
Abstract
Background
Depression is a common comorbidity among patients with type 2 diabetes. There are several reports supporting a bidirectional association between depression and type 2 diabetes. However, there is limited data from non-western countries. Therefore, the aim of this study was to assess the sociodemographic, clinical, and psychosocial factors associated with co-morbid depression among type 2 diabetic outpatients presenting to Black Lion General Specialized Hospital, Addis Ababa, Ethiopia.
Methods
This institution based cross-sectional study design was conducted on a random sample of 276 type 2 diabetic outpatients. Type 2 diabetes patients were evaluated for depression by administering a validated nine-item Patient Health Questionnaire (PHQ-9). Risk factors for depression among type 2 diabetes patients were identified using multiple logistic regression analysis.
Result
In total, 264 study participants were interviewed with a response rate of 95.6 %. The prevalence of depression was 44.7 %. In the multivariate analysis, the statistically significant risk factors for depression were monthly family income ≤ 650 (p-value = 0.056; OR = 2.0; 95 % CI = 1.01, 4.2), presence of ≥3 diabetic complications (p-value = 0.03; OR = 3.3; 95 % CI = 1.1, 10.0), diabetic nephropathy (p-value = 0.01; OR = 2.9; 95 % CI = 1.2, 6.7), negative life events (p-value = 0.01; OR = 2.4; 95 % CI = 1.2, 4.5), and poor social support (p-value = 0.001; OR = 2.7; 95 % CI = 1.5, 5.0).
Conclusion
This study demonstrated that depression is a common co-morbid health problem with a prevalence rate of 44.7 %. The presence of diabetic complications, low monthly family income, diabetic nephropathy, negative life event, and poor social support were the statistically significant risk factors associated with depression. We presume that the burden of mental health especially depression is high in the population with type 2 diabetes mellitus co-morbidity. Therefore, specific attention is needed to diagnose early and treat promptly.
Similar content being viewed by others

Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
The mental health consequences of diabetes have been studied by a number of research teams and they have reported bidirectional associations between depression and type 2 diabetes [1, 2]. In this study, we focused on the influence of type 2 diabetic associated problems on the presence of depressive symptoms. Based on the literature we classify these potential risk factors as sociodemographic, clinical, and psychosocial factors.
Several studies have shown that sociodemographic risk factors affect the development of co-morbid depression among diabetic patients. The prevalence rates of depression were significantly higher in females with type 2 diabetes mellitus compared with males with type 2 diabetes mellitus [3–6], varying from a doubled percentage for women than for men [7] and more than three times higher in women compared with men [3]. Other sociodemographic risk factors that were significantly associated with depression in people with diabetes includes age at diabetes diagnosis [8, 9], low socioeconomic status [3, 4, 6, 10], low educational status [1, 3, 4], being unmarried [1, 4, 9], urban dwelling [3], nature of relationship with sexual partners [11], ethnicity/race [12, 13], smoking habits [14–16], physical activity [14], sedentary life [8], and unemployment [17]. Some other studies, however, found that gender, age, residence, educational status, ethnicity, marital status, employment status, and socioeconomic status had no significant association with depression in diabetes patients [11, 17–19].
The effects of clinical and psychosocial factors on co-morbid depression have been supported by different studies as well. These factors encompass financial stress [1, 19, 20], poor social support [1, 4], negative life events [1, 19, 20], poor quality of life [20, 21], and medication burden [19, 22].
Depression was most strongly associated with functional impairment [1], large waist circumference [19], glycosylated hemoglobin level [1, 3], body mass index [7, 12], blood glucose level [3], diabetic retinopathy [23], diabetic neuropathy [1, 12, 19, 23], diabetic nephropathy [19, 23], peripheral vascular disease [19, 23], diabetic foot ulcer [19], coronary vascular disease [23], ischemic heart disease [16, 23], arteriosclerotic vascular disease [23], heart disorder [3], type of diabetic treatment [3, 24], and sexual dysfunction [23]. On the contrary depression was not significantly associated with poor body weight control, insulin treatment users, duration of diabetes, glycosylated hemoglobin (HbA1c), obesity, hypertensive disorder, retinopathy [3, 12, 17, 18].
The major barriers in diagnosing depression among type 2 diabetic patients were the lack of screening tool, time constraints, and overlapping of physical and cognitive symptoms [3, 25].
Thus, there are various sociodemographic, clinical, and psychosocial factors related to depression in type 2 diabetes mellitus. Identifying the significant predictors of depression is important to develop need-based clinical and community-based mental health interventions. Although these factors have been found to be associated with depression, most of these studies were based on Western samples, with only some exceptions. Therefore, we do not know whether these findings can be generalized to a non-western setting. Thus in the present study, we aimed to identify factors influencing the risk of co-morbid depression among patients with type 2 diabetes mellitus in patients treated at the Black Lion General Specialized Hospital in Ethiopia. We hypothesized that the same identified factors were associated with depression in this non-western sample.
Methods
Study site
Black Lion General Specialized Hospital (Tikur Anbessa in Amharic), located in the nation’s capital Addis Ababa, is Ethiopia’s largest general public hospital and one of University Hospitals in the country. The hospital provides a tertiary level referral treatment and is open for 24 h for emergency services. Black Lion hospital offers diagnosis and treatment for approximately 370,000- 400,000 patients a year [26].
Subjects and procedures
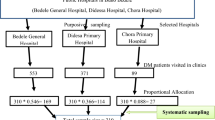
We conducted an institution based cross-sectional study design among 276 type 2 diabetic outpatients selected using systematic random sampling techniques from April 23, 2013 to May 13, 2013. Inclusion criteria were: (i) diagnosed as type 2 diabetic patients for at least one year, (ii) age ≥ 20 years old, and (iii) capable of independent communication and giving informed verbal consent. Individuals who were currently being treated for depression or other psychological problems (e.g. anxiety or personality disorders) as ascertained at recruitment were excluded. Patients with established type 2 diabetes mellitus were evaluated for depression by administering a validated nine-item questionnaire PHQ-9 (Amharic version-local language) [29].
Variables
The outcome variable is depression. The explanatory variables are sociodemographic, clinical, and psychosocial factors that were collected by patient interview and medical record review.
Tool reliability assessment
Cronbach’s α for the PHQ-9 scale was 0.72 indicating acceptable consistency of this psychometric scale for the study population. The correlations between nine items of the PHQ-9 and total PHQ-9 scores ranged from 0.22 to 0.69, and all correlations were significant at the 0.01 level.
Data analysis
After checking collected data visually for completeness, the response was coded and entered into the computer using EPI info version 3.5.1. Statistical packages, and then 10 % of the responses was randomly selected and checked for the consistency of data entry. Then printed frequencies were used for checking of outliers and to clean data. Data was cleaned accordingly and then exported to SPSS (Statistical package for Social Science) version 20.0 (IBM SPSS Corp.). Cleaned raw data is available as an additional file in a comma delimited (*.csv) format [Additional file 1]. The frequency distribution of dependent and independent variables was worked out. Multivariate logistic regression analysis was applied to identify statistically significant associated risk factors using significance level (α) 0.05. Odds ratios were calculated to determine the strength of associations of selected variables. The study was adherent to the STROBE criteria as outlined in Additional file 2.
Result
Sociodemographic characteristics
In total, 264 study participants were interviewed with a response rate of 95.6 %. Non response was due to participant’s lack of interest to participate, shortage of time, and critical illness. Of the interviewed participants 53.0 % (n = 140) were female, 69.3 % (n = 183) were married, 80.7 % (n = 213) were Orthodox Christian, and 57.2 % (n = 151) were Amhara. In addition, the mean ± SD age at diagnosis and current age of the subjects were 43.9 ± 10.9 and 55.9 ± 10.9 years, respectively. Besides, 86.4 % (n = 228) lived in Addis Ababa, and 61.7 % (n = 163) had a waist circumference of ≥ 95 cm (mean ± SD, 98.9 + 11.1). The median monthly income of the family was 750 ETB (651–1400 ETB) and 33.7 % (n = 89) had attended college/university level education.
Clinical characteristics
One hundred forty five patients (43.2 %) were on oral hypoglycemic treatment, 78.3 % (n = 141) had cardiovascular diseases (hypertension and heart failure), and 69.7 % (n = 140) had diabetic retinopathy. More than half (58.7 %, n = 155) of study participants reported 1 to 2 co-morbid disease (mean ± SD, 1.1 ± 0.9). Similarly, half of the respondents (n = 132) had a BMI ≤ 24.9 kg/m2 (mean ± SD, 25.4 ± 3.7). Regarding the laboratory reported fasting blood glucose level, 12.9 % (n = 34) had ≤ 100 mg/dl, 19.7 % (n = 52) 101–126 mg/dl, and 67.4 % (n = 178) had ≥ 127 mg/dl.
Prevalence of depression
The mean ± SD of PHQ 9 score was 5.2 ± 4.6. Twenty-five (9.5 %) type 2 diabetic outpatients did not report any of depressive symptoms, but 28.4 % of type 2 diabetic outpatients, fulfilled the criteria for mild depression, 12.1 % for moderate depression, 2.7 % for moderately severe depression, and 1.5 % for severe depression. Thus, the overall prevalence rate of depression was 44.7 %.
Statistical analysis
As revealed in Table 1, the prevalence of depressive symptoms was two times higher in female type 2 diabetic patients compared with male. This was found statistically significant. Other demographic variable that found risk for depression and statistically significant was monthly family income.
As shown in Table 2, among clinical variables the presence of diabetic complications (nephropathy, neuropathy, sexual dysfunction), body mass index 25.0–29.9 kg/m2 and, the presence of ≥3 co-morbid disease, and occurrence of 1–2 diabetic complication were found statistically significant risk factors of depression.
Negative life events in the last 6 months and poor social support were psychosocial risk factors significantly associated with depression. But, not fearing diabetic complication and doing daily recommended physical exercise were statistically significant preventive factors of depression among type 2 diabetic patients. This was presented in Table 3 below.
Table 4 depicted that, only monthly family income, presence of ≥3 diabetic complication, diabetic nephropathy, negative life event, and poor social support persisted as statistically significant risk factors for depression after controlling of other confounding factors.
Discussion
In the general diabetic population, it is difficult to accurately estimate the potential medical care needs and public health burdens of depression [28]. Unfortunately, in spite of the high impact of depression and diabetes comorbidity on the individual and its importance as a public health problem, little is known about the existence of depression in people with diabetes in Ethiopia. To our knowledge, this is the first study to assess sociodemographic, clinical, and psychosocial factors related to type 2 diabetes mellitus causing depression in a large sample. This study has tried to address this issue by identifying factors associated with depression in type 2 diabetic outpatients.
In this study low family monthly income was the significant independent predictor of depression. This result was consistent with other studies report [3, 4, 6, 10].
We found that sex, residence, marital status, ethnicity, educational status, waist circumference, current age, and age at diagnosis were not associated factors for depression. This study finding was also in line with several previous studies [11, 14, 17, 27].
However, many earlier published articles reported the prevalence rates of depression were significantly higher in females with type 2 diabetes mellitus compared with males with type 2 diabetes mellitus [3–5, 8–11]. Other demographic risk factors that were significantly associated in varying degree with depression in people with diabetes includes age at diabetes diagnosis [8, 9], low educational level [1, 3, 4], being unmarried [1, 4, 7], urban residence [3], nature of relationship with sexual partners [11], ethnicity/race [12, 13], smoking habits [14–16], physical activity [14], sedentary life [8], and unemployment [17]. This discrepancy was might be due to variation in study design, demographic characteristics of respondents, and selection method of respondents.
Regarding the clinical characteristics of participants, earlier studies conducted in different setting revealed depression was most strongly associated with large waist circumference [19], body mass index [7, 12], blood sugar level [3], diabetic retinopathy [23], diabetic neuropathy [1, 12, 19, 23], diabetic nephropathy [19, 23], peripherovascular disease [19, 23], diabetic foot ulcer [19], coronary vascular disease [23], ischemic heart disease [16, 23], arteriosclerotic vascular disease [23], heart disorder [3], type of diabetic treatment [3, 24], and sexual dysfunction [23].
Similarly, the result of this study demonstrated a significantly higher prevalence of depression in type 2 diabetic outpatients with the presence of ≥3 diabetic complication and diabetic nephropathy.
On the contrary depression was not significantly associated with diabetes treatment regimen co-morbid disease (cardiovascular, respiratory, renal, neurologic), complication of diabetes (retinopathy, neuropathy, sexual dysfunction), duration of diabetes, duration of diabetes treatment, fasting blood sugar, body mass index, number of co-morbidity, number of prescribed medication administration per day, and physical disability. This variation might be due to the level of country development, time frame, study setting, and lifestyle variation.
Moreover, we found out negative life events and poor social support were a statistically significantly psychosocial risk factor for depression. In line with this study the psychosocial factors that had a significant association with co-morbid depression comprises poor social support [2, 4] and experience chronic stressors or negative life events [2, 14, 17].
Previous studies also support increased health care costs/financial stress [2, 14, 20] and pill burden [14, 24] were associated factors for depression. Disparately, in this study high health care cost and medication burden were not associated with depression.
The outcomes of this study have implications for health care practice in Black Lion General Specialized Hospital and other health care organizations, where clinician’s diagnosis of psychiatric disorders rate is inadequate because of the high patient load, lack of screening tool, and poor undergraduate or in-service training in these skills. Principally this study has a presumption that the burden of mental health especially depression is high in the population with type 2 diabetes mellitus co-morbidity and requires attention to diagnose early and treat promptly. Laboratory test results and pharmacological treatment plan are not adequate to scaling up service delivery and bring about the expected change.
Limitations and strengths
The strengths of this study include a high response rate and the inclusive nature of this research as individuals could participate regardless of literacy level. Including patients from different ethnic backgrounds in Addis Ababa and outside Addis Ababa was a further strength. Additionally, rather than having to rely on self-report, health-related information was collected from patients’ medical records. Even though the association was temporary, depression and type 2 diabetes mellitus were causally related and deserves attention from clinicians to ensure better management. Also, a reasonable sample size and ascertaining depression with culturally standardized questionnaires are strengths of this study. Since it was the first study in type, it will provide basic information for those who are interested.
However, an important limitation of this study was that a psychiatric diagnostic interview which is considered as the gold standard for the diagnosis of depression was not used. Additionally, there was an absence of similar study done in Ethiopia health care setting to compare the finding. Moreover, due to cross-sectional nature of the study, causal relationships between depression and type 2 diabetes mellitus cannot be assumed.
Conclusion
In conclusion, this study demonstrated that depression is a common co-morbid health problem in type 2 diabetic out-patients in Black Lion General Specialized Hospital with a prevalence rate of 44.7 %. Within this sample of outpatients with type 2 diabetes mellitus, the study found that low monthly family income, presence of ≥3 diabetic complications, diabetic nephropathy, negative life event, and poor social support were highly statistically significant risk factors associated with depression. All the result should be interpreted cautiously and further prospective longitudinal research focusses on these sociodemographic and clinical factors in the different clinical group should be conducted. Finally, we presumed the burden of mental health especially depression is high in the population with type 2 diabetes mellitus co-morbidity and requires attention to diagnose early and treat promptly.
Ethics approval and consent to participate
In order to follow the ethical and legal standards of the scientific investigation, the study was conducted after the approval of the proposal by Addis Ababa University Institutional Review Board. Participation was voluntary and information was collected anonymously after obtaining written consent from each respondent by assuring confidentiality throughout the data collection period.
Consent for publication
Not applicable.
Availability of data and materials
The data is available to the concerned body when it is required.
References
Musselman DL, Betan E, Larsen H, Phillips LS. Relationship of Depression to Diabetes Types 1 and 2: Epidemiology, Biology, and Treatment. Biol Psychiatry. 2003;54:317–29.
Bogner HR, Morales KH, de Vries HF, Cappola AR. Integrated Management of Type 2 Diabetes Mellitus and Depression Treatment to Improve Medication Adherence: A Randomized Controlled Trial. Ann Fam Med. 2012;10(1):15–22.
Roy T, Lloyd CE, Parvin M, Mohiuddin KG, Rahman M. Prevalence of co-morbid depression in out-patients with type 2 diabetes in Bangladesh. BMC Psychiatry. 2012;12:123.
Charm Lindblad, Bruce A. Mann, Colleen Campbell, Alicia Chavez, Gloria Jean Collins, Sheila Conneen, et al.: Practical Information for New Mexico Health Care Professionals: A quarterly publication for clinicians caring for people with diabetes. 2011, 15(6).
Asghar S, Hussain A, Ali SM, Khan AK, Magnusson A. Prevalence of depression and diabetes: a population-based study from rural Bangladesh. Diabet Med. 2007;24:872–7.
Fisher L, Chesla CA, Mullan JT, Skaff M, Kanter RA. Contributors to depression in Latino and European-American patients with type 2 diabetes. Diabetes Care. 2001;24:1751–7.
Roupa Ζ, Κoulouri Α, Sotiropoulou P, Makrinika E, Marneras X, et al. Anxiety and depression in patients with Type 2 Diabetes Mellitus, depending on sex and body mass index. Health Sci J. 2009;3(1):32–40.
Ryerson B, Tierney EF, Thompson TJ, et al. Excess physical limitations among adults with diabetes in the U.S. population, 1997–1999. Diabetes Care. 2003;26:206–10.
Zahid N, Asghar S, Claussen B, Hussain A. Depression and diabetes in a rural community in Pakistan. Diabetes Res Clin Pract. 2007;79:124–7.
Everson SA, Maty SC, Lynch JW, Kaplan GA. Epidemiologic evidence for the relation between socioeconomic status and depression, obesity, and diabetes. J Psychosom Res. 2002;53:891–5.
Agbir TM, Audu MD, Adebowale TO, Goar SG. Depression among medical outpatients with diabetes: A cross-sectional study at Jos University Teaching Hospital, Jos, Nigeria. Ann Afr Med. 2010;9(1):5–10.
Pouwer F, Geelhoed-Duijvestijn PH, Tack CJ, Bazelmans E, Beekman AJ, et al. Prevalence of comorbid depression is high in out-patients with Type 1 or Type 2 diabetes mellitus: Results from three out-patient clinics in the Netherlands. Diabet Med. 2010;27:217–24.
Lustman PJ, Anderson RJ, Freedland KE, de Groot M, Carney RM, et al. Depression and Poor Glycemic Control: A meta-analytic review of the literature. Diabetes Care. 2000;23(7):934–42.
Egede LE, Zheng D. Independent factors associated with major depressive disorder in a national sample of individuals with diabetes. Diabetes Care. 2003;26:104–11.
Katon W, Von Korff M, Ciechanowski P, et al. Behavioral and clinical factors associated with depression among individuals with diabetes. Diabetes Care. 2004;27:914–20.
Guruprasad KG, Niranjan MR, Ashwin S. A Study of Association of Depressive Symptoms Among the Type 2 Diabetic Outpatients Presenting to a Tertiary Care Hospital. Indian J Psychol Med. 2012;34(1):30–3.
Egede LE, Ellis C. The Effects of Depression on Diabetes Knowledge, Diabetes Self-Management, and Perceived Control in Indigent Patients with Type 2 Diabetes. Diabetes Technol Ther. 2008;10(3):213–9.
Raval A, Dhanaraj E, Bhansali A, Grover S, Tiwari P. Prevalence & determinants of depression in type 2 diabetes patients in a tertiary care center. Indian J Med Res. 2010;132:195–200.
Naranjo DM, Fisher L, Areán PA, Hessler D, Mullan J. Patients with Type 2 Diabetes at Risk for Major Depressive Disorder Over Time. Ann Fam Med. 2011;9(2):115–20.
Ell K, Katon W, Cabassa LJ, Xie B, Lee PJ, et al. Depression and diabetes among low-income hispanics: design elements of a socio-culturally adapted collaborative care model randomized controlled trial. Int J Psychiatry. 2009;39(2):113–32.
Hermanns N, Kulzer B. Diabetes and Depression – A Burdensome Co-morbidity: a report. Eur Endocrinol. 2008;4(2):19–22.
Gilmer TP, Walker C, Johnson ED, Philis-Tsimikas A, Unützer J. Improving Treatment of Depression among Latinos With Diabetes Using Project Dulce and IMPACT. Diabetes Care. 2008;31(7):1324–6.
De Groot M, Anderson R, Freedland KE, Clouse RE, Lustman PJ. Association of Depression and Diabetes Complications: A Meta-Analysis. Psychosom Med. 2001;63:619–30.
Li C, Ford ES, Strine TW, Mokdad AH. Prevalence of depression among U.S. adults with diabetes: findings from the 2006 behavioral risk factor surveillance system. Diabetes Care. 2008;31:105–7.
Acee AM. Detecting and managing depression in type II diabetes: PHQ-9 is the answer! (Advanced Practice)(Disease/Disorder overview). Med Surg Nursing. 2010;19(1):32–9.
Alex's Medical and Educational Clinic (AMECA) in Africa. Black Lion Specialized Hospital. Retrieved on April 11, 2016 from http://ameca.org.uk/directory/listing/black-lion-specialized-hospital-ethiopia.
McIntyre RS, Mancini DA, Pearce MM, Silverstone P, Chue P, et al. Mood and Psychotic Disorders and Type 2 Diabetes: A Metabolic Triad. Can J Diabetes. 2005;29(2):122–32.
Khamseh ME, Baradaran HR, Rajabali H. Depression and diabetes in Iranian patients: a comparative study. Int J Psychiatry Med. 2007;37:81–6.
Gelaye B, Williams MA, Lemma S, Deyessa N, Bahretibeb Y, Shibre T, et al. Validity of the patient health questionnaire-9 for depression screening and diagnosis in East Africa. Psychiatry Res. 2013;210:653–61.
Acknowledgement
We would like to address our sincerest and heart –felt gratitude to our advisor Yoseph Tsige (Associate professor) and Dr. Abdurazak Ahmed (MD) for their concrete and expert advice, suggestions, and assistance in all aspects of this research work.
Our in-depth gratitude also goes to Addis Ababa University, College of Health Science, School of Allied Health science, Department of Nursing and Midwifery, for giving this chance and approval of the study too.
We would like to thank Dr. Yewondweson Tadesse, department head of Internal Medicine; Dr. Tedilla Kebede, Physicians coordinator in diabetes clinic; Sr. Abeba Mulugeta, Nurses coordinator in the diabetic clinic; in Black Lion General Specialized Hospital for their collaboration to permit and facilitate data collection.
Supervisors, data collectors, and respondents were highly acknowledged for investing their precious time in supervising, collecting data and providing the necessary information.
We would like to offer our great respect and appreciation to all our friends and senior instructors who gave us precious time for advice and comments during data entry and analysis.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interest
The authors declare that there is no conflict of interests regarding the publication of this research article.
Authors’ contributions
TD conceived and designed the study. SM supervised data collection and analyzed the data. YG drafted the manuscript. Additionally, all the authors read the manuscript several times and have given final approval of the version to be published.
Additional files
Additional file 1:
This is a cleaned comma delimited (*.csv) dataset titled “Patients sociodemographic, clinical, psychosocial, and depressive symptom raw data”. It comprises patients’ sociodemographic, clinical, psychosocial, and depressive symptoms information. All data was anonymized. (CSV 87 kb)
Additional file 2:
STROBE Statement. (DOC 89 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Habtewold, T.D., Alemu, S.M. & Haile, Y.G. Sociodemographic, clinical, and psychosocial factors associated with depression among type 2 diabetic outpatients in Black Lion General Specialized Hospital, Addis Ababa, Ethiopia: a cross-sectional study. BMC Psychiatry 16, 103 (2016). https://doi.org/10.1186/s12888-016-0809-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-016-0809-6