
Abstract
Background
Post-traumatic stress disorder (PTSD) is a mental illness that develops in some people after they have experienced a stunning, scary, or dangerous incident. Due to major disasters like as the Economic Crisis and the Beirut Blast, Lebanese people are struggling with a variety of mental health issues. The study objectives were to find the rate of PTSD and its association with stress, anxiety, depression, financial well-being and coping strategies among university students in Lebanon.
Methods
This is a cross-sectional study, conducted between May and August 2021, which enrolled 419 university students from all districts of Lebanon. The PTSD Checklist-Specific Version (PCL-S) was used to evaluate manifestation of PSTD.
Results
The results showed that 132 (31.5%), 109 (26.0%) and 169 (40.3%) had PTSD from COVID, Beirut blast and economic crisis respectively. More avoidant coping (Beta = 0.52) and more anxiety (Beta = 0.62) were significantly associated with more PTSD from the Beirut Blast. More avoidant coping (Beta = 0.56), depression (Beta = 0.40) and anxiety (Beta = 0.49) were significantly associated with more PTSD from the economic crisis, whereas more financial wellbeing (Beta = − 0.31) was significantly associated with less PTSD from the economic crisis.
Conclusion
Significant rates of PTSD were found in our sample of Lebanese university students, whether from the Beirut blast, or from the current economic crisis. Significant correlations of these PTSD rates were found with factors such as avoidant coping, depression, anxiety and financial wellbeing. Such findings must raise the attention to serious mental and psychosocial alteration endured by Lebanese youth that are still under fatal cumulative traumatic events, that were and even may be, intergenerationally and unintentionally transmissible, therefore, affecting not only the present, but also the future of a whole nation.
Similar content being viewed by others


Background
Post-traumatic stress disorder (PTSD) is a mental illness that develops in some people after they have experienced a stunning, scary, or dangerous incident. It establishes itself in both psychological and physical manifestations. The Diagnostic and Statistical Manual of Mental Disorders (DSM-5) defines PTSD as a trauma and stressor-related disorder with symptoms that last more than one month [1]. Psychological symptoms like nightmares [2] and intrusive thoughts are common in PTSD patients, but they can also exhibit symptoms such as hypervigilance, and being constantly on the lookout [3]. Hyperarousal can also be present, which can be sparked by any trigger [4]. Patients prefer to avoid places, people, and situations that bring up memories of the underlying trauma in order to stay away from reliving the memories of the experience [1]. Other functional and social consequences of this persistent attempt to avoid stressors and constant replay of events include sleep disturbances [5] and general irritability [6].
It is important to highlight that not all stressful situations result in the onset of PTSD [7]. A number of factors play a crucial role in determining whether or not individuals may develop PTSD, but one distinguishing aspect is the type of trauma they have experienced [8]. In contrast to occurrences like accidents or disasters, if the trauma has a more personal aspect, such as rape, the patient is more prone to acquire PTSD [9]. Another component is the coping tactics used, which can reduce future PTSD symptoms by, for example, offering emotional support to the patient [10]. Biological causes, such as a malfunction in the endogenous opioid system [11] or a deficit in the arousal and sleep regulating systems, can also cause PTSD [1]. Moreover, genetic predisposition to mood and anxiety disorders, which can be detected in a patient’s family history, can be a contributor in PTSD [12]. Anxiety and depression were found to be comorbid in many investigations of PTSD patients. Depression, anxiety, and phobic avoidance severity levels were all higher among patients suffering from Post-Traumatic Stress [13, 14].
A recent study conducted in Bangladesh showed that people living in poor conditions with low income had higher rates of PTSD. This correlation shows that financial wellbeing might play a major mediating role in people suffering of the repercussions of trauma [15].
Coping with trauma can be challenging, and how well a person can deal with trauma is a key factor in determining the outcome of their rehabilitation after a traumatic experience. People adopt many coping styles during psychological stress [16, 17].
Many coping styles have been previously analyzed, some of them include avoidant coping and approach coping. When dealing with unpleasant conditions, avoidance coping involves cognitive and behavioral strategies aimed at denying, dismissing, or in some other way avoiding stressors. Approach coping is characterized as actively addressing a stressor and look for info, social support, and make an effort to fix certain difficulties [18,19,20].
Avoidant coping methods were found to be linked to the establishment of PTSD symptoms [21].
Facing internal and external changes, the human body maintains homeostasis by a normal mechanism, called the stress response [22]. The duration and the source of exposure play a major role in late adaptive responses to stress. To a controllable stress trigger, a delicate behavioral approach is obtained that prepares well the organism for the subsequent encounter. However, if the source cannot be controlled, a more complex reorganization of neurons is needed in the brain, leading to the development of new coping techniques to deal with the stress source [23].
Lebanon, a Middle Eastern country, is in the midst of constant regional turmoil and adjacent warzones. Lebanese people are plagued with both macro and micro-traumas which puts them at higher risk of having PTSD [24]. The prevalence of PTSD in teenagers who went through the Lebanese 2006 July War, ranged from 15.4 to 35.0% [25].
Subjects in late adolescence-early adulthood (16- to 25-year-olds) seem to be at a higher risk of experiencing potentially traumatic events and/or developing PTSD symptoms [26]. In a study targeting a large sample of newly matriculated US college students [27], about 9% of the 3014 students have met criteria for PTSD. As explored by a recent study among University students in China, 14.1% of college students who experienced a major earthquake, developed PTSD [28]. Lebanese university students have survived constant Middle Eastern changes [24], and a global COVID-19 pandemic [29], adding to the potentially stressful time experienced by undergraduate students while transitioning to university [30], that’s why opting for avoidance as a potential coping mechanism would seem possible.
On August 4th 2020, one of the most powerful blasts ever recorded in contemporary history shook Beirut, the capital of Lebanon [31], which further strained the socio-economic situation in the country [32], and created severe psychological distress within Lebanese citizens [33]. Due to major disasters like as the Economic Crisis and the Beirut Blast, Lebanese people are struggling with a variety of mental health issues [29].
Adding to the above mentioned potential traumatic experiences, it has been demonstrated that mental illness is becoming very common among university students [34, 35]. In addition to academic stress, students are taking on many obligations and transitioning to adulthood with all its responsibilities and challenges, without being equipped with the necessary skills and maturity of adulthood [36]. Consequently, studying PTSD and its correlates in a sample of Lebanese university students would seem crucial.
Our study was guided by those three research questions: (1) What is the prevalence of PTSD among university students in Lebanon? (2) Which coping strategies are of highest relevance when it comes to Post Traumatic Symptoms? and (3) Is there a significant correlation between PTSD and financial well-being, stress, anxiety, and depression?
We evaluated the intensity of Post Traumatic Symptoms and its correlates based on a survey of college students. We initially hypothesized that PTSD levels will be elevated in our sample, and that it will be correlated with higher levels of stress, depression, anxiety and poor financial well-being, as well as negative coping strategies such as avoidant coping. To the best of our knowledge, little is known about the correlation between stress, anxiety, depression, financial well-being, coping strategies and PTSD among university students in Lebanon. Thus, the aim of this cross-sectional study was to find the rate and correlates of PTSD in Lebanese university students amid the socioeconomic crisis and in the aftermath of the Beirut port explosion.
Methods
Study design
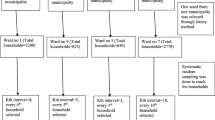
Between May and August 2021, 419 university students from various Lebanese universities participated in this cross-sectional research. No inclusion or exclusion criteria were defined during the recruitment procedure, but we demanded that all participants should be university students that were in Lebanon during the Beirut Blast and the Economic Crisis. The questionnaire was developed with Google Forms and distributed to participants via social media platforms and messaging applications. Data collection was done using snowball sampling and respondent-driven procedures due to the severe coronavirus pandemic imposing social distancing and the closure of all universities in Lebanon. Individual subjects received study objectives and general instructions online prior to participation. No credits were received for participation.
Minimal sample size calculation
The G-power software calculated a minimal sample of 395 students, based on an effect size f2 = 2%, α error = 5%, power = 80%, and a maximum of 15 factors to be included in the multivariable analysis.
Questionnaire
The survey was developed in English, which is widely used in Lebanon and specially among university students. Furthermore, we used English because it’s the most adopted language by Lebanese Universities at academic and teaching levels. The questionnaire was divided in three sections. The first part contained a written consent form that confirmed the participants’ permission to voluntarily complete the survey, in addition to other ethical considerations such as the insurance of the confidentiality and anonymity of the respondents. Moreover, the first part also included general information about the study and some essential instructions for the questionnaire. The second segment includes questions that evaluate the socio-demographic data of the participants (age, gender, district of residence, etc.). The survey also included questions about the presence of a personal history of PTSD, Depression and Anxiety Disorders. The Household Crowding Index (HCI) was calculated by dividing the number of people living in the house by the number of rooms in the house, which represents the family’s socioeconomic status (SES). A greater HCI indicates a lower SES. The third section of the survey comprised the following measures:
PTSD checklist- specific version (PCL-S)
This questionnaire was employed to evaluate the manifestations of PTSD according to the DSM-4 [37]. It has 17 items that are scored from 1 (not at all bothersome) to 5 (extremely bothersome); higher results imply greater severity. The PCL-S is a variation of the PCL-C (Civilian) that focuses on a specific “traumatic experience”, as opposed to stressful experiences in general, as in the PCL-C. In this study the PCL-S was used for the Lebanese economic crisis and the Beirut Blast respectively (current Cronbach’s α = 0.945 for COVID-19 pandemic, 0.947 for the Beirut blast and 0.959 for the economic crisis). Scores ≥44 indicate the presence of PTSD [38].
Financial wellbeing scale
This scale indicates how secure and safe a person feels regarding his financial situation. It is composed of 8 items rated from 1 to 10, with higher scores indicating the least pressure felt from the current financial situation in the country [39]. We obtained a written permission to use this scale (current Cronbach’s α = 0.931).
Beirut distress scale (BDS-10)
This short tool is valid and reliable to screen and recognize psychological distress in the Lebanese population [40]. It is made up of 10 items rated from 0 (never) to 3 (very much); higher scores indicate higher distress (current Cronbach’s α = 0.886).
Lebanese anxiety scale (LAS)
This is a 10-item scale used to rule out anxiety. 7 questions are rated from 0 to 4 and 3 questions graded from 1 to 4; higher scores indicate more anxiety [41, 42] (current Cronbach’s α = 0.907).
Patient health questionnaire (PHQ-9)
It is a self-administered multipurpose scale that assesses, screens and measures the severity of depression during the previous two weeks. This instrument is validated in Lebanon [43], and it’s made of 9 questions rated from “0” (not at all) to “3” (nearly every day); higher scores indicate higher depressive symptoms (current Cronbach’s α = 0.887).
Brief coping orientation to problems experiences (brief-COPE)
It is an abbreviated, 28-item self-report scale deriving from the COPE (Coping Orientation to Problems Experienced) Inventory [44]. Scores are presented under two subscales (Avoidant Coping and Approach Coping). The questions are rated from “1” (I haven’t been doing this at all) to “4” (I’ve been doing this a lot). The scale can determine someone’s primary coping styles as either Approach Coping, or Avoidant Coping [44], with higher scores indicating more coping strategies (current Cronbach’s α = 0.856 for approach coping and 0.790 for avoidant coping).
Statistical analysis
Statistical analysis was performed using SPSS software, version 23. There was no missing data since all questions were required in the Google form. Both PTSD scores had a normal distribution (skewness and kurtosis between − 1 and + 1 [45]). Accordingly, the Student t-test was used to check for an association between the PTSD scores and dichotomous variables (i.e., gender), while the Pearson correlation test was used to correlate two continuous variables (i.e., age, household crowding index, etc.). Effect sizes were calculated for all bivariate analyses; in psychological research, values of 0.1 were deemed to have small effect size, whereas values of 0.2 and 0.3 were classified as having medium and large effect sizes respectively [46]. Stepwise linear regressions were conducted taking the PTSD scores as dependent variables. Covariates that were included in the final models were those that showed an effect size or correlation > │0.24│ in the bivariate analysis to have parsimonious models [47]. P < 0.05 was considered significant.
Results
The sample consisted of 419 participants, with a mean age of 21.02 ± 2.59 years and 70.4% females. Other characteristics and description of the scores can be found in Table 1.
Based on the cutoff value of 44 for the PCL-S scale, the results showed that 132 (31.5%), 109 (26.0%) and 169 (40.3%) had PTSD from COVID, Beirut blast and economic crisis respectively.
Bivariate analysis
Higher depression, anxiety, stress, avoidant coping and coping approach were significantly associated with more PTSD from the Beirut blast and from the economic crisis, whereas higher financial wellbeing was significantly associated with less PTSD from the Beirut blast and from the economic crisis. Furthermore, higher household crowding index was significantly associated with more PTSD from the economic crisis only (Table 2). On another hand, higher mean PTSD from the Beirut blast and from the economic crisis scores were found in those who have a personal history of anxiety, PTSD and depression compared to those who do not. Finally, higher PTSD form the Beirut blast was seen in females compared to males (Table 3).
Multivariable analysis
The results of a first linear regression (enter method), taking the PTSD from the Beirut blast score as the dependent variable, showed that more avoidant coping (Beta = 0.52) and more anxiety (Beta = 0.62) were significantly associated with more PTSD from the Beirut Blast (Table 4, Model 1).
A second linear regression, taking the PTSD from the economic crisis score as the dependent variable, showed that more avoidant coping (Beta = 0.56), depression (Beta = 0.40) and anxiety (Beta = 0.49) were significantly associated with more PTSD from the economic crisis, whereas more financial wellbeing (Beta = − 0.31) was significantly associated with less PTSD from the economic crisis (Table 4, Model 2).
Discussion
To the best of our knowledge, there have been no studies in the current scientific literature to assess the correlation between PTSD and factors such as avoidant coping, depression, anxiety, and financial wellbeing in a sample of Lebanese university students, especially in the settings of two major traumas: the economic crisis and the Beirut Blast. The multivariable analyses results showed that more avoidant coping and more anxiety were significantly associated with more PTSD from the Beirut Blast and the economic crisis, whereas more financial wellbeing was significantly associated with less PTSD from the economic crisis.
In the current study, the results showed significant rates of PTSD, respectively, from the COVID-19 pandemic (31.5%), the Beirut blast (26.0%), and the economic crisis (40.3%). Concomitantly with other studies comparing prevalence values between university students’ samples and the general population, the latter values are hardly comparable with values from the Lebanese general population. In fact, almost all the studies from Lebanon about PTSD were cross-sectional, and focused on specific sub-groups from the population [24], such as South Lebanese civilians [48], battered women [49], victims of blasts [50], and hospitalized men after armed conflicts [51]. Thus, a wide range of PTSD prevalence estimates was found, varying from 2 to 98% [24]. Another hardship would be as well, to compare the rates of PTSD that we found in our sample to other values from other university students’ samples. In fact, while 14.1% of college students who experienced a major earthquake, developed PTSD in a sample of Chinese university students [52], 2.7% of a large Chinese college student sample experienced PTSD one month after the outbreak of the COVID-19 epidemic [53], and about 9% of 3014 newly matriculated US students [27] have met criteria for PTSD. However, these wide variances are to be explained by multifaceted factors, of which the “potentially traumatic event’s load/number of events” [8, 54], and whether the traumatic event is collective or interpersonal, and many other factors, differentiating the Lebanese university student’s population from any other population.
More avoidant coping correlated with more PTSD symptoms, whether from the Beirut blast event or from the recent economic crisis. In fact, prior findings from cross-sectional studies have shed the light on the tight correlation between avoidant coping and PTSD symptoms [55], in samples of war veterans [56], motor vehicle accident survivors [57], victims of sexual and nonsexual assaults [58], and hurricane flood survivors [59]. Other few longitudinal studies [60,61,62] predicted a moderating relationship between avoidant coping and PTSD symptoms, whether acutely or distantly to the traumatic event. In a longitudinal study [55] targeting PTSD after exposure to domestic violence, avoidant coping was found to predict more PTSD symptoms over time, independently of the level of intimate partner violence. Indeed, the current study was conducted around one year after the Beirut Blast, and 21 months from the beginning of the economic crisis. However, given the cross-sectional design of our study, the prediction of the severity of the PTSD symptoms by the avoidant coping cannot be discussed.
More anxiety was significantly associated with more PTSD from both the Beirut Blast and the economic crisis, while more depression was significantly associated with more PTSD from the economic crisis. In fact, in a report six months after the Beirut blast, increased need for mental health consultations was seen in the Lebanese population, not just after the collective trauma of the Beirut blast, but even months before, because of the collapsed economic situation in Lebanon with a consequent unemployment rate of more than 30%, and hyperinflation of food and basic medications’ prices because of devaluation of the Lebanese pound [63]. Thus, an increased prevalence of anxiety and depression was reported as well as higher incidents of suicides and calls to suicide hotlines. Many studies have reported a significant and frequent comorbidity among anxiety, depression, and PTSD [64, 65]. In 2018, a study about the relationship between PTSD and other psychiatric comorbidities [14], 40.8% of the subjects that were diagnosed of a mixed anxiety-depression disorder have reported at least one traumatic event exposure during their lifetime.
Many findings in the scientific literature have identified common neurobiological and psychological grounds for anxiety and PTSD [66, 67]. In subjects with a higher anxiety levels, the autonomic nervous system tends to overreact in the setting of traumatic events [68]. In a recent meta-analysis [69], there was neuroimaging evidence about common brain mechanisms between anxiety disorders and PTSD with certain interrelationships explaining some emotional dysregulation symptoms that extend beyond the simple exaggerated fear response. Furthermore, one other study [70] has suggested that anxiety may be a precursor of PTSD. Hence, our current results seem to strongly align with other research findings concerning the association between anxiety and PTSD.
Similarly, another common neurobiological basis was found between PTSD and depression [71]. In a study targeting the biological differences between trauma-related depression and PTSD [72], depression and PTSD, whether comorbid or not, were both found to participate in the suppression of the hypothalamo-pituitary-adrenocortical axis in traumatized subjects. Kessler et al. [73] have found a 49% rate of depression that was frequently comorbid with PTSD. Thus, in accordance with other literature findings, it was shown in the current study, that subjects with PTSD would have higher scores of depressive symptoms.
More financial wellbeing was significantly associated with less PTSD from the economic crisis. Although the same Lebanese population may seem to be struck by the same collective stressor, the economic crisis, the response and effects of such stressor may vary in function of many factors, of which, the financial and economic differences between subgroups of this same population. In fact, low socioeconomic status was found to be one of the several risk factors associated with the development of PTSD [73, 74]. Furthermore, people with a certain financial wellbeing may seem to have a better societal safety net, which may give them a certain psychological backup/resilience to buffer the striking trauma of economic crisis [75]. In a recent study about financial well-being and post-deployment adjustment among Iraq and Afghanistan war veterans [76], it was reported that financial strains and PTSD are mutually reinforcing, since subjects with PTSD, hence with poor adaptive mechanism, will hardly ensure their financial wellbeing. Furthermore, poor financial wellbeing would deprive subjects from tools to absorb there traumas [76]. However, in some other studies, it was found that affluent countries were more likely to be affected by PTSD than poor countries, given that poor countries are of a greater “resilience reserve”, given their frequent exposure to repeated traumas [77,78,79]. Thus, more studies are needed to explain this correlation between PTSD and financial wellbeing, especially in the Lebanese population, where repeated traumas have granted the population a certain “bounce-back –resilience”, that may however, start to be depleted after the latest several traumatic events [77,78,79].
Clinical implications
Our findings demonstrated considerable rates of PTSD among college students, whether correlated with coping strategies, anxiety, depression, or financial well-being. Thus, our data could orient health managers and universities (academic and teaching levels) to categorize specific risk factors and implement evidence-based interventions to predict the risk of the onset of PTSD. They could also provide preventive and diagnostic measures, as well as regular screenings in order to deliver subsequent high-quality care for the affected population. On another note, psychiatric caregivers and nurses, more than any other caregivers are concerned with occupational vulnerabilities, such as job burnout and compassion fatigue [80]. On the Lebanese national scale, just three mental hospitals and five units of psychiatry within general hospitals were operating prior to the Beirut blast [81]. Following the Beirut blast, and the current economic crisis, the need for mental health services has subsequently increased as well [63]. Hence, this would expose the psychiatric caregivers to further clinical exposure to mental illnesses’ emergence, such as PTSD and its correlates. Moreover, it would be a call to show more interest in possible subsequent occupational vulnerabilities that would be added to psychiatric caregivers in the settings of increased mental illnesses’ emergence.
Limitations
There are some limitations to this study. Even though our data revealed significant associations between PTSD and many correlates, the study’s cross-sectional design prevents us from establishing causality. The data was collected online via Google Forms due to the COVID-19 pandemic and social distancing, which may have led to selection bias. For a variety of reasons, the results cannot be considered typical of the general population: women were disproportionately represented, which is expected because women are more likely to respond to surveys than men [82, 83]. This gender difference could have led to an overestimation of the rates of PTSD in our sample knowing that gender differences are well known in this mental illness with a 2:1 ratio, favoring women [84]. Plus, several sociodemographic factors were not fairly distributed, which further limits the representativeness of our sample. In addition, the percentage of participants with a personal history of depression and anxiety disorders were higher than those with a personal history of PTSD. The symptoms were subjective and not evaluated by a healthcare professional; because reporting was subjective rather than clinically based, information bias is likely. During the data collection period, there were still numerous deaths from the pandemic: more than 700 from May to August, according to official records. This might have caused the pandemic to influence our responses. Some of the scales used (PTSD, financial wellbeing, brief cope) are not validated in Lebanon, that’s why the results should be interpreted with great caution. Because of the above-mentioned limitations, our results can’t be generalized. Further research taking into account these limitations is needed.
Conclusion
To conclude, significant correlations were found between PTSD and factors such as avoidant coping, depression, anxiety and financial wellbeing, in a sample of Lebanese university students. However, these results remain limited to a restrained sample among this age group. Nonetheless, such findings must raise the attention to serious mental and psychosocial alteration endured by Lebanese youth, that are still under fatal cumulative traumatic events, that were and even may be, intergenerationally and unintentionally transmissible [85], therefore, affecting not only the present, but also the future of a whole nation. Thus, in a country where treating mental disorders is much lesser than most other developing countries [86], this study would shed the light on the need for clinical interventions owing to detect mental vulnerabilities in the general population. Thus, longitudinal, and prospective studies to understand the multifactorial causes and correlates of PTSD, whether from previous collective traumas, or from individual traumatic history, are needed. Preventive and diagnostic procedures are to be initiated, whether acutely or distantly from the previous traumas, on a national level.
Availability of data and materials
All data generated or analyzed during this study are not publicly available due to restrictions from the ethics committee. The dataset supporting the conclusions is available upon request to the corresponding author (SH).
References
Association Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5. Arlington; 2013.
Germain A. Sleep disturbances as the hallmark of PTSD: where are we now? Am J Psychiatr. 2013;170(4):372–82.
Shipherd JC, Salters-Pedneault K. Attention, memory, intrusive thoughts, and acceptance in PTSD: an update on the empirical literature for clinicians. Cogn Behav Pract. 2008;15(4):349–63.
Kendall-Tackett KA. Physiological correlates of childhood abuse: chronic hyperarousal in PTSD, depression, and irritable bowel syndrome. Child Abuse Negl. 2000;24(6):799–810.
Richards A, Kanady JC, Neylan TC. Sleep disturbance in PTSD and other anxiety-related disorders: an updated review of clinical features, physiological characteristics, and psychological and neurobiological mechanisms. Neuropsychopharmacology. 2020;45(1):55–73.
Castillo DT, Baca JCD, Conforti K, Qualls C, Fallon SK. Anger in PTSD: general psychiatric and gender differences on the BDHI. J Loss Trauma. 2002;7(2):119–28.
Schnyder U. Prevalence of exposure to potentially traumatic events and PTSD. Eur Arch Psychiatry Clin Neurosci. 2006;256(3):151–8.
Breslau N, Davis GC, Andreski P, Peterson E. Traumatic events and posttraumatic stress disorder in an urban population of young adults. Arch Gen Psychiatry. 1991;48(3):216–22.
Jakob JM, Lamp K, Rauch SA, Smith ER, Buchholz KR. The impact of trauma type or number of traumatic events on PTSD diagnosis and symptom severity in treatment seeking veterans. J Nerv Ment Dis. 2017;205(2):83–6.
Dworkin ER, Ullman SE, Stappenbeck C, Brill CD, Kaysen D. Proximal relationships between social support and PTSD symptom severity: a daily diary study of sexual assault survivors. Depress Anxiety. 2018;35(1):43–9.
Torres-Berrio A, Nava-Mesa MO. The opioid system in stress-induced memory disorders: from basic mechanisms to clinical implications in post-traumatic stress disorder and Alzheimer's disease. Prog Neuro Psychopharmacol Biol Psychiatry. 2019;88:327–38.
Koenen KC, Harley R, Lyons MJ, Wolfe J, Simpson JC, Goldberg J, et al. A twin registry study of familial and individual risk factors for trauma exposure and posttraumatic stress disorder. J Nerv Ment Dis. 2002;190(4):209–18.
Spinhoven P, Penninx BW, Van Hemert AM, De Rooij M, Elzinga BM. Comorbidity of PTSD in anxiety and depressive disorders: prevalence and shared risk factors. Child Abuse Negl. 2014;38(8):1320–30.
Ozen S, Dalbudak E, Topcu M. The relationship of posttraumatic stress disorder with childhood traumas, personality characteristics, depression and anxiety symptoms in patients with diagnosis of mixed anxiety-depression disorder. Psychiatr Danub. 2018;30(3):340–7.
Islam M, Rahman E, Banik R, Ishraq Emran M, Saiara N, Hossain S, et al. Correlates of Financial Concerns and Symptoms of Depression and Posttraumatic Stress Disorder in Impoverished Urban-dwelling Individuals in Bangladesh During the COVID-19 Pandemic: Face-to-face Interview Findings. 2020. https://doi.org/10.31234/osf.io/nfr5m.
Nydegger R, Nydegger L, Basile F. Post-traumatic stress disorder and coping among career professional firefighters. AJHS. 2011;2(1):11–20.
Amir M, Kaplan Z, Efroni R, Levine Y, Benjamin J, Kotler M. Coping styles in post-traumatic stress disorder (PTSD) patients. Personal Individ Differ. 1997;23(3):399–405.
Eisenberg SA, Shen BJ, Schwarz ER, Mallon S. Avoidant coping moderates the association between anxiety and patient-rated physical functioning in heart failure patients. J Behav Med. 2012;35(3):253–61.
Finset A, Steine S, Haugli L, Steen E, Laerum E. The brief approach/avoidance coping questionnaire: development and validation. Psychol Health Med. 2002;7(1):75–85.
Penley JA, Tomaka J, Wiebe JS. The association of coping to physical and psychological health outcomes: a meta-analytic review. J Behav Med. 2002;25(6):551–603.
Hooberman J, Rosenfeld B, Rasmussen A, Keller A. Resilience in trauma-exposed refugees: the moderating effect of coping style on resilience variables. Am J Orthopsychiatry. 2010;80(4):557.
Ursin H, Eriksen HR. The cognitive activation theory of stress. Psychoneuroendocrinology. 2004;29(5):567–92.
Stam R. PTSD and stress sensitisation: a tale of brain and body part 1: human studies. Neurosci Biobehav Rev. 2007;31(4):530–57.
El Hajj M. Prevalence and associated factors of post-traumatic stress disorder in Lebanon: a literature review. Asian J Psychiatr. 2021;63:102800.
Shaar KH. Post-traumatic stress disorder in adolescents in Lebanon as wars gained in ferocity: a systematic review. J Public Health Res. 2013;2(2):e17.
Cusack SE, Hicks TA, Bourdon J, Sheerin CM, Overstreet CM, Kendler KS, et al. Prevalence and predictors of PTSD among a college sample. J Am Coll Heal. 2019;67(2):123–31.
Read JP, Ouimette P, White J, Colder C, Farrow S. Rates of DSM-IV-TR trauma exposure and posttraumatic stress disorder among newly matriculated college students. Psychol Trauma. 2011;3(2):148–56.
Fu Y, Chen Y, Wang J, Tang X, He J, Jiao M, et al. Analysis of prevalence of PTSD and its influencing factors among college students after the Wenchuan earthquake. Child Adolesc Psychiatry Ment Health. 2013;7(1):1–6.
El Rassoul AEA, Razzak RA, Hashim HT. Mental health effects of COVID-19 within the socioeconomic crisis and after the Beirut blast among health care workers and medical students in Lebanon. Prim Care Companion CNS Disord. 2021;23(4):35348.
Palmer A, Rodger S. Mindfulness, stress, and coping among university students. Can J Couns Psychother. 2009;43(3). Available from: https://cjc-rcc.ucalgary.ca/article/view/59019.
How powerful was the Beirut Blast? Available from: https://graphics.reuters.com/LEBANON-SECURITY/BLAST/yzdpxnmqbpx/.
Devi S. Lebanon faces humanitarian emergency after blast. Lancet (London, England). 2020;396(10249):456.
El Khoury Malhame M, Harajli DA, Reykowska D, Ohme R. Traumatic effect of Beirut port explosion on Lebanese people's experiences. http://dx.doi.org/10.2139/ssrn.3929408.
Holmes A, Silvestri R. Rates of mental illness and associated academic impacts in Ontario’s college students. Can J Sch Psychol. 2016;31(1):27–46.
Wang X, Hegde S, Son C, Keller B, Smith A, Sasangohar F. Investigating mental health of US college students during the COVID-19 pandemic: cross-sectional survey study. J Med Internet Res. 2020;22(9):e22817.
Pedrelli P, Nyer M, Yeung A, Zulauf C, Wilens T. College students: mental health problems and treatment considerations. Acad Psychiatry. 2015;39(5):503–11.
Wilkins KC, Lang AJ, Norman SB. Synthesis of the psychometric properties of the PTSD checklist (PCL) military, civilian, and specific versions. Depress Anxiety. 2011;28(7):596–606.
Blanchard EB, Jones-Alexander J, Buckley TC, Forneris CA. Psychometric properties of the PTSD checklist (PCL). Behav Res Ther. 1996;34(8):669–73.
Prawitz A, Garman ET, Sorhaindo B, O’Neill B, Kim J, Drentea P. InCharge financial distress/financial well-being scale: development, administration, and score interpretation. J Financ Couns Plan. 2006;17(1):669–73.
Malaeb D, Farchakh Y, Haddad C, Sacre H, Obeid S, Hallit S, et al. Validation of the Beirut distress scale (BDS-10), a short version of BDS-22, to assess psychological distress among the Lebanese population. Perspect Psychiatr Care. 2021;58(1):304–13.
Hallit S, Obeid S, Haddad C, Hallit R, Akel M, Haddad G, et al. Construction of the Lebanese anxiety scale (LAS-10): a new scale to assess anxiety in adult patients. Int J Psychiatry Clin Pract. 2020;24(3):270–7.
Merhy G, Azzi V, Salameh P, Obeid S, Hallit S. Anxiety among Lebanese adolescents: scale validation and correlates. BMC Pediatr. 2021;21(1):1–8.
Sawaya H, Atoui M, Hamadeh A, Zeinoun P, Nahas Z. Adaptation and initial validation of the patient health questionnaire–9 (PHQ-9) and the generalized anxiety disorder–7 questionnaire (GAD-7) in an Arabic speaking Lebanese psychiatric outpatient sample. Psychiatry Res. 2016;239:245–52.
Carver CS. You want to measure coping but your protocol’too long: consider the brief cope. Int J Behav Med. 1997;4(1):92–100.
George D: SPSS for windows step by step: a simple study guide and reference, 17.0 update, 10/e: Pearson Education India; 2011.
Funder DC, Ozer DJ. Evaluating effect size in psychological research: sense and nonsense. Adv Methods Pract Psychol Sci. 2019;2(2):156–68.
Vandekerckhove J, Matzke D, Wagenmakers E-J. Model comparison and the principle of parsimony. eScholarship, University of California; 2014.
Farhood LF, Dimassi H. Prevalence and predictors for post-traumatic stress disorder, depression and general health in a population from six villages in South Lebanon. Soc Psychiatry Psychiatr Epidemiol. 2012;47(4):639–49.
Khadra C, Wehbe N, Lachance Fiola J, Skaff W, Nehme M. Symptoms of post-traumatic stress disorder among battered women in Lebanon: an exploratory study. J Interpers Violence. 2015;30(2):295–313.
Fares J, Gebeily S, Saad M, Harati H, Nabha S, Said N, et al. Post-traumatic stress disorder in adult victims of cluster munitions in Lebanon: a 10-year longitudinal study. BMJ Open. 2017;7(8):e017214.
Yaacoub H, Haddad C, Dib T, Zoghbi M, Assaad S, Obeid S, et al. Posttraumatic stress disorders and depression among male inpatient adults involved in the Lebanese war. Perspect Psychiatr Care. 2020;56(2):263–9.
Zhang Z, Ran MS, Li YH, Ou GJ, Gong RR, Li RH, et al. Prevalence of post-traumatic stress disorder among adolescents after the Wenchuan earthquake in China. Psychol Med. 2012;42(8):1687–93.
Tang W, Hu T, Hu B, Jin C, Wang G, Xie C, et al. Prevalence and correlates of PTSD and depressive symptoms one month after the outbreak of the COVID-19 epidemic in a sample of home-quarantined Chinese university students. J Affect Disord. 2020;274:1–7.
Kaysen D, Rosen G, Bowman M, Resick PA. Duration of exposure and the dose-response model of PTSD. J Interpers Violence. 2010;25(1):63–74.
Krause ED, Kaltman S, Goodman LA, Dutton MA. Avoidant coping and PTSD symptoms related to domestic violence exposure: a longitudinal study. J Trauma Stress. 2008;21(1):83–90.
Sutker PB, Davis JM, Uddo M, Ditta SR. War zone stress, personal resources, and PTSD in Persian gulf war returnees. J Abnorm Psychol. 1995;104(3):444.
Bryant RA, Harvey AG. Processing threatening information in posttraumatic stress disorder. J Abnorm Psychol. 1995;104(3):537.
Chivers-Wilson KA. Sexual assault and posttraumatic stress disorder: a review of the biological, psychological and sociological factors and treatments. MJM. 2006;9(2):111.
Bistricky SL, Long LJ, Lai BS, Gallagher MW, Kanenberg H, Elkins SR, et al. Surviving the storm: avoidant coping, helping behavior, resilience and affective symptoms around a major hurricane-flood. J Affect Disord. 2019;257:297–306.
Manne SL, Ostroff J, Winkel G, Grana G, Fox K. Partner unsupportive responses, avoidant coping, and distress among women with early stage breast cancer: patient and partner perspectives. Health Psychol. 2005;24(6):635.
Pineles SL, Mostoufi SM, Ready CB, Street AE, Griffin MG, Resick PA. Trauma reactivity, avoidant coping, and PTSD symptoms: a moderating relationship? J Abnorm Psychol. 2011;120(1):240.
Thompson NJ, Fiorillo D, Rothbaum BO, Ressler KJ, Michopoulos V. Coping strategies as mediators in relation to resilience and posttraumatic stress disorder. J Affect Disord. 2018;225:153–9.
Rayes D. The Beirut Explosion’s Impact on Mental Health. 2021. Available from: https://timep.org/commentary/analysis/the-beirut-explosions-impact-on-mental-health/.
Ginzburg K, Ein-Dor T, Solomon Z. Comorbidity of posttraumatic stress disorder, anxiety and depression: a 20-year longitudinal study of war veterans. J Affect Disord. 2010;123(1–3):249–57.
Campbell SB, Renshaw KD, Righter JB. The role of personality traits and profiles in posttrauma comorbidity. J Trauma Dissociation. 2015;16(2):197–210.
Grupe DW, Nitschke JB. Uncertainty and anticipation in anxiety: an integrated neurobiological and psychological perspective. Nat Rev Neurosci. 2013;14(7):488–501.
Steimer T. The biology of fear-and anxiety-related behaviors. Dialogues Clin Neurosci. 2002;4(3):231.
Marais A, Stuart A. The role of temperament in the development of post-traumatic stress disorder amongst journalists. S Afr J Psychol. 2005;35(1):89–105.
Etkin A, Wager TD. Functional neuroimaging of anxiety: a meta-analysis of emotional processing in PTSD, social anxiety disorder, and specific phobia. Am J Psychiatr. 2007;164(10):1476–88.
Collimore KC, McCabe RE, Carleton RN, Asmundson GJ. Media exposure and dimensions of anxiety sensitivity: differential associations with PTSD symptom clusters. J Anxiety Disord. 2008;22(6):1021–8.
Brady KT, Killeen TK, Brewerton T, Lucerini S. Comorbidity of psychiatric disorders and posttraumatic stress disorder. J Clin Psychiatry. 2000;61:22–32.
Savic D, Knezevic G, Damjanovic S, Spiric Z, Matic G. Is there a biological difference between trauma-related depression and PTSD? DST says ‘NO’. Psychoneuroendocrinology. 2012;37(9):1516–20.
Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson CB. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry. 1995;52(12):1048–60.
Trepasso-Grullon E. Differences among ethnic groups in trauma type and PTSD symptom severity. Grad Stud J Psychol. 2012;14(1):102–12.
Morrell-Bellai T, Goering P, Katherine B. Becoming and remaining homeless: a qualitative investigation. Issues Ment Health Nurs. 2000;21(6):581–604.
Elbogen EB, Johnson SC, Wagner HR, Newton VM, Beckham JC. Financial well-being and postdeployment adjustment among Iraq and Afghanistan war veterans. Mil Med. 2012;177(6):669–75.
Rakesh G, Morey RA, Zannas AS, Malik Z, Marx CE, Clausen AN, et al. Resilience as a translational endpoint in the treatment of PTSD. Mol Psychiatry. 2019;24(9):1268–83.
El Hayek S, Bizri M. Beirut blast and mental health in Lebanon: finding ways out. Asian J Psychiatr. 2020;54:102458.
Dückers ML, Brewin CR. A paradox in individual versus national mental health vulnerability: are higher resource levels associated with higher disorder prevalence? J Trauma Stress. 2016;29(6):572–6.
Franza F, Del Buono G, Pellegrino F. Psychiatric caregiver stress: clinical implications of compassion fatigue. Psychiatr Danub. 2015;27(Suppl 1):S321–7.
Yehia F, El Jardali F. Applying knowledge translation tools to inform policy: the case of mental health in Lebanon. Health Res Policy Syst. 2015;13:29.
Curtin R, Presser S, Singer E. The effects of response rate changes on the index of consumer sentiment. Public Opin Q. 2000;64(4):413–28.
Moore DL, Tarnai J. Evaluating nonresponse error in mail surveys. Surv Nonresponse. 2002;64(4):197–211.
Christiansen DM, Berke ET. Gender-and sex-based contributors to sex differences in PTSD. Curr Psychiatry Rep. 2020;22(4):1–9.
Sochos A. Post-traumatic stress during the Greek economic crisis: is there evidence for mass traumatisation? 2018;18(1):65–283. https://doi.org/10.1111/asap.12155.
Karam EG, Mneimneh ZN, Karam AN, Fayyad JA, Nasser SC, Chatterji S, et al. Prevalence and treatment of mental disorders in Lebanon: a national epidemiological survey. Lancet. 2006;367(9515):1000–6.
Acknowledgements
We would like to thank all participants.
Funding
None.
Author information
Authors and Affiliations
Contributions
SO and SH designed the study; MM, CZ and AC wrote the paper; CZ and AC collected the data; SH carried out the analysis and interpreted the results; all authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The Psychiatric Hospital of the Cross Ethics and Research Committee approved this study protocol (HPC-028-2021). An informed written informed consent was considered obtained from each participant when submitting the online form. All methods were performed in accordance with the relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors have nothing to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
El Zouki, CJ., Chahine, A., Mhanna, M. et al. Rate and correlates of post-traumatic stress disorder (PTSD) following the Beirut blast and the economic crisis among Lebanese University students: a cross-sectional study. BMC Psychiatry 22, 532 (2022). https://doi.org/10.1186/s12888-022-04180-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-022-04180-y