
Abstract
Background
Antipsychotic prescribing to Medicaid-enrolled youth has been the target of numerous policy initiatives, including prior authorization and quality monitoring programs, which often target specific populations. Whether these efforts have changed the level or composition of antipsychotic prescribing is unclear.
Methods
Using 2014–2018 administrative claims data for Medicaid enrollees aged 21 years and under in Philadelphia, Pennsylvania,
we measured antipsychotic prescription fills overall and for youth without an approved indication (autism, bipolar disorder, or psychosis). We then assessed whether trends differed for populations that have been targeted by policy initiatives, including younger children and foster care-enrolled youth. We also identified the most common approved and unapproved indications and examined whether the treatment duration of antipsychotic prescriptions differed based on whether the youth had an approved or unapproved indication.
Results
Overall, the number of Medicaid youth with an antipsychotic prescription fill halved between 2014 and 2018. Youth aged 17 years and under and foster care-enrolled youth, who were targeted by prior authorization and quality improvement efforts, experienced larger declines. Roughly half of prescriptions were for unapproved indications in both 2014 and 2018; the most common unapproved indication was ADHD, and the treatment duration was shorter for unapproved indications compared to approved indications.
Conclusions
Antipsychotic prescribing to Medicaid-enrolled youth is declining, particularly among populations that have been targeted by policy initiatives like prior authorization and quality monitoring programs. Despite the fact that these initiatives often assess diagnostic criteria, half of antipsychotic prescriptions were for unapproved indications in both 2014 and 2018. More research is needed to gauge whether this prescribing is appropriate.
Similar content being viewed by others


Introduction
Beginning in the 1980s, antipsychotics were increasingly prescribed to children and adolescents in the United States (U.S.) [1, 2]. The uptick in antipsychotic prescribing, particularly among vulnerable populations like Medicaid enrollees and youth in foster care, raised concerns about the appropriateness of prescribing given the risks involved, including weight gain and side effects like tardive dyskinesia [3,4,5,6,7,8].
To date, the Food and Drug Administration (FDA) has approved antipsychotic use for bipolar disorder, psychosis, and symptoms associated with autism, and there were additional concerns that antipsychotics were being prescribed excessively to children with unapproved indications, such as attention deficit/hyperactivity disorder (ADHD) [9,10,11,12]. Approval from regulatory agencies, including the FDA, indicate that there is enough rigorous scientific support demonstrating that the clinical benefits of antipsychotic use for a given population and diagnosis outweigh the risk of adverse events [13].
However, prescribing without an FDA-approved indication is an important element of clinical practice, and studies have shown it is safe and efficacious when there is scientific support for its use [14]. Yet off-label prescribing—which encompasses prescribing for unapproved indications, as well as unapproved age categories, dosages, or method of administration—frequently occurs with little to no scientific support, especially in psychiatry [13, 15]. This may increase the risk of adverse drug events and improper medication management [10, 16, 17].
There is some evidence that antipsychotic prescribing is declining, but studies are inconsistent. A claims-based study found that the number of publicly-insured youth in the U.S. receiving antipsychotic prescriptions fell nearly 40% from 2008 to 2013 [18]. A more recent claims-based study also found a decline in antipsychotic prescribing from 2009 through 2017, but the study was restricted to privately-insured youth aged 2 to 7 in the U.S. [19] In contrast, a national survey in the U.S. reported increases in antipsychotic prescribing through 2014 [20]. Another national survey in the U.S. reported decreases in antipsychotic prescribing among toddlers, a plateau among elementary school-age children, and an increase among adolescents between 1999 and 2014 [21].
The inconsistent trends may be attributable to the policy environment, which includes various initiatives geared toward antipsychotic prescribing [22]. For example, thirty-one state Medicaid programs in the U.S. implemented prior authorization for antipsychotic prescribing to Medicaid-enrolled youth by 2015, which requires pre-approval from the insurer or managed care organization prior to a prescription fill [22]. Fifteen states also incorporated clinical review and other quality monitoring programs by 2015 [23]. Some of these initiatives targeted specific populations, e.g., Pennsylvania launched a quality monitoring program focused exclusively on antipsychotic prescribing to foster care-enrolled youth [24, 25].
Studies have found that approaches like prior authorization effectively decrease prescribing rates, including antipsychotic prescribing [26,27,28]. But it is unclear whether these efforts have had disproportionate effects on certain populations, such as foster care-enrolled youth. It is also unclear whether they are more likely to reduce prescribing to youth without approved indications, although a recently published study in Texas between 2013 and 2016, which examined unapproved antipsychotic use among publicly-insured children and adolescents, found a reduction in the proportion of antipsychotic prescriptions without an approved indication [29]. Diagnostic criteria are often included in prior authorization forms and in quality monitoring programs, which could change the composition of antipsychotic prescribing [ 30].
Using administrative claims data for a large cohort of Medicaid-enrolled youth living in Philadelphia, Pennsylvania between 2014 and 2018, this study provides a relatively up-to-date assessment of antipsychotic prescribing. We separately estimate trends in antipsychotic prescribing for approved versus unapproved indications, then examine whether trends are more pronounced in certain populations, including foster care-enrolled youth.
Methods
Study setting and population
Our study sample consisted of Medicaid enrollees aged 0 through 21 years in Philadelphia County who filled at least one antipsychotic prescription between January 1, 2014 and December 31, 2018. Philadelphia, Pennsylvania is the sixth largest city in the U.S., with a population of 1.6 million [31]. Philadelphia is among the poorest large cities in the U.S., and roughly a quarter of its population lives below the poverty line [32]. The racial/ethnic distribution is 8% Asian, 44% Black, 15% Hispanic, and 45% white [32].
Medicaid is the publicly-funded insurer of millions of Americans, primarily low-income adults, youth, and individuals with disabilities; in Philadelphia, over 650,000 individuals were enrolled in Medicaid in 2018 [32]. Medicaid is the primary insurer for youth enrolled in foster care, sometimes called out-of-home care, which refers to children and adolescents under 18 years old who have been temporarily removed from their familial home and placed with either relatives or unrelated foster parents [33].
Statistical analyses
We used administrative claims data to measure antipsychotic prescription fills which could be identified using National Drug Codes outlined by the Healthcare Effectiveness Data and Information Set (HEDIS) quality measure that focuses on antipsychotic prescribing [34]. Following other claims-based studies, we defined approved indications based on whether the youth had at least one approved diagnostic code (i.e., autism spectrum disorder, bipolar disorder, and/or psychosis) in the same calendar year as a given antipsychotic prescription fill [35, 36]. Diagnoses were identified using outpatient behavioral health claims and International Classification of Disease codes (ICD-9 in 2014 and ICD-10 afterwards). Sociodemographic characteristics of youth were drawn from the Medicaid eligibility file.
We first documented antipsychotic prescribing trends over time, overall and by gender and race/ethnicity, and separately measured trends among children and adolescents who did not have an approved indication. We then examined the potential impact of two initiatives in Philadelphia—the rollout of prior authorization for antipsychotic prescribing and a quality monitoring program focused on foster care-enrolled youth, which was commissioned by the Pennsylvania Office of Mental Health and Substance Abuse [24, 28]—by separately estimating trends for youth aged 17 years and younger, who were targeted by prior authorization, and for youth enrolled in foster care, whose prescriptions were under increased scrutiny due to the quality monitoring program. Differences in the number of Medicaid-enrolled youth with an antipsychotic prescription between 2014 and 2018 (overall, by age category, foster care status, gender, and race/ethnicity) were assessed using two-tailed tests at the 95% level of significance.
Given our interest in unapproved indications, we identified the top approved and unapproved diagnoses associated with an antipsychotic prescription fill in 2018. We also compared the treatment duration, as measured by days supplied (30 days and under, 31–60 days, 61–90 days, 91–180 days, and 181–365 days), of antipsychotic prescriptions for approved versus unapproved indications in 2018.
The study was approved by the Institutional Review Board of the City of Philadelphia and the University of Pennsylvania.
Results
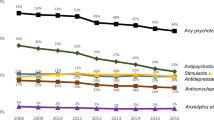
Between 2014 and 2018 there was a 49% decline (p < 0.001) in the number of youths with an antipsychotic prescription fill—from 5253 to 2688 (Fig. 1). When adjusting for fluctuations in Medicaid enrollment, the rate of antipsychotic prescribing fell from 17 per 1000 Medicaid-enrolled youth in 2014 to 8 per 1000 Medicaid-enrolled youth in 2018 (p < 0.001).

Number of Medicaid-Enrolled Youth in Philadelphia, PA who Filled Antipsychotic Prescriptions, 2014–2018
The characteristics of youth receiving antipsychotic prescriptions changed significantly as well (Table 1). Between 2014 and 2018, the average age increased from 13.8 years to 15.2 years (p < 0.001) and the proportion of females increased by over four percentage points (p < 0.001).
Notably, the reduction in antipsychotic prescribing was more pronounced among Medicaid enrollees aged 17 and under (particularly children aged 10 and under) and foster care-enrolled youth, two groups that were targeted by local prescribing initiatives. By comparison, the decrease was more modest among Medicaid enrollees between the ages of 18 and 21 years, who were not targeted in prior authorization efforts and had aged out of the foster care system.
While the raw number of antipsychotic prescriptions for unapproved indications fell between 2014 and 2018, the share of antipsychotic prescribing for unapproved indications increased slightly: 44.4% in 2014 versus 47.3% in 2018. Females (p < 0.001) and Black (p < 0.001) and Hispanic (p = 0.003) youth comprised a substantially larger share of prescriptions for unapproved indications in 2018 compared to 2014.
The most common FDA-approved diagnosis among youth with an antipsychotic prescription fill in 2018 was autism, followed by bipolar disorder and psychosis. The most common unapproved diagnosis was ADHD, followed by depression, adjustment disorders (which includes post-traumatic stress disorder), and conduct disorders (Table 2).
On average, antipsychotic prescriptions for approved indications tended to have longer treatment durations—nearly 30% of youth without an approved indication had antipsychotic prescriptions that were 30 or fewer days compared to 16% of youth with approved indications (Fig. 2).

Annual Treatment Duration for Antipsychotic Prescriptions to Youth Enrolled in Philadelphia Medicaid, 2018
Discussion
This study measured trends in antipsychotic prescribing to Medicaid-enrolled youth residing in Philadelphia, Pennsylvania, finding a large reduction in antipsychotic prescribing between 2014 and 2018. The decline was concentrated among Medicaid enrollees who were 17 years of age and under, which suggests that the drop-off was associated with age requirements for prior authorization that were introduced by Pennsylvania Medicaid fee-for-service in 2006 and expanded to Medicaid managed care organizations in Philadelphia [22, 28]. The decline was also concentrated among foster care-enrolled youth, who were subject to a statewide quality monitoring program [24].
While overall rates declined, we found an increase in the proportion of antipsychotics prescribed to female patients. There could be a number of factors driving this trend, but one possibility is the historic discrepancy in diagnoses for certain conditions based on gender is narrowing. Studies have found that females have been under-diagnosed for approved and unapproved indications commonly associated with antipsychotic use, such as autism and ADHD, due to the lack of recognition and referral bias [37, 38]. More awareness of clinical symptoms in female patients could increase the likelihood that they receive a psychiatric diagnosis and accompanying antipsychotic prescription.
Both prior authorization and quality monitoring for foster care-enrolled youth assessed diagnostic criteria for antipsychotic prescribing, yet we found that the share of antipsychotic prescriptions for unapproved indications remained steady—nearly half of prescriptions occurred for unapproved indications in both 2014 and 2018. While few studies have assessed the impact of these types of initiatives on the composition of prescribing, this finding contrasts a recent study of youth in Texas Medicaid [29]. Our finding also contrasts a study of a prior authorization program that focused exclusively on diagnostic criteria for gabapentin prescriptions, which reported a significant decline in gabapentin prescribing for unapproved indications [39].
Providers have cited many reasons for relying on off-label prescribing to patients in psychiatry, including the dearth of effective medications for mood swings and aggression [40, 41]. When we explored the diagnoses of youth with antipsychotic prescription fills in 2018, we found high rates of ADHD, conduct disorders, and other conditions that are sometimes marked by these behavioral symptoms.
One dimension of antipsychotic prescribing that has not been explored, to our knowledge, is whether there are differences in the duration of antipsychotic use for approved and unapproved indications. We found that prescriptions for unapproved indications were shorter on average—antipsychotic prescriptions that lasted 30 or fewer days comprised nearly 30% of prescriptions for unapproved indications, nearly double the rate of prescriptions for approved indications. This suggests that providers are taking a more cautious approach when prescribing to youth without an approved indication.
While these findings may not be generalizable to other populations, studies have found that youth enrolled in Medicaid are over three times more likely to receive an antipsychotic prescription than youth with commercial insurance, making this an important population to study [42]. We face other limitations. Following other claims-based studies, our approach to determining whether antipsychotic prescriptions were for approved indications was based on available diagnoses in Medicaid behavioral health claims in a given year [28, 29]. Without chart review, it is unclear whether providers were targeting key symptoms that warranted antipsychotic prescribing. For example, if providers were targeting symptoms associated with autism spectrum disorder but did not specify autism spectrum disorder in insurance claims, the antipsychotic prescription would be categorized as unapproved [43]. Another limitation is the study period, which begins in 2014 and ends in 2018 (data standardization and availability prevent us from analyzing more recent years of data and the full impact of policies like prior authorizations). Given these limitations, we cannot conclusively estimate the causal effects of policy initiatives.
Conclusion
Despite these limitations, our findings have important implications. Antipsychotic prescribing to Medicaid-enrolled youth in Philadelphia is declining dramatically. However, the share of antipsychotic prescribing for unapproved indications has been relatively steady and females and Black and Hispanic youth comprised a larger share of youth with antipsychotic prescriptions for unapproved indications in 2018 compared to 2014, which may be driven by disparities in quality or access to health care. More research is needed to understand whether these trends reflect more judicious antipsychotic prescribing or if the drop-off in antipsychotic prescribing has resulted in unintended effects, particularly among those without affordable and accessible treatment alternatives.
Availability of data and materials
Our primary data source are Medicaid claims, which are not publicly accessible. The SAS code used to generate the findings is available upon request. Requests can be sent to the corresponding author at molly.candon@pennmedicine.upenn.edu, 3535 Market Street, 3rd Floor, Philadelphia, PA 19104, U.S.
Abbreviations
- FDA:
-
Food and drug administration
- ICD:
-
International classification of disease
- ADHD:
-
Attention deficit/hyperactivity disorder
References
Teicher MH, Glod CA. Neuroleptic drugs; indications and guidelines for their rational use in children and adolescents. J Child Adolesc Psychopharmacol. 1990;1(1):33–56. https://doi.org/10.1089/cap.1990.1.33.
Christian R, Saavedra L, Gaynes BN, et al. Future research needs for first- and second-generation antipsychotics for children and Young adults [internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2012 Feb. (future research needs papers, no. 13.) appendix a, Tables of FDA-Approved Indications for First- and Second-Generation Antipsychotics.
Rettew DC, Greenblatt J, Kamon J, Neal D, Harder V, Wasserman R, Berry P, MacLean CD, Hogue N, McMains W. Antipsychotic medication prescribing in children enrolled in medicaid. Pediatrics. 2015;135(4):658-65.
Dosreis S, Yoon Y, Rubin DM, Riddle MA, Noll E, Rothbard A. Antipsychotic treatment among youth in foster care. Pediatrics. 2011;128(6):e1459–66. https://doi.org/10.1542/peds.2010-2970.
Saloner B, Matone M, Kreider AR, Budeir MS, Miller D, Huang YS, et al. Second-generation antipsychotic use among stimulant-using children, by organization of Medicaid mental health. Psychiatr Serv. 2014;65(12):1458–64. https://doi.org/10.1176/appi.ps.201300574.
Burcu M, Zito JM, Ibe A, Safer DJ. Atypical antipsychotic use among Medicaid-insured children and adolescents: duration, safety, and monitoring implications. J Child Adolesc Psychopharmacol. 2014;24(3):112–9. https://doi.org/10.1089/cap.2013.0094.
Crystal S, Olfson M, Huang C, Pincus H, Gerhard T. Broadened use of atypical antipsychotics; safety, effectiveness, and policy challenges. Health Affairs. 2009;28(1):w770-w781.
Harrison JN, Cluxton-Keller F, Gross D. Antipsychotic medication prescribing trends in children and adolescents. J Pediatr Health Care. 2012;26(2):139–45. https://doi.org/10.1016/j.pedhc.2011.10.009.
Sohn M, Moga DC, Blumenschein K, Talbert J. National trends in off-label use of atypical antipsychotics in children and adolescents in the United States [published correction appears in Medicine (Baltimore). 2016;95(28):e0916].
Gore R, Chugh PK, Tripathi CD, Lhamo Y, Gautam S. Pediatric off-label and unlicensed drug use and its implications. Curr Clin Pharmacol. 2017;12(1):18–25. https://doi.org/10.2174/1574884712666170317161935.
Department of Health and Human Services, Office of Inspector General. Executive Summary: Second-Generation Antipsychotic Drug Use Among Medicaid-enrolled Children: Quality of Care Concerns. OEI-07-12-00320. March 2015.
Fullerton CA, Epstein AM, Frank RG, Normand SL, Fu CX, McGuire TG. Medication use and spending trends among children with ADHD in Florida's Medicaid program, 1996-2005. Psychiatr Serv. 2012;63(2):115–21. https://doi.org/10.1176/appi.ps.201100095.
US Food and Drug Administration. Benefit-Risk Assessment in Drug Regulatory Decision-Making. Drafter PDUFA VI Implementation Plan, FY 2018–2022. Taken from https://www.fda.gov/files/about%20fda/published/Benefit-Risk-Assessment-in-Drug-Regulatory-Decision-Making.pdf on August 17, 2021.
Eguale T, Buckeridge DL, Verma A, Winslade NE, Benedetti A, Hanley JA, et al. Association of off-label Drug use and Adverse Drug Events in an adult population. JAMA Intern Med. 2016;176(1):55–63. https://doi.org/10.1001/jamainternmed.2015.6058.
Radley DC, Finkelstein SN, Stafford RS. Off-label prescribing among office-based physicians. Arch Intern Med. 2006;166(9):1,021–6. https://doi.org/10.1001/archinte.166.9.1021.
Choonara I, Conroy S. Unlicensed and off-label drug use in children. Drug Saf. 2002;25(1):1–5. https://doi.org/10.2165/00002018-200225010-00001.
Zito JM, Derivan AT, Kratochvil CJ, Safer DJ, Fegert JM, Greenhill LL. Off-label psychopharmacologic prescribing for children: history supports close monitoring. Child Adolesc Psychiatry Ment Health. 2008;2(24):1. https://doi.org/10.1186/1753-2000-2-24.
Edelsohn GA, Karpov I, Parthasarathy M, Hutchison SL, Castelnovo K, Ghuman J, et al. Trends in antipsychotic prescribing in Medicaid-eligible youth. J Am Acad Child Adolesc Psychiatry. 2017;56(1):59–66. https://doi.org/10.1016/j.jaac.2016.10.005.
Bushnell GA, Crystal S, Olfson M. Trends in Antipsychotic Medication Use in Young Privately Insured Children. J Am Acad Child Adolesc Psychiatry. 2021;60(7):877-86.
Lopez-Leon S, Lopez-Gomez MI, Warner B, Ruiter-Lopez L. Psychotropic medication in children and adolescents in the United States in the year 2004 vs 2014. DARU J Pharm Sci. 2018;26(1):2014–0. https://doi.org/10.1007/s40199-018-0204-6.
Hales CM, Kit BK, Gu Q, Ogden CL. Trends in prescription medication use among children and adolescents—United States, 1999-2014. JAMA. 2018;319(19):2,009–20. https://doi.org/10.1001/jama.2018.5690.
Centers for Medicare and Medicaid Services. A Review of State Medicaid Approaches on Child Antipsychotic Monitoring Programs. Accessed from https://www.medicaid.gov/medicaid-chip-program-information/by-topics/prescription-drugs/downloads/state-medicaid-dur-summaries.pdf on November 4, 2020.
Schmid I, Burcu M, Zito JM. Medicaid prior authorization policies for pediatric use of antipsychotics. JAMA. 2015;313(9):966-8.
Mackie TI, Schaefer A, Karpman HE, Lee SM, Bellonci C, Larson J. Systematic review: system-wide interventions to monitor pediatric antipsychotic prescribing and promote best practice. J Am Acad Child Adolesc Psychiatry. 2020;S0890-8567(20):31880–3.
Matone M, Zlotnik S, Miller D, Kreider A, Rubin D, Noonan K. Psychotropic medication use by Pennsylvania children in Foster Care and enrolled in Medicaid: an analysis of children ages 3–18 years. Philadelphia: PolicyLab at the Children’s Hospital of Philadelphia; 2015.
Dillender M. What happens when the insurer can say no? Assessing prior authorization as a tool to prevent high-risk prescriptions and to lower costs. J Public Econ. 2018;165:170–200. https://doi.org/10.1016/j.jpubeco.2018.07.006.
Marsico M. Assessing the impact of Pennsylvania’s prior authorization policy intended to reduce antipsychotic prescribing in Medicaid-insured children. Philadelphia: Temple University, ProQuest Dissertations Publishing; 2019. p. 13426908. https://scholarshare.temple.edu/handle/20.500.12613/3242.
Stein BD, Leckman-Westin E, Okeke E, Scharf DM, Sorbero M, Chen Q, et al. The effects of prior authorization policies on Medicaid-enrolled children's use of antipsychotic medications: evidence from two mid-Atlantic states. J Child Adolesc Psychopharmacol. 2014;24(7):374–81. https://doi.org/10.1089/cap.2014.0008.
Chen S, Barner JC, Cho E. Trends in off-label use of antipsychotic medications among Texas Medicaid children and adolescents from 2013 to 2016. J Managed Care Spec Pharm. 2021;27(8):1,035–45. https://doi.org/10.18553/jmcp.2021.27.8.1035.
Pennsylvania Department of Human Services. Medical Assistance Bulletin: Prior Authorization of Antipsychotics – Pharmacy Services. Accessed from https://www.dhs.pa.gov/providers/Pharmacy-Services/Documents/Clinical Guidelines SW PDL/Antipsychotics.pdf on November 4, 2020.
US Census Bureau. QuickFacts: Philadelphia County, Pennsylvania. Taken from https://www.census.gov/quickfacts/fact/table/philadelphiacountypennsylvania/PST045219 on August 17, 2021.
Pew Charitable Trust. Philadelphia: The State of the City. Taken from https://www.pewtrusts.org/-/media/assets/2021/04/philadelphia-2021-state-of-the-city.pdf on August 17, 2021.
US Department of Health & Human Services, Administration for Children & Families. Child Welfare Information Gateway. Taken from https://www.childwelfare.gov/topics/outofhome/foster-care/ on August 17, 2021.
National Committee for Quality Assurance. HEDIS 2017 Final NDC Lists. Accessed from https://www.ncqa.org/hedis/measures/hedis-2017-national-drug-code-ndc-license/hedis-2017-final-ndc-lists/ on November 4, 2020.
Driessen J, Baik SH, Zhang Y. Trends in off-label use of second-generation antipsychotics in the Medicare population from 2006 to 2012. Psych Serv. 2016;67(8):898–903. https://doi.org/10.1176/appi.ps.201500316.
Chen H, Reeves JH, Fincham JE, Kennedy WK, Dorfman JH, Martin BC. Off-label use of antidepressant, anticonvulsant, and antipsychotic medications among Georgia Medicaid enrollees in 2001. J Clin Psychiatry. 2006;67(06):972–82. https://doi.org/10.4088/JCP.v67n0615.
Young S, Adamo N, Ásgeirsdóttir BB, Branney P, Beckett M, Colley W, et al. Females with ADHD: an expert consensus statement taking a lifespan approach providing guidance for the identification and treatment of attention-deficit/ hyperactivity disorder in girls and women. BMC Psychiatry. 2020;20(1):404. https://doi.org/10.1186/s12888-020-02707-9.
Gould J. Towards understanding the under-recognition of girls and women on the autism spectrum. Autism. 2017;21(6):703–5. https://doi.org/10.1177/1362361317706174.
Fullerton CA, Busch AB, Frank RG. The rise and fall of gabapentin for bipolar disorder: a case study of off-label pharmaceutical diffusion. Med Care. 2010;48(4):372–9. https://doi.org/10.1097/MLR.0b013e3181ca404e.
Haw C, Stubbs J. A survey of the off-label use of mood stabilizers in a large psychiatric hospital. J Psychopharmacol. 2005;19(4):402–7. https://doi.org/10.1177/0269881105053307.
LeClerc S, Easley D. Pharmacological therapies for autism Spectrum disorder: a review. Pharm Ther. 2015;40(6):389–97.
Crystal S, Olfson M, Huang C, Pincus H, Gerhard T. Broadened use of atypical antipsychotics: safety, effectiveness, and policy challenges: expanded use of these medications, frequently off-label, has often outstripped the evidence base for the diverse range of patients who are treated with them. Health Aff. 2009;28(5):w770–81. https://doi.org/10.1377/hlthaff.28.5.w770.
Kamble P, Chen H, Johnson ML, Bhatara V, Aparasu RR. Concurrent use of stimulants and second-generation antipsychotics among children with ADHD enrolled in Medicaid. Psychiatr Serv. 2015;66(4):404–10. https://doi.org/10.1176/appi.ps.201300391.
Acknowledgments
N/A
Funding
This study was funded in part through a contract between the University of Pennsylvania, Community Behavioral Health, and the Department of Behavioral Health and Intellectual disAbility Services of Philadelphia. The funder facilitated administrative data collection and management and granted the authors a Data License Agreement to permit publication.
Author information
Authors and Affiliations
Contributions
All authors conceptualized and designed the study and critically reviewed the manuscript for important intellectual content. Dr. Candon drafted the manuscript and performed data analyses. Ms. Shen and Dr. Smith performed data analyses. Dr. Rothbard and Dr. Fadeyibi coordinated, supervised, and interpreted data analyses. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Institutional Review Boards of the City of Philadelphia and the University of Pennsylvania, who also approved a waiver of informed consent on the grounds that (a) the research involves no more than minimal risk to participants; (b) the waiver will not adversely affect the rights and welfare of participants; and (c) this research, which was retrospective and used secondary data, could not be practically carried out without the waiver. All methods were performed in accordance with the relevant guidelines and regulations.
Consent for publication
N/A
Competing interests
The authors have no relevant financial or non-financial interests related to the present study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Candon, M., Shen, S., Fadeyibi, O. et al. Trends in antipsychotic prescribing for approved and unapproved indications to Medicaid-enrolled youth in Philadelphia, Pennsylvania between 2014 and 2018. BMC Psychiatry 21, 524 (2021). https://doi.org/10.1186/s12888-021-03533-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-021-03533-3