16% of participants were ranging between 14 and 18 years old. More than half the number (58.68%) of the participants was males, meanwhile 60.63% of them were living in urban areas as shown in Table 1 below.
Clinical characteristics of the respondents
Out of total participants, 41.1% had posttraumatic stress disorder, 11.1% of students had a history of chronic medical illness, and 12.6% of students had a family history of mental illness, 15.7% had a family history of suicide, 39.52% anxiety, and 38.5% depression as seen in Fig. 1.

Shows clinical characteristics of study participants
Substance related characteristics of participants
Regarding substance use, out of the students 66.8% were ever alcohol drinkers, whereas khat and cigarette ever users were 22.1% and 9.3%, respectively, 38.6% of them were current alcohol drinkers as seen in Fig. 2.

Shows substance -related characteristics of study participants and the number of study participants with specific substance related characteristics
Psychosocial characteristics of participants
From the participants, about one-third of students had strong social supports 33.1%, whereas students who had moderate and poor social supports were 41.2%, and 25.7%, respectively as seen in Fig. 3. Students who have been absented for greater than or equal to 4 days per month from school were 11.98%, and 12.87% of students experienced physical harm and 44.6% of the students were disappointed with their school results.

Shows social support level of study participants
Prevalence and associated factors of suicidal ideation and attempt
Prevalence of suicidal ideation and associated factors
In this study, the overall prevalence of suicidal ideation among high school students was 16.29% (95%, CI: 13.67%, 19.29%). Being female in sex, urban residency of students, having chronic medical illness, poor social support, having PTSD, having family history of suicide, ever and current alcohol drinking, having anxiety, and depression were factors associated with suicidal ideation at p < 0.2 in binary logistic regression.
Finally, in the analysis of multivariable logistic regression model findings revealed that having depression, family history of suicide, PTSD, anxiety and poor social support were found to be significantly associated with suicidal ideation with 95% of CI and at p- value < 0.05 as shown in Table 2 below.
Students who had poor social support were 2.86 times more likely to have suicidal ideation compared to students who had strong social support (AOR = 2.86, 95% CI: 1.49, 5.46).
Students who had a family history of suicide were about 3.9 times more likely to have suicidal ideation compared to those who had not a family history of suicide (AOR = 3.94, 95% CI: 2.21, 7.04).
Students who had PTSD were about 2.1 times more likely to have suicidal ideation than students who had not (AOR = 2.15, 95% CI:1.20, 3.85). Students who had anxiety were 3.5 times more likely to have suicidal ideation than students who had not anxiety (AOR = 3.45, 95% CI:1.72, 6.89).
Students who had depression reported 2.3 times higher suicidal ideation than students who had not depression (AOR = 2.31, 95% CI:1.24, 4.33).
Prevalence of suicidal attempts and associated factors
In the current study, the overall prevalence of suicidal attempts among high school students demonstrated 12.87% (95%, CI: 10.53%, 15.64%). Of those who attempted suicide, five methods of suicide attempt were used. Hanging was more used by boys (7.11%) than girls (6.32%) and poisoning was more (16.7%) used by the girls than boys (2.86%).
Jumping from high places and the use of sharp tools were less frequently used as means of suicidal attempts. Concerning the seriousness of the suicidal attempts, 54.6% of study participants report” I made a serious attempt to kill myself and it was only luck that I did not succeed” and 20.1% had attempted suicide to “cry for help”. Among attempters of suicide to cry for help, girls were higher than boys. Respondents gave a variety of reasons for their suicide attempt, among these family conflict, history of mental illness, and other reason than from response options were the most frequent reasons for suicidal attempts. Family conflict, and other reason from the response options were more frequently given as reasons for suicide attempts for the girls than boys, but having history of mental illness were the reason for suicidal attempts reasoned by both sexes equally.
Being female in sex, urban residency background, having chronic medical illness, poor social support, having PTSD, having family history of suicide, mental illness, current alcohol drinking, having anxiety, and depression were factors associated with suicidal attempt at p < 0.2 in binary logistic regression. Finally, the multivariable analysis model revealed that having depression, female sex, and having poor social support were found to be significantly associated with suicidal attempts with 95% of CI and at p < 0.05 as shown in Table 3 below.
Students who had poor social support were 2.8 times more likely to have a suicidal attempt compared to students who had strong social support (AOR = 2.75, 95% CI:1.38, 5.47). Female students reported 2.1 times greater suicidal attempt than male (AOR = 2.12, 95% CI:1.22, 3.69). Students who had depression were 4.3 times more likely to have a suicidal attempts than students who had not depression (AOR = 4.27, 95% CI:2.10, 8.67).
Discussion
The findings of the current study showed that the prevalence of suicidal ideation among high school students in Woldia town was 16.29% (95%, CI: 13.67%, 19.29%), which was inline with studies done in Ghana, Mozambique, US, middle and high income countries (M-HICs) from the six World Health Organization (WHO) regions, whose reported prevalence indicated 18.2%, 17.7%, 18.8%, and 14% respectively [35, 40, 44, 45].
However, the prevalence of suicidal ideation in this study was higher than previous studies done in Bangladesh, India, Thailand, with suicidal ideation of 9.3%, 5%, 8.8% respectively [38, 46, 47]. The possible reason for this difference may be due to the difference in socioeconomic and availability of health facilities and health professionals between those countries and Ethiopia in which factors like depression and other mental health risk factors of suicidal ideation may early detected and treated [48].
On the other hand, the current prevalence was lower than the prevalence of suicidal ideation found in the studies done in Benin, Poland, and Peru, which was 23.2%, 24.66% and 26.3% respectively [33, 49, 50]. The possible reason for this variation may be due to the difference in the composition of the study participant in the study, for example, in the study of Poland there were the greater proportion of female participants(70%) were involved in the study when compared with this study(41.3%) which might increase the risk of suicidal ideation [51].
The prevalence of suicidal attempts among high school students in this study was 12.87% (95%, CI: 10.53%, 15.64%), which was consistent with previous studies done in Bhutan and South Africa with a suicidal attempts of 11.3% and 14.8% respectively [51, 52].
However, the prevalence of suicidal attempts in this study was higher than previous studies done in Bangladesh, China, and United states of America, which showed the prevalence of suicidal attempt as 5.9%, 3.3% and 8.9% respectively [45, 53, 54]. The possible reason for this difference may be due to the difference in socioeconomic and availability of health facilities and health professionals between those countries and Ethiopia in which factors like depression and other mental health risk factors of suicidal ideation may early detected and treated [48].
On the other hand, the current prevalence was lower than the previous studies done in Benin, Liberia, Guatemala, and Mongolia, which found the prevalence of suicidal attempts as 28.3%, 33.7%, 16.6% and 32.2% respectively [32, 49, 55, 56]. The reason for this variation may be that in a study of Guatemala and Mongolia, there had been a greater number of female participants(more than 50%), but in the current study, females were lower than male participants 41.3%, and the risk of suicidal attempts was increased among female than males [57].
The odds of suicidal ideation were 2.86 times higher among high school students who had poor social support compared to those who had strong social support. This was supported by studies done in 46 low-and middle-income countries, Ethiopia and Malaysia [7, 29, 37]. The reason for this may be that social support makes a person feel that he/she is cared for and loved, regarded, and a member of a network of mutual duties which might decrease the risk of suicidal ideation [58]. Furthermore, social support can also aid people in coping with stressful situations and the challenges brought on by psychopathology, which may lower the risk of suicide [58]. Thus, indicating that social support may be particularly valuable for helping the most vulnerable individuals.
The odds of having suicidal ideation were 2.1 times higher among students who had posttraumatic stress disorder (PTSD) compared to those who had not posttraumatic stress disorder (PTSD). Studies had also been revealed results [22,23,24, 59]. The reason for this could be that those with PTSD are more likely to experience suicidal ideation because they have trouble controlling their emotions and their urges [60]. The other reason for this may be that sometimes those who suffer from PTSD also struggle with despair, panic attacks, extreme anxiety, or substance abuse, this could increase the chance of suicidal ideation, and individuals might believe that the only option is to commit suicide [61]. Hence, we have to give concern about the symptoms of PTSD by having treatment options like either PE (prolonged exposure) or CPT (cognitive processing therapy) [62]
The odds of having suicidal ideation were 3.9 times more likely among students who had a family history of suicide compared to those who had not a family history of suicide. This finding was supported by studies done in different countries [39, 63,64,65]. The reason for this could be a genetic etiology [66].The other possible reason may be that mental health problems, such as depression, are inherent, which may increase the risk of suicidal ideation on off spring [67]. This suggests emphasizing students with a family history of depression or suicide.
Students who had anxiety were 3.5 times more likely to have suicidal ideation compared to their counter parts. This was supported by studies done in Malaysia, and Mozambique [40, 68]. The reason for this may be that a person with anxiety symptoms faces an intolerance of the pain that anxiety causes, especially, when /she reaches the level of panic, and a person may have suicidal ideation as a solution to escape from this pain. Another possible reason could be that individuals with anxiety symptoms have an increased risk of having comorbidities with depression, which has a direct effect on suicidal ideation [69]. This finding suggested that working on anxiety is paramount to reduce suicidal ideation. We may have the following means of managing anxiety disorder such as learning about anxiety, mindfulness, relaxation techniques, correct breathing techniques, dietary adjustments, exercise, learning to be assertive, building self-esteem, cognitive therapy, exposure therapy, structured problem solving, medication and support groups (https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/anxiety-treatment-options#managing-anxiety).
Students who had depression were 2.3 times more likely to have suicidal ideation as compared to those who had not depression. This was supported by studies done in Sub Saharan Africa, in Zambia, Tunisia, and Nigeria and in Thailand [47, 70,71,72]. The reason for this could be that the direct impact of depression, which makes people feel hopeless and worthless, which in turn increases the risk of suicidal ideation [73]. Hence, giving priority for depressed individual is vital means to reduce suicidal ideation. Here are typical examples to reduce depression; practicing self-care such as getting regular sleep and exercise, and maintaining healthy nutritional practices; having open, honest conversations about what you or someone else with depression with suicidal ideation may be experiencing and feeling; learning and recognizing the warning signs of depression with suicidal ideation (https://www.healthline.com/health/depression/suicidal-depression).
The odds of suicidal attempts were 2.8 times higher among students who had poor social support compared to those who had strong social support. This was supported by studies done in 46 low-and middle-income countries and two studies done in Ethiopia [7, 31, 37]. The reason for this could be due to that those with poor social support feel that their existence was a burden on others such as family members. In addition, social support can refer to the presence of those who can aid people in coping with stressful situations and the challenges brought on by psychopathology, which may lower the risk of suicidal attempt [58]. Therefore, comprehensive MHPSS programs for war-affected people that integrate somatic health concerns, social support, education, and targeted psychiatric/psychological interventions are urgently needed [74].
Students who had depression were 4.3 times more likely to have suicidal attempts compared to their counter parts. Studies done in Ethiopia, India, Tunisia and Nigeria were also revealed this [37, 38, 70, 71]. The reason behind this may be that it was indicated that the decreased level of serotonin neurotransmitters in the brain of a depressed individual was found to be associated with increased suicidal attempt [75]. The other reason for this could be that the direct impact of depression, which makes people feel hopeless and worthless, which in turn increases the risk of suicidal attempt [73]. In addition, peoples may have symptoms like hopelessness, helplessness, giving up, feeling of isolation, and despair which were the core features of demoralization which in turn leads to suicidal attempts [76].
The odds of having suicidal attempts were 2.1 times more likely among female students than males. This was supported by studies done in Ethiopia and Benin [7, 37, 49]. The reason for this association may be due to the fact that gender related vulnerability to psychopathology and to psychosocially disadvantageous circumstances. More specifically, depression is the most common risk factor for serious suicidal attempts in both men and women, but happens twice as often in girls as in men. This implies that great emphasis should be given for females.
Limitations of the study
This study is conducted with some limitations. Since it was cross-sectional study, it could be difficult to declare cause-and effect relationship between suicidal ideation and attempt and factors like social support, depression, PTSD, and anxiety in addition, recall bias may occur during data collection since the study collected retrospective data of 12 months. Furthermore, we did not use a specific scale to assess suicidal ideation such as Beck's scale. Beck’s scale contain 19 items and each item is scored from 0 to 2 in ascending order of.severity, giving a total score ranging from 0 to 38 [77].
Conclusions and recommendations
This study revealed that at least one in six of the high school students in the sample had experienced suicidal ideation and one in eight had attempted suicide. The distribution of suicidal ideation among high school students showed that it was higher in students with PTSD, anxiety, depression and among those who have a family history of suicide and poor social support. The current study had also showed that suicidal attempt was higher among female students, students who had poor social support, and students who had depression. Therefore, we recommend that Ministry of Education shall work with Ministry of Health to extend and implement mental health services in high schools and provide social support to those students who need the services in order for the prevention of suicidal ideation and attempts.
Availability of data and materials
Data is available upon request from the corresponding author.
References
Lester D. The language of suicide. The end of suicidology continued: David Lester 2 An ecological study of handedness and suicide rates: David Lester & Behnam Tavakkol 6 Nick: Drake: An analysis of the song lyrics of a suicide: David Lester 12. 2021;2(3):37.
Silva LSD, Silva PAD, Demenech LM, Vieira MECD, Silva LN, Dumith SC. Suicide risk in high school students: who are the most vulnerable groups? Rev Paul Pediatr. 2022;41:e2021236. https://doi.org/10.1590/1984-0462/2023/41/2021236.
Constantinou SJ. Risk Factors of Suicidal Behaviour in Children & Adolescents. 2021.
Alves C, Dell’Aglio D. Social support and risk behavior in adolescence. Psico. 2015;46:165–75.
Jacob L, Stubbs B, Koyanagi A. Consumption of carbonated soft drinks and suicide attempts among 105,061 adolescents aged 12–15 years from 6 high-income, 22 middle-income, and 4 low-income countries. Clin Nutr. 2020;39(3):886–92.
WHO. SUICIDE in low and middle income countries. 2019.
Li L, You D, Ruan T, Xu S, Mi D, Cai T, Han L. The prevalence of suicidal behaviors and their mental risk factors among young adolescents in 46 low-and middle-income countries. J Affect Disord. 2021;281:847–55.
Liu X, Huang Y, Liu Y. Prevalence, distribution, and associated factors of suicide attempts in young adolescents: School-based data from 40 low-income and middle-income countries. PLoS One. 2018;13(12): e0207823.
Chen Y-Y, Chien-Chang Wu K, Yousuf S, Yip PS. Suicide in Asia: opportunities and challenges. Epidemiol Rev. 2012;34(1):129–44.
Tolulope O, Olutayo A, Babatunde S, Adesanmi A. Suicidality in a non-clinical sample of Nigerian adolescents: prevalence and correlates. Suicidology Online. 2019;10(7):1–8.
APA. Diagnostic Statistical Manual 5-Text Revision. 2022.
Silva M, Pereira H. The impact of life trauma on mental health and suicidal behavior: a study from portuguese language countries. Behav Sci. 2022;12(4):102.
Neyazi A, Haidarzada AS, Rangelova V, Erfan A, Bashiri B, Neyazi M, Faizi N, Konşuk-Ünlü H, Griffiths MD. Prevalence and predictors of depression among women in Afghanistan: a cross-sectional study. Discover Psychol. 2023;3(1):7.
Rastegar PJ, Chenoweth F, Schwebel DC. Mental health and injury outcomes in Liberia, 1990–2017: an ecological systems analysis. Soc Health Sci. 2022;20(1):1–20.
Venter N. The role of resilience in the relationship between exposure to trauma and suicide ideation (Doctoral dissertation, University of the Free State). 2017:22–3.
Baroud E, Ghandour LA, Alrojolah L, Zeinoun P, Maalouf FT. Suicidality among Lebanese adolescents: prevalence, predictors and service utilization. Psychiatry Res. 2019;275:338–44.
Rahman ME, Saiful Islam M, Mamun MA, Moonajilin MS, Yi S. Prevalence and factors associated with suicidal ideation among university students in Bangladesh. 2020:1–10.
Okello J, De Schryver M, Musisi S, Broekaert E, Derluyn I. Differential roles of childhood adversities and stressful war experiences in the development of mental health symptoms in post-war adolescents in northern Uganda. BMC Psychiatry. 2014;14(1):1–8.
Sorsdahl K, Stein DJ, Williams DR, Nock MK. Associations between traumatic events and suicidal behaviour in South Africa. J Nervous Mental Dis. 2011;199(12):928.
Lee E. Experiences of bereaved families by suicide in South Korea: a phenomenological study. Int J Environ Res Public Health. 2022;19(5):2969.
Peterson C, Miller GF, Barnett SBL, Florence C. Report MW: economic cost of injury-United States, 2019. Morbid Mortal Wkly Rep. 2021;70(48):1655.
Panagioti M, Angelakis I, Tarrier N, Gooding P. A prospective investigation of the impact of distinct posttraumatic (PTSD) symptom clusters on suicidal ideation. Cogn Ther Res. 2017;41(4):645–53.
Panagioti M, Gooding PA, Tarrier N. A meta-analysis of the association between posttraumatic stress disorder and suicidality: the role of comorbid depression. Comprehensive Psychiatry. 2012;53(7):915–30.
Stanley IH. Advancements in the understanding of PTSD and suicide risk: Introduction to a special section. Psychol Trauma. 2021;13(7):723.
Baertschi M, Costanza A, Richard-Lepouriel H, Pompili M, Sarasin F, Weber K, Canuto A. The application of the interpersonal-psychological theory of suicide to a sample of Swiss patients attending a psychiatric emergency department for a non-lethal suicidal event. J Affect Disord. 2017;210:323–31.
Costanza A, Ambrosetti J, Wyss K, Bondolfi G, Sarasin F, Khan R. Prevention of suicide at Emergency Room: from the «Interpersonal Theory of Suicide» to the connectedness. Revue medicale suisse. 2018;14(593):335–8.
Joiner TE. “Why people die by suicide”. Harvard University Press; 2005. p. 38–9.
Van Orden KA, Witte TK, Cukrowicz KC, Braithwaite SR, Selby EA, Joiner TE Jr. The interpersonal theory of suicide. Psychol Rev. 2010;117(2):575.
Chan YY, Lim KH, Teh CH, Kee CC, Ghazali SM, Lim KK, Khoo YY, Tee EO, Ahmad NA, Ibrahim N et al. Prevalence and risk factors associated with suicidal ideation among adolescents in Malaysia. 2018, 30(3).
Khan M, Ali M, Rahman M, Islam M, Karim M, Hasan M, Jesmin SS. Suicidal behavior among school-going adolescents in Bangladesh: findings of the global school-based student health survey. Soc Psychiatry Psychiatr Epidemiol. 2020;55(11):1491–502.
Amare T, Meseret Woldeyhannes S, Haile K, Yeneabat T. Prevalence and associated factors of suicide ideation and attempt among adolescent high school students in Dangila Town Northwest Ethiopia. Psychiatry J. 2018;2018:7631453.
Badarch J, Chuluunbaatar B, Batbaatar S, Paulik E. Suicide attempts among school-attending adolescents in Mongolia: associated factors and gender differences. Int J Environ Res Public Health. 2022;19(5):2991.
Sharma B, Nam EW, Kim HY, Kim JK. Factors associated with suicidal ideation and suicide attempt among school-going urban adolescents in Peru. Int J Environ Res Public Health. 2015;12(11):14842–56.
Valdez-Santiago R, Solórzano EH, Iñiguez MM, Burgos LÁ, Hernández HG, González ÁM. Attempted suicide among adolescents in Mexico: prevalence and associated factors at the national level. Inj Prev. 2018;24(4):256–61.
Asante KO, Kugbey N, Osafo J, Quarshie EN-B, Sarfo JO. The prevalence and correlates of suicidal behaviours (ideation, plan and attempt) among adolescents in senior high schools in Ghana. SSM Popul Health. 2017;3:427–34.
Epstein S, Roberts E, Sedgwick R, Polling C, Finning K, Ford T, Dutta R, Downs J. School absenteeism as a risk factor for self-harm and suicidal ideation in children and adolescents: a systematic review and meta-analysis. Eur Child Adolesc Psychiatry. 2020;29(9):1175–94.
Giru BW. Prevalence and associated factors of suicidal ideation and attempt among high school adolescent students in Fitche Town, north Shoa, Oromia region, Ethiopia, 2012: Institutional based cross sectional study. Journal of Health, Medicine and Nursing. 2016;23.
Ismail IS, Abdulsatar K, Baey HA. Prevalence and associated factors of suicidal behaviorl among secondary school students in Kut City. Med J Babylone. 2011, 8(4).
Giru BW: Prevalence and associated factors of suicidal ideation and attempt among high school adolescent students in Fitche Town, north Shoa, Oromia region, Ethiopia, 2012: Institutional based cross sectional study. J Health Med Nurs 2016, 23.
Seidu A-A, Amu H, Dadzie LK, Amoah A, Ahinkorah BO, Ameyaw EK, Acheampong HY, Kissah-Korsah K. Suicidal behaviours among in-school adolescents in Mozambique: Cross-sectional evidence of the prevalence and predictors using the Global School-Based Health Survey data. PLoS One. 2020;15(7):e0236448.
Gryczynski J, Kelly SM, Mitchell SG, Kirk A, O’Grady KE, Schwartz RP. Validation and performance of the A lcohol, S moking and S ubstance I nvolvement S creening T est (ASSIST) among adolescent primary care patients. Addiction. 2015;110(2):240–7.
Newcombe D, Tanielu-Stowers H, McDermott R, Stephen J, Nosa V. The validation of the alcohol, smoking and substance involvement screening test (ASSIST) amongst Pacific people in New Zealand. NZJ Psychol. 2016;45(1).
Dalgard OS, Dowrick C, Lehtinen V, Vazquez-Barquero JL, Casey P, Wilkinson G, Ayuso-Mateos JL, Page H, Dunn G. Negative life events, social support and gender difference in depression. Soc Psychiatry Psychiatr Epidemiol. 2006;41(6):444–51.
Biswas T, Scott JG, Munir K, Renzaho AM, Rawal LB, Baxter J, Mamun AA. Global variation in the prevalence of suicidal ideation, anxiety and their correlates among adolescents: a population based study of 82 countries. EClinicalMedicine. 2020;24:100395.
Ivey-Stephenson AZ, Demissie Z, Crosby AE, Stone DM, Gaylor E, Wilkins N, Lowry R, Brown M. Suicidal ideation and behaviors among high school students—youth risk behavior survey, United States, 2019. MMWR Suppl. 2020;69(1):47.
Farheen S, Jahan M. depression and suicidal ideation among school going adolescents does gender matters? Adv Innov Res. 2019;6(2):26.
Peltzer K, Pengpid S. Suicidal ideation and associated factors among school-going adolescents in Thailand. Int J Environ Res Public Health. 2012;9(2):462–73.
Kapusta ND, Posch M, Niederkrotenthaler T, Fischer-Kern M, Etzersdorfer E, Sonneck G. Availability of mental health service providers and suicide rates in Austria: a nationwide study. Psychiatr Serv. 2010;61(12):1198–203.
Randall JR, Doku D, Wilson ML, Peltzer K. Suicidal behaviour and related risk factors among school-aged youth in the Republic of Benin. PLoS One. 2014;9(2):e88233.
Zygo M, Pawłowska B, Potembska E, Dreher P, Kapka-Skrzypczak L. Prevalence and selected risk factors of suicidal ideation, suicidal tendencies and suicide attempts in young people aged 13–19 years. Ann Agric Environ Med. 2019;26(2):329–36.
Dema T, Tripathy JP, Thinley S, Rani M, Dhendup T, Laxmeshwar C, Tenzin K, Gurung MS, Tshering T, Subba DK. Suicidal ideation and attempt among school going adolescents in Bhutan–a secondary analysis of a global school-based student health survey in Bhutan 2016. BMC Public Health. 2019;19(1):1–12.
Khuzwayo N, Taylor M, Connolly C. High risk of suicide among high-school learners in uMgungundlovu District, KwaZulu-Natal Province South Africa. South Afr Med J. 2018;108(6):517–23.
Liu B-P, Wang X-T, Liu Z-Z, Wang Z-Y, Liu X, Jia C-X. Stressful life events, insomnia and suicidality in a large sample of Chinese adolescents. J Affect Disord. 2019;249:404–9.
Irish A, Murshid NS. Suicide ideation, plan, and attempt among youth in Bangladesh: Incidence and risk factors. Children Youth Serv Rev. 2020;116:105215.
Pengpid S, Peltzer K. Prevalence and correlates of past 12-month suicide attempt among in-school adolescents in Guatemala. Psychol Res Behav Manag. 2019;12:523.
Quarshie EN-B, Onyeaka HK, Oppong Asante K. Suicidal behaviours among adolescents in Liberia. BMC Psychiatry. 2020;20(1):1–12.
Tang J, Li G, Chen B, Huang Z, Zhang Y, Chang H, Wu C, Ma X, Wang J, Yu Y. Prevalence of and risk factors for non-suicidal self-injury in rural China: results from a nationwide survey in China. J Affect Disord. 2018;226:188–95.
Kleiman EM, Liu RT. Social support as a protective factor in suicide: Findings from two nationally representative samples. J Affect Disord. 2013;150(2):540–5.
Holliday R, Borges LM, Stearns-Yoder KA, Hoffberg AS, Brenner LA, Monteith LL. Posttraumatic stress disorder, suicidal ideation, and suicidal self-directed violence among US military personnel and veterans: a systematic review of the literature from 2010 to 2018. Front Psychol. 1998;2020:11.
Kachadourian LK, Gandelman E, Ralevski E, Petrakis IL. Suicidal ideation in military veterans with alcohol dependence and PTSD: The role of hostility. Am J Addict. 2018;27(2):124–30.
Sher L, Braquehais MD, Casas M. Posttraumatic stress disorder, depression, and suicide in veterans. Cleveland Clinic J Med. 2012;79(2):92.
Gradus JL, Suvak MK, Wisco BE, Marx BP, Resick PA. Treatment of posttraumatic stress disorder reduces suicidal ideation. Depress Anxiety. 2013;30(10):1046. https://doi.org/10.1002/da.22117.
Dendup T, Zhao Y, Dorji T, Phuntsho S. Risk factors associated with suicidal ideation and suicide attempts in Bhutan: an analysis of the 2014 Bhutan STEPS Survey data. PLoS One. 2020;15(1):e0225888.
Qaddoura N, Dardas LA, Pan W. Psychosocial determinants of adolescent suicide: a national survey. Arch Psychiatr Nurs. 2022;40:15–24.
Simbar M, Golezar S, Alizadeh S, Hajifoghaha M. Suicide risk factors in adolescents worldwide: a narrative review. J Rafsanjan Univ Med Sci. 2018;16(12):1153–68.
Lengvenyte A, Conejero I, Courtet P, Olié E. Biological bases of suicidal behaviours: a narrative review. Eur J Neurosci. 2021;53(1):330–51.
Jang S-I, Bae H-C, Shin J, Jang S-y, Hong S, Han K-T, Park E-C. The effect of suicide attempts on suicide ideation by family members in fast developed country. Korea Comprehensive Psychiatry. 2016;66:132–8.
Chan YY, Lim KH, Teh CH, Kee CC, Ghazali SM, Lim KK, Khoo YY, Tee EO, Ahmad NA, Ibrahim N. Prevalence and risk factors associated with suicidal ideation among adolescents in Malaysia. Int J Adolesc Med Health. 2016;30(3):20160053.
Derese A, Tesfaye G, Teshome M. Prevalence and Factors Associated with Depression, Suicidal Ideation and Attempt among Haramaya University Students. 2015:11.
Adewuya AO, Oladipo EO. Prevalence and associated factors for suicidal behaviours (ideation, planning, and attempt) among high school adolescents in Lagos. Nigeria Eur Child Adolesc Psychiatry. 2020;29(11):1503–12.
Guedria-Tekari A, Missaoui S, Kalai W, Gaddour N, Gaha L. Suicidal ideation and suicide attempts among Tunisian adolescents: prevalence and associated factors. Pan Afr Med J. 2019;34:105.
Page RM, West JH. Suicide ideation and psychosocial distress in sub-Saharan African youth. Am J Health Behav. 2011;35(2):129–41.
Pompili M, Gibiino S, Innamorati M, Serafini G, Del Casale A, De Risio L, Palermo M, Montebovi F, Campi S, De Luca V. Prolactin and thyroid hormone levels are associated with suicide attempts in psychiatric patients. Psychiatry Res. 2012;200(2–3):389–94.
Costanza A, Amerio A, Aguglia A, Magnani L, Huguelet P, Serafini G, Pompili M, Amore M. Meaning-centered therapy in Ukraine’s war refugees: An attempt to cope with the absurd? Front Psychol. 2022;13:1067191.
Modestino EJ, Blum K, Dennen CA, Downs BW, Bagchi D, Llanos-Gomez L, Elman I, Baron D, Thanos PK, Badgaiyan RD. Theorizing the Role of Dopaminergic Polymorphic Risk Alleles with Intermittent Explosive Disorder (IED), Violent/Aggressive Behavior and Addiction: Justification of Genetic Addiction Risk Severity (GARS) Testing. J Personal Med. 2022;12(12):1946.
Costanza A, Vasileios C, Ambrosetti J, Shah S, Amerio A, Aguglia A, Serafini G, Piguet V, Luthy C, Cedraschi C, Bondolfi G. Demoralization in suicide: a systematic review. J Psychosom Res. 2022;1(157): 110788.
Baertschi M, Costanza A, Canuto A, Weber K. The dimensionality of suicidal ideation and its clinical implications. Int J Methods Psychiatr Res. 2019;28(1): e1755.
Acknowledgements
We would like to express our thanks to the University of Gondar for giving us the chance to conduct this research. The author’s appreciation also goes to the study participants, data collectors, and supervisors.
Funding
Funding is not applicable.
Author information
Authors and Affiliations
Contributions
MA conceptualized the study and was involved in the design, analysis, interpretation, report, and manuscript writing. GN, GN, MS,SFF,KM,NA and BG made substantial contributions to conception, analysis, and interpretation of data, drafting the manuscript, and critical revision for important intellectual content. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study followed the ethical standards of the Declaration of Helsinki. And it was obtained the ethical approval from the Institutional Review Board (IRB) of the University of Gondar. All the study participants were well informed about the study by including an information sheet as part of the questionnaire. Study participants with the age of 18 and above were given a written informed consent and assent from those less than 18 years old along with written informed consent from their parents/ caregiver/guardians was obtained. The right to refuse or discontinue participation at any time, and the chance to ask anything about the study was given. The privacy and confidentiality of information were secured by not including any personal identifiers in the questionnaire. Students were also well informed that participate in the study or not participate will not give any special advantages or harm.
Consent for publication
Not applicable.
Competing interests
The authors declare no financial or another conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kassa, M.A., Srahbzu, M., Goshu Nenko et al. Suicidal ideation and attempts among high school students of war- affected area at Woldia town, Northeast, Ethiopia, 2022. BMC Psychiatry 23, 384 (2023). https://doi.org/10.1186/s12888-023-04889-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-023-04889-4