
Abstract
Background
Nonsuicidal self-injury (NSSI) is a serious problem in the adolescent population worldwide. Childhood trauma and bullying have been identified as risk factors for NSSI. We explored the relationships among Childhood trauma, Bullying victimization and the severity of NSSI behaviours, and test the effect of Bullying victimization in mediating the association between Childhood trauma and the NSSI behaviours.
Methods
A total of 123 adolescents were recruited. They were diagnosed with depression or depressive episodes of bipolar disorder and had experienced NSSI in the last year. They were assessed using the Chinese version of the Childhood Trauma Questionnaire (CTQ-C), the Revised Olweus Bullying Victimization Questionnaire (OBVQ-R), and the Adolescent Self-Harm Questionnaire (ASHQ).
Results
Females presented a significantly greater prevalence of sexual abuse and relationship bullying than boys. Individuals in the younger age group (10–14 years) presented a greater incidence of emotional neglect, verbal bullying, relationship bullying, and total bullying, and their NSSI score was also higher than that of those in the older age group (15–19 years). Only children show a greater prevalence of sexual abuse than nononly children. Single-parent families scored higher on emotional abuse, emotional neglect, physical neglect and physical bullying than two-parent families. There was a significant positive correlation between each dimension of childhood trauma and all the dimensions of bullying, between childhood trauma and NSSI, and between bullying and NSSI. Childhood trauma can not only directly affect the severity of NSSI but also indirectly aggravate the severity of NSSI through bullying victimization. The mediating effects of bullying victimization on emotional abuse, physical abuse, emotional neglect and physical neglect were 14%, 21%, 20%, 13% and 20%, respectively.
Conclusion
There was a significant positive correlation between childhood trauma and bullying, between childhood trauma and NSSI, and between bullying and NSSI. Childhood trauma can not only directly affect the severity of NSSI but also indirectly aggravate the severity of NSSI through bullying victimization. Bullying victimization played the partial mediating effects between Childhood trauma and NSSI.
Similar content being viewed by others

Background
NSSI is deliberate damage to the surface of the skin (e.g., cutting, scratching, or burning) without suicidal intent [1]. Furthermore, NSSI has been identified as a risk factor for suicide in several studies [2]. Because young people’s physiological and psychological development is not complete, adolescents who experience higher levels of subjective psychological distress in response to adverse or stressful situations and who are less capable of tolerating distress are at increased risk of engaging in NSSI [3]. Studies have found that NSSI is very common among adolescents, with international lifetime prevalence rates of approximately 17.2% [4]. An epidemiological survey in China also revealed that the self-harm rate among young people in rural areas was 13.5% in 2015–2016 [5].And another study in China showed that its prevalence has been to 15.9% among adolescents in urban areas [6].
NSSI is associated with a variety of psychiatric diagnoses and behavioural concerns. The Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5), has identified a independent code to be applied as a specifier to any nosographic diagnosis.The pathogenesis of NSSI is still unclear. The risk factors leading to NSSI behaviours in adolescents involve many factors, such as society, family and individuals [7].School bullying and childhood trauma seem to be the most common factors experienced by those engaging in NSSI .
Bullying is defined by Olweus [8] as an “intentional, repeated, negative (unpleasant or hurtful) behaviour by one or more persons directed against a person who has difficulty defending himself or herself”. Multiple studies support a positive association between bullying victimization and NSSI [9, 10]. The greater the frequency of bullying is, the greater the risk of NSSI [11]. A large sample meta-analysis [12] showed that the probability of NSSI among bullied adolescents was 2.1 times higher than that of the general population.
Childhood trauma has five forms: physical abuse, emotional abuse, sexual abuse, emotional neglect, and physical neglect. To date, most evidence has shown that emotional abuse and neglect are related to engagement in NSSI [13].The experience of at least one type of childhood trauma was reported by approximately 30% of the general population of Germany in two independent studies [14, 15]. In another study, among participants with a lifetime history of NSSI, approximately 65% reported at least one type of trauma. Approximately 50% of patients reported multiple types of trauma, while this was true for approximately only 12% of the general population [16].
A large body of research [17,18,19,20] has shown that childhood trauma can not only directly affect the occurrence of adolescent NSSI but also indirectly affect NSSI through mediating factors. In turn, several potential mediators of the relationship between trauma and NSSI have been identified, including dissociation, self-esteem, depression, alexithymia, shame, self-criticism, pessimism [21, 22]. However, studies on the mediating role of bullying in the relationship between childhood trauma and NSSI in adolescents are still scarce.
In addition, it is worth noting that individuals with mental disorders have a high prevalence of NSSI. According to one study, 87.6% of adolescents with NSSI are first diagnosed with psychiatric diseases [23]. A meta-analysis revealed a 17.2% prevalence of NSSI in nonclinical samples of community adolescents [4] and 35–80% among clinical adolescents [24]. It is believed that NSSI might be overrepresented in clinical samples such as those adolescents with mental disorders. Therefore, the current study included patients with depression or depressive episodes of bipolar disorder as our research objects. We aimed to explore the relationships among childhood trauma, bullying victimization and the severity of NSSI behaviours, and test the effect of bullying victimization in mediating the association between childhood trauma and the NSSI behaviours.
Methods
Participants
This study was approved by the ethics committee of the Affiliated Kangning Hospital of Ningbo University in accordance with the Declaration of Helsinki, and all participants and/or their guardians provided written informed consent. The ethics trial number is NBKNYY-2020-LC-52.
Participants were recruited from the outpatient or inpatient department of the Affiliated Kangning Hospital of Ningbo University from January 2022 to December 2023. These individuals had been diagnosed as depression or depressive episodes of bipolar disorder according to the International Classification of Diseases 11th Revision( ICD-11) Diagnostic Criteria and had experienced NSSI behaviour in the last year. The inclusion criteria were as follows: (1) aged between 12 and 19 years with NSSI behaviour in the last year; (2) met the diagnostic criteria for NSSI in the DSM-5; (3) were diagnosed with depression or depressive episodes of bipolar disorder by an attending psychiatrist or above; and (4) did not have verbal communication barriers. The exclusion criteria were as follows: (1) had psychotic symptoms or severe mental disorders; (2) had a history of suicide attempts; (3) had serious physical illness; and (4) had a history of substance abuse. A total of 130 subjects were recruited, and 123 participants provided valid questionnaires. 3 participants data were removed due to data coding errors.4 participants Questionnaires were excluded due to obvious logic errors or omissions of more than 15%.
Measurements
All information was collected using the General Demographic Information Questionnaire (GDIQ), Chinese Version of Childhood Trauma Questionnaire (CTQ-C), Revised Olweus Bullying Victimization Questionnaire (OBVQ-R) and Adolescent Self-Harm Questionnaire (ASHQ) conducted by qualified psychologists.
General Demographic Information Questionnaire (GDIQ)
We used open questions in the GDIQ to explore demographic information and the disease type currently diagnosed (depression or depressive episodes of bipolar disorder). The GDIQ is actually a record of an interview between a doctor and a subject. We set up numerous related questions. The data collected included gender, age, academic performance, basic information on the family and current disease type, etc.
Chinese version of the Childhood Trauma Questionnaire (CTQ-C)
The CTQ is a screening tool developed by Bernstein for assessing childhood trauma [25]. The CTQ-C was translated and revised by Zhao Xingfu in China and shows good reliability and validity, meaning it can be used to assess the severity of childhood trauma in Chinese adolescents [26]. The CTQ-C has 28 items and a five-factor superstructure. It contains five subscales, each assessed by five items, including physical abuse, emotional abuse, sexual abuse, physical neglect and emotional neglect. Each participant was asked to answer questions that measured the severity of childhood trauma. They were also asked to rate the extent of the stated questions. Each item is answered on a 5-point scale. “Never” is assigned a score of 1, “occasionally” is assigned a score of 2, “sometimes” is assigned a score of 3, “often” is assigned a score of 4, and “always” is assigned a score of 5. Individuals with a physical abuse score ≥ 10, an emotional abuse score ≥ 13, a sexual abuse score ≥ 8, a physical neglect score ≥ 10, or an emotional neglect score ≥ 15 (i.e., if any of the subscale scores meet the above criteria) can be regarded as having experienced moderate to severe childhood trauma. Higher scores indicate greater childhood trauma. In the present sample, the Cronbach’s α coefficient of internal consistency of this scale was 0.853.
Revised Olweus Bullying Victimization Questionnaire (OBVQ-R)
The Olweus Bully/Victim Questionnaire is one of the most widely used instruments to measure adolescents’ bullying perfusion/victimization [27]. It was revised by Zhang Wenxin et al. in China. The scale has demonstrated good reliability and validity among Chinese adolescents [28]. The scale included two subscales: bullying perpetration and bullying victimization. We used the latter (OBVQ-R) in the current study. The “bullying” mentioned in the remainder of this article refers to “bullying victimization”. Bullying victimization was assessed with six items in total, covering three types: physical bullying (questions 3 and 5), verbal bullying (questions 1 and 6), and relationship bullying (questions 2 and 4).
Participants were asked how often they had experienced different types of bullying in the past year, and the response options included the following: 0 = never in the past year, 1 = only once or twice; 2 = two or three times a month; 3 = approximately once a week; 4 indicates how many times per week 2 = happened a year ago, 3 = a few times within a year, and 4 = a few times a week. If an individual scored ≥ 2 points on any one of the six questions, they were classified as having been victims of bullying. Higher total scores indicate more severe bullying. The Cronbach’s α in the sample for the bullying victimization subscale was 0.807.
Adolescent Self-Harm Questionnaire (ASHQ)
The ASHQ is a self-reported measure developed by Zheng Ying and then revised by Feng Yu [29] for assessing NSSI behaviour in the past year. The ASHQ has good reliability and validity [30]. It assess the prevalence of 18 types of NSSI behaviour. Each participant was asked to answer questions that measured the frequency and extent of harm to the body or NSSI behaviour separately. According to the frequency of NSSI, 0 points are recorded for 0 times, 1 point for 1 time, 2 points for 2 to 4 times, and 3 points for 5 times or more. The extent of harm to the body was divided into 5 levels, namely, none, mild, moderate, severe and extremely severe, which were recorded as 0, 1, 2, 3 and 4 points, respectively. The sum of all the products (frequency multiplied by harm extent) represents the participant’s NSSI score. If the score is not 0, self-injury behaviour is determined, with higher numbers indicating higher levels of NSSI. In the present study, the Cronbach’s α coefficient for the internal consistency of this scale was 0.940.
Statistical analyses
We performed statistical analyses using SPSS version 26.0. The Cronbach’s alpha coefficient was utilized to assess the internal consistency among the items of each scale. Descriptive statistical analysis was performed to determine the prevalence rates of childhood trauma, school bullying and NSSI.
The Kolmogorov-Smirnov test is used to evaluate the normality of the data distribution. In cases of non-normal distribution, non-parametric tests were employed. To examine the differences in childhood trauma, school bullying and NSSI across demographic variables, we used the Mann-Whitney U test for two-group comparisons and the Kruskal-Wallis H test for multi-group comparisons. For the academic performance variable, significance values were adjusted by using Bonferroni correction to account for multiple comparisons.
Pearson correlation was conducted to analyse the relationships among childhood trauma, school bullying and the severity of NSSI. Additionally, Five path analysis models were used to examine the influence of five types of childhood trauma as independent variables on NSSI, with school bullying serving as a mediating variable. These models were constructed using stepwise linear regression and validated through. the bootstrap method, respectively.
Results
Demographics
A total of 130 participants and the effective response rate of the questionnaires was 94.62%. The participants ranged in age from 12 to 19 years, The mean ± standard deviation of age was 15.37 ± 1.72. A detailed description of the participants’ general demographic information can be found in Table 1.
Characteristics of childhood trauma, bullying and NSSI
According to the criteria mentioned above, 93 participants (75.6%) reported having experienced at least one type of childhood trauma. Concerning bullying victimization, 83 participants (67.5%)were classified as victims of bullying. And all 123 participants in this study reported engagement in NSSI in the past year. A detailed description of the participants’ childhood trauma, bullying and NSSI information can be found in Table 2.
Differences in the demographic variables associated with childhood trauma, school bullying and NSSI
Demographic variables such as gender, age, academic performance, and without siblings were taken as independent variables, and all dimensions of childhood trauma, school bullying and NSSI were taken as dependent variables. Differences between each demographic variable were tested by Mann-Whitney U test or Kruskal-Wallis H test.
Overall, Females presented a significantly greater prevalence of emotional abuse, sexual abuse, emotional neglect and childhood trauma than males. Individuals without siblings had a greater prevalence of sexual abuse than individuals having siblings. The single-parent families or left-behind children had greater scores for emotional abuse, physical abuse, sexual abuse and childhood trauma than the both-parents present families. For NSSI, compared to individuals with good and excellent academic performance, individuals with poor and ordinary academic performance had greater scores. For relationship bullying, compared to individuals with good and ordinary academic performance, individuals with poor academic performance had greater scores. Further details on all the demographic variables can be found in the Table 1.
Correlations among childhood trauma, school bullying and NSSI
There was a significant positive correlation between types of childhood trauma and the severity of NSSI (r = 0.494 for emotional abuse, r = 0.421 for physical abuse, and so on). Types of bullying were positively correlated with NSSI. There was also a significant positive correlation between each dimension of childhood trauma and all the dimensions of bullying. Further details can be found in Table 3.
Mediating effects of school bullying
The mediating role of bullying in the relationship between emotional abuse and NSSI
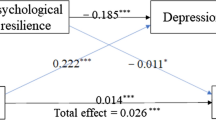
In the first step (Model 1), emotional abuse had a significant influence on NSSI (B = 3.328, p < 0.001), which means that there was a total effect. In the second step (Model 2), emotional abuse had a significant influence on bullying (B = 0.413, p < 0.01). In Model 3, emotional abuse and bullying both had significant effects on NSSI (B = 2.852, p < 0.001; B = 1.225, p < 0.05). Therefore, the effect of emotional abuse on NSSI was partially mediated by bullying (for details, see Table 4; Fig. 1.)
The bootstrap method was used to test the mediating role of bullying in the model. The indirect effect was 0.476, and the 95% CI [0.032–1.086] did not contain 0. This indicates an indirect effect. Therefore, bullying plays a significant mediating role in the model. The direct effect value was 2.852, and the 95% CI [1.708, 3.997] did not contain 0, which indicates a direct effect. According to the effect proportion calculation results, the effect proportion of bullying between emotional abuse and NSSI was 14%. (for details see Table 5).
The mediating role of bullying in the relationship between physical abuse and NSSI, between sexual abuse and NSSI, between emotional neglect and NSSI, between physical neglect and NSSI.
As shown in Tables 4 and 5; Fig. 1, the mediating role of school bullying in the relationship between physical abuse and NSSI is clear, and the effect of physical abuse on NSSI was partially mediated by bullying. In the same way, the effect of sexual abuse, emotional neglect and physical neglect on NSSI was also partially mediated by bullying. The effect proportion of bullying victimization on physical abuse, sexual abuse, emotional neglect and physical neglect were 21%, 20%, 13% and 20%, respectively.(for details see Tables 4 and 5; Fig. 1).

Path analysis model of various dimensions of childhood trauma related to NSSI with campus bullying as a mediating factor. B1: Analysis of the mediating effect of bullying on the relationship between emotional abuse and NSSI: in Model 3, the mediating effect of bullying on NSSI, B1 = 1.225*. B2: Analysis of the mediating effect of bullying on the relationship between physical abuse and NSSs, B2 = 1.372*. B3: Analysis of the mediating effect of bullying on the relationship between sexual abuse and NSS, B3 = 3.229**. B4: Analysis of the mediating effect of bullying on the relationship between emotional neglect and NSS, B4 = 3.239**. B5: Analysis of the mediating effect of bullying on the relationship between physical neglect and NSS, B5 = 3.257***. *p < 0.05; **p < 0.01; ***p < 0.001
Discussion
Differences in the demographic variables associated with NSSI, childhood trauma and school bullying victimization
According to literature reports, among sociodemographic factors, gender is one of the most powerful predictors of NSSI [7, 31]. Females are more likely to develop NSSI than males are, and this difference is greater in the clinical population than in the general population [24, 32]. The results of our current study are basically consistent with the literature reports. Our study focused on adolescents with depression or depressive episodes of bipolar disorder; 77.2% of NSSI patients were female, which was significantly more than male adolescents. However, it is worth noting that the test for differences in NSSI scores according to gender showed no difference between females and males in our study. The reasons may be as follows: the prevalence of NSSI was greater in female adolescents with depression or depressive episodes of bipolar disorder than in male adolescents, but there was no difference in the severity of NSSI. On the other hand, our sample size may be small, and the results of our study did not reveal a difference in NSSI severity between males and females.
A total of 83.7% of the participants in our study were diagnosed with depression, which was much higher than the percentage of participants diagnosed with bipolar depressive episodes. This finding corroborates the findings of past studies in which depression was the main diagnostic factor in clinical NSSI patients [33]. Our study revealed no significant difference in the severity of NSSI between adolescents with depression and those with depressive episodes of bipolar disorder. The reasons may be that emotional regulation is one of the main purposes of NSSI behaviour [34], and patients with depression and bipolar disorder are characterized by significant emotional dysregulation.
In addition, for the differences of childhood trauma in the demographic variables such as gender, without siblings, single-parents and so on, our findings are basically consistent with previous literature reports [35,36,37,38]. But, in terms of bullying, there was little difference in other demographic variables except academic achievement in current study.And this is different from the previous literature reports [39].Maybe it has something to do with our insufficiently large sample size.
Associations between childhood trauma, bullying victimization and NSSI
Associations between childhood trauma and NSSI
Previous research has shown that all types of childhood trauma lead to greater vulnerability to NSSI [16, 40]. Adolescents who experience adverse childhood experiences are at increased risk of developing cognitive distortions that can lead to the endorsement of NSSI behaviours. [17, 41, 42].The results concerning the correlation between childhood trauma and NSSI in the present study are basically consistent with those studies mentioned above. For adolescents with depression or depressive episodes of bipolar disorder, there was also a significant positive correlation between all dimensions of childhood trauma and NSSI; that is, the more severe the childhood trauma was, the more severe the NSSI behaviour. This is in line with theories such as the Developmental Psychopathology Network [43] or the Biopsychosocial Model of Marsha Linehan [44], both of which link adverse childhood experiences with the development of dysfunctional emotion regulation and thus the development of dysfunctional coping skills such as NSSI. Individuals reduce their emotional distress and decrease their memories of abuse through self-injurious behaviour [45].
Association between bullying experiences and NSSI
Previous studies have shown that bullying is a risk factor for NSSI [7], and our study further confirms this finding. The relevant analysis results of our study showed that bullying and all of its dimensions, including physical bullying, relational bullying, and verbal bullying, were significantly positively correlated with NSSI in adolescents with depression or depressive episodes of bipolar disorder.
The reasons are as follows. First, bullying can be a stressor. Bullied individuals are likely to be at risk for poor adjustment compared to noninvolved adolescents. The difficulty of adapting and the decline in quality of life caused by stress can lead to the accumulation of negative emotions [21], which leads to self-injury behaviour for their relief. Second, adolescents who suffer from school bullying may also use self-harm as a form of recourse or self-punishment [12]. In this way, they try to obtain interpersonal support and convey emotional distress [46], and then negative emotions can be effectively alleviated.
Association between childhood trauma and bullying experiences
In our study, there was a significant positive correlation between childhood trauma and school bullying. This result corresponds well to findings from Canada that victims of child sexual abuse were more likely to experience bullying, and females who had experienced sexual abuse were cyberbullied at twice the rate of those who had not [47].All of these findings can be explained by parent–child attachment theory. That is, adolescents who have suffered childhood trauma are more likely to develop insecure attachments, and they are more likely to become involved in bullying because they do not have appropriate coping styles when facing new situations [48, 49].
Mediating effects of bullying victimization on the relationship between childhood trauma and NSSI
As we mentioned in the previous section of this article, some research has shown bullying to be a risk factor for NSSI [7], but bullying is also known to occur as a consequence of childhood trauma [48, 49]. According to previous studies, some factors, such as dissociation, self-esteem, depression, or alexithymia, might mediate the relationship between the experience of childhood trauma and engaging in NSSI [21, 22]. These factors were not assessed in the current study. In our study, we focused on the mediating role of school bullying in the relationship between childhood trauma and NSSI. We found that childhood trauma can impact NSSI not only directly but also through the mediating role of bullying in the adolescent population with depression or depressive episodes of bipolar disorder. Bullying partially mediates the relationships between various types of childhood trauma (including emotional abuse, physical abuse, sexual abuse, emotional neglect and physical neglect) and NSSI behaviour.
According to the above our findings, we analyze the reasons as follows, childhood trauma, especially repeated trauma, can disrupt children’s emotional regulation and acquisition of interpersonal skills [50]. Bullying as a negative experience can also lead to deficits in emotion regulation [9]. These deficits may result from individuals’ own psychological experiences but may also result from neurophysiological dysregulation caused by trauma [51, 52], which can then in turn lead to engaging in maladaptive coping strategies, such as NSSI. The fact that NSSI is most often engaged in as a dysfunctional emotion regulation strategy might explain why childhood trauma and school bullying are both associated with NSSI, as they can all affect a person’s ability to regulate emotions. Adolescents with childhood trauma are more likely to exhibit NSSI behaviours after experiencing adverse events such as school bullying.
On the one hand, adolescents who experience childhood trauma can directly adopt NSSI as a maladaptive adjustment strategy. On the other hand, due to emotional dysregulation and a decrease in interpersonal skills, the risk of suffering from bullying increases. In turn, bullying leads individuals to adopt NSSI to regulate their emotions. Namely, bullying played mediating role in the relationship between childhood trauma and NSSI. This is consistent with the principle elaborated in the empirical avoidance model proposed by Chapman [53]. That is, stimuli cause individuals to produce certain emotional responses. Under the interaction of many other factors, individuals choose to avoid through NSSI, which temporarily alleviates their negative emotional experiences. In turn, the relief of this negative emotion further strengthens NSSI and promotes the maintenance of NSSI [54].
Childhood and adolescence are important periods in human development during which harmful experiences can significantly influence the course of life in the long term. It is the common responsibility of the whole society to create a healthy and good growth environment for young people. In particular, adolescents with depression and bipolar disorder need more attention. The current research explored the correlations among childhood trauma, school bullying victimization and NSSI and the mediating effect of bullying victimization on the relationship between childhood trauma and NSSI in this depressed population, which will be helpful for families, schools and society to pay more attention to childhood trauma and school bullying. The results of this study also have implications for preventative and therapeutic interventions for NSSI.
Conclusion
There was a significant positive correlation between childhood trauma and bullying, between childhood trauma and NSSI, and between bullying and NSSI. Childhood trauma can not only directly affect the severity of NSSI but also indirectly aggravate the severity of NSSI through bullying victimization. Bullying victimization played the partial mediating role in the relationship between Childhood trauma and NSSI.
Limitations
This study has some limitations that should be considered when interpreting the findings. First, participants were asked to report on only NSSI that occurred within the past year. The lifetime data are unknown, which may have impacted the results. Second, as this was a retrospective and self-reported cross-sectional study, the possibility of memory bias regarding NSSI, childhood trauma and bullying must be considered when interpreting the results. Self-reported data may also be subject to bias. Third, in this study, we used the bullied subscale, and only bullying victimization was studied. Future studies should be conducted to assess bullying perpetration. Furthermore, the sample size of this study was small, which may have influenced the results. We will expand the sample size in future studies to further verify the results.
Data availability
All data generated or analysed during this study are included in this published article.
References
Zetterqvist M. The DSM-5 diagnosis of nonsuicidal self-injury disorder: a review of the empirical literature[J]. Child Adolesc Psychiatry Mental Health. 2015;9(1):1–13.
Baer MM, LaCroix JM, Browne JC, et al. Non-suicidal self-injury elevates suicide risk among United States military personnel with lifetime attempted suicide[J]. Archives Suicide Res. 2018;22(3):453–64.
Anestis M, Knorr A, Tull M et al. The importance of high distress tolerance in the relationship between non-suicidal self-injury and suicide potential. Life-Threatening Behav, 43(6), 663–75.
Swannell SV, Martin GE, Page A, et al. Prevalence of nonsuicidal self-injury in nonclinical samples: systematic review, meta-analysis and meta-regression. Suicide Life-Threatening Behav. 2014;44(3):273–303.
Chen Y, Zhang M, Guo H, et al. Associations of neglect and physical abuse with non-suicidal self-injury behaviors among adolescents in rural China. Chin J Sch Health. 2019;40(7):984–90.
Chaiquan LIJ, Zhang R, Lv, et al. Self-harm and its association with bullying victimization among junior high school students in Beijing. Chin J Public Health. 2020;36(6):884–8.
Yujing WX, Li,Chee H et al. Ng,Risk factors for non-suicidal self-injury (NSSI) in adolescents: a meta-analysis. eClinicalMedicine 2022,46: 101350.Published online 21 March 2022 https://doi.org/10.1016/j.eclinm.2022.101350
Olweus D, Limber SP. Bullying in school: evaluation and dissemination of the Olweus bullying prevention program. Am J Orthopsychiatry. 2010;80(1):124–34.
Serafini G, Aguglia A, Amerio A, et al. The relationship between bullying victimization and perpetration and non-suicidal self-injury: a systematic review[J]. Child Psychiatry Hum Dev. 2023;54(1):154–75.
Claes L, Luyckx K, Baetens I, et al. Bullying and victimization, depressive mood, and nonsuicidal self-injury in adolescents: the moderating role of parental support. J Child Family Stud. 2015;24(11):3363–71.
Vergara GA, Stewart JG, Cosby EA, et al. Non-suicidal self-injury and suicide in depressed adolescents:impact of peer victimization and bullying. J Affect Disord. 2019;245(1):744–49.
Van Geel M, Goemans A, Vedder P. A meta-analysis on the relation between peer victimization and adolescent nonsuicidal self-injury[J]. Psychiatry Res. 2015;230(2):364–8.
Lang CM, Sharma-Patel K. The relation between childhood maltreatment and self-injury: a review of the literature on conceptualization and intervention. Trauma Violence Abuse. 2011;12(1):23–37.
Iffland B, Brahler E, Neuner F, et al. Frequency of child maltreatment in a representative sample of the German population. BMC Public Health. 2013;13(1):1–12.
Witt A, Brown RC, Plener PL, et al. Child maltreatment in Germany: prevalence rates in the general population. Child Adolesc Psychiatry Mental Health. 2017;11(1):1–9.
Brown RC, Heines S, Witt A, et al. The impact of child maltreatment on non-suicidal self-injury: data from a representative sample of the general population[J]. BMC Psychiatry. 2018;18(1):1–8.
Thomassin K, Shaffer A, Madden A, et al. Specificity of childhood maltreatment and emotion deficit in nonsuicidal self-injury in an inpatient sample of youth. Psychiatry Res. 2016;244:103–8.
Maniglio R. The role of child sexual abuse in the etiology of suicide and non-suicidal self-injury. Acta Psychiatr Scand. 2011;124(1):30–41.
Glassman LH, Weierich MR, Hooley JM, Deliberto TL, Nock MK. Child maltreatment, non-suicidal self-injury, and the mediating role of selfcriticism. Behav Res Ther. 2007;45(10):2483–90.
Xueqian XU, Zhenyu HU. A review of psychosocial mediating factors between childhood trauma and non-suicidal self-injury in adolescents. Chin Mental Health J 2022,36(12): 1079–83.
Ford JD, Gómez JM. The relationship of psychological trauma and dissociative and posttraumatic stress disorders to nonsuicidal self-injury and suicidality: a review. J Trauma Dissociation 2015,16(3):232–71.
De Berardis D, Fornaro M, Orsolini L, et al. Alexithymia and suicide risk in psychiatric disorders: a mini-review. Front Psychiatry. 2017;8:148.
Glenn CR, Klonsky ED. Nonsuicidal self-injury disorder: an empirical investigation in adolescent psychiatric patients. J Clin Child Adolesc Psychol. 2013;42(4):496–507.
Yongjie YS. Zhou, Non-suicidal self-injury function: prevalence in adolescents with depression and its associations with non-suicidal self-injury severity, duration and suicide.Frontiers in Psychiatry,2023,14,1188327.
Bernstein DP. Stein JA,Newcomb MD,El al.Development and validation of a brief screening version of the Childhood Trauma Questionnaire. Child Abuse Negl 2003,27(2):169–90.
Xingfu Zhao,Yalin Zhang,Longfei Li,et al.Evaluation on reliability and validity of Chinese version of childhood trauma questionnaire[J]. Chin J Tissue Eng Res 2005,9(16):209–11.
Green JG, Felix ED, Sharkey JD, et al. Identifying bully victims: definitional versus behavioral approaches. Psychol Assess. 2013;25(2):651–57.
Zhang W. JianFen Wu,Jones Kevin. Revision of the Chinese version of Olweus child bullying questionnaire[J]. Psychol Dev Educ. 1999;38(2):8–12.
Yu, Feng. Guang-rong Jiang.The Relation of Adolecents Self-Harm Behaviors, Individual Emotion Characteristics and Family Environment Factors. Collection of abstracts from the 12th National Psychological Academic Conference(2009):632 – 33.
Quan L, Yu L, Fei X et al. Sensitivity of emotional reactivity in non-suicidal self-injury. Chin J Clin Psychol 2020,28(6):1094–101.
Jeong JY, Kim DH. Gender differences in the prevalence of and factors related to non-suicidal self-injury among middle and high school students in South Korea[J]. Int J Environ Res Public Health. 2021;18(11):5965.
Brown RC, Plener PL. Non-suicidal self-injury in adolescence[J]. Curr Psychiatry Rep,2017,19: 1–8.
Lijun KR, Li H, Liu, et al. Nonsuicidal self-injury in undergraduate students with major depressive disorder: the role of psychosocial factors. J Affect Disord. 2021;290:102–8.
Nock MK. Why do people hurt themselves? New insights into the nature and functions of self-injury[J]. Curr Dir Psychol Sci. 2009;18(2):78–83.
Zhang Y, Li J. Xueqin Yin.Relative weights analysis on the impacts of childhood maltreatment forms on adolescent anxiety and depression.Chinese. J Sch Health. 2022;43(3):407–10.
Negele A, Kaufhold J, Kallenbach L et al. Childhood Trauma and Its Relation to Chronic Depression in Adulthood[J]. Depression Research and Treatment, 2015, 2015: 650804–650804.
Mathews B, Bromfield L, Walsh K, et al. Reports of child sexual abuse of boys and girls: longitudinal trends over a 20-year period in Victoria, Australia[J]. Volume 66. Child Abuse & Neglect; 2017. pp. 9–22.
Codispoti M, Surcinelli P, Baldaro B. Watching emotional movies: affective reactions and gender differences. Int J Psychophysiol. 2008;69(2):90–5.
Duntley JD, Buss DM. Evolutionary psychology is a metatheory for Psychology[J]. Psychol Inq. 2008;19(1):30–4.
Can Shao XW, Ma Q, et al. Analysis of risk factors of non-suicidal self-harm behavior in adolescents with depression[J]. Annals Palliat Med. 2021;10(9):9607–13.
Vaughn MG, Salas-Wright C, Underwood S, et al. Subtypes on non-suicidal self-injury based on childhood adversity. Psychiatr Q. 2015;86(1):137–51.
Kaess M, Parzer P, Mattern M, Plener PL, et al. Adverse childhood experiences and their impact on frequency,severity,and the individual function of nonsuicidal self-injury in youth. Psychiatry Res. 2013;206(2–3):265–72.
Yates TM. The developmental psychopathology of self-injurious behavior:compensatory regulation in posttraumatic adaptation. Clin Psychol Rev. 2004;24(1):35–74.
Linehan MM. Dialectical behavior therapy for treatment of borderline personality disorder: implications for the treatment of substance abuse.NIDA Research Monograph. 1993;137:201–16.
Huiying Liu W, Wang J, Yang et al. The effects of alexithymia, experiential avoidance, and childhood sexual abuse on non-suicidal self-injury and suicidal ideation among Chinese college students with a history of childhood sexual abuse[J]. J Affect Disorders 2021,282: 272–79.
Muehlenkamp J, Brausch A, Quigley K, et al. Interpersonal features and functions of nonsuicidal self-injury[J]. Suicide life-threatening Behav. 2013;43(1):67–80.
Hébert M, Cénat JM, Blais M, et al. Child sexual abuse, bullying, cyberbullying, and mental health problems among high schools students: a moderated mediated model[J]. Depress Anxiety. 2016;33(7):623–29.
Riggs SA, Kaminski P. Childhood emotional abuse, adult attachment, and depression as predictors of relational adjustment and psychological aggression[J]. J Aggress Maltreatment Trauma. 2010;19(1):75–104.
Li W, He X, Wang R et al. Effect of adverse childhood experiences on university studengts’interpersonal relationship difficulties:The mediation effect of adult attachment and mobile phone addiction.China Journal of Health Psychology.2022,30(12):1852-58.
Dvir Y, Ford JD, Hill M, et al. Childhood maltreatment, emotional dysregulation, and psychiatric comorbidities[J]. Harv Rev Psychiatry. 2014;22(3):149–61.
Connor DF, Doerfler LA. Characteristics of children with juvenile bipolar disorder or disruptive behavior disorders and negative mood: can they be distinguished in the clinical setting?[J]. Ann Clin Psychiatry. 2012;24(4):261–70.
De Bellis MD. Developmental traumatology: the psychobiological development of maltreated children and its implications for research, treatment, and policy[J]. Dev Psychopathol. 2001;13(3):539–64.
Chapman AL, Gratz KL, Brown MZ. Solving the puzzle of deliberate self-harm: the experiential avoidance model[J]. Behav Res Ther. 2006;44(3):371–94.
Huifang YIN, Haolin XU,Zhaorui LIU, et al. A review of theoretical models of non-suicidal self-injury (NSSI) in adolescents[J]. Chin Mental Health J. 2022;36(8):707–13.
Funding
This research was supported by the Zhejiang Medical and Health Science and Technology Planning Program (NO. 2021452728) and the Ningbo Medical and Health Brand Discipline (NO. PPXK 2018-08).
Author information
Authors and Affiliations
Contributions
Each author substantially contributed to the paper.ZH and HL carried out the methodological search on the research topic and supervised the writing of the manuscript; YL performed data analysis, conceived and wrote the first draft of the paper; XQX contributed with data analysis and draft preparation; XH and QH participated in all the questionnaire survey , data collection; LL and XHX contributed to the statistics of all the data in this study; WC and WS provided help in reviewing the literature.All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethical approval and consent to participate
This study was approved by the ethics committee of Affiliated Kangning Hospital of Ningbo University in accordance with the Declaration of Helsinki. The ethics trial no. is NBKNYY-2020-LC-52. Informed consent was obtained from all subjects and/or their legal guardian(s).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Liu, Y., Xu, X., Huang, X. et al. The mediating effects of school bullying victimization in the relationship between childhood trauma and NSSI among adolescents with mood disorders. BMC Pediatr 24, 524 (2024). https://doi.org/10.1186/s12887-024-04986-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-024-04986-7