
Abstract
Background
This study was designed and conducted to determine the status of depression literacy (D-Lit) and its relationship with the quality of life across the Iranian population.
Methods
This cross-sectional study was conducted in 2020 among 1382 participating from the general population in Gonabad, Iran. Participants were selected and recruited using a multistage sampling method. Data were collected using three sets of questionnaires (demographic section, D-Lit scale, and quality of life questionnaire). Data were analyzed by SPSS software version 24 and using independent samples t- test, Chi-square test, One-way ANOVA, and Pearson correlation.
Results
Based on the results, the mean (± standard deviation) of D-Lit and quality of life were 44.14 (± 4.69) and 35.81 (± 5.17), respectively. Based on the results of Pearson correlation coefficient, there was a significant positive correlation between D-Lit and quality of life (r = 0.104, p < 0.001). D-Lit was significantly higher in those who reported having consulted with a psychiatrist compared with those who did not (p < 0.001). Participants with a family history of mental illness and those whose family members were referred to a psychologist for psychological issues had significantly higher levels of D-Lit than others (p < 0.001).
Conclusion
Based on the results of this study, some D-Lit projects should be improved. Also, the results revealed that D-Lit is a potential factor that can affect people's mental health status and enhance their quality of life. Therefore, it is necessary to develop appropriate educational programs to enhance D-Lit in the community and ultimately improve the quality of life in the community by reducing mental illness.
Similar content being viewed by others


Background
Depression literacy (D-Lit) is a special type of mental health literacy and is defined as the ability to recognize depression as well as make informed decisions about treatment [1]. The results of a study in Iran showed that the state of mental health literacy in the general population is not enough [2]. A study in Iran showed that D-Lit was low, with 48.5% of participants failing to identify mental disorders and 47.5% not intending to help search [3]. Higher D-Lit is associated with appropriate help [4], and adequate D-Lit can improve prevention, early detection, intervention, and prognosis of depression [5].
Depression is one of the top four causes of disability globally [6], and by 2030, depression will be the leading cause of the world's disease burden [7]. It is a common, chronic, recurrent, and treatable disorder associated with illness and death [8]. Depression is characterized by disturbed mood, lack of happiness, sleep problems, weight changes, feelings of guilt, inattention, daily dysfunction, and in severe cases, suicide [9,10,11].
Depression is associated with decreased of quality of life and can have a significant impact on the quality of life [8, 12]. The World Health Organization defines the quality of life as “an individual's perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns” [13]. Thus, the quality of life is a subjective and multidimensional issue and related to people's understanding of various aspects of life [14]. Quality of life can predict the extent and impact of illness, injury, disability, and assess community mental health [15]. Various studies have examined factors associated with quality of life [16,17,18,19,20], but these studies have not investigated various aspects of D-Lit and quality of life. Therefore, this study aimed to determine the status of D-Lit and its relationship with the quality of life of the Iranian population.
Methods
This cross-sectional study was conducted in 2020 among 1382 participating from the general population in Gonabad, Iran (Gonabad is one of the cities in Khorasan Razavi province in eastern Iran).
Sample size
Based on a similar study [21], the sample size of this study was considered to be 1382 participants (0.95% confidence level, D-Lit rate/ p = 0.53, accuracy/d = 0.03, 25% of sample loss).
Sampling method
The multi-stage sampling method was used to select and include the participants. In the first stage, proportional stratified sampling is used, and in the second stage, a simple random sampling method is used. In the proportional stratified sampling method, all health centers (n = 3) with their population were identified and then each center was considered as a stratum. In the next step, the required sample size was selected from each center by simple random sampling from among those willing to participate in the study and who met the inclusion criteria for entry into the study. In the end, 553 people in the No. 1 health center, 525 people in the No. 2 health center, and 304 people in the health center. No. 3 entered the study. It should be noted that health centers are different from medical centers in Iran. The most important purpose of these centers is to provide primary health care services to all target populations, usually to people of all age groups.
To collect the data, the questioners referred to the health center, and after explaining the purpose of the study to the participants, the questionnaire was provided and completed by self-report. Also, questionnaires for illiterate participants were completed by questioners who were not part of the research team. In this study, inclusion criteria were e.g. participants residing in Gonabad, age 18 years and older, no specific medical conditions, and signed informed consent.
Data Collection Instruments
Data were collected using three sets of questionnaires, including a demographic questionnaire, a D-Lit questionnaire, and a quality of life questionnaire (SF-12).
-
1) Demographic questionnaire: In this section, data were collected on sex, job status, marital status, age group, income, education level, participants consulted psychologist / psychiatrist for psychological issues, family history of mental illness, obtain information related to mental illness, and refer your family member to a psychologist/psychiatrist for psychological issues.
-
2) D-Lit Questionnaire: This questionnaire was designed and confirmed by Griffiths et al. and includes 22 items that survey the status of D-Lit [22, 23]. These items are assessed on a three-point scale (true, false, I don't know) with a score range of 22 to 66. For each correct answer, a score is assigned, with higher scores indicating better D-Lit status. Based on the results of Griffiths study, Cronbach's alpha and 3 month test–retest were reported 0.70 and 0.71, respectively [22]. The validity and reliability of the Persian version of the D-Lit questionnaire was investigated in the Tehrani study [24]. Based on exploratory factor analysis, 5 factors with eigenvalues greater than 1 were extracted, accounting for 56.30% of the variance (F1: Knowledge of the psychological symptoms, F2: Knowledge about the effectiveness of available treatment methods, F3: Knowledge about cognitive-behavioral symptoms, F4: Knowledge about taking medications and their side effects, and F5: Knowledge of severity of disease) [24]. In the confirmatory factor analysis, these five factors were examined, 1 question was removed and the final questionnaire was confirmed with 21 items with a score range of 21 to 63. Finally, Cronbach's alpha coefficient for the all items was 0.890 [24].
-
3) Quality of life questionnaire (SF-12): This tool was designed by Ware and Keller [25]. This questionnaire is a shortened version of quality of life with 8 subscales and contains 12 items [25]. This instrument examines the quality of life in terms of role limitations due to physical problems (RP-2 questions), bodily pain (BP-1 question), physical functioning (PF-2 questions), role limitations due to emotional problems (RE-2 questions), general health (GH-1 questions), social functioning (SF-1 question), vitality (VT-1 question), and perceived mental health (MH-2 questions). These 8 variables are divided into two subscales of Physical Health with 6 items (RF, RP, BP, GH), and Mental Health with 6 items (SF, RE, VT, MH). The validity and reliability of the Persian version of this questionnaire was confirmed by Montazeri et al. and Cronbach's alpha for subscales of Physical Health and Mental Health were 0.73 and 0.72, respectively [26].
Statistical analysis
This study was performed using software version 22. Independent samples t-test, Chi-square test, One-way ANOVA, and Pearson correlation test have been used for data analysis. In this study, for data analysis, a significance level of less than 0.05 was considered.
Results
In this study, the majority of participants were female (n = 781, 56.9%), 79.1% (n = 1009,) lived in urban, 67.6% (n = 922) were in the age group of 18 to 35 years, and 69.1% (n = 942) were married. The majority of them (n = 858, 64.8%) had an academic level of education and 65.9% of them (n = 850) had medium income. In terms of job status, 33.9% (n = 444) were laborers and 30% (n = 393) were employed. In this study, only 15.5% (n = 210) of participants stated that they had referred to a psychologist for psychological issues, 14.5% (n = 198) reported that there was a history of mental illness among their family members, and 18.4% (n = 245) also stated that some of their family members had a history of referred to a psychologist. The majority of participants (n = 1061, 77.3%) reported that they received information about mental disorders.
According to the results of Table 1, there was a significant relationship between sex and D-Lit and women had higher level of D-Lit (p < 0.001). Also, 63.7% of women answered most of the questions correctly (p < 0.001). The results showed a significant relationship between age groups and D-Lit levels (p < 0.001). The level of education of the study participants was significantly related to their level of D-Lit, and people with a higher education level had a higher level of D-Lit (p < 0.001). Also, 65% of participants who had an academic level were able to answer most of the questions correctly (p < 0.001) (Table 1).
The participants who reported having consulted with psychologist for their psychological issues had significantly higher levels of D-Lit compared with those who did not (p < 0.001). Participants with a family history of mental illness and those whose family members were referred to a psychologist for psychological issues had significantly higher levels of D-Lit than others (p < 0.001). Also, the participants who obtained information related to mental disorders showed significantly higher levels of D-Lit than those who did not (p < 0.001). There was no significant relationship between financial status and D-Lit, but people with better financial status had higher D-Lit scores (p > 0.05) (Table 1).
The results of Table 1 showed the status of participants' answers to the D-Lit questionnaire. Based on the results, 37.8% (n = 522) were able to answer 1 to 7 questions correctly, 55.4% (n = 765) were able to answer 8 to 14 questions correctly, and only 3.9% (n = 54) were able to answer 15 and more questions correctly. Of the participants, only 3% (n = 41) of the participants did not have D-Lit and answered all the questions incorrectly. The results of this study showed that the majority of people who answered the D-Lit questions incorrectly were male (n = 25), laborer (n = 15), married (n = 26), aged 18–35 (n = 28), had high school education (n = 19), and had moderate financial status (n = 21). More information can be seen in Table 1.
In this study, 23.7% (n = 327) answered all questions on knowledge of psychological symptoms subscale, 0.4% (n = 5) answered all questions on knowledge about the available effectiveness of treatment methods subscale, 3.1% (n = 43) answered all questions on knowledge about cognitive-behavioral symptoms subscale, 5.2% (n = 71) answered all questions on knowledge about taking medications and their side effects subscale, and 15.5% (n = 214) answered all questions on knowledge of severity of disease subscale (Table 2).
Based on the results of Table 3, the mean (± SD) of D-Lit and quality of life were 44.14 (± 4.69) and 35.81 (± 5.17), respectively. The mean (± SD) D-Lit subscales and quality of life are shown in Table 3. Based on the results of Pearson correlation coefficient, there was a significant positive correlation between D-Lit and quality of life (r = 0.104, p < 0.001) (Table 4).
Discussion
This study aimed to determine the status of D-Lit and its relationship with the quality of life of the Iranian population. According to the results of this study, most of the participants did not have an adequate level of D-Lit and only a small number had an adequate level of D-Lit. The results of this study was similar with other studies [11, 27, 28]. The results of Bernstein's study showed that participants answered correctly 41.73% of the questions [29]. Results from another study showed that participants answered 52.8% of the questions [21].
The results of this study also showed that there was a significant positive correlation between D-Lit and participants' quality of life. With the development of medical technology and the improvement of life expectancy, people are paying more and more attention to their quality of life. Health managers and researchers are more concerned about whether improving D-Lit improves people's quality of life [30]. We found in our study that people with low of D-Lit had a low quality of life. This suggests that people with low D-Lit may be less concerned about their health and thus have unhealthy behaviors that reduce their quality of life. Evidence supports a significant longitudinal relationship between literacy skills and depressive symptoms and that people with low health literacy are three times more likely to suffer from depression [31]. Health skills and D-Lit refer to an individual's ability to translate mental health knowledge into healthy behaviors.
Based on the results of this study, there was a significant relationship between sex and D-Lit, with women having significantly higher levels of D-Lit than men. The results of various studies have also indicated that women have a higher level of D-Lit than men [32, 33], are more able to diagnose mental disorders [34, 35], and are more likely than men to seek occupational mental health services [36]. In addition, women tend to learn more about mental health and are more likely to interact with people with mental disorders [37, 38]. This sex difference may be related to the lower prevalence of depression in men and thus their lack of exposure to disorder. However, this lack of awareness may also cause fewer men seeking depression. Men also attribute depression primarily to weak personality and believe in the use of alcohol for relaxation [39, 40]. Men may need to be targeted as a way to improve their mental health literacy for increasing the proper amount of support.
The findings of this study also showed a significant relationship between age groups and D-Lit levels, with D-Lit rates higher in the 18- to 35-year-old age group than in other age groups. These findings are consistent with previous studies showing that older populations have poorer D-Lit [41, 42]. Poor D-Lit among older adults may be due to a variety of reasons. Mental health information may be provided through media that are less commonly used by older adults, such as the Internet. School curricula are a major source of mental health literacy for young people, but such programs have not been systematically available in recent decades. Current mental health literacy campaigns may not target the elderly. Social stigma may also be higher in older adults and prevent them from receiving information about mental health literacy [43].
Based on the results of this study, there was a significant relationship between participants' education level and their D-Lit and with increasing education level, D-Lit level also increases. Previous research has shown that people with higher education are more likely to be diagnosed with depression than people with less education [44]. At the same time, according to previous research, with the improvement of education level, the quality of life will be significantly improved in both physical and psychological dimensions. [45]. Education and area of residence appear to be significant predictors of a depression diagnosis, and people living in cities also had more Knowledge of depression [46]. Today, many villages have access to mass media (television, radio, and the Internet). Therefore, the media must provide programming in local languages to raise public awareness of mental health issues and reduce false beliefs and negative attitudes towards mental disorders.
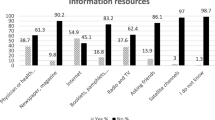
In this study, those who reported seeing a psychologist for their psychological issues had significantly D-Lit levels than those who didn't. Also, participants who mentioned that had a family history of mental illness, and those whose family members were referred to a psychologist for psychological issues, showed significantly higher levels of D-Lit than others. Based on the results of this study, people who received information about mental disorders from various sources showed significantly higher levels of D-Lit than others. It is important to note that people often obtain mental health information from a variety of sources, which may not be reliable.; Therefore, it should be emphasized that psychologists, psychiatrists, and healthcare providers are the best sources of mental health information from which individuals should obtain reliable information [47].
People prefer to seek help from less formal sources such as the family for mental health problems [48]. Studies have shown that the most common source of help for people about health treatment is talking to family or friends [49, 50]. Seeking appropriate help from professional sources is very important for the prevention, early diagnosis, and treatment as well as recovery of mental disorders, and timely referral to these sources is essential [50, 51]. Asking less for help from a psychiatrist or psychologist may indicate poor knowledge of psychiatric services or a lack of understanding of the effective treatments offered by such specialists. Also, in another study, although many participants rated the services of psychiatrists and counselors as likely to be helpful, less than 10% of the population endorsed psychiatrists as the best help for a person with depression [40]. General practitioners or family physicians topped the list, indicating the fact that most people with depression are often seen and treated by general practitioners [40]. Behaviors of people and patients may also be influenced by culture and religion, which play an important role in mental health literacy and D-Lit [46]. In response to cultural factors, individuals may be reluctant to raise their mental health concerns with mental health professionals and psychologists. Therefore, they may decide to trust their family or friends. Also, the social stigma that manifests itself in prejudice, mistrust, stereotyping, fear, embarrassment, anger, and avoidance [52] may be another deterrent and an obstacle to utilizing services in Asian societies.
This study had some strengths and limitations. This has been a population-based study, and the use of a standard and valid assessment tool (D-Lit) has minimized some measurement bias for exposure and outcome variables. Also, this study had a good sample size. Some possible limitations have also been identified in this study. This cross-sectional study can be considered as an appropriate blueprint for discovering potential risk factors for a disease. However, the evidence presented in this study can only showed an association and is not sufficient to show a temporal relationship between exposure and outcome. This study can be considered as an exploratory study to identify a potential link between D-Lit and quality of life. Meanwhile, some important risk factors for depression, such as recent life stressors and family problems, have not been included in the analysis as potential distortions, and this may lead to biased estimation of the strength of the relationship between exposure and outcome variables. Future studies can be conducted with a better design, such as a longitudinal cohort study, and include potentially important confounding factors to determine the cause of the relationship. Also, since the questionnaires for illiterate participants were filled out by the questioners, there may be some errors in the information collected.
Conclusion
The purpose of this study was to investigate the relationship between D-Lit and quality of life. The results revealed that D-Lit is a potential factor that can affect people's mental health status and enhance their quality of life. Increasing the level of D-Lit should be considered as an important preventive strategy for the mental problems of the community. Also, it is necessary to develop appropriate educational programs to enhance D-Lit in the community and ultimately improve the quality of life in the community by reducing mental illness. Mental health education can be provided in patient-physician communication, in training campaigns and programs such as first aid mental health skills training. Dissemination of information about evidence-based therapies should be considered in clinical practice, as well as in promotion and training programs. Also, further research on self-help for depression is needed. Such efforts should focus not only on diagnosing symptoms but also on disseminating information on risk factors, evidence-based therapies on risk factors, and depression factors.
Availability of data and materials
All data generated or analysed during this study are included in this published article.
Abbreviations
- D-Lit:
-
Depression literacy
- SF-12:
-
The 12-item Short Form Health Survey
- RP:
-
Role limitations due to physical problems
- PF:
-
Physical Functioning
- GH:
-
General Health
- BP:
-
Bodily Pain
- SF:
-
Social Functioning
- VT:
-
Vitality; MH: Mental Health
- RE:
-
Role limitations due to emotional problems
References
Wang JACFG, Lai D, Evans B, Perry BW, et al. Depression literacy in Alberta: findings from a general population sample. Can J Psychiatry. 2007;52(7):442–9.
Noroozi AKF, Lari H, Tahmasebi R. The mediator role of mental health literacy in the relationship between demographic variables and health-promoting behaviours. Iran J Psychiatry Behav Sci. 2018;12(2):e12603.
Ghadirian L, Sayarifard A. Depression literacy in urban and suburban residents of Tehran, the Capital of Iran; recognition, help seeking and stigmatizing attitude and the predicting factors. Int J Prev Med. 2019;10:134.
Wright AJAHM, McGorry PD. What’s in a name?Is accurate recognition and labeling of mental disorders by young people associated with better help-seeking and treatment preferences? Psychiatry Psychiatr Epidemiol. 2007;42(3):244–50.
Singh S, Zaki RA, Farid NDN. A systematic review of depression literacy: knowledge, help-seeking and stigmatising attitudes among adolescents. J Adolesc. 2019;74:154–72.
Arafat SY, Shams SF, Chowdhury MHR, Chowdhury EZ, Hoque MB, Bari MA. Adaptation and validation of the Bangla version of the depression literacy questionnaire. J Psychiatry. 2017;20(4):412.
Organization WH. The global burden of disease: 2004 update. Accessed http://www.who.int/healthinfo/global_burden_disease/2004_report_update/ 2008.
Arafat SY, Ahmed S, Uddin S. Depression literacy status in Bangladesh: a cross-sectional comparative observation. J Behav Health. 2018;7(2):91–7.
Disu T, Anne N, Griffiths M. Risk factors of geriatric depression among elderly Bangladeshi people: a pilot interview study. Asian J Psychiatr. 2019;44:163–9.
Mamun M, Huq Z, et al. Prevalence of depression among Bangladeshi village women subsequent to a natural disaster: a pilot study. Psychiatry Res. 2019;276:124–8.
Mamun MA, Naher S, Moonajilin MS, Jobayar AM, Rayhan I, Kircaburun K, Griffiths MDJH. Depression literacy and awareness programs among Bangladeshi students: an online survey. Heliyon. 2020;6(9):e04901.
Lima M, Foulce T. Over general autobiographical memory at baseline predicts depressive symptoms at follow-up in patients with firstepisode depression. Psychiatry Res. 2014;243:123–7.
Hagerty MR, Cummins R, Ferriss AL, Land K, Michalos AC, Peterson M, Sharpe A, Sirgy J, Vogel J. Quality of life indexes for national policy: Review and agenda for research. Soc Indic Res. 2001;71(1):58–78.
Nejat S. Quality of Life and its Measurement. Iran J Epidemiol. 2008;4(2):57–62.
Ogundare OM, Shah VG, Salunke SR, et al. Fifteen Dimensions of Health and their Associations with Quality of Life among Elderly in Rural Villages in Maharashtra, (India). Indian J Gerontol. 2017;31(1):12–21.
Ahmadzadeh K, Farshidi H, Nikparvar M, Ezati-Rad R, Mahmoodi M. The Relationship Between Health Literacy Level and Quality of Life in Heart Failure Patients. J Health Lit. 2021;6(2):61–8.
Kooshiar H, Shoorvazi M, Dalir Z, Hosseini M. Health Literacy and Health-Related Quality of Life in Older Adults with Type 2 Diabetes: The Mediating Role of Treatment Regimen Adherence. J Health Lit. 2021;5(4):31–40.
Zarezadeh Y, Eskandari N, Moradi M, Abdi N. The Relationship between Health Literacy and Quality of Life of Employees in Campus of Kurdistan University of Medical Sciences. J Health Lit. 2020;4(4):38–45.
Kamalinedjad F, Rafiepoor A, Sabet M. Structural Equation Modeling Relationship of the between Coping Strategies with Quality of Life by mediating Lifestyle in Cardiovascular Patients. Iran J Health Educ Health Promot. 2020;8(4):348–58.
AbbasalizadFarhangi M, Dehghan P, Jahangiry L. Mental health problems in relation to eating behavior patterns, nutrient intakes and health related quality of life among Iranian female adolescents. PLoS One. 2018;13(4):e0195669.
Kheirabadi D, Kheirabadi GR, Tarrahi M. Depression literacy and the related factors among a group of hospitals’ staff in Iran. Int J Soc Psychiatry. 2020;67:20764020954886.
Griffiths KM, Christensen H, Jorm AF, Evans K, Groves C. Effect of web-based depression literacy and cognitive–behavioural therapy interventions on stigmatising attitudes to depression: Randomised controlled trial. Br J Psychiatry. 2004;185(4):342–9.
Gulliver A, Griffiths KM, Christensen H, Mackinnon A, Calear AL, Parsons A, Bennett K, Batterham PJ, Stanimirovic R. Internet-based interventions to promote mental health help-seeking in elite athletes: an exploratory randomized controlled trial. J Med Internet Res. 2012;14(3):e69.
Tehrani H, Nejatian M, Moshki M, Jafari A. Psychometric properties of Persian version of depression literacy (D-Lit) questionnaire among general population. Int J Ment Heal Syst. 2022;16(1):40.
Ware JE Jr, Kosinski M, Keller SD. A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34(3):220–33.
Montazeri A, Vahdaninia M, Mousavi SJ, Omidvari S. The Iranian version of 12-item Short Form Health Survey (SF-12): factor structure, internal consistency and construct validity. BMC Public Health. 2009;9(1):341.
Ho GWK, Bressington D, Leung SF, Lam KKC, Leung AYM, Molassiotis A, Ligot J, Ranoco C, Sophal C, Valimaki M. Depression literacy and health-seeking attitudes in the Western Pacific region: a mixed-methods study. Soc Psychiatry Psychiatr Epidemiol. 2018;53(10):1039–49.
Loureiro LM, Jorm AF, Mendes AC, Santos JC, Ferreira RO, Pedreiro AT. Mental health literacy about depression: a survey of portuguese youth. BMC Psychiatry. 2013;13:129.
Bernstein K, Han S, Park CG, Lee Y-M, Hong O. Evaluation of Health Literacy and Depression Literacy Among Korean Americans. Health Educ Behav. 2020;47(3):457–67.
Berkman ND, Sheridan SL, Donahue KE, Halpern DJ, Crotty K. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. 2011;155(2):97–107.
Gazmararian J, Baker D, Parker R, Blazer DG. A multivariate analysis of factors associated with depression: evaluating the role of health literacy as a potential contributor. Arch Intern Med. 2000;160(21):3307–14.
Dias P, Campos L, Almeida H, Palha F. Mental health literacy in young adults: adaptation and psychometric properties of the mental health literacy questionnaire. Int J Environ Res Public Health. 2018;15(7):1318.
Martínez-Zambrano F, García-Morales E, García-Franco M, Miguel J, Villellas R, Pascual G, Arenas O, Ochoa S. Intervention for reducing stigma: assessing the influence of gender and knowledge. World J Psychiatry. 2013;3(2):18.
Ghadirian L, Sayarifard A. Depression literacy in urban and suburban residents of Tehran, the capital of Iran; recognition, help seeking and stigmatizing attitude and the predicting factors. Int J Prev Med. 2019;10:134.
Picco L, Seow E, Chua BY, Mahendran R, Verma S, Chong SA, Subramaniam M. Recognition of mental disorders: findings from a cross-sectional study among medical students in Singapore. BMJ Open. 2017;7(12):e019038.
Yu Y, Liu ZW, Hu M, Liu HM, Yang JP, Zhou L, Xiao SY. Mental health help-seeking intentions and preferences of rural Chinese adults. PloS One. 2015;10(11):e0141889.
Rong Y, Glozier N, Luscombe GM, Davenport TA, Huang Y, Hickie IB. Improving knowledge and attitudes towards depression: a controlled trial among Chinese medical students. BMC Psychiatry. 2011;11(1):1–10.
Li J, Li J, Thornicroft G, Huang Y. Levels of stigma among community mental health staff in Guangzhou, China. BMC Psychiatry. 2014;14(1):1–7.
Bendik I, Friedel A, Roos FF, Weber P, Eggersdorfer M. Vitamin D: a critical and essential micronutrient for human health. Front Physiol. 2014;5:248.
Wang J, Adair C, Fick G, Lai D, Evans B, Perry BW, Jorm A, Addington D. Depression literacy in Alberta: findings from a general population sample. Can J Psychiatry. 2007;52(7):442–9.
Fisher LJ, Goldney RD. Differences in community mental health literacy in older and younger Australians. Int J Geriatr Psychiatry. 2003;18(1):33–40.
Farrer L, Leach L, Griffiths KM, Christensen H, Jorm AF. Age differences in mental health literacy. BMC Public Health. 2008;8(1):125.
Griffiths KM, Christensen H, Jorm AF. Predictors of depression stigma. BMC Psychiatry. 2008;8(1):1–12.
Nguyen TT, TchetgenTchetgen EJ, Kawachi I, Gilman SE, Walter S, Glymour MM. The role of literacy in the association between educational attainment and depressive symptoms. SSM - Population Health. 2017;3:586–93.
Hu Z, Qin L, Xu H. Association between diabetes-specific health literacy and health-related quality of life among elderly individuals with pre-diabetes in rural Hunan Province, China: a cross-sectional study. BMJ Open. 2019;9(8):e028648.
Loo P-W, Furnham A. Knowledge and beliefs about depression among urban and rural Indian Malaysians. Ment Health Relig Cult. 2013;16(10):1009–29.
Reavley NJ, Mackinnon AJ, Morgan AJ, Alvarez-Jimenez M, Hetrick SE, Killackey E, Nelson B, Purcell R, Yap MBH, Jorm AF. Quality of information sources about mental disorders: a comparison of Wikipedia with centrally controlled web and printed sources. Psychol Med. 2012;42(8):1753–62.
Shumet S, Azale T, Angaw DA, Tesfaw G, Wondie M, GetinetAlemu W, Amare T, Kassew T, Mesafint G. Help-Seeking Preferences to Informal and Formal Source of Care for Depression: A Community-Based Study in Northwest Ethiopia. Patient Prefer Adherence. 2021;15:1505–13.
Griffiths KM, Crisp DA, Barney L, Reid R. Seeking help for depression from family and friends: a qualitative analysis of perceived advantages and disadvantages. BMC Psychiatry. 2011;11:196–196.
Picco L, Abdin E, Chong SA, Pang S, Vaingankar JA, Sagayadevan V, Kwok KW, Subramaniam M. Beliefs About Help Seeking for Mental Disorders: Findings From a Mental Health Literacy Study in Singapore. Psychiatr Serv. 2016;67(11):1246–53.
Aguirre Velasco A, Cruz ISS, Billings J, Jimenez M, Rowe S. What are the barriers, facilitators and interventions targeting help-seeking behaviours for common mental health problems in adolescents? A systematic review. BMC Psychiatry. 2020;20(1):293.
Li H, Seidman L. Engaging Asian American youth and their families in quality mental health services. Asian J Psychiatr. 2010;3(4):169–72.
Acknowledgements
The authors of the study express their sincere gratitude of Mashhad University of Medical Sciences. We would like to thanks all participants who assisted the authors to run this study.
Funding
Mashhad University of Medical Sciences funded this project.
Author information
Authors and Affiliations
Contributions
Authors HT, AJ, MM, MV, ECh, and MN designed the study. HT, AJ, MV, MM and MN participated in the conception of the study. HT and AJ managed and conducted the statistical analyses and interpreted the data. AJ and HT wrote the first draft and AJ and HT revised it to make the final manuscript. All authors have approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study is based on a research project approved by Ethics Committee of Mashhad University of Medical Sciences with the code of ethics IR.MUMS.REC.1399.434. All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable. Written Informed Consent was obtained from all subjects and/or their legal guardian(s) and for illiterate participants.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tehrani, H., Vali, M., Nejatian, M. et al. The status of depression literacy and its relationship with quality of life among Iranian public population: a cross sectional study. BMC Psychiatry 22, 607 (2022). https://doi.org/10.1186/s12888-022-04251-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-022-04251-0