
Abstract
Background
Emotional and stress-related disorders show high incidence, prevalence, morbidity, and comorbidity rates in Mexico. In recent decades, research findings indicate that cognitive behavioral interventions, from a disorder-specific perspective, are the effective front-line treatment for anxiety and depression care. However, these treatments are not often used. Reasons include limited access and low availability to effective interventions and comorbidity between mental disorders. Emotional deregulation of negative affectivity has been found to be a mediating factor in addressing emotional disorders from a transdiagnostic perspective, aimed at two or more specific disorders. In addition, technological advancement has created alternatives for psychological assistance, highlighting the possibilities offered by technologies since Internet-supported intervention programs have been empirically tested for effectiveness, efficiency and efficacy and can be key to ensuring access to those who are inaccessible. The aim of the study is to evaluate the efficacy, moderators of clinical change and acceptability of a transdiagnostic guided Internet-delivered intervention versus a transdiagnostic self-guided Internet-delivered intervention for emotional, trauma and stress-related disorders, and waiting list in community sample.
Methods
A three-armed, parallel group, superiority randomized controlled clinical trial with repeated measurements at four times: pretest, posttest, follow-up at 3, 6 and 12 months. Outcomes assessor, participant, care provider and investigator will be blinded. Participants aged 18 to 70 years will be randomly allocated 1:1:1 to one of three study arms: a) Transdiagnostic guided internet-delivered intervention with synchronous assistance, b) Transdiagnostic self-guided internet-delivered intervention, c) Waiting list group. Based on sample size estimation, a minimum of 207 participants (69 in each intervention group) will be included.
Discussion
The study could contribute to improving the efficacy of transdiagnostic internet-delivered interventions to promote the dissemination of evidence-based treatments and eventually, to decrease the high prevalence of emotional and trauma-related disorders in the Mexican population.
Trial registration
ClinicalTrial.gov: NCT05225701. Registered February 4, 2022.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Background
Globally, mental disorders are a serious public health problem with a high social cost that affects people regardless of age, sex, socioeconomic status, or culture [1]. In particular, Emotional Disorders (ED), defined as anxiety and mood disorders (unipolar depression), have been identified as the main causes of psychological disability [2], due to their high prevalence, morbidity and comorbidity. In this regard, the Pan American Health Organization (PAHO) revealed high prevalence estimates for anxiety disorders (28.8%) and mood disorders (20.8%), with comorbidity rates ranging from 40 to 80% [3]. In Mexico, the last National Survey of Psychiatric Epidemiology, in 2003 reported that among the most common disorders of the population are those related to anxiety (14.3%) [4]; while depression accounts for 4.3% of the overall burden of mental disorders [3]. Thus, the impact on the health of the general population, and in particular the Mexican population, lies not only in statistics, but also in the emotional and economic consequences when considering the detrimental effects in the functioning of the person within the family, social and labor spheres, limiting possibilities for personal development and quality of life.
Individuals suffering from depression are more likely to develop comorbidity with other mental disorders. An estimated 53% have concurrent symptomatology with some anxiety disorder [5]. Stress and traumatic events are among the most relevant causes, between 60 and 80%, contributing to the etiology of EDs. Depression and anxiety have also been deemed to create a condition of greater disability by increasing the severity and chronicity rate of psychological discomfort and is associated with increased mortality in medical conditions such as heart disease, chronic-degenerative or psychiatric conditions [6]. In Mexico, one in four people between the age of 18 and 65 have experienced at some point in their lives an ED, but only one in five of those with it receive treatment and the time to receive care in a health center ranges from four to 20 years depending on the reason for consultation [6].
In recent decades, cognitive behavioral interventions (e.g., cognitive restructuring, exposure therapy, anxiety management techniques, cognitive therapy), from a disorder-specific perspective, constitute an effective and first-line treatment for anxiety and depression care [7, 8]. However, they are not often used [9] because of the following reasons: limited access and low availability to effective interventions, a minority of people actively seek psychological care because of their own distress condition, fearing social stigma, geographical barriers that separate them from health centers, time availability, preference for other treatment or self-help, high treatment costs, which makes it inaccessible and unaffordable to both, the user and the public health system [6]. It has also been stated that the comorbidity between mental disorders as well as the gap between research findings and clinical practice could influence the poor dissemination of effective treatments and contribute to a lack of up-to-date professionals providing relevant interventions [10]. This has motivated studies aimed at knowing the moderating, mediating variables and psychological mechanisms that improve the process of clinical change [11]. In addition, the need to implement innovative solutions that contribute to the dissemination of effective treatments for the care of EDs has been raised [8]. In particular, emotional deregulation of negative affection is a factor of interest in research that is providing relevant data for better understanding and approaching EDs from a transdiagnostic perspective, a term coined from a dimensional conception to designate effective treatments targeting two or more specific disorders [12].
In this regard, Barlow returns to the tripartite theory of emotion [13] and proposes a unified transdiagnostic behavioral cognitive protocol for the treatment of EDs with an emphasis on emotional regulation [14]. The Unified Protocol for the Treatment of Emotional Disorders [UP] addresses four main components to decrease emotional dysregulation: emotional avoidance, promotion of cognitive flexibility, exposure to avoided situations and sensations, and emotional awareness focused on the present. UP has shown its effectiveness not only in achieving the decrease in target symptomatology, but also increases attendance at therapeutic sessions compared to conventional psychological interventions [15]. In addition, some meta-analyses have been performed which reveal the effectiveness of transdiagnostic protocols for anxiety disorders [16], and for anxiety and/or depression [17].
In recent years there has been an increase in initiatives aimed at the promotion and intervention in mental health mediated by technology that has favored access and dissemination of effective interventions regardless of distance, physical and social barriers [18]. Currently, internet- delivered psychological interventions can reduce the time of contact between patient and therapist and reaching people who would not otherwise receive treatment [19]. Evidence suggests that Internet-based treatments are effective for the treatment of depression, anxiety, substance abuse and eating disorders [20]. In addition, meta-analysis data reveal that these interventions are as effective as face-to-face treatments [21]. Internet-delivered interventions can be classified into: treatments administered by the therapist, treatments with minimum assistance from the therapist, and fully self-applied treatments [22].
In this sense, there is evidence of effective transdiagnostic internet-delivered interventions focusing on the emotion enhance the scope and impact of psychological treatment programs for emotional disorders [5, 23, 24]. However, there is incipient research into the efficiency of transdiagnostic Cognitive Behavioral Treatments (CBT) via the Internet for Trauma and Stress-related Disorders. Some studies have documented the effectiveness of computer-based interventions showing significant changes in anxiety reduction, presenting moderate effect sizes (g = 0.78) and large effect sizes in cases of depression (g = 0.84) [7, 25, 26]. Other studies that have investigated the efficacy of transdiagnostic CBT provided over the Internet in cases with concurrent symptomatology of anxiety and depression; have found moderate to large effects for both depression and anxiety (anxiety: g = 0.82, 95% CI: 0.58 to 1.05; depression: g = 0.79; 95% CI: 0.59–1.00) compared to control groups that included waiting list. However, there are few controlled clinical studies investigating the effects of transdiagnostic treatment via the Internet for ED adapted to the Mexican context and culture.
Evidence of the effectiveness of preventive and/or remedial interventions over the Internet in the context of public health for the reduction of the incidence of depressive and anxious symptomatology is still low; the latest systematic review identified seven uncontrolled clinical studies that evaluated the effect of Internet-mediated interventions with positive results [11]. However, only one clinical study aimed at preventing general anxiety was found, and it did not produce significant results [27], while three studies managed to reduce the incidence of depression [28, 29]. In the study conducted by Dear et al., the authors reported that the self-applied Internet-guided intervention decreased depressive symptomatology in a group of adults and managed to reduce the risk of chronic depression by 39% per follow-up year [29]. Recent research on the effectiveness of self-applied interventions via the Internet with and without the support of a trained psychologist has indicated that fully self-applied technology-mediated treatments show fewer rates of improvement compared to those who did have synchronous support with a therapist [30]. Other studies that have researched the influence of support or guidance during self-applied Internet-based interventions have reported that participants who received weekly support significantly improved in reducing depression compared to a waiting list group, while participants who did not receive support by a psychotherapist did not show significant improvement [31]. However, some authors propose that the differences in results obtained between guided and non-guided interventions are small or non-existent [32]. This aspect is relevant for assessing the efficiency of interventions provided with technology, as they could benefit more people who need it. In general, research findings available in the literature are promising; however, it is also important to note that most studies have been conducted in the Anglo-Saxon or Spanish populations. Hence it becomes necessary to know the results in controlled studies in the Mexican context and culture and with larger samples to reach stronger conclusions regarding the effectiveness and efficiency of transdiagnostic Internet-delivered interventions for the care of EDs.
In Mexico, research in this area is incipient, emphasizing the need to go beyond traditional face-to-face interventions and to design new intervention strategies. In this regard, the possibilities offered by technologies are highlighted since Internet-supported intervention programs have been empirically tested to achieve effectiveness and efficiency/cost–benefit and can be key to ensuring access to those who are inaccessible.
Finally, most of the research that has documented efficacy of transdiagnostic treatments have excluded PTSD from the research, a disorder which continues to be in Mexico more and more prevalent, related to migration, earthquakes, and violence [33]. Transdiagnostic interventions have been used on anxiety and now stress and trauma disorders correspond to a new DSM5 category, and as Gutber et al. [34] underlies, there is a need for trials so we can understand how the transdiagnostic model works with specific symptoms related to PTSD.
Aims
The primary aim of the study is to evaluate the efficacy and acceptability of a transdiagnostic guided Internet-delivered intervention versus a transdiagnostic self-guided Internet-delivered intervention for emotional, trauma and stress-related disorders, and a waiting list in a Mexican community sample. The second aim is to examine the moderator of clinical change, particularly emotional regulation, in the transdiagnostic Internet-delivered intervention for emotional, trauma and stress-related disorders.
Hypothesis
-
The transdiagnostic guided Internet-delivered intervention will show statistical greater gains in reducing symptoms of anxiety/depression/acute or post-traumatic stress and a more clinically significant improvement compared to the transdiagnostic self-guided Internet-delivered intervention and waiting list groups.
-
The transdiagnostic self-guided Internet-delivered intervention will reduce symptoms of anxiety/depression/acute or post-traumatic stress compared to a waiting list group.
-
A higher acceptance/satisfaction rate reported by participants in transdiagnostic guided Internet-delivered intervention will be found compared to the transdiagnostic self-guided Internet-delivered intervention.
-
Emotional Regulation will be a moderating variable for clinical change.
-
Changes will be maintained three, six and 12 months after the end of the intervention program with and without synchronous psychological support.
Methods
Study design
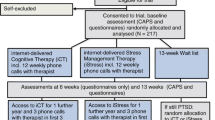
A three-armed, parallel group, superiority randomized controlled clinical trial with repeated measurements at four times: pretest, posttest, follow-up at three, six and 12 months. Outcomes assessor, participant, care provider and investigator will be blinded. Participants aged 18 to 70 years will be randomly allocated 1:1:1 to one of three study arms: a) Transdiagnostic guided Internet-delivered intervention with synchronous assistance, b) Transdiagnostic self-guided Internet-delivered intervention, c) Waiting list group. This study will follow the CONSORT statement [35] and the SPIRIT guidelines [36]. The study’s trial registration number is ClinicalTrials.gov NCT05225701. Figure 1 shows the flow chart of the study design.

Shows the flow chart of the study design
Participants
Sampling: non probabilistic, convenience sampling will be performed. Participants aged 18 to 70 years.
Eligibility criteria
Inclusion criteria: a) be of legal age; b) voluntarily participate in the study; c) meet diagnostic criteria for emotional disorders (anxiety/depression) and trauma, stress-related disorders in accordance with the International Neuropsychiatric Interview- Mini, version 5.0 [37], and show a score ≤ 25 in Beck’s Anxiety Depression Inventory [38] and/or ≤ 30 in the Beck-BDI-II Depression Inventory [39]; d) have access to computer equipment with an Internet connection; e) have a valid email address; f) have basic digital skills in the use of an operating system and Internet browsing.
Exclusion criteria: a) psychotic disorder; b) alcohol and drug abuse; c) medical condition whose severity or characteristics prevent the intervention; d) be receiving psychological and/or pharmacological treatment during the study.
Elimination criteria: a) not accepting the conditions of informed consent and b) absence on web or mobile platforms for more than 15 days or having missed two consecutive sessions of synchronous treatment sessions.
Recruitment procedure
Recruitment of participants will be carried out through advertisements in digital media (institutional website, thematic forums), as well as through dissemination on social networks. The Transdiagnostic Internet-delivered intervention program will be aimed at adults who will be able to connect via the Internet from anywhere in Mexico. Potential participants will be contacted via telephone calls or emails. The research coordinator will provide the participants with the information about the nature of the study and clarify doubts. Participants will be asked for their consent to participate. Independent evaluators will determine the suitability of participants to be included in the study based on the initial synchronous interview (via videoconference or telephone) and the self-reports related to the selection criteria that will be available in digital format on the web platform.
Ethics approval and consent to participate
The project is supported by the Ethics Committee of the Faculty of Higher Studies Iztacala at National Autonomous University of Mexico (CE/FESI/082020/1363). The development of the study will strictly adhere to the guidelines expressed in the Mexican Psychologist’s Code of Ethics [40] and the ethical standards that apply to traditional clinical practice and recommendations for online psychotherapy will be observed [41]. The therapist will protect the patient’s confidentiality and interaction records during the therapeutic process. All participants must sign an informed consent form and the rights to the confidentiality and privacy of personal data will be respected. The participant’s personal data will be encrypted through a standard algorithm and accessed only by the principal investigator.
Randomization and blinding
Participants who meet the inclusion criteria for the study will be randomly assigned to one of the study conditions. Randomization will be performed by an independent researcher unaware of the study characteristics through online open software [42] in a 1:1:1 ratio per block saturation of 12 per condition. The coordinator will inform the patient of their participation in the study and, depending on the characteristics of the study design condition, the user will be assigned to the self-guided/ guided intervention. Participants in the waiting list control group will receive the access data needed to complete the intervention 8 weeks after randomization and will be assigned to the intervention that has shown greater efficiency and user satisfaction. All participants may withdraw from treatment at any time.
Outcome’s assessor, participant and investigator will be blinded. The researcher who administers baseline assessments will be blind to the patients’ treatment group. This researcher will be different from the one who administers the other measures throughout the study.
Participant timeline an outcomes assessment
Clinical evaluation of program users will be carried out at five times (pre-post and three, six and 12 months after treatment). The instruments covered by the evaluation protocol are aimed at obtaining information necessary to assess whether the change, in addition to having statistical relevance, presents clinical significance and social validation of psychological intervention, allowing to analyze the factors (procedures, goals and results) that will influence the degree of patient satisfaction with respect to the treatment used. Table 1 provides an overview of the measures used at each time point.
Diagnosis interview
International Neuropsychiatric Interview, Version 5.0.0 (MINI) [43]. It is a structured diagnostic interview. It includes major psychiatric disorders of DSM-IV-R and IDS-10. The Spanish version of Heinze [44] presents a reliability with Kappa de > 0.75.
Symptom checklist (SCL-90). Screening instrument to identify symptoms of various psychopathologies. It is made up of 90 items that make up nine dimensions: Somatization, obsessive–compulsive, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoia, and psychoticism [45]. Cronbach’s Alpha of all subscales greater than 0.7.
Primary outcome measures
Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5) [46]. This instrument describes the symptoms of post-traumatic stress taking into consideration the diagnostic criteria of activation, alterations, avoidance and reexperimentation. It has 20 items that are scored on a Likert-type scale that goes from 0 (not at all) to 4 (totally). In its adaptation to the Mexican population, the psychometric properties of the scale show adequate internal consistency with an alpha of 0.97, as well as an appropriate convergent validity (rs = 0.58 to 0.88) [47]. Items are scored on a Likert scale ranging from 0 to 4, where higher scores indicate more pronounced PTSD symptoms. A cut-off score of 33 was suggested to have a partial diagnosis of PTSD.
Beck’s Anxiety Inventory (BAI) [48]. Self-administered instrument consisting of 21 questions that determine the severity of symptomatic and behavioral categories of anxious symptomatology present in an individual by means of a four-point scale (0 to 3), where 0 indicates the absence of the symptom, and 3 its maximum severity. These categories correspond to the symptoms that are usually included to make the diagnosis of an anxiety disorder. Previous studies suggest that it is a measure with high internal consistency and construct, divergent and convergent validity [49].
Beck Depression Inventory (BDI-II) [50]. Consists of 21 items that fundamentally evaluate the clinical symptoms of melancholy and the intrusive thoughts present in depression. Among depression measures, it is the one with the highest percentage of cognitive items presented, which is in line with Beck’s cognitive theory of depression. Validated Mexican version of the BDI [51] and for version II (α = 87-0.92) [52].
Secondary outcome measures
Scale of Difficulties in Emotional Regulation (DERS) [53]. It is a self-applied instrument that measures two dimensions through 15 items, emotional regulation strategies and awareness of emotions. The version validated in Mexican population by De la Rosa et al. [54], presents a Cronbach’s Alpha valued between 0.84—0.74.
General Anxiety and the Impairment Severity Scale (OASIS) [55]. It consists of five questions within a scale of 0 to 4, which measures frequency, severity, and avoidance of anxiety in different fields: work / academic interference / family, and deterioration of social and daily life. It has good internal consistency (α = 0.80) and test–retest reliability (k = 0.82). The Spanish language version confirmed the factorial structure and reliability and validity data obtained by the original authors: internal consistency in both populations, in general and clinical (α = 0.86) and test-fail reliability (k = 0.84) [56].
General Depression and the Impairment Gravity Scale (ODSIS) [57]. This scale evaluates experiences related to depression. It consists of five items with different answer options ranging from 0 to 4 for each item. It measures the frequency and severity of depression, as well as the level of avoidance to work/academic/home interference, and social life. In the Spanish language version, the internal consistency has proven to be excellent, with a Cronbach alpha between 0.91 and 0.94 and a good convergent and discriminatory validity [56].
Opinion measures
Opinion on Treatment [58, 59]. This is measured by means of four questions that inform on the level of satisfaction with treatment, (for example “I would recommend treatment to a friend or family member, treatment is considered useful for your case and if you think the treatment was difficult to manage or aversive. On a scale of 1 (nothing) to 10 (very much).
Usability Scale (SUS) [60]. Measures the usability of a tool, computer program, instrument, etc. It consists of 10 items within a five-point scale, where the 1 is totally at odds and 5 totally agree.
The measures included in the evaluation protocol will be delivered online, except for the mini-Interview, which will be conducted by videoconference or / by telephone by an evaluator.
Interventions
Transdiagnostic guided Internet-delivered intervention with synchronous assistance (UP- guided)
Is an Internet-delivered intervention based on a manualized unified protocol for the transdiagnostic treatment for emotional disorders (to anxiety and mood disorders -unipolar depression-) and derived from stress and trauma disorders structured in a therapist handbook and a patient handbook [61]. The unified protocol incorporates psychological techniques that have proven their effectiveness [14] and includes the following therapeutic modules: 1) motivation for change, understanding emotions, recognition and observation of emotional response; 2) learning to observe experiences, evaluation and re-evaluation of thoughts; 3) what is emotional avoidance, emotion and behavior, and awareness and tolerance of physical sensations; 4) emotional exposure to physical sensations and situations and achievements, maintenance and prevention of relapses.
E-moción is a self-applied treatment web system (web/mobile app) based on a transdiagnostic approach for emotional, stress and trauma-derived disorders organized into eight sequential modules (see Table 2), it takes about eight to 12 weeks to complete it. All the modules present the same structure: Module 0. Pre-evaluation, Module 1. Psychoeducation and motivation for change (e.g., understanding emotional reactions to stressors), Module 2. Emotional Coping Skills (p. e.g., emotional regulation), Module 3. Acceptance and awareness-raising skills focused on the present moment (e.g., mindfulness, metaphors); Module 4 and 5 Cognitive coping skills (e.g., cognitive re-evaluation, cognitive flexibility); Module 6 and 7. Behavioral coping skills (e.g., exposure to emotional experiences), Module 8. Achievements, maintenance, and prevention of relapses; Module 9. Post-evaluation. The Internet-delivered treatment program is compatible with desktop devices (PC/Mac), tablet or mobile phone, and will allow participants to access the intervention modules from anywhere and at their own pace. Participants will be encouraged to advance one module per week. The program also sends text messages with motivational content to remind participants to access their modules. Each module includes exercises and tasks for the practice of each technique.
Synchronous assistance and psychological counseling
To monitor the participant’s progress, each user will be assigned an advisor who will be a health personnel (psychologists) to get a weekly personalized videoconferencing assistance and psychological counseling. The support will be provided by experienced psychologists who will have at least a bachelor’s degree in Clinical Psychology. Before taking part in the trial, they will receive training on the transdiagnostic unified protocol and training in telepsychology to ensure that everyone provides the same support. The role of the psychological advisor is to motivate, guide and listen to the doubts and comments of each participant during one-hour individual online weekly sessions.
Transdiagnostic self-guided Internet delivered intervention (UP- unguided)
Self-applied treatment web system based on a transdiagnostic approach for emotional and stress and trauma-derived disorders. The system will contain eight modules (Table 2). The duration of the intervention program may vary between users; however, the participant will have access permits for a maximum period of 12 weeks. To monitor the participant’s progress, at the end of each intervention module, the user will be asked to answer two brief questionnaires to assess anxiety and depression (OASIS, ODSIS). All modules are sequential, allowing the user to go step by step. This arm does not have personalized online assistance.
Under both conditions of intervention, automatic emails with notifications will be sent out to prompt participants to access the intervention if they have not entered within the last 15 days.
Waiting list control group (WL)
Participants on the waiting list group will be offered the intervention after two months and will join the Transdiagnostic guided Internet-delivered intervention with synchronous assistance.
Statistical analysis
Data management
The requested Personal Data will be processed for research, teaching, and statistical purposes. They will be protected through a code (folio) that guarantees their confidentiality. Access to the data will be limited to the main researcher of the study and the institutional server management technician. Likewise, the data will be kept during the study and once completed, will be kept for an additional period of up to five years to subsequently be eliminated to avoid improper treatment of the same. The information provided through the web and mobile application will be treated with all appropriate security measures, in accordance with the principles contained in the Mexican Federal Law on Protection of Personal Data Held by Private Parties, its Regulations and the Guidelines of the Privacy Notice of the United Mexican States.
Sample size
For the calculation of the sample size, suggestions reported in the scientific literature regarding the size of the effect in controlled clinical studies where they tested the effectiveness of transdiagnostic interventions for anxiety and depression via online platforms were considered. Cohen’s d index will be used for this study, as it will be assumed that the variances of the three groups will be homogeneous, otherwise the Hedges g-index would be used. In addition, for the calculation of the sample size, since the study will include 3 experimental conditions a One-way ANOVA will be performed for comparison between 3 groups. A conservative approach was adopted and an average magnitude effect size of 0.25 (Cohen’s d) (equivalent to g × 0.5), a significance level (α) of 0.05 (p < 0.05, 95% confidence) and a conventional statistical power of 80% (1- β 0.8). For a priori analysis, GPower*v3.1.6 software [62] was used and a required sample size of 159 participants (53 per group) was obtained. However, an additional 30% of participants will be recruited keeping in mind attrition rates, as reported in the literature on internet treatments [63, 64]. Thus, the required sample size is estimated to include 207 participants in total (69 participants per group).
Statistical analysis plan
Descriptive analyses will be carried out to characterize the study sample according to demographic variables: age, sex, occupation, residence, etc. Experimental condition abandonment data associated with diagnosis, intensity of clinical symptoms and sociodemographic characteristics shall be considered. For the analysis of indicators of psychopathology, the intensity of symptomatology, duration of the disorder in months, comorbidity with other psychological problems will be reviewed. To ascertain the homogeneity / heterogeneity in demographic and diagnostic variables that could affect the effectiveness of the study among the two internet-delivered treatment groups (UP-guided vs UP-unguided) and the control group (WL), a statistical analysis will be performed before the intervention. The analysis of the data will be carried out with the SPSS statistical package in its latest version. It will be calculated for categorical and continuous variables, the One-way ANOVA. The results shall be presented in three sections: a) contrast analyses to measure the effectiveness of interventions, with specific measures of anxiety, depression, and trauma-stress symptomatology analyzed before and after the online treatment; b) analysis for moderating variable (emotional regulation), and c) acceptance/satisfaction and usability measures of the online intervention. To determine the effectiveness of the intervention program, an analysis of repeated measures variance will be computed through the SPSS statistical program, which will compare the pretest measures against posttest measures under the three experimental conditions. The results will be controlled by performing effect size analysis for each intervention group and between treatment groups (UP-guided, UP-unguided) in relation to the control group, through G*Power 3.1.6 software [62]. A conservative approach will be pursued, and the size of the magnitude effect will be estimated using Cohen’s d index, a significance level (α) of 0.05 (p < 0.05, which corresponds to 95% reliability) with a conventional statistical power of 80% (1- β × 0.8). For the analysis of clinical significance associated with clinically significant change, which refers to whether an intervention makes any real difference in people in their daily lives [8], the Reliable Change Rate (ICF) [65] will be calculated, using the criteria of ± 1.64 and ± 1.96 in the area under the normal curve, corresponding to 90 and 95% confidence levels. This method has been chosen because as Jacobson et al. [65] proposes, the amount of statistical change will first be estimated to assess whether the observed difference exceeds the error of measurement of the questionnaire, and second, it will be estimated whether the participant’s score has approached the mean of the functional group. This will be estimated through the normative data of the Mexican version of Beck’s anxiety and depression inventories. Clinical change will be taken as relevant if the participant reduces its levels to < 15 for anxiety, and < 16 for depression. In addition, although the calculation is based on the difference in score means, it incorporates the pre- and post-treatment measurement error. Thus, to assess whether there was a significant clinical change, both criteria must be met: the change must be statistically reliable and clinically relevant. Multiple regression will be used for mediation analyses to test the interaction effects between reference predictor (emotional regulation) and intervention condition, using macro/interface/Process for SPSS.
Discussion
The present paper describes an Internet-delivered intervention study protocol designed to evaluate the efficacy and acceptability of a transdiagnostic guided Internet-delivered intervention versus a transdiagnostic self-guided Internet-delivered intervention for emotional, trauma and stress-related disorders, and a waiting list in a Mexican adults community sample, and also, to examine the moderators of clinical change, particularly emotional regulation, in the transdiagnostic Internet-delivered intervention for emotional, trauma and stress-related disorders.
Anxiety and mood disorders have been identified as the main causes of psychological disability due to their high prevalence, morbidity and comorbidity in the world and in Mexico; coupled with the impact on the mental health of the population caused by the health contingency due to COVID-19, which has increased the incidence and/or exacerbation of emotional crises and suicidal risk, anxious symptoms, depression and acute stress that could develop if not treated in a timely manner chronically and develop post-traumatic stress, pathological grief and severe and serious emotional disorders. Thus, attention to this priority problem focused on psychological intervention based on a transdiagnostic model that has shown efficacy for the treatment of two or more specific disorders becomes relevant, and thereby contribute to overcoming the inconveniences related to comorbidity between disorders that prevent the full recovery of the person. Likewise, the intervention provided by the Internet will allow better dissemination and will allow addressing the challenge of achieving a greater reach to the vulnerable target population that has not been able to access an effective intervention.
The study has strengths and clinical implications. First, to the best of our knowledge, this is the first Mexican randomized controlled clinical trial to apply a transdiagnostic Internet-delivered intervention to treat EDs and Trauma, stress-related disorders. Second, this study proposes two transdiagnostic Internet-delivered intervention: guided and unguided, to compare the efficacious, acceptance and satisfaction from the users’ view, which will contribute in terms of feasibility of applying the Internet-delivered intervention in different social context to achieve generalization or external validity. Also, the participants will be the direct beneficiaries of the results of the study by reducing anxious and depressive symptoms and will be able to strengthen their coping skills in the face of stressful events.
There are some estimated limitations in the study, one linked to the dropout rate, it is documented [18] that Internet-delivered and self-administered interventions show high dropout rates, particularly participants in the waiting list group. The reasons could be the preference for face-to-face treatments or the lack of access to the Internet or electronic devices to receive the treatment. To reduce this incidence of dropouts, it has been planned to send weekly follow-up reminders and notifications to users to motivate them to continue with the intervention. Another limitation could be the small effect size estimated between the intervention groups because both are based on the same transdiagnostic Internet-delivered intervention and the variant to be compared will be the guide of a clinician who follows the intervention through a weekly videoconferencing session. However, it is estimated that a superiority will be found between the intervention groups compared to the waiting list group.
Finally, the central mechanism of action on the project is the development of a transdiagnostic Internet-delivered intervention program, which can be implemented for dissemination in health centers, universities, community centers, etc. The study is expected to provide evidence of an intervention with content rigorously elaborated and contextualized to society and culture which, with the support of innovative technological resources, provides functional strategies for target users.
Trial status
The study has not yet started with participant recruitment, it will begin in September 2022. There are no data derived from this study; There are no publications containing the results of this study.
Availability of data and materials
Not applicable.
Abbreviations
- BAI:
-
Beck Anxiety Inventory
- BDI-II:
-
Beck Depression Inventory
- CBT:
-
Cognitive Behavioral Treatments.
- CONSORT:
-
Consolidated Standards of Reporting Trials
- DERS:
-
Scale of Difficulties in Emotional Regulation
- DSM-IV-R:
-
Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision
- ED:
-
Emotional Disorders.
- ICF:
-
Reliable Change Rate
- IDS-10:
-
Inventory of Depressive Symptomatology
- MINI:
-
International Neuropsychiatric Interview, Version 5.0.0
- OASIS:
-
General Anxiety and the Impairment Severity Scale.
- ODSIS:
-
General Depression and the Impairment Gravity Scale.
- PC:
-
Personal Computer
- SPSS:
-
Statistical Package for Social Sciences
- SPIRIT:
-
Standard Protocol Items: Recommendations for Intervention Trials
- SMP:
-
Mexican Psychologist’s Code of Ethics
- SCL-90:
-
Symptom checklist
- PCL-5:
-
Posttraumatic Stress Disorder Checklist for DSM-5
- PTSD:
-
Posttraumatic Stress Disorder
- SUS:
-
Usability Scale
- UP:
-
Unified Protocol for the Treatment of Emotional Disorders
References
Organización Mundial de la Salud. Plan de acción sobre salud mental 2013–2020; 2013 [Consultado 2021 Mayo 10]. Disponible en: https://apps.who.int/iris/bitstream/handle/10665/97488/9789243506029_spa.pdf
Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386(9995):743–800. https://doi.org/10.1016/S0140-6736(15)60692-4.
Pan American Health Organization. Mexico. 2018. Available at: http://www.paho.org/mex/. Accessed 11 May 2022.
Medina-Mora, ME, Borges G, Lara C, Benjet C, Blanco J, Fleiz C, Villatoro J, Rojas E, Zambrano J, Casanova L, Aguilar-Gaxiola S. Prevalencia de trastornos mentales y uso de servicios: resultados de la Encuesta Nacional de Epidemiología Psiquiátrica en México. Salud Mental. 2003; 26:1–16. Retrieved from: https://www.redalyc.org/articulo.oa?id=58242601
Weisel KK, Zarski A, Berger T, Schaub MP, Krieger T, Moser CT, Berking M, David D, Ebert DD. Transdiagnostic tailored internet-and mobile-based guided treatment for major depressive disorder and comorbid anxiety: study protocol of a randomized controlled trial. Front Psychiatry. 2018;9:274. https://doi.org/10.3389/fpsyt.2018.00274.
Berenzon S, Saavedra N, Medina-Mora ME, Aparicio V, Galván J. Evaluación del sistema de salud mental en México: ¿Hacia dónde encaminar la atención? Rev Panam Salud Publica. 2013;33(4):252–8.
Cuijpers P, Sijbrandij M, Koole SL, Andersson G, Beekman AT, Reynolds CF. Adding psychotherapy to antidepressant medication in depression and anxiety disorders: a meta-analysis. World Psychiatry. 2014;13(1):56–67. https://doi.org/10.1002/wps.20089.
Kazdin AE. Research Design in Clinical Psychology. 6th ed. Michigan: Pearson; 2016.
Mohr DC, Ho J, Duffecy J, Baron KG, Lehman KA, Jin L, Reifler D. Perceived barriers to psychological treatments and their relationship to depression. J Clin Psychol. 2010;66(4):394–409. https://doi.org/10.1002/jclp.20659.
Holmes E, Craske M, Graybiel A. Psychological treatments: a call for mental-health science. Nature. 2014;511:287–9. https://doi.org/10.1038/511287a.
Ebert DD, Reins J, Buntrock C, Zimmermann J, Cuijpers P. Efficacy and moderators of psychological interventions in treating subclinical symptoms of depression and preventing major depressive disorder onsets: protocol for an individual patient data meta-analysis of randomized controlled trials. BMJ Open. 2018;8:e018582. https://doi.org/10.1136/bmjopen-2017-018582.
Hernández-Guzmán L, Del Palacio A, Freyre M, Alcázar-Olán R. La perspectiva dimensional de la psicopatología. Rev Mex de Psicol. 2011;28:111–20.
Clark LA, Watson D. Tripartite model of anxiety and depression: psychometric evidence and taxonomic implications. J Abnorm Psychol. 1991;100(3):316–36. https://doi.org/10.1037/0021-843X.100.3.316.
Ellard KK, Fairholme CP, Boisseau CL, Farchione TJ, Barlow DH. Unified protocol for the transdiagnostic treatment of emotional disorders: protocol development and initial outcome data. Cogn Behav Pract. 2010;17(1):88–101. https://doi.org/10.1016/j.cbpra.2009.06.002.
Bullis JR, Fortune MR, Farchione TJ, Barlow DH. A preliminary investigation of the long-term outcome of the unified protocol for transdiagnostic treatment of emotional disorders. Compr Psychiatry. 2014;55(8):1920–7. https://doi.org/10.1016/j.comppsych.2014.07.016.
Reinholt N, Krogh J. Efficacy of transdiagnostic cognitive behaviour therapy for anxiety disorders: a systematic review and meta-analysis of published outcome studies. Cogn Behav Ther. 2014;43(3):171–84. https://doi.org/10.1080/16506073.2014.897367.
Newby JM, Twomey C, Yuan Li SS, Andrews G. Transdiagnostic computerised cognitive behavioural therapy for depression and anxiety: a systematic review and meta-analysis. J Affect Disord. 2016;199:30–41. https://doi.org/10.1016/j.jad.2016.03.018.
Carly E, McCord J, Saenz J, Armstrong TW, Elliott TR. Training the next generation of counseling psychologists in the practice of telepsychology. Couns Psychol Q. 2015;28(3):324–44. https://doi.org/10.1080/09515070.2015.1053433.
Dworschak C, Heim E, Maercker A. Efficacy of internet-based interventions for common mental disorder symptoms and psychosocial problems in older adults: a systematic review and meta-analysis. Internet Interv. 2022;27:100498. https://doi.org/10.1016/j.invent.2022.100498.
Taylor C, Graham A, Flatt R, Waldherr K, Fitzsimmons-Craft E. Current state of scientific evidence on Internet-based interventions for the treatment of depression, anxiety, eating disorders and substance abuse: an overview of systematic reviews and meta-analyses. Eur J Public Health. 2021;31:i3–10. https://doi.org/10.1093/eurpub/ckz208.
Lin T, Heckman TG, Anderson T. The efficacy of synchronous teletherapy versus in-person therapy: a meta-analysis of randomized clinical trials. Clin Psychol: Sci Pract. 2021. https://doi.org/10.1037/cps0000056.
Glasgow R, Rosen G. Self-help behaviour therapy manuals: recent development and clinical usage. Clinic Behav Ther Rev. 1982;1:1–20.
Díaz-García A, González-Robles A, Fernández-Álvarez J, García-Palacios A, Baños RM, Botella C. Efficacy of a transdiagnostic internet-based treatment for emotional disorders with a specific component to address positive affect: Study protocol for a randomized controlled trial. BMC Psychiatry. 2017;17(1):145. https://doi.org/10.1186/s12888-017-1297-z.
Titov N, Dear BF, Johnston L, Lorian C, Zo J, Wootton B, Spence J, McEvoy PM, Rapee RM. Improving adherence and clinical outcomes in self-guided internet treatment for anxiety and depression: randomised controlled trial. PLoS ONE. 2013;8(7):e62873. https://doi.org/10.1371/journal.pone.0062873.
González-Robles A, García-Palacios A, Baños RM, Riera A, Llorca G, Traver F, Haro G, Palop V, Lera G, Romeu JE, Botella C. Effectiveness of a transdiagnostic internet-based protocol for the treatment of emotional disorders versus treatment as usual in specialized care: study protocol for a randomized controlled trial. Trials. 2015;16:488. https://doi.org/10.1186/s13063-015-1024-3.
Hadjistavropoulos HD, Nugent MM, Alberts NM, Staples L, Dear BF, Titov N. Transdiagnostic Internet-delivered cognitive behaviour therapy in Canada: An open trial comparing results of a specialized online clinic and nonspecialized community clinics. J Anxiety Disord. 2016;42:19–29. https://doi.org/10.1016/j.janxdis.2016.05.006.
Christensen H, Batterham P, Mackinnon A, Griffiths KM, Kalia Hehir K, Kenardy J, Gosling J, Bennett K. Prevention of generalized anxiety disorder using a web intervention, iChill: Randomized Controlled Trial. J Med Internet Res. 2014;16(9):e199. https://doi.org/10.2196/jmir.3507.
Buntrock C, Ebert DD, Lehr D, Smit F, Riper H, Berking M, Cuijpers P. Effect of a web-based guided self-help intervention for prevention of major depression in adults with subthreshold depression. JAMA. 2016;315(17):1854–63. https://doi.org/10.1001/jama.2016.4326.
Dear BF, Staples LG, Terides MD, Fogliati VJ, Sheehan J, Johnston L, Kayrouz R, Dear R, McEvoy PM, Titov N. Transdiagnostic versus disorder-specific and clinician-guided versus self-guided internet-delivered treatment for social anxiety disorder and comorbid disorders: a randomized controlled trial. J Anxiety Disord. 2016;39:88–102. https://doi.org/10.1016/j.janxdis.2016.03.005.
Richards D, Richardson T. Computer-based psychological treatments for depression: a systematic review and meta-analysis. Clin Psychol Rev. 2012;32(4):329–42. https://doi.org/10.1016/j.cpr.2012.02.00.
Kleiboer A, Donker T, Seekles W, van Straten A, Riper H, Cuijpers P. A randomized controlled trial on the role of support in Internet-based problem-solving therapy for depression and anxiety. Behav Res Ther. 2015;72:63–71. https://doi.org/10.1016/j.brat.2015.06.013.
Mira A, Bretón-López J, García-Palacios A, Quero S, Baños RM, Botella C. An internet-based program for depressive symptoms using human and automated support: a randomized controlled trial. Neuropsychiatr Dis Treat. 2017;13:987–1006. https://doi.org/10.2147/NDT.S130994.
Cooper DK, Erolin KS, Wieling E, Durtschi J, Aguilar E, Diaspro-Higuera MO, Garcia-Huidobro D. Family violence, PTSD, and parent–child interactions: dyadic data analysis with Mexican families. Child Youth Care Forum. 2020;49(6):915–40. https://doi.org/10.1007/s10566-020-09564-3.
Gutner CA, Galovski T, Bovin MJ, Schnurr PP. Emergence of transdiagnostic treatments for PTSD and posttraumatic distress. Curr Psychiatry Rep. 2016;18(10):95. https://doi.org/10.1007/s11920-016-0734-x.
Moher D, Hopewell S, Schulz KF, Montori V, Gøtzsche PC, Devereaux PJ, et al. CONSORT explanation and elaboration: updated guidelines for reporting parallel group randomised trials. Int J Surg. 2012;10(1):28–55. https://doi.org/10.1016/j.ijsu.2011.10.001.
Chan AW, Tetzlaff JM, Altman DG, Laupacis A, Gøtzsche PC, Krleža-Jerić K, Hróbjartsson A, Mann H, Dickersin K, Berlin JA, Doré CJ, Parulekar WR, Summerskill WS, Groves T, Schulz KF, Sox HC, Rockhold FW, Rennie D, Moher D. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann Intern Med. 2013;158(3):200–7. https://doi.org/10.7326/0003-4819-158-3-201302050-00583.
Sheehan DV, Lecrubrier Y, Harnett-Sheehan K, Janavs J, et al. Reliability and validity of the MINI International Neuropsychiatric Interview (MINI): according to the SCID-P. Eur Psychiatry. 1997;12:232–41.
Beck AT, Steer RA. Manual for the Beck Anxiety Inventory. San Antonio: Psychological Corporation; 1990.
Beck AT, Steer RA, Brown GK. Manual for the Beck Depression Inventory-II. San Antonio: Psychological Corporation; 1996.
Sociedad Mexicana de Psicología. Código ético del psicólogo. 5a ed. México: Trillas; 2010.
American Psychological Association. Guidelines for the Practice of Telepsychology. American psychologist. 2013. Available at: https://www.apa.org/practice/guidelines/telepsychology. Accessed 11 May 2022.
Urbaniak G C. Plous S. Research Randomizer (Version 4.0). 2013. Available at: http://www.randomizer.org/. Accessed 12 May 2022.
Horton AM, Alana S. Validation of the Mini-Mental State Examination. Int J Neurosci. 1990;53(2–4):209–12. https://doi.org/10.3109/00207459008986604.
Heinze M, Sheehan D, Cortés J. Mini International Neuropsychiatric Interview (MINI): Spanish version (South and Central America) 500 DSM-IV. Mexico: Instituto Nacional de Psiquiatría; 2000.
Cruz Fuentes CS, López BL, Blas GC, González ML, Chávez BR. Datos sobre la validez y confiabilidad de la Symptom Check List 90 (SCL 90) en una muestra de sujetos mexicanos. Salud Ment. 2005;28(1):72–81.
Weathers FW, Litz B., Keane TM, Palmieri PA, Marx BP, Schnurr PP. The PTSD Checklist for DSM-5 (PCL-5). 2013. Available at: www.ptsd.va.gov. Accessed 2022 Myo 12.
Durón-Figueroa R, Cárdenas-López G, Castro-Calvo J, Rosa-Gómez A. Adaptación de la Lista Checable de Trastorno por Estrés Postraumático para DSM-5 en Población Mexicana. Acta de investigación; 9(1): 26–36. doi: https://doi.org/10.22201/fpsi.20074719e.2019.1.03.
Beck AT, Epstein N, Brown G, Steer R. Beck Anxiety Inventory. APA PsycTests. 1998. https://doi.org/10.1037/t02025-000
Robles R, Varela R, Jurado S, Páez F. Versión mexicana del Inventario de Ansiedad de Beck: Propiedades psicométricas. Rev Mex de Psicol. 2001;18:211–8.
Beck TA, Steer AR, Garbin GM. Psychometric properties of the Beck Depression Inventory: twenty-five years of evaluation. Clin Psychol Rev. 1988;8(1):77–100. https://doi.org/10.1016/0272-7358(88)90050-5.
Jurado S, Villegas M, Méndez L, Rodríguez F, Loperena V. Varela R. La estandarización del Inventario de Depresión de Beck para los residentes de la Ciudad de México. Salud Ment. 1998; 21: 26-31. http://www.revistasaludmental.mx/index.php/salud_mental/article/view/706
González D, Reséndiz A, Reyes-Lagunes I. Adaptation of the BDI-II in Mexico. Salud Ment. 2015;38:237–44. https://doi.org/10.17711/sm.0185-3325.2015.033.
Gratz KL, Roemer L. Multidimensional assessment of emotion regulation and dysregulation: development, factor structure, and initial validation of the difficulties in emotion regulation scale. J Psychopathol Behav Assess. 2008;26:41–54. https://doi.org/10.1007/s10862-008-9102-4.
De la Rosa-Gómez A, Hernández-Posadas A, Valencia PD, Guajardo-Garcini DA. Análisis dimensional de la Escala de Dificultades en la Regulación Emocional (DERS-15) en universitarios mexicanos. Revista Evaluar. 2021;21(2):80–97. https://doi.org/10.35670/1667-4545.v21.n2.34401.
Norman SB, Campbell-Sills L, Hitchcock CA, Sullivan S, Rochlin A, Wilkins KC, et al. Psychometrics of a brief measure of anxiety to detect severity and impairment: the Overall Anxiety Severity and Impairment Scale (OASIS). J Psychiatr Res. 2011;45(2):262–8. https://doi.org/10.1016/j.jpsychires.2010.06.011.
Osma J, Quilez-Orden A, Suso-Ribera C, Peris-Baquero O, Norman SB, Bentley KH, Sauer-Zavala S. Psychometric properties, and validation of the Spanish versions of the overall anxiety and depression severity and impairment scales. J Affect Disord. 2019;252:9–18. https://doi.org/10.1016/j.jad.2019.03.063.
Bentley KH, Gallagher MW, Carl JR, Barlow DH. Development and validation of the Overall Depression Severity and Impairment Scale. Psychol Assess. 2014;26(3):815–30. https://doi.org/10.1037/a0036216.
Borkovec TD, Nau SD. La credibilidad de razones de terapia analógica. JBTEAB. 1972;3(2):257–60. https://doi.org/10.1016/0005-7916(72)90045-6.
Botella C, Gallego MJ, García-Palacios A, Guillén V, Baños RM, Quero S, Alcañiz M. An internet-based self-help treatment for fear of public speaking: a controlled trial. Cyberpsychol Behav Soc Netw. 2010;13(4):407–21. https://doi.org/10.1089/cyber.2009.0224.
Brooke J. SUS: A quick and dirty usability scale. In: Jordan. Thomas BA, Weerdmeester IL, McClelland, editor. Usability Evaluation in Industry. London: Taylor & Francis; 1996. p. 189–194.
Barlow DH, Allen LB, Choate ML. Toward a unified treatment for emotional disorders. Behav Ther. 2016;47(6):838–53. https://doi.org/10.1016/j.beth.2016.11.005.
Faul F, Erdfelder E, Lang A-G, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–91. https://doi.org/10.3758/bf03193146.
Saad A, Bruno D, D´Agostino J, Bolea-Alamanac B. P.0262 Self-directed virtual care: a review of the evidence for current digital therapeutic methods in adult mental health patients. Eur Neuropsychopharmacol. 2021;53(1):s191-192. https://doi.org/10.1016/j.euroneuro.2021.10.252.
Vöhringer M, Knaevelsrud C, Wagner B, Slotta M, Schmidt A, Stammel N, Böttche M. Should I stay or must I go? Predictors of dropout in an internet-based psychotherapy programme for posttraumatic stress disorder in Arabic. Eur J Psychotraumatol. 2020;11(1):1706297. https://doi.org/10.1080/20008198.2019.1706297.
Jacobson NS, Truax P. Clinical significance: a statistical approach to defining meaningful change in psychotherapy research. J Consult Clin Psychol. 1991;59(1):12–9. https://doi.org/10.1037//0022-006x.59.1.12.
Acknowledgements
ITSON-CA-30 Actores y procesos psicoeducativos, Centro de Atención e Investigación del Comportamiento Humano CAICH of Technological Institute of Sonora.
Funding
The study is supported by external funding of the National Council of Science and Technology (Mexico), CONACyT. Call 2020–04: Research Projects and Social Incidence in Mental Health and Addictions. Grant number 1401. The funding institution had no role in the design of the study; data collection, analysis, and interpretation; and will not have any role in the writing of the manuscript.
Author information
Authors and Affiliations
Contributions
ARG conceived, designed, and got the funding of the study. ARG, LFP, EES and CSTT wrote the first draft of the manuscript. RGF, ADR, PAL, RCV, EBR, RSR, GMD, DDS, AHP, AFE, PV and MVS revised the manuscript and completed the final draft. All authors contributed feedback, read, and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study has the endorsement by the Research Ethics Committee of the Faculty of Higher Studies Iztacala of the National Autonomous University of México (CE/FESI/082020/1363), and it is registered in Clinical Trials (NCT05225701). Registered February 4, 2022, https://clinicaltrials.gov/ct2/show/NCT05225701. All participants must give their written consent to participate.
Consent for publication
Not applicable in this study.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
de la Rosa-Gómez, A., Flores-Plata, L.A., Esquivel-Santoveña, E.E. et al. Efficacy of a transdiagnostic guided internet-delivered intervention for emotional, trauma and stress-related disorders in Mexican population: study protocol for a randomized controlled trial. BMC Psychiatry 22, 537 (2022). https://doi.org/10.1186/s12888-022-04132-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-022-04132-6