
Abstract
Background
The Patient Health Questionnaire-9 (PHQ-9) has been proposed as a reliable and valid screening instrument for depressive symptoms with one latent factor. However, studies explicitly testing alternative model structures found support for a two-dimensional structure reflecting a somatic and a cognitive-affective dimension. We investigated the bidimensional structure of the PHQ-9, with a somatic (sleeping problems, fatigability, appetitive problems, and psychomotor retardation) and a cognitive-affective dimension (lack of interest, depressed mood, negative feelings about self, concentration problems, and suicidal ideation), and tested for sex- and regional-differences.
Methods
We have included data from the GEnder-Sensitive Analyses of mental health trajectories and implications for prevention: A multi-cohort consortium (GESA). Privacy-preserving analyses to provide information on the overall population and cohort-specific information and analyses of variance to compare depressive, somatic and cognitive-affective symptoms between sexes and cohorts were executed in DataSHIELD. In order to determine the dimensionality and measurement invariance of the PHQ-9 we tested three models (1 factor, 2 correlated factors, and bifactor) via confirmatory analyses and performed multi-group confirmatory factor analysis.
Results
Differences between sex and cohorts exist for PHQ-9 and for both of its dimensions. Women reported depressive symptoms in general as well as somatic and cognitive-affective symptoms more frequently. For all tested models an acceptable to excellent fit was found, consistently indicating a better model fit for the two-factor and bifactor model. Scalar measurement invariance was established between women and men, the three cohorts, and their interaction.
Conclusions
The two facets of depression should be taken into account when using PHQ-9, while data also render support to a general factor. Somatic and cognitive-affective symptoms assessed by the PHQ-9 can be considered equivalent across women and men and between different German populations from different regions.
Similar content being viewed by others

Background
The Patient Health Questionnaire-9 (PHQ-9) [1] has been proposed as a reliable and valid screening instrument for assessing depressive symptoms with one latent factor [2, 3]. It is based on DSM-IV diagnostic criteria for major depressive symptoms, the core criteria also apply to DSM-V [4]. However, studies explicitly testing alternative model structures by confirmatory factor analyses found support for a two-dimensional structure of the PHQ-9 reflecting a somatic and a cognitive-affective dimension [5,6,7,8].
This distinction is consistent with the fact that the majority of depressed patients in primary care present with somatic, rather than psychological complaints. Based on 863 participants from the Heart and Soul Study in the U.S., de Jonge and colleagues [9] identified a somatic (sleeping problems, fatigability, appetitive problems, and psychomotor agitation/ retardation) and a cognitive symptom factor (lack of interest, depressed mood, negative feelings about self, concentration problems and suicidal ideation) in the PHQ-9 using a theoretical and a factor analytical approach. Excellent model fit was observed for the proposed bidimensional PHQ-9 structure. They found that somatic, but not cognitive depressive symptoms, were associated with reduced heart rate variability, which may indicate worse cardiovascular prognosis. Subsequent papers have underscored the validity of the distinction by differential associations of the somatic (and not the cognitive) dimension. Applying the bi-factor structure in the German Gutenberg Health Study [10] only the somatic factor was associated with inflammation, vascular function and adverse life style factors (obesity, hyperlipidemia). In the Dutch Nijmegen Biomedical Study (NBS) somatic, but not cognitive items of the Beck Depression Inventory (BDI) [11] were found to be associated with atherosclerosis [12].
In general, prevalence rates of depression differ between sexes. Women’s depression rates are known to exceed the men’s rates by a factor of two across populations [13]. Yet, the question has not been settled whether this gender gap reflects sex-related differences of vulnerability, help-seeking behaviors, symptom reporting, quality of symptoms, diagnosing or gender role socialization [14]. Men may express depression behaviorally by aggression, violence, alcohol, and drug use, increasing the risk of somatic disease. Women may present with expressed anhedonia, negative emotions, sleep, appetite and weight disturbance, worthlessness and guilt.
Despite the widespread use of the PHQ-9 in more than 25 languages, only two studies have examined the underlying bidimensional symptom structure with regard to sex-differences [14, 15]. In a sample of 1168 depressed patients after spinal cord injury in the U.S., Kalpakjian and colleagues [14] analyzed item pattern loading differences between men and women. They reported low congruence when comparing the two dimensions of the PHQ-9 for both sexes, e.g. psychomotor disturbances loading on the somatic factor for women, but not for men. Using data nationally representative for the U.S. of 31,366 adult participants from the National Health and Nutrition Examination Survey (NHANES) who had filled out the PHQ-9 in one of several surveys from 2005 to 2016, Patel and colleagues [15] found a two-factor structure. However, discrepant to de Jonge and colleagues [9] and Michal and colleagues [10], the somatic dimension contained three items: sleep disturbance, fatigue and appetite changes (excluding psychomotor disturbances). The other six items were assigned to the cognitive-affective dimension. Strict measurement invariance of the bidimensional PHQ-9 held across sex. Psychometric properties would have also supported the dimension structure proposed previously [9, 10].
The factor structure of the PHQ-9 has been examined in numerous countries and languages. For most countries and subgroups, a one-factor model of the PHQ-9 was found as best fitting to the data (e.g. in a large German cohort study, in Hispanic American women [16, 17], and the general population in Hong Kong [18]. However, a systematic review of the factor structure and measurement invariance of the PHQ-9 among Portuguese speaking people found evidence for both the one- and two factor models of the PHQ-9 [19]. As underlined by previous research, not only cross-cultural [15, 16, 20], but also regional variation [21] have long been considered crucial variables of influence regarding depressive symptoms. In the eastern and western states of Germany, different political and economic systems have evolved over the 40 years from the 2nd World War to reunification in 1990. Under Eastern socialist politics of gender equality, women have been more strongly involved in education and work life, whereas traditional roles prevailed in the western states. These differences between formally eastern and western Germany potentially affect women to answer the PHQ-9 questionnaire distinctively in different regions.
Previous research has shown that the PHQ-9 is a valid screening instrument for assessing depressive symptoms with one latent factor in the general population and among women and men. Studies explicitly testing a two-dimensional structure of the PHQ-9 reflecting a somatic and a cognitive-affective dimension found a better fit to the data using two dimensions. However, only very limited sex-specific findings for this two factor-structure exist. Among other countries and subgroups, mostly a one-factor structure for PHQ-9 was found. However, a review article including studies testing factor structure and measurement invariance of the PHQ-9 for Portuguese speaking people found support for both the one- and two-factor model.
Objective of the study
Beyond the widely common unidimensional PHQ-9 model, we investigated the bidimensional structure originally proposed by de Jonge and colleagues [9], and additionally tested a bifactor model incorporating a general factor and two specific factors [22] of the PHQ-9 for the German population taking sex differences into account. This study included data from several regions in Germany, therefore we were able to additionally test for potential socialization effects in examining the bidimensional structure of the PHQ-9 in Germany [23,24,25].
Methods
Study design and sample
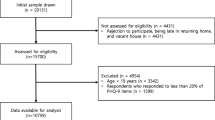
The GESA consortium (GEnder-Sensitive Analyses of mental health trajectories and implications for prevention: A multi-cohort consortium) [24] included three major, ongoing, longitudinal cohorts in middle, southern and northeast Germany: the Gutenberg Health Study (GHS) [26], the Cooperative Health Research in the Augsburg Region (KORA) [27, 28] and the Study of Health in Pomerania (SHIP) [29]. These regions differ in their socioeconomic and regional characteristics [24]. Middle and southern Germany are economically stronger than northeast Germany (e.g. higher discretionary incomes and lower unemployment rates). Furthermore, these regions differ with regard to life expectancy, which is lowest in northeast Germany. Lastly, regions differ with regard to religiosity. Religiosity is higher in southern Germany and lowest in northeast Germany [30]. Based on the assessments of specific psychosocial variables, different waves of these cohorts were selected for the GESA consortium [24]. For this study GHS F1, KORA F4 and SHIP3 including data from the years 2006–2016 were selected, 304 (1.5%) (GHS 278, KORA 16 and SHIP 10) respondents with missings on all PHQ-9 items were excluded, which lead to a total sample of N = 19,504.
Measures
The PHQ-9 was administered through questionnaires, either within a face-to-face interview (KORA) or filled out by the respondents (GHS, SHIP), to assess depressive symptoms over the past 2 weeks [1, 31]. Respondents indicated, on a 0–3 scale (0 = not at all; 1 = several days; 2 = more than half the days; 3 = nearly every day) the frequency with which they experienced the following symptoms: (a) anhedonia, (b) depressed mood, (c) sleep disturbance, (d) fatigue, (e) appetite changes, (f) low self-esteem, (g) concentration difficulties, (h) psychomotor disturbances, and (i) suicidal ideation. The total scores range from 0 to 27, with scores ≥10 representing clinical moderate to severe depression [1, 32]. Internal consistency of the entire questionnaire is excellent [1, 8]. Variables for a somatic depression scale and a cognitive-affective depression scale were constructed. For somatic depression the items sleep disturbance, fatigue, appetite changes, and psychomotor disturbances were combined and its total sum score ranged from 0 to 12. For cognitive-affective depression the items anhedonia, depressed mood, low self-esteem, concentration problems and suicidal ideation were combined and with a total sum score from 0 to 15.
Sociodemographic factors sex, age, years of education, marital status, living with partner, number of persons in household, employment and household income were examined. The sample consisted of 9813 females (7304 GHS; 1592 KORA; 917 SHIP) and 9691 males (7428 GHS, 1472 KORA; 791 SHIP). Age ranged from 20 to 79 (M = 55.5; SD = 11.6). For full details of the variable harmonization process, see Additional Table 1.
Data analysis
Analyses were performed in DataSHIELD version 4.1 [33,34,35], which is a system for privacy-preserving analyses where individual-level data of different cohorts does not have to be pooled for joint analyses. DataSHIELD allows for analyses via several R packages, based on R-version 3.5.2 [36]. First, we performed descriptive analyses in DataSHIELD in order to provide information on the overall population and the population per cohort. Second, covariances between the items of the PHQ-9 were calculated. The covariance matrices were exported to R and used to perform confirmatory factor analysis (CFA) as well as multi-group confirmatory factor analysis (MG-CFA) with the Lavaan R-package 3.6.1 [37].
The CFAs were conducted to test the one-dimensional, two-dimensional and the bifactor model version of the PHQ-9 for women and men. In our confirmatory analyses (CFA), the variance of each latent variable was fixed to 1.0 for scaling purposes [38]. A good model fit is indicated by a non-significant (p-value > 0.05) or a χ2-value/df ≤ 3 [39]. In order to justify the baseline model, we considered the following fit indices: standardized root mean square residual (SRMR) root mean square error of approximation (RMSEA), Tucker-Lewis index (TLI), and comparative fit index (CFI). The results of McNeish, An, and Hancock [40] suggest adapting the levels at which good and acceptable fit are defined to the level of measurement quality, in particular the size of the factor loadings, which might lead to lower thresholds for models with better measurement. Thus, the respective cut-offs for good/acceptable/mediocre model fit are: RMSEA ≤ .060/ .080/ .100, SRMR ≤ .050/ .070/ .090, and TLI/CFI ≥ .900/ .850/ .800.
In order to determine measurement invariance of the PHQ-9 between sex, cohorts, and sex within the cohorts, we applied multi-group confirmatory factor analysis (MGCFA). In these MG-CFA’s, four models were tested sequentially, whereby each level measures an additional restriction on the model. These models are the configural, metric, scalar and strict model testing invariance for the factor structure, factor loadings, intercept values and error variance between groups. Measurement invariance testing included a series of model comparisons by applying adjusted χ2-difference tests [41]. A non-significant χ2-difference (p ≥ .010) indicates measurement invariance among the tested models. As the χ2-statistic is sensitive to sample size, we focus on the differences ΔCFI and ΔRMSEA. Values ≤ .010 indicate the invariance of the models [42, 43]. Finally, analyses of variance (ANOVA) was performed to compare women and men, the GHS, KORA and SHIP cohort and women and men within the cohorts on their scores on overall depressive symptoms, somatic and cognitive-affective depressive symptoms.
For this study, all methods were carried out in accordance with current guidelines and regulations.
Results
Sociodemographic characteristics
In all cohorts, depressive symptoms were more often present in women. Additionally, women scored higher than men on both the somatic and cognitive-affective dimension of depression. Male participants were on average slightly older, more often married, fulltime employed and had a higher household income. In the GHS and KORA cohort, men reported more educational years and more often lived with a partner compared to women. In SHIP these differences were not found. The number of persons in the household were only statistically significant between women and men in the GHS cohort, yet with neglectable effect size. For details, see Table 1.
PHQ-9 factor structure
In the CFA, the one-, the correlated two-factor (cognitive-affective and a somatic dimension), and the bifactor model (general depression factor plus the two specific factors cognitive-affective and somatic depression) of the PHQ-9 were tested for the complete sample and for women and men separately. For an overview of all three tested models of the PHQ-9, see Additional Figure 1.
In order to determine the optimal factor structure of the PHQ-9, we conducted CFAs for women and men separately, for the complete sample, and stratified for cohorts (see Table 2). While the χ2/ df ≤ 3 ratio [44] indicated bad model fit in sum for all considered sample combination, other indices implied acceptable to excellent model fit for both the one- and two-factor models. Yet, the one-factor model consistently showed worse model fit compared to the correlated two-factor or bifactor model. This indicates the statistical superiority of the correlated two-factor and the bifactor model. According to the global model fit indices, on the one hand, the bifactor model turned out to fit data best. However, for two subgroups (KORA total sample and SHIP total sample) estimation problems occurred in the bifactor models. For four subgroups (men, GHS men, KORA women, SHIP women) estimation problems also occurred, but could be solved by applying the bifactor-(S·I – 1) model, as proposed by Eid and colleagues [45], using the fatigue item (item 4) as reference for the general factor. On the other hand, factor loadings and reliability coefficients ω are higher in the correlated two-factor model compared to the bifactor model. In the two-factor models both PHQ-9 subscales were highly correlated r = .875 overall, among women r = .883, and men r = .865 in the entire sample. In addition, sex and cohort stratified analyses emphasize the superiority of the two-factor model. The factor correlation between both dimensions varied when analyzing at cohort level: in KORA, the correlation between both dimensions was the highest overall/men/women r = .925/ .935/ .913; followed by SHIP: overall/men/women r = .898/ .866/ .902 and GHS: overall/men/women r = .860/ .850/ .870. Internal consistencies of the subscales (overall, women and men McDonald’s ω = .89–.95) and the overall scales (overall, women and men McDonald’s ω = .96) were good to excellent (see Table 3).
Factor loadings for the three competing models were estimated for the entire sample and for subpopulations stratified by sex and cohort (see Table 3). The highest factor loadings were observed for item 2 (depressed mood – cognitive-affective) and item 4 (fatigue - somatic), irrespective of the underlying factor model solution. Thus, both items can be regarded as marker variables for each dimension.
When comparing descriptive statistics at the item level (see Table 3), the highest scores were reported for the somatic factor item 3 (sleep problems), followed by item 4 (fatigue), for women and men across cohorts. The lowest scores were reported for the cognitive-affective item 9 (suicidal ideation) followed by either item 8 (psychomotor problems) or item 6 (low self-esteem). In sum, descriptive statistic patterns regarding overall item rank orders between men and women in the three cohorts appear to be similar.
PHQ-9 measurement invariance across sex, cohort and their interaction
In order to further evaluate the two-dimensional PHQ-9 we performed MG-CFA. Since we encountered estimation problems for subgroups when applying bifactor models, MG-CFA were tested only for the correlated two-factor model. The results are shown in Table 4. For the MGCFA including sex, the configural model had an acceptable model fit (CFI value 0.95, RMSEA value 0.06). The changes in CFI and RMSEA in the metric compared to the configural model and the scalar compared to the metric model were smaller than 0.01. This indicated that factor structures, factor loadings and intercept values are similar for women and men. In the strict model, the change in CFI was slightly above 0.01, but since the change in RMSEA was smaller than 0.01, this model was still invariant and indicated that the error variances were equal for both sexes. When analyzing the cohorts separately, results were similar. In the configural model, the CFI value was 0.95 and the RMSEA value slightly above 0.06. These values indicate an acceptable model fit. The changes in CFI and RMSEA between the metric and configural, and the scalar and the metric model did not exceed 0.01, which indicates equal factor structure, factor loadings and intercept values between the cohorts. In the strict model, the change in CFI was above 0.01, but the change in RMSEA smaller than .01, still indicating an invariant model and equal error variances between the cohorts.When testing measurement invariance for the two-dimensional PHQ-9 for sex and cohort, in the configural model, the CFI value was slightly below 0.95 and the RMSEA value slightly above 0.06. This indicated a good fit of the model. The changes in CFI and RMSEA between the metric and configural and the scalar and the metric model did respectively slightly exceed and not exceed 0.01, which indicated equal factor structure, factor loadings and intercept values between the sexes within the different cohorts. The changes in CFI and RMSEA between the strict and the scalar model were higher than 0.01. This indicated that this last restriction caused the model to fit the data worse. It implied that the error variances between the sexes in the different cohorts differed from each other. Since this difference was only present on the strict scale, one can conclude that the bidimensional structure of the PHQ-9 can be applied when measuring sex in the three different cohorts.
Frequency and distribution of depressive symptoms
Overall, 7.1% of the respondents suffered from clinically relevant depressive symptoms. Across cohorts, women were more frequently affected (8.7%) than men (5.5%). Mean scores for somatic depression vs. cognitive-affective depression were 2.3 (SD = 1.99), respectively 1.6 (SD = 1.91) overall. Women scored higher on both PHQ-9 subscales; 2.6 (SD = 2.07) on the somatic scale (versus 2.0 (SD = 1.86) for men) and 1.8 (SD = 1.97) on the cognitive-affective scale (versus a score of 1.4 (SD = 1.82) for men) with small effect sizes. In sum, GHS participants of both sexes reported higher scores on the somatic and cognitive-affective scale compared to their KORA and SHIP counterparts, but with negligible differences. Larger differences between cohorts were observed for the somatic factor compared to the cognitive-affective factor. While differences between cohorts and sexes were significant, their interaction did not reveal significant effects. Detailed ANOVA results are displayed in Additional Table 2 (one-way ANOVA) and Additional Table 3a and b (two-way ANOVA).
Discussion
Due to its brevity and its compatibility with the DSM-IV and DSM-V definitions of major depression, the PHQ-9 has become one of the mostly used screening measures for depressive symptoms. A bidimensional structure describing somatic, respectively cognitive-affective symptoms is clinically highly plausible establishing links to risk factors for cardiovascular disease, one of the major sequelae of depression [9, 10]. While depressive symptoms are presumed to differ between men and women, only two studies to date have compared patterns between men and women based on the PHQ-9 [14, 15].
We therefore investigated the common unidimensional model, the bidimensional structure originally proposed by de Jonge and colleagues [9], and additionally tested a bifactor model incorporating a general factor and two specific factors of the PHQ-9 for the German population taking sex differences into account. Using data of three large cohort studies from different areas in Germany, we were able to include regional variation of symptom patterns. In general, 7.1% of the respondents suffered from clinically relevant depressive symptoms. CFA revealed acceptable to excellent model fit for all three models. However, the correlated two-factor and bifactor models consistently showed better model fit than the one-factor model. Across cohorts, depressive symptoms and somatic and cognitive-affective symptoms were stronger present in women. Analyses of variance confirmed differences between sex and between cohorts for PHQ-9 and for both of its dimensions. Overall, we demonstrated factorial validity and provided psychometric data regarding the bidimensional PHQ-9 for the German population. Although our data clearly supports the incorporation of both facets of depression, the bifactor model tests also provide evidence justifying the assumption of a general depression factor. Scalar, but not strict measurement invariance were established between women and men, the three cohorts, and their interaction. Thus, we provided evidence that psychometrically meaningful interpretations of observed mean score differences when using the two PHQ-9 dimensions to compare the tested groups can be made. Somatic and cognitive-affective symptoms assessed by the PHQ-9 can be considered equivalent across women and men and between different German populations from different regions.
Thus, our data support previous sex-specific findings of Patel and colleagues [15] and differed from the findings of Kalpakjian and colleagues [14]. However, based on our two-correlated factor and bifactor model, we endorse the previous four-item scale of somatic symptoms including fatigue, appetite changes, sleep and psychomotor disturbances. The cognitive –affective dimension consists of depressed mood, low self-esteem, anhedonia, concentration difficulties and suicidal ideation. Irrespective of the underlying factor model solution, the highest factor loadings were observed for item 2 (depressed mood – cognitive-affective) and item 4 (fatigue - somatic).
A strength of the study is the large sample using of three cohorts across the life range and different living conditions, with equal proportions of men and women. Participants were recruited from the general population of the Eastern German States (SHIP), from middle (GHS) and southern Germany (KORA). Thus, cohorts differed regarding gender-related characteristics. As expected, there was a large gender gap between women and men in the western states regarding education, employment and household income. Thirty years after German reunification, there were also indicators for a gender gap in the SHIP cohort from the Eastern German states regarding household income and a higher rate of fully employed men vs. women. At the same time, more women worked full-time compared to the cohorts from the western states, there was a low rate of marginal employment among women, and women had a level of education comparable to men. Thus, findings are stable under different degrees of gender gap.
Limitations and outlook
The empirical results reported herein should be considered in the light of some limitations. First, the interpretation is limited by a small number of external variables for validation. While we considered relevant sociodemographic differences between women and men in the analyses, we had no specific gender measure to assess sex role behavior or identity. Second, future studies should define and validate separate cut-off scores for the somatic and the cognitive-affective dimensions. Nonetheless, the use of cut-off scores to examine depression and consequently for dimensions of depression is a controversial issue. For depression, ambiguity of the optimal screening measure exists [46]. Cut-off scores can be preferable over other screening measures e.g. diagnostic algorithms [47], since accuracy is better when screening for major depression with PHQ-9. A cut-off score of ≥10 maximizes the sensitivity and specificity of the PHQ-9 in the general population [48]. Yet, compared to diagnostic criteria, the cut-off score of ≥10 for the PHQ-9 tends to overestimate prevalence of depression [49,50,51]. Fried and colleagues [52] argue that cut-off scores for depression should only be applied in case of confirmed uni-dimensionality and established measurement invariance. In our study, where we confirmed a multifactorial structure of the PHQ-9, a sum score should only be calculated when the constructs are highly correlated [52]. A strong latent factor correlation was present in our findings (total sample r = .875, women r = .883, men r = .865), therefore one could apply a calculated PHQ-9 sum score, which is also supported by the good internal consistency of a one-factor solution. Therefore, when screening for depression, the PHQ-9 is an adequate instrument. However, our results also emphasize that it is preferable to use a somatic and cognitive-affective dimension in epidemiological studies. Third, future studies should further test the two-dimensional structure of the PHQ-9 in other subpopulations. Our study showed consistent findings between women and men and populations from different German regions, but that could be different for other subpopulations. For example, scores of depressive symptoms based on PHQ-9 were much higher in cancer patients [53] and coronary heart disease patients [54] compared to the general population. Additionally, a similar but not identical two-dimensional structure of the PHQ-9 was identified in cancer patients [55]. Therefore, the underlying dimensional structure of the PHQ-9 could also differ in subgroups and focusing on somatic and cognitive-affective symptoms could be especially helpful in chronically physically ill patients. Our results provide a fundamental basis to examine somatic and cognitive-affective symptoms assessed by the PHQ-9 in women and men in the German population.
Conclusions
Psychometrically meaningful interpretations of observed mean score differences when using the two PHQ-9 dimensions to compare the tested groups can be made. Somatic symptoms (fatigue, appetite changes, sleep and psychomotor disturbances) and cognitive-affective symptoms (depressed mood, low self-esteem, anhedonia, concentration difficulties and suicidal ideation) assessed by the PHQ-9 can be considered equivalent across women and men and between different German populations from different regions.
Availability of data and materials
The data that support the findings of this study are available from Freiburg Center of Data Analysis and Modelling, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of each individual cohort (GHS, KORA and SHIP). Data can only be analysed within the program DataSHIELD. This is a system for privacy-preserving analyses where individual-level data of different cohorts does not have to be pooled for joint analyses. Codes are available from DZ of the Center of Data Analysis and Modelling upon reasonable request. For this study, all methods were carried out in accordance with current guidelines and regulations.
Change history
29 October 2021
The funding note was missing in the original publication. The article has been updated to rectify the error.
Abbreviations
- ANOVA:
-
Analyses of variance
- CFA:
-
Confirmatory factor analysis
- CFI:
-
Comparative fit index
- GESA:
-
GEnder-Sensitive Analyses of mental health trajectories and implications for prevention: A multi-cohort consortium
- GHS:
-
Gutenberg Health Study
- KORA:
-
Cooperative Health Research in the Augsburg Region
- MCGFA:
-
Multi-group confirmatory factor analysis
- PHQ-9:
-
Patient Health Questionnaire-9
- RMSEA:
-
Root mean square error of approximation
- SHIP:
-
Study of Health in Pomerania
- SRMR:
-
Standardized root mean square residual
- TLI:
-
Tucker-Lewis index
References
Kroenke K, Spitzer RL, Williams JBW. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–13. https://doi.org/10.1046/j.1525-1497.2001.016009606.x.
Gilbody S, Richards D, Brealey S, Hewitt C. Screening for depression in medical settings with the patient health questionnaire (PHQ): a diagnostic meta-analysis. J Gen Intern Med. 2007;22(11):1596–602. https://doi.org/10.1007/s11606-007-0333-y.
Moriarty AS, Gilbody S, McMillan D, Manea L. Screening and case finding for major depressive disorder using the patient health questionnaire (PHQ-9): a meta-analysis. Gen Hosp Psychiatry. 2015;37(6):567–76. https://doi.org/10.1016/j.genhosppsych.2015.06.012.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders (DSM-5), Fifth Edition. Washington, DC: American Psychiatric Association; 2013. https://doi.org/10.1176/appi.books.9780890425596.
Krause JS, Bombardier C, Carter RE. Assessment of depressive symptoms during inpatient rehabilitation for spinal cord injury: is there an underlying somatic factor when using the PHQ? Rehabil Psychol. 2008;53(4):513–20. https://doi.org/10.1037/a0013354.
Richardson EJ, Richards JS. Factor structure of the PHQ-9 screen for depression across time since injury among persons with spinal cord injury. Rehabil Psychol. 2008;53(2):243–9. https://doi.org/10.1037/0090-5550.53.2.243.
Elhai JD, Contractor AA, Tamburrino M, Fine TH, Prescott MR, Shirley E, et al. The factor structure of major depression symptoms: a test of four competing models using the patient health Questionnaire-9. Psychiatry Res. 2012;199(3):169–73. https://doi.org/10.1016/j.psychres.2012.05.018.
Kocalevent RD, Hinz A, Brahler E. Standardization of the depression screener patient health questionnaire (PHQ-9) in the general population. Gen Hosp Psychiatry. 2013;35(5):551–5. https://doi.org/10.1016/j.genhosppsych.2013.04.006.
de Jonge P, Mangano D, Whooley MA. Differential association of cognitive and somatic depressive symptoms with heart rate variability in patients with stable coronary heart disease: findings from the heart and soul study. Psychosom Med. 2007;69(8):735–9. https://doi.org/10.1097/PSY.0b013e31815743ca.
Michal M, Wiltink J, Kirschner Y, Wild PS, Münzel T, Ojeda FM, et al. Differential Associations of Depressive Symptom Dimensions with Cardio-Vascular Disease in the Community: Results from the Gutenberg Health Study. PLoS One. 2013;8(8). https://doi.org/10.1371/journal.pone.0072014.
Beck AT, Steer RA. Internal consistencies of the original and revised Beck depression inventory. J Clin Psychol Med Settings. 1984;40(6):1365–7. https://doi.org/10.1002/1097-4679(198411)40:6<1365::AID-JCLP2270400615>3.0.CO;2-D.
Bus BA, Marijnissen RM, Holewijn S, Franke B, Purandare N, de Graaf J, et al. Depressive symptom clusters are differentially associated with atherosclerotic disease. Psychol Med. 2011;41(7):1419–28. https://doi.org/10.1017/S0033291710002151.
Kuehner C. Why is depression more common among women than among men? Lancet Psychiatry. 2017;4(2):146–58. https://doi.org/10.1016/S2215-0366(16)30263-2.
Kalpakjian CZ, Toussaint LL, Albright KJ, Bombardier CH, Krause JK, Tate DG. Patient health Questionnaire-9 in spinal cord injury: an examination of factor structure as related to gender. J Spinal Cord Med. 2009;32(2):147–56. https://doi.org/10.1080/10790268.2009.11760766.
Patel JS, Oh Y, Rand KL, Wu W, Cyders MA, Kroenke K, et al. Measurement invariance of the patient health questionnaire-9 (PHQ-9) depression screener in U.S. adults across sex, race/ethnicity, and education level: NHANES 2005–2016. Depress Anxiety. 2019;36(9):813–23. https://doi.org/10.1002/da.22940.
Tibubos AN, Beutel ME, Schulz A, Klein EM, Brähler E, Michal M, et al. Is assessment of depression equivalent for migrants of different cultural backgrounds? Results from the German population-based Gutenberg health study (GHS). Depress Anxiety. 2018;35(12):1178–89. https://doi.org/10.1002/da.22831.
Merz EL, Malcarne VL, Roesch SC, Riley N, Sadler GR. A multigroup confirmatory factor analysis of the patient health Questionnaire-9 among English- and Spanish-speaking Latinas. Cultur Divers Ethnic Minor Psychol. 2011;17(3):309–16. https://doi.org/10.1037/a0023883.
Yu X, Tam WWS, Wong PTK, Lam TH, Stewart SM. The patient health Questionnaire-9 for measuring depressive symptoms among the general population in Hong Kong. Compr Psychiatry. 2012;53(1):95–102. https://doi.org/10.1016/j.comppsych.2010.11.002.
Lamela D, Soreira C, Matos P, Morais A. Systematic review of the factor structure and measurement invariance of the patient health questionnaire-9 (PHQ-9) and validation of the Portuguese version in community settings. J Affect Disord. 2020;276:220–33. https://doi.org/10.1016/j.jad.2020.06.066.
Tibubos AN, Kröger H. A cross-cultural comparison of the ultrabrief mental health screeners PHQ-4 and SF-12 in Germany. Psychol Assess. 2020;32(7):690–7. https://doi.org/10.1037/pas0000814.
Alegria M, Atkins M, Farmer E, Slaton E, Stelk W. One size does not fit all: taking diversity, culture and context seriously. Admin Pol Ment Health. 2010;37(1):48–60. https://doi.org/10.1007/s10488-010-0283-2.
Rodriguez A, Reise SP, Haviland MG. Evaluating bifactor models: calculating and interpreting statistical indices. Psychol Methods. 2016;21(2):137–50. https://doi.org/10.1037/met0000045.
Beutel ME, Brähler E, Tibubos AN. Gender und psychische Gesundheit: Bedeutung für die psychotherapeutische Praxis. In: Moeslein-Teising I, Schäfer G, Martin R, editors. Geschlechter-Spannungen. 1 ed. Gießen: Psychosozial-Verlag; 2019. p. 54–65. https://doi.org/10.30820/9783837976229-54.
Burghardt J, Tibubos AN, Otten D, Brähler E, Binder H, Grabe H, et al. A multi-cohort consortium for GEnder-sensitive analyses of mental health trajectories and implications for prevention (GESA) in the general population in Germany. BMJ Open. 2020;10(2):e034220. https://doi.org/10.1136/bmjopen-2019-034220.
Otten D, Tibubos AN, Schomerus G, Brähler E, Binder H, Kruse J, et al. Similarities and differences of mental health in women and men: A systematic review of findings in three large German cohorts. Front Public Health. 2021;9(40). https://doi.org/10.3389/fpubh.2021.553071.
Wild P, Zeller T, Beutel M, Blettner M, Dugi K, Lackner K, et al. Die Gutenberg Gesundheitsstudie. Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz. 2012;55(6–7):824–30. https://doi.org/10.1007/s00103-012-1502-7.
Holle R, Happich M, Löwel H, Wichmann H-E, for the MONICA/KORA Study Group. KORA-a research platform for population based health research. Gesundheitswesen. 2005;67(S 01):19–25. https://doi.org/10.1055/s-2005-858235.
Jiang L, Atasoy S, Johar H, Herder C, Peters A, Kruse J, et al. Anxiety boosts progression of prediabetes to type 2 diabetes: findings from the prospective cooperative Health Research in the region of Augsburg F4 and FF4 studies. Diabet Med. 2020;37(10):1737–41. https://doi.org/10.1111/dme.14232.
Völzke H, Alte D, Schmidt CO, Radke D, Lorbeer R, Friedrich N, et al. Cohort profile: the study of health in Pomerania. Int J Epidemiol. 2011;40(2):294–307. https://doi.org/10.1093/ije/dyp394.
Forschungsgruppe Weltanschauungen in Deutschland. Religionszugehörigkeit nach Bundesland, 2002–2011. Retrieved from: https://fowid.de/meldung/religionszugehoerigkeit-nach-bundesland-2002-2011. Accessed 3 Dec 2020.
Kroenke K, Spitzer RL, Williams JB, Löwe B. The patient health questionnaire somatic, anxiety, and depressive symptom scales: a systematic review. Gen Hosp Psychiatry. 2010;32(4):345–59. https://doi.org/10.1016/j.genhosppsych.2010.03.006.
Kroenke K, Spitzer RL. The PHQ-9: a new depression diagnostic and severity measure. Psychiatr Ann. 2002;32(9):509–15. https://doi.org/10.3928/0048-5713-20020901-06.
Gaye A, Marcon Y, Isaeva J, LaFlamme P, Turner A, Jones EM, et al. DataSHIELD: taking the analysis to the data, not the data to the analysis. Int J Epidemiol. 2014;43(6):1929–44. https://doi.org/10.1093/ije/dyu188.
Jones EM, Sheehan NA, Masca N, Wallace SE, Murtagh MJ, Burton PR. DataSHIELD – shared individual-level analysis without sharing the data: a biostatistical perspective. Norsk Epidemiologi. 2012;21(2). https://doi.org/10.5324/nje.v21i2.1499.
Wilson RC, Butters OW, Avraam D, Baker J, Tedds JA, Turner A, et al. DataSHIELD – new directions and dimensions. Data Science Journal. 2017;16. https://doi.org/10.5334/dsj-2017-021.
R core Team. R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing; 2014.
Rosseel Y. Lavaan: An R Package for Structural Equation Modeling. J Stat Softw. 2012;48(2):1–36. https://doi.org/10.18637/jss.v048.i02.
Little TD, Slegers DW, Card NA. A non-arbitrary method of identifying and scaling latent variables in SEM and MACS models. Struct Equ Modeling. 2006;13(1):59–72. https://doi.org/10.1207/s15328007sem1301_3.
Kline RB. Promise and pitfalls of structural equation modeling in gifted research. Methodologies for conducting research on giftedness. Washington, DC, US: American Psychological Association; 2010. p. 147–69.
McNeish D, An J, Hancock GR. The thorny relation between measurement quality and fit index cutoffs in latent variable models. J Pers Assess. 2018;100(1):43–52. https://doi.org/10.1080/00223891.2017.1281286.
Satorra A, Bentler PM. A scaled difference chi-square test statistic for moment structure analysis. Psychometrika. 2001;66(4):507–14. https://doi.org/10.1007/BF02296192.
Cheung GW, Rensvold RB. Evaluating goodness-of-fit indexes for testing measurement invariance. Struct Equ Modeling. 2002;9(2):233–55. https://doi.org/10.1207/S15328007SEM0902_5.
Putnick DL, Bornstein MH. Measurement invariance conventions and reporting: the state of the art and future directions for psychological research. Dev Rev. 2016;41:71–90. https://doi.org/10.1016/j.dr.2016.06.004.
Schermelleh-Engel K, Moosbrugger H, Müller H. Evaluating the fit of structural equation models: tests of significance and descriptive goodness-of-fit measures. Psychol Methods. 2003;8:23–74.
Eid M, Geiser C, Koch T, Heene M. Anomalous results in G-factor models: explanations and alternatives. Psychol Methods. 2017;22(3):541–62. https://doi.org/10.1037/met0000083.
Joffres M, Jaramillo A, Dickinson J, Lewin G, Pottie K, Shaw E, et al. Recommendations on screening for depression in adults. Can Med Assoc J. 2013;185(9):775–82. https://doi.org/10.1503/cmaj.130403.
He C, Levis B, Riehm KE, Saadat N, Levis AW, Azar M, et al. The accuracy of the patient health Questionnaire-9 algorithm for screening to detect major depression: An individual participant data meta-analysis. Psychother Psychosom. 2020;89(1):25–37. https://doi.org/10.1159/000502294.
Levis B, Benedetti A, Thombs BD. Accuracy of patient health Questionnaire-9 (PHQ-9) for screening to detect major depression: individual participant data meta-analysis. BMJ. 2019;365:l1476. https://doi.org/10.1136/bmj.l1476.
Levis B, Benedetti A, Ioannidis JPA, Sun Y, Negeri Z, He C, et al. Patient Health Questionnaire-9 scores do not accurately estimate depression prevalence: individual participant data meta-analysis. J Clin Epidemiol. 2020;122:115–28.e1. https://doi.org/10.1016/j.jclinepi.2020.02.002.
Levis B, Yan XW, He C, Sun Y, Benedetti A, Thombs BD. Comparison of depression prevalence estimates in meta-analyses based on screening tools and rating scales versus diagnostic interviews: a meta-research review. BMC Med. 2019;17(1):65. https://doi.org/10.1186/s12916-019-1297-6.
Thombs BD, Kwakkenbos L, Levis AW, Benedetti A. Addressing overestimation of the prevalence of depression based on self-report screening questionnaires. Can Med Assoc J. 2018;190(2):E44–9. https://doi.org/10.1503/cmaj.170691.
Fried EI, van Borkulo CD, Epskamp S, Schoevers RA, Tuerlinckx F, Borsboom D. Measuring depression over time . . . Or not? Lack of unidimensionality and longitudinal measurement invariance in four common rating scales of depression. Psychol Assess. 2016;28(11):1354–67. https://doi.org/10.1037/pas0000275.
Hartung TJ, Brähler E, Faller H, Härter M, Hinz A, Johansen C, et al. The risk of being depressed is significantly higher in cancer patients than in the general population: prevalence and severity of depressive symptoms across major cancer types. Eur J Cancer. 2017;72:46–53. https://doi.org/10.1016/j.ejca.2016.11.017.
Lichtman JH, Bigger JT, Blumenthal JA, Frasure-Smith N, Kaufmann PG, Lespérance F, et al. Depression and coronary heart disease. Circulation. 2008;118(17):1768–75.56. https://doi.org/10.1161/CIRCULATIONAHA.108.190769.
Hinz A, Mehnert A, Kocalevent R-D, Brähler E, Forkmann T, Singer S, et al. Assessment of depression severity with the PHQ-9 in cancer patients and in the general population. BMC Psychiatry. 2016;16(1):22. https://doi.org/10.1186/s12888-016-0728-6.
Acknowledgements
The authors are grateful to all study participants. Further, the authors thank the staff involved in the planning, organisation and conduct of the GHS, KORA and SHIP study.
Funding
GESA is funded by the Federal Ministry of Education and Research (BMBF; Nr.01GL1718A). The Gutenberg Health Study (GHS) is funded through the government of Rhineland-Palatinate (“Stiftung Rheinland-Pfalz für Innovation”, contract AZ 961–386261/733), the research programs “Wissen schafft Zukunft” and “Center for Translational Vascular Biology (CTVB)” of the Johannes Gutenberg-University of Mainz, and its contracts with Boehringer Ingelheim, and PHILIPS Medical Systems, including an unrestricted grant for the Gutenberg Health Study. PSW is funded by the Federal Ministry of Education and Research (BMBF 01EO1503). PSW and TM are PI of the German Center for Vascular Research (DZHK). The KORA study was initiated and financed by the Helmholtz Zentrum München – German Research Center for Environmental Health, which is funded by the German Federal Ministry of Education and Research (BMBF) and by the State of Bavaria.
SHIP is part of the Community Medicine Research net of the University of Greifswald, which is funded by the Federal Ministry of Education and Research (01ZZ9603, 01ZZ0103, and 01ZZ0403), the Ministry of Cultural Affairs and the Social Ministry of the Federal State of Mecklenburg-West Pomerania. Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
This research article was written as part of the GESA Project. All authors contributed to the development and refinement of the GESA consortium. MB, EB, HB, HG, JKr, KL, GS and PSW are grant holders. AT, MB and EB devised the research question and proposal and the main conceptual ideas. The harmonization of the variables was an interactive process in which AT, DO, DZ, TF, LS, HJ and SA participated. DO performed the analyses with assistance of AT and DZ. AT, DO and MB wrote the manuscript. HB, DZ, PSW, KL, GS, BL, HG, JKr, CS, TM, JKö and EB provided critical feedback on the manuscript and herewith contributed to the final manuscript. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All three cohort studies included in the GESA consortium were approved by ethic committees.
GHS: The GHS and its procedure were approved by the ethics committee of the Statutory Board of Rhineland-Palatinate, Germany (approval at 22.3.2007, latest update 20.10.2015, reference no. 837.020.07). Participation was voluntary and written informed consent was obtained from each subject upon entry into the study.
KORA: All study methods were approved by the ethics committee of the Bavarian Chamber of Physicians, Munich (F4 and FF4: reference no. 06068).
SHIP: This institutional ethics committee of the University Medicine Greifswald evaluated the study, design and instruments and testified its compliance with ethical requirements (reference no. BB 39/08).
Consent for publication
Not applicable.
Competing interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Figure 1.
Overview of the Patient Health Questionnaire-9 (PHQ-9) models tested
Additional file 2: Table 1.
Harmonizing demographic variables.
Additional file 3: Table 2.
ANOVA of overall depressive symptoms, somatic, and cognitive-affective depressive symptoms stratified by cohorts or sex.
Additional file 4: Table 3a.
Descriptive statistics of overall depressive symptoms, somatic, and cognitive-affective depressive symptoms stratified by sex and cohorts. Table 3b. Two-way ANOVA of depression, somatic, cognitive-affective depression stratified by cohorts, sex and cohort*sex.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tibubos, A.N., Otten, D., Zöller, D. et al. Bidimensional structure and measurement equivalence of the Patient Health Questionnaire-9: sex-sensitive assessment of depressive symptoms in three representative German cohort studies. BMC Psychiatry 21, 238 (2021). https://doi.org/10.1186/s12888-021-03234-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-021-03234-x