
Abstract
Backgrounds
Components of addiction (salience, tolerance, mood modification, relapse, withdrawal, and conflict) is the most cited theoretical framework for problematic social media use (PSMU). However, studies criticized its ability to distinguish problematic users from engaged users. We aimed to assess the association of the six criteria with depression, anxiety, and stress at a symptom level.
Methods
Ten thousand six hundred sixty-eight participants were recruited. Bergen Social Media Addiction Scale (BSMAS) was used to detect six addiction components in PSMU. We applied the depression-anxiety-stress scale to assess mental distress. Latent profile analysis (LPA) was conducted based on BSMAS items. Network analysis (NA) was performed to determine the symptom-symptom interaction of PSMU and mental distress.
Results
(1) Social media users were divided into five subgroups including occasional users (10.6%, n = 1127), regular users (31.0%, n = 3309), high engagement low risk users (10.4%, n = 1115), at-risk users (38.1%, n = 4070), and problematic users (9.8%, n = 1047); (2) PSMU and mental distress varied markedly across subgroups. Problematic users had the most severe PSMU, depression, anxiety, and stress symptoms. High engagement users scored high on tolerance and salience criteria of PSMU but displayed little mental distress; (3) NA showed conflict and mood modification was the bridge symptoms across the network, while salience and tolerance exhibited weak association with mental distress.
Conclusions
Salience and tolerance might not distinguish engaged users from problematic users. New frameworks and assessment tools focusing on the negative consequences of social media usage are needed.
Similar content being viewed by others


Background
With the rapid development of social media, problematic social media use (PSMU) has attracted increasing attention [1,2,3]. According to a recent meta-analysis, the global prevalence of PSMU in social media users is 17.42% [4]. While there is no universally accepted definition of PSMU, most researchers recognize it as excessive use of social media, which leads to negative consequences on the user’s functioning and psychological well-being [1].
Six addiction components of problematic social media use
The theoretical frameworks for PSMU remain undetermined. To date, the most cited theory for PSMU is the six components of addiction proposed by Griffiths, which also serves as the theoretical basis for most of the PSMU assessment tools [2, 5]. It conceptualizes PSMU as a combination of salience (spending a lot of time thinking about or planning to use social media), tolerance (need to spend an increased amount of time on social media), mood modification (using social media to forget about the emotional problem), relapse (failure in cutting down the social media usage), withdrawal (feeling troubled when unable to use social media), and conflict (negative impacts of excessive usage of social media on the user’s life) [6]. However, emerging studies suggest that the components of the addiction model might not be suitable for PSMU [1]. They criticize the ability of salience and tolerance criteria to distinguish problematic users from high engagement users, which might pathologize normal social media use [1]. For example, a recent study by Fournier et al. found that the six addiction components of PSMU failed to form a unitary construct [7]. They reported that salience and tolerance criteria showed no relationship with psychopathological symptoms, suggesting that these two criteria might be peripheral features of PSMU. Our previous study also demonstrates that salience and tolerance symptoms contribute little to PSMU according to the machine learning procedure [8].
Numerous studies report that PSMU exhibits substantial association with mental distress such as depression, anxiety, and impaired sleep [9,10,11,12,13,14]. However, the assessment of the relationship between PSMU and mental distress in previous studies has been predominantly limited to the use of total scores of measurement instruments (e.g., calculating total scores on six addiction components and interpreting the total score as the severity of PSMU). The potential heterogeneity of the symptoms might be obscured [15]. Describing the unique association between the six addiction components in PSMU and mental distress might help better understand their relationship and conceptualize PSMU.
Latent profile analysis and network analysis
Latent profile analysis (LPA) is a widely used, person-centered, categorical latent variable modeling approach [16]. LPA could identify latent subpopulations who shared similarities in a certain set of variables. In the case of PSMU, LPA allows for uncovering how social media users can be similarly “grouped” or “profiled” based on their PSMU symptoms and determining the similarities and differences across the profiles [17]. Network analysis (NA) is an emerging analysis tool for clarifying whether and how symptoms interact and reinforce one another [18]. In particular, NA offers a new angle on comorbidity by identifying the “bridge symptoms” across distinct psychiatric disorders [19, 20]. Both LPA and NA have been widely used in evaluating the association of mental distress with internet gaming disorder (IGD) or internet addiction [21,22,23,24]. However, studies on the PSMU via the two tools were very limited.
The present study
Hence, our study aimed to: (1) determine the subtypes of Chinese social media users based on their PSMU symptoms (i.e., six components of addiction in PSMU); (2) to evaluate the mental distress (depression, anxiety, and stress) across different subtypes; and (3) to assess the bridge symptoms which linked PSMU and mental distress.
Method
Participants and procedure
The present study is a part of a large project on mental health and changes in the usage of internet gaming [25], social media [26], alcohol [27], and tobacco [28] in the Chinese general population in the late stage of the COVID-19 pandemic. The online survey was conducted from May 2020 to August 2020. Participants across China were recruited through snowball sampling via social media such as WeChat. Participants completed the questionnaire on WenJuanXin (www.wjx.cn, the most popular online survey platform in China), and could only submit the questionnaire after responding to all questions. All participants aged over 18 were eligible for this study. Before the start of the survey, participants gave their informed consent. Ethical approval was obtained from the Ethics Committee of Sir Run Run Shaw hospital (NO. 20200505–33).
Measurements
Basic information including age, gender, education, occupation, partnership status, and residency were collected through self-designed questionnaire.
The changes in social media were assessed through self-reported questionnaires [26]. Participants were asked to recall their average time on social media (including but not limited to WeChat, QQ, Weibo, and TikTok) on weekdays and weekends both before and after the COVID-19 pandemic. Similar questionnaires were adapted in studies regarding the changes in internet use during the pandemic [29]. Weekly time on social media was calculated as (daily using time spent on a working day × 5) + (daily using time spent on a weekend day × 2).
We used the Bergen Social Media Addiction Scale (BSMAS) to assess PSMU, which has gained strong validity in the Chinese population [30, 31]. BSMAS is designed based on the components of addiction theory. It assesses the six addiction criteria including salience, tolerance, mood modification, relapse), withdrawal, and conflict of PSMU. BSMAS applied a 5-Likert scale and participants rated their frequency of symptoms ranging from 1 (very rarely) to 5 (very often). Higher scores indicated more severe PSMU. The Cronbach ‘s α of BSAMS was 0.862 in our study, suggesting its high internal consistency.
Depression, anxiety, and stress were assessed via the 21-item Depression-Anxiety-Stress Scale (DASS-21). It has three subscales and included 21 items. A 4-Likert scale ranging from 0 (Not at all) to 3 (Almost always) was used. The DASS-21 was widely used in the Chinese population and had gained strong validity [32]. The total scores of each subscale were calculated by multiplying the raw total scores by 2. The cutoff point of 14, 10, and 19 was used to screen for clinically relevant depression, anxiety, and stress symptoms. The Cronbach ‘s α of DASS-21, DASS-21 depression subscale, DASS-21 anxiety subscale, DASS-21 stress subscale was 0.956, 0.897, 0.876, and 0.887, respectively.
Statistical analysis
We presented the continuous data as the median and interquartile range (IRQ; 25–75%) and the categorical data as frequency and percentage. All the tests were 2-tailed with p < 0.05 implying statistically significant. All the statistical analysis was done in R (ver.4.2.0).
Latent profile analysis
We conducted the latent profile analysis (LPA) based on the scores of the items of the six components of BSMAS via the R package “tidyLPA”. We estimated the model with 2–5 latent profiles. The following metrics of each model were calculated: the Bayesian information criterion (BIC), Akaike’s information criterion (AIC), and entropy [8]. The model was selected based on previous guidelines [16]. Specifically, the following indicators were considered: (1) lower relative fit information criteria, which includes lower AIC and BIC, (2) high entropy of at least 0.8, and (3) the results of bootstrap likelihood ratio (BLRT). BLRT p-value less than 0.05 indicated a significant improvement in model fit when compared to the solution with one less class. We compared the inter-group differences in demographic information, social medial variables, and mental health through the Chi-square test and Wilcoxon rank-sum test. We further conducted a multivariate logistic regression to determine the correlates of each subgroup of social media users.
Network analysis
We estimated the network of PSMU, depression, anxiety, and stress symptoms via the EBICglasso model, which was widely used in psychological networks [33]. The R package “bootnet” and “qgraph” was used to estimate and visualize the network. In the network, each symptom was represented as a “node” and the unique association within the symptoms after controlling for other nodes in the network was represented as an “edge”. Thicker edges suggested a stronger association. Red and blue edges suggested positive and negative associations, respectively. We calculated the expected influence (EI) and bridge expected influence (BEI) to determine the central and bridge symptoms within the PSMU-Depression-Anxiety -Stress network [19]. Nodes with higher BEI were recognized as bridge symptoms that linked the PSMU community and the depression-anxiety-stress community. We used a case-dropping bootstrap approach to test the stability of BEI and EI [33]. The correlation stability coefficient (CS-C) represented the stability of the network. A CS-C higher than 0.5 was considered to be good. Nonparametric bootstrapping with 1000 bootstrap samples was performed to test the accuracy of the edges within the network.
Result
Sample Characteristics
A total of 11, 029 participants were recruited. After removing responses with a logic error such as abnormal age or daily social media use and responses which were submitted within 2 min or longer than one hour, 10, 668 validated responses were included in the final analysis (Table 1). The majority of the participants were female (6099, 57%), employed (8307, 78%), married (6378, 60%), had a bachelor’s degree (7167, 67%), and lived in the urban (8027, 75%). The median weekly social usage was 960 (420, 1680) minutes, and 3070 (29%) of the participants increased their social media usage by 3.5 h per week during the pandemic. The prevalence of clinically relevant depression, anxiety, and stress was 18%, 26%, and 10%, respectively.
Latent profile analysis
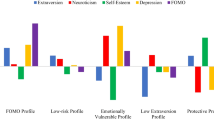
Table 2 describes the class solutions from 2 to 5, and a five-class model was considered the best fit. It has the lowest AIC and BIC and has good entropy. The LMR-LRT indicates that the five-class model was statistically greater than a four-class model. Figure 1 illustrated the five-class model of PSMU. The first class (“occasional user”) and the second class (“regular user”) contained 1127 (10.6%), and 3309 (31.0%) participants, respectively. They generally reported “very rarely” and “rarely” in all BSMAS items. Participants in class 3 were characterized by reporting “sometimes” in all BSMAS items, and thus class 3 (4070, 38.1%) was named the “at-risk user” group. Class 4, named the “high engagement low risk user” group, contained 1115 members who rated “often” in “salience” and “tolerance” symptoms but scored “rarely” in other items of BSMAS. 1047 participants were included in the fifth class, named “problematic user” groups. They scored highest on the BSMAS items as “often” or “very often”.

The five subgroups of social media users. X-axis represents the BSAMS items. Y-axis represents the scores of each BSAMS item
There was a significant difference in demographic characteristics, social media usage, and mental health conditions among the five classes. Participants in the problematic user class spent significantly more time on social media both before and during the pandemic and were at a much higher risk for depression (45%), anxiety (58%), and stress (35%) compared with the other four classes. In contrast, regular users and occasional users tended to spend less time on social media and scored lower in depression, anxiety, and stress.
Participants in the “high engagement low risk user” and “at-risk user” groups had similar weekly social media time, which was higher than that of “occasional user” and “regular user”. However, “at-risk users” members were more prone to depression (23% vs 8.9%), anxiety (33% vs 15%), and stress (12% vs 5.8%) than “High engagement low risk” members (all p < 0.05). Also, despite the high social media usage, “High engagement low risk” members were not at a higher risk for mental distress than “regular users” members.
Table 3 described the independent correlate of each subgroup identified by LPA. Compared to occasional user, anxiety and social media usage were significantly associated with all other four subgroups. Notably, problematic user was additionally related to age, education level, married status, depression, and stress. Age, gender, depression, and education level was independently associated with at-risk user.
Network analysis
We conducted the network analysis in the “problematic user” class and “at-risk user” class members, who were at a higher risk for PSMU, depression, anxiety, and stress. No items in BSMAS and DASS-21 were excluded for redundancy or low informativeness. Figure 2 illustrated the PSMU-Depression-Anxiety-Stress network, which had a density of 0.575 (202/351). The strongest edge within the network was BSMAS1 (Salience) and BSMAS2 (Tolerance), followed by DASS-17 (Self-deprecation) and DASS-21 (Devaluation of life). The centrality plot (Fig. 3a) suggested that DASS-11 (Agitated), DASS-15 (Panic), DASS-13 (Sad mood), and DASS-12 (Trouble relaxing) were the central symptoms of the PSMU-Depression-Anxiety-Stress network. BSMAS3 (Mood modification) exhibited the highest EI among PSMU symptoms. BSMAS6 (Conflict) was the bridge symptom that drove the comorbid mental symptoms and PSMU (Fig. 3b). It exhibited a substantial positive association with DASS-1 (Restlessness), DASS-5 (Inertia), and DASS-17 (Self-deprecation). Other bridge symptoms included BSMAS3 (Mood modification), DASS-1 (Restlessness), and BSMAS5 (Withdrawal). Of note, BSMAS2 (Tolerance) and BSMAS1 (Salience) displayed a very weak or negative association with depression, anxiety, and stress symptoms. The correlation matrix of BSMAS-DASS items were presented in Table S1.

The network analysis of PSMU, depression, anxiety, and stress in at-risk users and problematic users. Orange, blue, green, and yellow nodes represent PSMU, stress, anxiety, and depression symptoms, respectively. Blue and red edges indicate positive and negative associations. Thicker edges suggest stronger associations

The centrality plot and bridge expected influence plot of the network. a The X-rays represented the expected influence of each node. Nodes with higher expected influence have stronger impact in other nodes within the network. b The X-rays represented the bridge expected influence of each node. Nodes with higher bridge expected influence are recognized as bridge symptoms that drove the comorbid depression and anxiety symptoms
The network had excellent stability and accuracy. Figure S1 displayed the central and bridge stability of the network. The CS-C of both nodes and bridge expected influence was 0.75, which suggested the two indexes remained correlated with the original data (r = 0.75) after dropping out 75% of the data. The 95% CI of the estimated edges was narrow, indicating excellent accuracy of the network (Figure S2).
Discussion
In the present study, we assessed the relationship between six criteria of addiction in PSMU and mental distress via a person-centered and symptom-based approach among a large sample of Chinese social media users. The major findings included: (1) Based on their PSMU symptoms, social media users could be divided into five subgroups including occasional users, regular users, high engagement low risk users, at-risk users, and problematic users; (2) PSMU and mental distress symptoms varied markedly across the subgroups. Problematic users had the most severe PSMU, depression, anxiety, and stress symptoms. High engagement users scored high on tolerance and salience criteria of PSMU but displayed little mental distress; (3) network analysis showed conflict and mood modification was the bridge symptoms across the network, while salience and tolerance exhibited a rather weak association with mental distress. Taken together, our findings indicated that the tolerance and salience criteria of PSMU might not distinguish healthy users with high engagement from problematic users, which called for an updated framework of PSMU.
The 5-class model of social media users in the Chinese adult population perfectly replicated our previous findings in a large sample of Chinese college students [8], implying itself as a suitable classification for Chinese social media users. Almost half of the social media users were at high risk for PSMU, with 10% being problematic users and 38% being at-risk users. The prevalence of PSMU was highly variable in previous studies (range 3.5%-44.8%) [4, 8, 34, 35], which might result from the different study populations, measurement tools, and cutoff points. In line with previous studies [9,10,11, 34], problematic users spent more time on social media, scored higher in all PSMU symptoms, and had much higher levels of depression, anxiety, and stress. Hence, timely monitoring and intervention for PSMU are in urgent need.
Notably, we found a novel subgroup named high engagement low risk users, which was rarely reported in previous studies on internet addiction and IGD [24, 36,37,38]. They were characterized by a high level of salience and tolerance and scored low in other PSMU symptoms, which suggested that they were highly passionate social media users without suffering from the negative consequences of high social media usage. While their social media usage and BSMAS scores were higher than regular and occasional users, they didn’t exhibit worse depression, anxiety, and stress symptoms. This finding suggested the two criteria might be an indicator of high engagement in social media. Fournier et al. reported similar results with ours, finding that salience and tolerance were peripheral rather than central components of PSMU [7]. Studies in IGD also found that the two criteria had a low ability to distinguish normal and passionate users from problematic and addictive users [39,40,41,42,43]. Hence, a further theoretical framework for PSMU should focus more on the negative consequences of social media usage, which might help avoid pathologizing social media usage.
The NA provided new evidence about the relationship between PSMU and mental distress from a symptom perspective. In line with our LPA results, we found salience and tolerance exhibited a very weak association with mental distress, which was in accordance with that of Yue et al. in the association between internet addiction and depression symptoms [44]. Studies from other cultural backgrounds reported similar results. For example, a network analysis of PSMU and psychiatric symptoms in Italian social media users reported that salience and tolerance showed no relationship with psychiatric symptoms [7]. Cheng et al. also reported that these two symptoms displayed rather weak relationship with the depression in samples from the United Kingdom and the United States [34]. Our study suggested that conflict and mood modification were the bridge symptoms that drove the comorbidity of PSMU and mental distress. This finding supported two widely accepted conceptual frameworks in the association of problematic internet use and mental distress [30]. The first framework was the cognitive-behavioral model of pathological Internet use proposed by R.A. Davis, which suggested that mental distress was vital in the establishment of pathological internet use [45]. Users with mental distress tended to use the internet as a coping strategy and were more prone to problematic internet use. Another framework suggested that excessive internet use might contribute to mental distress due to disruption and impairment in real life [46]. While our study was cross-sectional and therefore could not identify the causal relationship between mental distress and PSMU, the NA indicated that both frameworks might be suitable for understanding their relationships. Restlessness (i.e., finding it hard to wind down) was another bridge symptom within the network, which exhibited a positive association with mood modification, relapse, conflict, and withdrawal symptoms. Further longitudinal studies are still warranted to confirm our findings.
While our studies provided novel insights into the relationship between PSMU and mental distress, there were several limitations. Firstly, the cross-sectional study design prohibited us from developing the causal relationship between PSMU and mental distress. Also, the data was collected during the COVID-19 pandemic. It is unclear whether and how the pandemic might affect our results. However, both the results of LPA and NA has successfully replicated previous studies prior to the pandemic [7, 8]. Hence, it is likely that the impact of the pandemic on our survey results might be modest. Further studies are needed to verify our findings. Secondly, the sample was collected via online may limit its representativeness of the Chinese population. However, this large sample size study recruited participants from 32 provinces in China, which enhances the generalizability of our findings; the demographic characteristics (such as age, sex ratio, education level, and employment status) [47, 48] and daily social media use [49] were similar to those of other large-scale representative studies in China. Moreover, the prevalence of PSMU in our sample was consistent with other epidemiological studies during the pandemic, indicating reasonable representativeness of our sample [50]. Another limitation was the application of self-reported questionnaire rather than a clinical interview. PSMU was assessed with one single scale, which might fail to cover several important dimensions of PSMU such as function impairment, displacement, and deception [5]. In addition, PSMU may reflect welfare problems through a proxy such as loneliness, which was not measured in our study [51, 52]. The association of salience and tolerance symptoms with these proxies remained unknown, which should be reminded in further studies.
Conclusion
Almost half of the social media users were at high risk for PSMU, who were more prone to depression, anxiety, and stress. Both LPA and NA suggested that tolerance and salience criteria exhibited a weak association with mental distress and might not distinguish healthy and engaged users from problematic users. Further theoretical frameworks and assessment tools for PSMU, which focus more on the negative consequences of PSMU, are needed to avoid the pathologization of normal usage of social media.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BSAMS:
-
Bergen Social Media Addiction Scale
- DASS-21:
-
21-Item Depression Anxiety Stress Scales
- PSMU:
-
Problematic social media usage
- LPA:
-
Latent profile analysis
- NA:
-
Network analysis
- BIC:
-
Bayesian information criterion
- AIC:
-
Akaike’s information criterion
- BLRT:
-
Bootstrap likelihood ratio
- EI:
-
Expected influence
- CS-C:
-
Correlation stability coefficient
- BEI:
-
Bridge expected influence
References
Cataldo I, Billieux J, Esposito G, Corazza O. Assessing problematic use of social media: where do we stand and what can be improved? Curr Opin Behav Sci. 2022;45:101145.
Sun Y, Zhang Y. A review of theories and models applied in studies of social media addiction and implications for future research. Addict Behav. 2021;114:106699.
SchouAndreassen C, Billieux J, Griffiths MD, Kuss DJ, Demetrovics Z, Mazzoni E, et al. The relationship between addictive use of social media and video games and symptoms of psychiatric disorders: a large-scale cross-sectional study. Psychol Addict Behav. 2016;30:252–62.
Meng SQ, Cheng JL, Li YY, Yang XQ, Zheng JW, Chang XW, et al. Global prevalence of digital addiction in general population: a systematic review and meta-analysis. Clin Psychol Rev. 2022;92:102128.
Varona MN, Muela A, Machimbarrena JM. Problematic use or addiction? A scoping review on conceptual and operational definitions of negative social networking sites use in adolescents. Addict Behav. 2022;134:107400.
Griffiths M. A ‘components’ model of addiction within a biopsychosocial framework. J Subst Use. 2005;10:191–7.
Fournier L, Schimmenti A, Musetti A, Boursier V, Flayelle M, Cataldo I, et al. Deconstructing the components model of addiction: an illustration through “addictive” use of social media. Addict Behav. 2023;143:107694.
Luo T, Qin L, Cheng L, Wang S, Zhu Z, Xu J, et al. Determination the cut-off point for the Bergen social media addiction (BSMAS): Diagnostic contribution of the six criteria of the components model of addiction for social media disorder. J Behav Addict. 2021;10:281–90.
Aydin O, Çökmüş FP, Balikçi K, Sücüllüoğlu-Dikici D, Ünal-Aydin P. The problematic use of social networking sites associates with elevated symptoms in patients with major depressive disorder. Int J Soc Psychiatry. 2020;66:496–503.
Hussain Z, Griffiths MD. Problematic social networking site use and comorbid psychiatric disorders: a systematic review of recent large-scale studies. Front Psychiatry. 2018;9:686.
Shannon H, Bush K, Villeneuve PJ, Hellemans KG, Guimond S. Problematic social media use in adolescents and young adults: systematic review and meta-analysis. JMIR Ment Health. 2022;9:e33450.
Zhang W, Pu J, He R, Yu M, Xu L, He X, et al. Demographic characteristics, family environment and psychosocial factors affecting internet addiction in Chinese adolescents. J Affect Disord. 2022;315:130–8.
Hjetland GJ, Skogen JC, Hysing M, Sivertsen B. The association between self-reported screen time, social media addiction, and sleep among Norwegian University students. Front Public Health. 2021;9:794307.
Lopes LS, Valentini JP, Monteiro TH, Costacurta MC de F, Soares LON, Telfar-Barnard L, et al. Problematic social media use and its relationship with depression or anxiety: a systematic review. Cyberpsychol Behav Soc Netw. 2022. https://doi.org/10.1089/cyber.2021.0300.
Fried EI, Nesse RM. Depression sum-scores don’t add up: why analyzing specific depression symptoms is essential. BMC Med. 2015;13:72.
Spurk D, Hirschi A, Wang M, Valero D, Kauffeld S. Latent profile analysis: a review and “how to” guide of its application within vocational behavior research. J Vocat Behav. 2020;120:103445.
Howard MC, Hoffman ME. Variable-centered, person-centered, and person-specific approaches: where theory meets the method. Organ Res Methods. 2018;21:846–76.
Hevey D. Network analysis: a brief overview and tutorial. Health Psychol Behav Med. 2018;6:301–28.
Jones PJ, Ma R, McNally RJ. Bridge Centrality: A Network Approach to Understanding Comorbidity. Multivar Behav Res. 2021;56:353–67.
Fonseca-Pedrero E. Network analysis: a new way of understanding psychopathology? Revista de Psiquiatría y Salud Mental (English Edition). 2017;10:206–15.
Cai H, Bai W, Sha S, Zhang L, Chow IHI, Lei S-M, et al. Identification of central symptoms in Internet addictions and depression among adolescents in Macau: a network analysis. J Affect Disord. 2022;302:415–23.
Cai H, Xi H-T, An F, Wang Z, Han L, Liu S, et al. The association between internet addiction and anxiety in nursing students: a network analysis. Front Psychiatry. 2021;12:723355.
Cerniglia L, Griffiths MD, Cimino S, De Palo V, Monacis L, Sinatra M, et al. A latent profile approach for the study of internet gaming disorder, social media addiction, and psychopathology in a normative sample of adolescents. Psychol Res Behav Manag. 2019;12:651–9.
Kim D, Lee J, Nam JK. Latent profile of internet and internet game usage among South Korean adolescents during the COVID-19 Pandemic. Front Psychiatry. 2021;12:714301.
Wu Q, Luo T, Tang J, Wang Y, Wu Z, Liu Y, et al. Gaming in China Before the COVID-19 Pandemic and After the Lifting of Lockdowns: a Nationwide Online Retrospective Survey. Int J Ment Health Addict. 2022:1–13. https://doi.org/10.1007/s11469-022-00792-3.
Luo T, Chen W, Liao Y. Social media use in China before and during COVID-19: preliminary results from an online retrospective survey. J Psychiatr Res. 2021;140:35–8.
Wang Y, Lu H, Hu M, Wu S, Chen J, Wang L, et al. Alcohol consumption in China before and during COVID-19: preliminary results from an online retrospective survey. Front Psychiatry. 2020;11:597826.
Liao Y, Tang J, Quah ACK, Fong GT, McNeill A. Attitudes towards smoking and COVID-19, and changes in smoking behaviors before and after the outbreak of COVID-19: a nationwide cross-sectional survey study in China. Tob Induc Dis. 2022;20:18.
Higuchi S, Mihara S, Kitayuguchi T, Miyakoshi H, Ooi M, Maezono M, et al. Prolonged use of Internet and gaming among treatment seekers arising out of social restrictions related to COVID-19 pandemic. Psychiatry Clin Neurosci. 2020;74:607–8.
Chang CW, Huang RY, Strong C, Lin YC, Tsai MC, Chen IH, et al. Reciprocal relationships between problematic social media use, problematic gaming, and psychological distress among university students: a 9-month longitudinal study. Front Public Health. 2022;10:858482.
Yue H, Zhang X, Cheng X, Liu B, Bao H. Measurement invariance of the bergen social media addiction scale across genders. Front Psychol. 2022;13:879259.
Zhang Z, Wang T, Kuang J, Herold F, Ludyga S, Li J, et al. The roles of exercise tolerance and resilience in the effect of physical activity on emotional states among college students. Int J Clin Health Psychol. 2022;22:100312.
Epskamp S, Borsboom D, Fried EI. Estimating psychological networks and their accuracy: a tutorial paper. Behav Res. 2018;50:195–212.
Cheng C, Ebrahimi OV, Luk JW. Heterogeneity of prevalence of social media addiction across multiple classification schemes: latent profile analysis. J Med Internet Res. 2022;24:e27000.
Tang CSK, Wu AMS, Yan ECW, Ko JHC, Kwon JH, Yogo M, et al. Relative risks of Internet-related addictions and mood disturbances among college students: a 7-country/region comparison. Public Health. 2018;165:16–25.
Chen J, Liu J, Zhao G, Kong F. Internet behavior preferences predict pathological internet use: a latent profile analysis. Front Psychol. 2021;12:644623.
Zhang Y, Liu Z, Zhao Y. Impulsivity, social support and depression are associated with latent profiles of internet addiction among male college freshmen. Front Psychiatry. 2021;12:642914.
Shu MY, Ivan Jacob AP, Meng Xuan Z, Anise MSW. Psychometric validation of the internet gaming disorder-20 test among Chinese middle school and university students. J Behav Addict. 2019;8:295–305.
Kardefelt-Winther D, Heeren A, Schimmenti A, van Rooij A, Maurage P, Carras M, et al. How can we conceptualize behavioural addiction without pathologizing common behaviours? Addiction. 2017;112:1709–15.
Starcevic V. Internet gaming disorder: Inadequate diagnostic criteria wrapped in a constraining conceptual model. J Behav Addict. 2017;6:110–3.
Kardefelt-Winther D. Meeting the unique challenges of assessing internet gaming disorder. Addiction. 2014;109:1568–70.
Charlton JP, Danforth IDW. Distinguishing addiction and high engagement in the context of online game playing. Comput Hum Behav. 2007;23:1531–48.
Luo T, Wei D, Guo J, Hu M, Chao X, Sun Y, et al. Diagnostic contribution of the DSM-5 criteria for internet gaming disorder. Front Psychiatry. 2022;12:777397.
Zhao Y, Qu D, Chen S, Chi X. Network analysis of internet addiction and depression among Chinese college students during the COVID-19 pandemic: a longitudinal study. Comput Human Behav. 2023;138:107424.
Davis RA. A cognitive-behavioral model of pathological Internet use. Comput Hum Behav. 2001;17:187–95.
Andreassen CS. Online social network site addiction: a comprehensive review. Curr Addict Rep. 2015;2:175–84.
Lu ZA, Shi L, Que JY, Zheng YB, Wang QW, Liu WJ, et al. Long-term psychological profile of general population following COVID-19 outbreak: symptom trajectories and evolution of psychopathological network. Epidemiol Psychiatr Sci. 2022;31:e69.
Shi L, Lu ZA, Que JY, Huang XL, Liu L, Ran MS, et al. Prevalence of and risk factors associated with mental health symptoms among the general population in China during the coronavirus disease 2019 pandemic. JAMA Netw Open. 2020;3:e2014053.
Zhong B, Jiang Z, Xie W, Qin X. Association of social media use with mental health conditions of nonpatients during the COVID-19 outbreak: insights from a national survey study. J Med Internet Res. 2020;22:e23696.
Alimoradi Z, Lotfi A, Lin CY, Griffiths MD, Pakpour AH. Estimation of behavioral addiction prevalence during COVID-19 pandemic: a systematic review and meta-analysis. Curr Addict Rep. 2022;9:486–517.
Huang C. A meta-analysis of the problematic social media use and mental health. Int J Soc Psychiatry. 2022;68:12–33.
Moretta T, Buodo G. Problematic internet use and loneliness: how complex is the relationship? A short literature review. Curr Addict Rep. 2020;7:125–36.
Acknowledgements
We show the greatest attitudes to all the participants and volunteers who helped deliver the online questionnaires.
Funding
This study was supported by the STI 2030—Major Projects—"Brain Science and Brain-like Research" Project (Grant No. 2022ZD0211200 to Yanhui Liao). The funders had no role in study design, data collection, and analysis, writing the manuscript, or the decision to submit the paper for publication.
Author information
Authors and Affiliations
Contributions
Yanhui Liao contributed to all aspects of the study. Pu Peng contributed to the analysis and interpretation of data, statistical analysis, and the drafting of the manuscript. All authors have approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study procedures were carried out in accordance with the Declaration of Helsinki. Ethical approval was obtained from the Ethics Committee of Sir Run Run Shaw hospital (NO. 20200505–33). Before the start of the survey, participants gave informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary Figure 1.
The stability of the network. Supplementary Figure 2. The accuracy of the edges estimated.
Additional file 2: Supplementary Table 1.
Correlation matrix of BSMAS and DASS-21 items.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Peng, P., Liao, Y. Six addiction components of problematic social media use in relation to depression, anxiety, and stress symptoms: a latent profile analysis and network analysis. BMC Psychiatry 23, 321 (2023). https://doi.org/10.1186/s12888-023-04837-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-023-04837-2