
Abstract
Background
Covid-19 pandemic has been profoundly affecting people around the world. While contact restrictions, school closures and economic shutdown were effective to reduce infection rates, these measures go along with high stress for many individuals. Persons who have experienced adverse childhood experiences (ACEs) have an increased risk for mental health problems already under normal conditions. As ACEs can be associated with a higher vulnerability to stress we aimed to assess the role of ACEs on depressive symptoms during the Covid-19 pandemic.
Methods
In a cross-sectional online survey, 1399 participants above the age of 18 years were included during the first lockdown in Germany. Via two-way repeated measures ANOVA, differences in depressive symptoms before (retrospectively assessed) and during the pandemic were analyzed. Linear regression analyses were performed in order to identify predictors for increase of depressive symptoms.
Results
Compared to prior to the Covid-19 pandemic, depressive symptoms increased among all participants. Participants with ACEs and income loss reported about a stronger increase of depressive symptoms. Other predictors for increased depressive symptoms were young age and a lack of social support.
Conclusions
Based on these results, ACEs are a significant predictor for an increase in depressive symptoms during the pandemic, indicating that personss with ACEs may be a risk group for mental health problems during the current and potential later pandemics. These findings underline the relevance of support for persons who have experienced ACEs and may help to provide more targeted support in possible scenarios due to the current or possible other pandemics. Besides, economic stability seems to be of prior importance for mental health.
Similar content being viewed by others


Introduction
The novel severe acute respiratory syndrome coronavirus-2 (SARS CoV-2) pandemic has been profoundly affecting people around the world. Contact restrictions, school closures and economic shutdown have proven to be effective reactions to fight against increasing numbers of Coronavirus disease 19 (Covid-19) cases and fatalities [1, 2]. However, this success comes with a dark side. Negative consequences of measures such as “social distancing” and quarantine for mental health have been discussed in reviews [3,4,5,6], and confirmed by studies [7,8,9,10].
While in most countries, lockdown phases have ended, currently, numerous areas face a still high numbers of Covid-19 infections. Moreover, the occurrence of new pandemics is expected in the next decades. Because depression is even under normal conditions the third leading cause of disability (as measured by years lived with disability; YLDs) [11], an increase can be expected triggered by the challenges of the pandemic. Consequently, to identify predictors of an increase of depression is of major public health interest.
Existing literature suggests that loneliness [12] and less social support [13, 14] are associated with depressive symptoms during the pandemic. Economic stressors were shown to predict depressive symptoms during the pandemic [15]. Younger age is associated with increased mental health problems during the pandemic [9, 16]. Preexisting psychiatric disorders were also identified to predict depressive symptoms [17, 18].
Another predictor for poorer mental health during and in the aftermath of the pandemic may be adverse childhood experiences (ACEs) [19]. Even in more normal times, ACEs are associated with psychosocial and economic impairments, a significant reduction in quality of life, risky behavior and increased morbidity due to both, mental and somatic health problems [20,21,22,23,24,25,26]. Importantly, evidence for moderate to strong associations between ACEs and depression, just as for other major psychiatric disorders, were numerously shown in prospective and retrospective studies [20, 25,26,27]. Lower social support, associated to the experience of childhood adversity [28], was shown to mediate the association between ACEs and mental health [29, 30]. ACEs are associated with lower household income, but also with financial wellbeing and financial literacy [31].
The experience of adversity during childhood is associated with heightened neural response to signals of threat [32], increased emotional reactivity and decreased emotion regulation [33]. Based on these facts, it seems not surprising that ACEs were found to be associated with higher depressive symptoms [10, 34] and emotional exhaustion [35] during the pandemic. However, as ACEs are known to predict depressive symptoms, in order to assess the role of ACEs during the pandemic, change of depressive symptoms compared to before the pandemic has to be assessed. Previously, we have found ACEs to be associated with a stronger decrease in quality of life, general health status, dysfunctional coping strategies [35, 36] and a higher risk for intrafamiliar problems [35, 37, 38]. A higher stress-vulnerability and a decrease of emotion regulation [32, 33] was shown for people who have experienced ACEs, affecting coping of stressful situations.Here, we hypothesized that childhood adversities predict an increase of depressive symptoms during the pandemic. Therefore, in an online survey, we have assessed depressive symptoms before the pandemic retrospectively and current depressive symptoms during the pandemic. Moreover, we aimed to identify other predictors increasing depressive symptoms in order to help identifying high risk groups and developing targeted care.
Methods
Study design
Using the platform Unipark, we have conducted a cross-sectional online survey which was available from May 18th–July 21th 2020. The first lockdown in Germany began on March 23, 2020 and ended with gradual relaxations. First schools reopened on April 22, openings of schools and kindergartens stretched to the end of June 2020. We distributed information on the survey by our homepage, social media and print media and existing mailing lists from other studies and interested parties.
Ethics
Electronic informed consent was obtained from each participant prior to starting the survey. Information on the study and data analysis were given. Participation was voluntary and anonymous. Participants could withdraw from the survey at any moment without providing any justification. The study was conducted in accordance with the Declaration of Helsinki. After consultation with the ethics committee of the University of Ulm, the committee officially stated that there is no requirement for an ethics vote due to the anonymous character of the study.
Measures
Socio-demographic questions covered among others age, gender, educational level, occupation, marital status, number of persons under 18 years in the household and number of own children. Covid-19 associated questions included and whether the household income decreased by more than a quarter since the beginning of the CoVid-19 crisis. Moreover, it was included whether the participant has been working in a system-relevant work. In Germany, this term refers to people working in jobs that were not paused during the first lockdown in spring 2020 and not affected by working from home, such as personnel in medical institutions, supermarkets, police, etc.
The adverse childhood experiences were assessed using the German version of the Adverse Childhood Experiences Questionnaire, a standard tool for retrospective assessment of ACEs with satisfactory internal consistency (Cronbachs α = 0.76) [39].
Depressive symptoms were assessed by the eight-item Patient Health Questionnaire depression scale (PHQ-8), an established and valid diagnostic and severity measure for depressive disorders [40]. Additionally, we included one item on alcohol and tranquilizer use asking the question: “When everything becomes too much for me, I resort to alcohol or tranquilizers”. Social support was assessed by the question “I have people with whom I can talk about my problems and who understand me”, answers on a scale between [1] stands for "does not apply at all", [10] stands for "applies completely. The assessment of depressive symptoms before the pandemic were assessed retrospectively, as our study had a cross-sectional design.
Data analysis
All statistical analyses were performed with SPSS version 21. The prevalence rates were determined using descriptive analyses, only valid cases were included. Valid numbers are given for each analysis.
A two-way repeated measures ANOVA was used to test differences in depressive symptoms before (retrospectively assessed) and during the pandemic (main effect time), between groups with different numbers of ACEs (main effect ACE) as well as income loss due to the pandemic (main effect income loss) and a differential effect of ACEs on the increase of depressive symptoms over time (interaction effect time x ACE). The number of ACEs were categorized for this analyses into three groups: 0 vs 1–3 vs 4 and more ACEs.
Linear regression analyses were performed in order to identify predictors for increase of depressive symptoms. As dependent variable, the difference from the PHQ8 total score before and during lockdown was used. Thus, if the PHQ-8 score was higher during lockdown, the difference is negative. If the score was higher compared to before lockdown, the difference is positive. In a first block, gender and age at the point of entry into the institution were analyzed as predictors. In a second block, number of ACEs were included. In a third block, the additional variables systematically important work, decrease of household income since the beginning of the pandemic, living alone, social support, and pre-existing mental illness were included step-wise.
Results
Participants
A total of 1399 participants completed the survey. For a detailed analysis of the participants, see Table 1.
Change of depressive symptoms
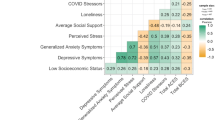
The results of the two-way repeated measures ANOVA revealed that there was a significant main effect of time for all items. In detail, significant effects were seen for PHQ total score (F = 436.79, p < 0.001) and the items sleep (F = 211.87, p < 0.001), tiredness/little energy (F = 309.71, p < 0.001), little interest/pleasure (F = 289.25, p < 0.001), feeling down, depressed, hopeless (F = 159.06, p < 0.001), poor appetite or overeating (F = 175.06, p < 0.001), feeling bad about oneself (F = 83.86, p < 0.001), trouble in concentration (F = 229.75, p < 0.001) and moving/speaking slowly or fidgety/restlessness (F = 141.51, p < 0.001). Moreover, there was a significant main effect of time on resorting to alcohol/tranquilizers (F = 35.38, p < 0.001) (see Fig. 1).

Capture: Depressive symptoms during Covid-19-pandemic. Repeated measure statistic for depressive symptoms during Covid-19-pandemic. A significant interaction effect between time and ACEs was seen for PHQ total score, tiredness/little energy, little interest/pleasure, trouble in concentration and resorting to alcohol/tranquilizers
Severity of depressive symptoms in dependence of ACEs and income loss
Regarding ACEs, significant between-subject effects (in dependence of ACEs) were seen for PHQ total score (F = 71.26, p < 0.001) and the sub items sleep (F = 43.19, p < 0.001), tiredness/little energy (F = 45.65, p < 0.001), little interest/pleasure (F = 27.01, p < 0.001), feeling down, depressed, hopeless (F = 38.80, p < 0.001), poor appetite or overeating (F = 19.97, p < 0.001), feeling bad about oneself (F = 40.46, p < 0.001), trouble in concentration (F = 38.63, p < 0.001) and moving/speaking slowly or fidgety/restlessness (F = 23.42, p < 0.001). Moreover, there was a significant between-subject effect on resorting to alcohol/tranquilizers (F = 22.80, p < 0.001) (see Fig. 1).
Focusing on income loss, significant between-subject effects (in dependence of income loss) were seen for PHQ total score (F = 39.39, p < 0.001) and all assessed subitems: little interest/pleasure (F = 21.89, p < 0.001), feeling down, depressed, hopeless (F = 23.99, p < 0.001), poor sleep (F = 20.30, p < 0.001), tiredness/little energy (F = 14,85, p < 0.001), poor appetite or overeating (F = 10.22, p = 0.001), feeling bad about oneself (F = 28.55, p < 0.001), trouble in concentration (F = 15.92, p < 0.001) and moving/speaking slowly or fidgety/restlessness (F = 29.87, p < 0.001). Additionally, for resorting to alcohol/tranquilizers, there was a significant between-subject effect (F = 4.39, p = 0.036) (see supplementary material).
Change of depressive symptoms in dependence of ACEs and income loss
For ACEs, a significant interaction effect between time and ACEs was seen for PHQ total score (F = 5.075, p = 0.006 with a mean of 4.2, 5.5 and 7.2 for 0, 1–3 and ≥ 4 ACEs before the pandemic and a mean of 6.1, 7.9 and 10.0 for 0, 1–3 and ≥ 4 ACEs during the pandemic). With regard to the items of the PHQ-8, significant interaction effects emerged for tiredness/little energy (F = 4.92, p = 0.007 with a mean of 1.78, 2.03 and 2.26, for 0, 1–3 and ≥ 4 ACEs before the pandemic and a mean of 2.20, 2.45 and 2.80 for 0, 1–3 and ≥ 4 ACEs during the pandemic), little interest/pleasure (F = 4.69, p = 0.009 with a mean of 1.69, 1.79 and 1.97, for 0, 1–3 and ≥ 4 ACEs before the pandemic and a mean of 1.99, 2.20 and 2.45 for 0, 1–3 and ≥ 4 ACEs during the pandemic), trouble in concentration (F = 4.04, p = 0.018 with a mean of 1.43, 1.61 and 1.83, for 0, 1–3 and ≥ 4 ACEs before the pandemic and a mean of 1.65, 1.89 and 2.19 for 0, 1–3 and ≥ 4 ACEs during the pandemic) and resorting to alcohol/tranquilizers (F = 3.15, p = 0.043 with a mean of 1.12, 1.20 and 1.34, for 0, 1–3 and ≥ 4 ACEs before the pandemic and a mean of 1.15, 1.25 and 1.44 for 0, 1–3 and ≥ 4 ACEs during the pandemic) (see Fig. 1).
Regarding income loss, a significant interaction effect between time and income loss was seen for PHQ total score (F = 27.84, p < 0.001 with a mean of 6.43 with and 5.20 without income loss before the pandemic and a mean of 10.28 with and 7.32 without income loss during the pandemic) and all assessed subitems: little interest/pleasure (F = 17.26, p < 0.001 with a mean of 1.89 with and 1.78 without income loss before the pandemic and a mean of 2.53 with and 2.13 without income loss during the pandemic) feeling down, depressed, hopeless (F = 20.68, p < 0.001 with a mean of 1.77 with and 1.64 without income loss before the pandemic and a mean of 2.38 with and 1.96 without income loss during the pandemic), poor sleep (F = 12.98, p < 0.001 with a mean of 2.03 with and 1.85 without income loss before the pandemic and a mean of 2.56 with and 2.14 without income loss during the pandemic), tiredness/little energy (F = 11.59, p < 0.001 with a mean of 2.11 with and 2.00 without income loss before the pandemic and a mean of 2.73 with and 2.39 without income loss during the pandemic), poor appetite or overeating (F = 5.67, p = 0.017 with a mean of 1.81 with and 1.67 without income loss before the pandemic and a mean of 2.19 with and 1.91 without income loss during the pandemic), feeling bad about oneself (F = 19.71, p < 0.001 with a mean of 1.73 with and 1.49 without income loss before the pandemic and a mean of 2.06 with and 1.62 without income loss during the pandemic), trouble in concentration (F = 15.96, p < 0.001 with a mean of 1.71 with and 1.58 without income loss before the pandemic and a mean of 2.18 with and 1.83 without income loss during the pandemic), and moving/speaking slowly or fidgety/restlessness (F = 10.98, p < 0.001 with a mean of 1.37 with and 1.19 without income loss before the pandemic and a mean of 1.66 with and 1.34 without income loss during the pandemic). For resorting to alcohol/tranquilizers, there was also a significant interaction effect between time and income loss (F = 9.99, p = 0.002 with a mean of 1.23 with and 1.19 without income loss before the pandemic and a mean of 1.37 with and 1.23 without income loss during the pandemic); (see supplementary material).
Predictors for change of depressive symptoms
Results of the multiple linear regression indicated that there was a significant effect between age, sum of ACEs, systematically important work, decrease of household income, living alone, social support and pre-existing mental illness (F = 8.84, p < 0.001, R2 = 0.05) on change of depressive symptoms. At the individual level, a higher number of ACEs (t = -2.61, p = 0.009), and a decrease of household income (t = -4.08, p < 0.001) predicted an increase of depressive symptoms while age (t = 3.41, p = 0.001) and social support (t = 4.31, p < 0.001) were significant predictors for a decrease of depressive symptoms (see Table 2).
Discussion
To the best of our knowledge, this is the first study assessing the role of ACEs on the change of depressive symptoms during the Covid-19 pandemic. Importantly, the experience of adversity during childhood and/or adolescence is associated with an increase of depressive symptoms. Therefore, our results identify persons who have experienced adversity during childhood or adolescence as a risk group for mental health problems during the pandemic. This has been hypothesized before [19], as personss with ACEs have a higher sensitivity to stress and threat and lower coping abilities, resulting in a higher vulnerability to stress exposure [32, 33]. While it was shown before that ACEs are associated with higher depressive symptoms during the pandemic [10, 34] and higher post-traumatic stress symptoms if they or someone in the family, neighborhood or among friends have suffered from Covid-19 [41], this study is the first to confirm a particular vulnerability for subjects with ACEs for an increase of depressive symptoms during the current pandemic in Germany.
Besides the relevance of ACEs, our findings show an increase of depressive symptoms in all participants. This finding is in line with studies indicating an increase of depressive symptoms during the pandemic [8, 16, 42, 43]. Our findings thereby substantiate results on the mental health burden during the current pandemic.
Additionally, the data presented show that ACEs where associated with higher depressive symptoms in a dose dependent manner. This association was shown already more than 20 years ago in the famous ACE study [27] and has been confirmed also in German population representative samples [44].
In a next step, we assessed further predictors for an increase of depressive symptoms during the pandemic, were ACEs were shown to be associated with a stronger increase in depressive symptoms. In line with this finding, ACEs were shown to be associated with a stronger decrease in quality of life and general health status during the pandemic [37, 45]. Moreover, ACEs we have demonstrated that ACEs are associated with dysfunctional familiar coping strategies during the pandemic [35, 36] and a higher risk for intrafamiliar problems [35, 37, 38]. The reason for this seen higher risk of problems during the pandemic may be manifold. A higher stress-vulnerability and a decrease of emotion regulation [32, 33] was shown for individuals having experienced ACEs, potentially affecting coping of stressful situations. ACEs affect stress regulation via one main stress axis of the body, the hypothalamic–pituitary–adrenal (HPA) axis in the long-term [46]. Consequently, cortisol metabolism is known to be altered in adults who have experienced ACEs [47]. This may contribute to the higher vulnerability of persons who have experienced ACEs during the stressful times of a pandemic. In a population-based sample of the German population, a significant impact of ACEs and stressful life events during adulthood, such as, death of a loved one, was demonstrated. Nevertheless, no significant interaction was shown, meaning that ACEs did not modify the association between major stressful life events in adulthood and health [48]. However, the interplay between ACEs and stressful life events in adulthood is not well explored and should be topic of further research.
Beside ACEs, lack of social support was associated with a significant increase of depressive symptoms. Loneliness has been identified before as major mental health concern during the pandemic [12]. Living alone, on the other hand, did not predict an increase in depressive symptoms, indicating that social support is more relevant for an increase of depressive symptoms, whether someone lives alone or not.
While a systemically important work was not a significant predictor, our results show that a decrease of income is associated with a higher risk for increased depressive symptoms. The role of economic hardship on mental health has been shown numerously [49,50,51]. In a recent cross-sectional online survey in an Austrian sample, no work and low income were predictors for higher symptoms of depression and anxiety during the pandemic [16], just as discontinued working activity in an Italian sample [43] and economic stressors in a US sample [15]. ACEs are known to increase the risk for a lower household income, but also financial wellbeing and financial literacy [31]. The modifying effect of income loss on change of depressive symptoms during the pandemic was even higher compared to ACEs. This points towards the relevance of financial security for mental health during crisis such as the pandemic. However, the association between income loss and increased risk for depressive symptoms as well as an increase of depressive symptoms may be more complex. Besides the financial aspect, other factors encompassing job loss and thus loss of structure, social contacts and appreciation may play a role in the observed increase of depressive symptoms. However, as in our study besides income loss no further assessments were conducted, further studies are necessary in order to disentangle this complex field.
Gender had no significant impact on increase of depressive symptoms during the pandemic. Although depression is more frequent in females, studies assessing depression during the pandemic reveal contradicting results for the role of gender [9, 16]. However, as the number of male participants in our sample has been very low, this may impair the validity of this result. Our data reveal younger age as a significant predictor of an increase of depressive symptoms during the pandemic, which is in line with the literature [10, 52].
One major limitation of the study is that the participants cannot be considered as representative for the general public as a non-probability sample based on participation in an online survey was used. Compared to the general population in Germany, our sample comprised far more females, was younger [53], academic achievement was higher [54] and less subjects in our sample lived alone [55]. This bias may have occurred due to our ways of recruitment (our homepage, social media and print media and existing mailing lists from other studies and interested parties). These methods may have prioritized the academic, and in particular the medical field, as our homepage is a clinical one and the majority of persons on our mailing list are somehow related to the medical field As the impact of economic loss was already highly significant in our well educated sample, it can be assumed that the impact of income loss may be even more relevant in a sample with a more representative socioeconomic status. A similar bias may be assumed for ACEs. Lower education correlates with higher rates of ACEs [56, 57]. Consequently, the results in our sample may underestimate the negative impact of ACEs during the pandemic. Together, the generalizability of our findings is limited. The assessment of depressive symptoms before the pandemic are based on retrospective self-report. Importantly, recall bias was shown to diverge between depressed patients and healthy controls in a complex way [58], why the validity of the retrospectively assessed depressive symptoms prior to the pandemic is reduced. The use of retrospectively assessed ACEs is debated [59]. However, the relevance of subjective adversity for health was underlined recently [60]. In our cross-sectional study, causality cannot be deduced. Due to reasons of feasibility, some items were merged, e.g. the use of alcohol and tranquilizers. However, the presented results give a meaningful first insight into the relevance of ACEs on coping with the pandemic.
Conclusion
ACEs are a significant predictor for an increase in depressive symptoms during the pandemic, indicating that subjects with ACEs may be a risk group for mental health problems during the current and potential later pandemics. An even stronger association was found between income loss and increase of depressive symptoms. Other predictors are young age and lack of social support.
These findings underline the relevance of interventions against social isolation, economic loss and the need of mental health services during pandemics. To know about the increased risk for people with ACEs during the pandemic may help to provide more targeted support in possible scenarios due to the current or possible other pandemics. Economic stability seems to be of prior importance for mental health.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
References
Alfano V, Ercolano S. The efficacy of lockdown against covid-19: a cross-country panel analysis. Appl Health Econ Health Policy. 2020;18(4):509–17.
Vinceti M, Filippini T, Rothman KJ, Ferrari F, Goffi A, Maffeis G, et al. Lockdown timing and efficacy in controlling COVID-19 using mobile phone tracking. EClinicalMedicine. 2020;25:100457.
Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. 2020;395(10227):912–20.
Holmes EA, O’Connor RC, Perry VH, Tracey I, Wessely S, Arseneault L, et al. Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. Lancet Psychiatry. 2020;7(6):547–60.
Hossain MM, Sultana A, Purohit N. Mental health outcomes of quarantine and isolation for infection prevention: a systematic umbrella review of the global evidence. Epidemiol Health. 2020;42:e2020038.
Pfefferbaum B, North CS. Mental Health and the Covid-19 Pandemic. N Engl J Med. 2020;383(6):510–2.
Tso IF, Park S. Alarming levels of psychiatric symptoms and the role of loneliness during the COVID-19 epidemic: A case study of Hong Kong. Psychiatry Res. 2020;293:113423.
Casagrande M, Favieri F, Tambelli R, Forte G. The enemy who sealed the world: effects quarantine due to the COVID-19 on sleep quality, anxiety, and psychological distress in the Italian population. Sleep Med. 2020;75:12–20.
Huang Y, Zhao N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: a web-based cross-sectional survey. Psychiatry Res. 2020;288:112954.
Prout TA, Zilcha-Mano S, Aafjes-van Doorn K, Békés V, Christman-Cohen I, Whistler K, et al. Identifying predictors of psychological distress during COVID-19: a machine learning approach. Front Psychol. 2020;11: 586202.
WHO. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789–858.
Killgore WDS, Cloonan SA, Taylor EC, Dailey NS. Loneliness: A signature mental health concern in the era of COVID-19. Psychiatry Res. 2020;290: 113117.
Li Y, Zhao J, Ma Z, McReynolds LS, Lin D, Chen Z, et al. Mental Health Among College Students During the COVID-19 Pandemic in China: A 2-Wave Longitudinal Survey. J Affect Disord. 2020;281:597–604.
Li TW, Lee TM, Goodwin R, Ben-Ezra M, Liang L, Liu H, et al. Social Capital, Income Loss, and Psychobehavioral Responses amid COVID-19: A Population-Based Analysis. Int J Environ Res Public Health. 2020;17(23):8888.
Ettman CK, Abdalla SM, Cohen GH, Sampson L, Vivier PM, Galea S. Low assets and financial stressors associated with higher depression during COVID-19 in a nationally representative sample of US adults. J Epidemiol Community Health. 2020.
Pieh C, Budimir S, Probst T. The effect of age, gender, income, work, and physical activity on mental health during coronavirus disease (COVID-19) lockdown in Austria. J Psychosom Res. 2020;136: 110186.
Sheridan Rains L, Johnson S, Barnett P, Steare T, Needle JJ, Carr S, et al. Early impacts of the COVID-19 pandemic on mental health care and on people with mental health conditions: framework synthesis of international experiences and responses. Soc Psychiatry Psychiatr Epidemiol. 2020.
Hao F, Tan W, Jiang L, Zhang L, Zhao X, Zou Y, et al. Do psychiatric patients experience more psychiatric symptoms during COVID-19 pandemic and lockdown? A case-control study with service and research implications for immunopsychiatry. Brain Behav Immun. 2020;87:100–6.
Fegert JM, Vitiello B, Plener PL, Clemens V. Challenges and burden of the Coronavirus 2019 (COVID-19) pandemic for child and adolescent mental health: a narrative review to highlight clinical and research needs in the acute phase and the long return to normality. Child Adolesc Psychiatry Ment Health. 2020;14:20.
Norman RE, Byambaa M, De R, Butchart A, Scott J, Vos T. The long-term health consequences of child physical abuse, emotional abuse, and neglect: a systematic review and meta-analysis. PLoS Med. 2012;9(11): e1001349.
Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study. Am J Prev Med. 1998;14(4):245–58.
Clemens V, Huber-Lang M, Plener PL, Brahler E, Brown RC, Fegert JM. Association of child maltreatment subtypes and long-term physical health in a German representative sample. Eur J Psychotraumatol. 2018;9(1):1510278.
Rehkopf DH, Headen I, Hubbard A, Deardorff J, Kesavan Y, Cohen AK, et al. Adverse childhood experiences and later life adult obesity and smoking in the United States. Ann Epidemiol. 2016;26(7):488-92.e5.
Gilbert R, Widom CS, Browne K, Fergusson D, Webb E, Janson S. Burden and consequences of child maltreatment in high-income countries. Lancet. 2009;373(9657):68–81.
Clemens V, Berthold O, Witt A, Sachser C, Brähler E, Plener PL, et al. Child maltreatment is mediating long-term consequences of household dysfunction in a population representative sample. Eur Psychiatry. 2019;58:10–8.
Clemens V, Berthold O, Witt A, Sachser C, Brähler E, Plener PL, et al. Lifespan risks of growing up in a family with mental illness or substance abuse. Sci Rep. 2020;10(1):15453.
Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: the adverse childhood experiences (ACE) study. Am J Prev Med. 1998;14(4):245–58.
Karatekin C, Ahluwalia R. Effects of adverse childhood experiences, stress, and social support on the health of college students. J Interpers Violence. 2020;35(1–2):150–72.
Cheong EV, Sinnott C, Dahly D, Kearney PM. Adverse childhood experiences (ACEs) and later-life depression: perceived social support as a potential protective factor. BMJ Open. 2017;7(9): e013228.
Sheikh MA, Abelsen B, Olsen JA. Clarifying Associations between Childhood Adversity, Social Support, Behavioral Factors, and Mental Health, Health, and Well-Being in Adulthood: A Population-Based Study. Front Psychol. 2016;7:727.
Harter CL, Harter JFR. The link between adverse childhood experiences and financial security in adulthood. J Fam Econ Issues. 2021;9:1–11.
Hein TC, Monk CS. Research Review: Neural response to threat in children, adolescents, and adults after child maltreatment - a quantitative meta-analysis. J Child Psychol Psychiatry. 2017;58(3):222–30.
Duffy KA, McLaughlin KA, Green PA. Early life adversity and health-risk behaviors: proposed psychological and neural mechanisms. Ann N Y Acad Sci. 2018;1428(1):151–69.
Kim AW, Nyengerai T, Mendenhall E. Evaluating the mental health impacts of the COVID-19 pandemic: perceived risk of COVID-19 infection and childhood trauma predict adult depressive symptoms in urban South Africa. Psychol Med. 2020:1–13.
Clemens V, Beschoner P, Jarczok MN, Weimer K, Kempf M, Morawa E, et al. The mediating role of COVID-19-related burden in the association between adverse childhood experiences and emotional exhaustion: results of the egePan - VOICE study. Eur J Psychotraumatol. 2021;12(1):1976441.
Köhler-Dauner F, Clemens V, Hildebrand K, Ziegenhain U, Fegert JM. The interplay between maternal childhood maltreatment, parental coping strategies as well as endangered parenting behavior during the current SARS-CoV-2 pandemic. Developmental Child Welfare. 2021;3(2):71–84. https://doi.org/10.1177/25161032211014899.
Clemens V, Köhler-Dauner F, Ziegenhain U, Fegert JM. Predictors of parental coping during the covid-19 pandemic: a survey in Germany. Front Psychol. 2021;12:715327.
Sachser C, Olaru G, Pfeiffer E, Brähler E, Clemens V, Rassenhofer M, et al. The immediate impact of lockdown measures on mental health and couples’ relationships during the COVID-19 pandemic - results of a representative population survey in Germany. Soc Sci Med. 2021;278:113954.
Wingenfeld K, Schäfer I, Terfehr K, Grabski H, Driessen M, Grabe H, et al. Reliable, valide und ökonomische Erfassung früher Traumatisierung: Erste psychometrische Charakterisierung der deutschen Version des Adverse Childhood Experiences Questionnaire (ACE). Psychother Psych Med. 2011;61(01):e10–4.
Kroenke K, Strine TW, Spitzer RL, Williams JBW, Berry JT, Mokdad AH. The PHQ-8 as a measure of current depression in the general population. J Affect Disord. 2009;114(1):163–73.
Guo J, Fu M, Liu D, Zhang B, Wang X, van IJzendoorn MH. Is the psychological impact of exposure to COVID-19 stronger in adolescents with pre-pandemic maltreatment experiences? A survey of rural Chinese adolescents. Child Abuse Negl. 2020;110(Pt 2):104667.
Bäuerle A, Steinbach J, Schweda A, Beckord J, Hetkamp M, Weismüller B, et al. Mental Health Burden of the COVID-19 outbreak in Germany: predictors of mental health impairment. J Prim Care Community Health. 2020;11:2150132720953682.
Rossi R, Socci V, Talevi D, Mensi S, Niolu C, Pacitti F, et al. COVID-19 pandemic and lockdown measures impact on mental health among the general population in Italy. Front Psychiatry. 2020;11:790.
Witt A, Sachser C, Plener PL, Brähler E, Fegert JM. The prevalence and consequences of adverse childhood experiences in the German population. Dtsch Arztebl Int. 2019;116(38):635–42.
Klein S, Fegert JM, Geprägs A, Brähler E, Clemens V. The impact of the COVID-19 pandemic on health, quality of life and intrafamilial relations - a population-based survey in Germany. Front Psychol. 2022;13: 844057.
Bunea IM, Szentágotai-Tătar A, Miu AC. Early-life adversity and cortisol response to social stress: a meta-analysis. Transl Psychiatry. 2017;7(12):1274.
Marques-Feixa L, Palma-Gudiel H, Romero S, Moya-Higueras J, Rapado-Castro M, Castro-Quintas Á, et al. Childhood maltreatment disrupts HPA-axis activity under basal and stress conditions in a dose-response relationship in children and adolescents. Psychol Med. 2021:1–14.
Clemens V, Bürgin D, Huber-Lang M, Plener PL, Brähler E, Fegert JM. The Interplay between child maltreatment and stressful life events during adulthood and cardiovascular problems-a representative study. J Clin Med. 2021;10(17):3937.
Sareen J, Afifi TO, McMillan KA, Asmundson GJG. Relationship between household income and mental disorders: findings from a population-based longitudinal study. Arch Gen Psychiatry. 2011;68(4):419–27.
Wickrama KA, Surjadi FF, Lorenz FO, Conger RD, Walker C. Family economic hardship and progression of poor mental health in middle-aged husbands and wives. Fam Relat. 2012;61(2):297–312.
Fegert J, Harsch D, Koelch M. Poverty hits children first? A child and adolescent psychiatry perspective on effects of the economic crisis. Psychiatrie. 2017;14:67–74.
Qiu J, Shen B, Zhao M, Wang Z, Xie B, Xu Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: implications and policy recommendations. Gen Psychiatr. 2020;33(2):e100213-e.
Statista. Bevölkerung - Verteilung der Einwohner in Deutschland nach relevanten Altersgruppen am 31. Dezember 2019 https://de.statista.com/statistik/daten/studie/382409/umfrage/verteilung-der-bevoelkerung-deutschlands-nach-altersgruppen/2020
Statista. Bildungsstand https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Bildung-Forschung-Kultur/Bildungsstand/_inhalt.html2020
Statista. 42 % der Alleinlebenden wohnten 2019 in Großstädten https://www.destatis.de/DE/Presse/Pressemitteilungen/2020/11/PD20_N073_122.html2020
Kotch JB, Browne DC, Ringwalt CL, Stewart PW, Ruina E, Holt K, et al. Risk of child abuse or neglect in a cohort of low-income children. Child Abuse Negl. 1995;19(9):1115–30.
Berthold O, Clemens V, Witt A, Brahler E, Plener PL, Fegert JM. Awareness of abusive head trauma in a German population-based sample: implications for prevention. Pediatr Res. 2019;86(4):537–41.
Ben-Zeev D, Young MA. Accuracy of hospitalized depressed patients’ and healthy controls’ retrospective symptom reports: an experience sampling study. J Nerv Ment Dis. 2010;198(4):280–5.
Baldwin JR, Reuben A, Newbury JB, Danese A. Agreement between prospective and retrospective measures of childhood maltreatment: a systematic review and meta-analysis. JAMA Psychiat. 2019;76(6):584–93.
Danese A, Widom CS. Objective and subjective experiences of child maltreatment and their relationships with psychopathology. Nat Hum Behav. 2020;4(8):811–8.
Acknowledgements
We thank all participants of the survey.
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
VC interpreted the data and wrote the manuscript. UZ supported conceptualized the survey and recruitment of the sample. FKD supported recruitment of the sample and manuscript drafting. FK supported data analyses. JF conceptualized the survey and supervised data analyses. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Electronic informed consent was obtained from each participant prior to starting the survey. Information on the study and data analysis were given. Participation was voluntary and anonymous. Participants could withdraw from the survey at any moment without providing any justification. The study was conducted in accordance with the Declaration of Helsinki. After consultation with the ethics committee of the University of Ulm, the committee officially stated that there is no requirement for an ethics vote due to the anonymous character of the study: “I can now inform you that no ethics application is necessary for this. We will therefore not make a substantive statement or evaluation from the point of view of professional law or ethics. A file number will not be assigned. This e-mail complies with the written form as defined in § 126 para. 3 BGB (German Civil Code). You can use it as proof in the event of any enquiries by for an ethics vote by scientific journals, authorities or third-party funders.”
Consent for publication
Not applicable.
Competing interests
VC, FK, FKD and UZ declare that they have no competing interests.
JMF has received research funding from the EU, DFG (German Research Foundation), BMG (Federal Ministry of Health), BMBF (Federal Ministry of Education and Research), BMFSFJ (Federal Ministry of Family, Senior Citizens, Women and Youth), G-BA Innovationsfonds, several state ministries, State Foundation Baden-Württemberg, Volkswagen Foundation, Porticus Foundation, Diocese of Rottenburg-Stuttgart. Moreover, he received travel grants, honoraria and sponsoring for conferences and medical educational purposes from APK, Deutschlandfunk, DFG, DJI, DKSB, Infectopharm, med update, UNICEF, several universities, professional associations, political foundations, and German federal and state ministries during the last 5 years. Professor Fegert holds no stocks of pharmaceutical companies.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Clemens, V., Köhler-Dauner, F., Keller, F. et al. Adverse childhood experiences are associated with a higher risk for increased depressive symptoms during Covid-19 pandemic – a cross-sectional study in Germany. BMC Psychiatry 22, 540 (2022). https://doi.org/10.1186/s12888-022-04177-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-022-04177-7