
Abstract
Background and aim
The evidence about the acceptability and effectiveness of innovative paediatric models of care for Type 1 diabetes is limited. To address this gap, we synthesised literature on implemented models of care, model components, outcomes, and determinants of implementation and sustainability.
Methods
A systematic review was conducted and reported in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Database searches of Medline, CINAHL, EMBASE and Scopus were conducted. Empirical studies focused on Type 1 diabetes paediatric models of care, published from 2010 to 2022 in English were included.
Results
Nineteen extant studies reported on models and their associations with health and psychosocial outcomes, patient engagement with healthcare, and healthcare costs. Thirteen studies described multidisciplinary teamwork, education and capacity building that supported self-care. Four studies involved shared decision making between providers and patients, and two discussed outreach support where technology was an enabler. Fourteen studies reported improvements in health outcomes (e.g. glycaemic control), mostly for models that included multidisciplinary teams, education, and capacity building (11 studies), outreach support or shared care (3 studies). Four studies reported improvements in quality of life, three reported increased satisfaction for patients and carers and, and one reported improved communication. Four of five studies describing shared care and decision-making reported improvements in quality of life, support and motivation. Outreach models reported no negative outcomes, however, accessing some models was limited by technological and cost barriers. Eight studies reported on model sustainability, but only half reported implementation determinants; none reported applying a theoretical framework to guide their research.
Conclusion
Some health and psychosocial benefits were associated with newer models. To address knowledge gaps about implementation determinants and model sustainability, longitudinal studies are needed to inform future adoption of innovative models of care for children with Type 1 diabetes.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
Type 1 diabetes (T1D) is typically diagnosed in childhood. In 2021 there were approximately 8.4 million individuals worldwide with T1D and of these, 1.5 million (18%) were younger than 20 years [1]. In Australia, T1D affects around 140,000 young people [2]. Despite advances in care, children and adolescents who develop T1D have a reduced life expectancy by around 12–16 years compared with those without T1D [3, 4]. Increased morbidity and mortality is attributed to an ongoing gap between the recommended glycaemic control levels and the levels achieved in practice, and this poor glycaemic management can lead to cardiovascular disease [5], nephropathy and mental health disorders [6]. Increased attention on the models used to deliver care is needed to better understand how and whether these are associated with improved outcomes, e.g., optimising the maintenance of glycaemic levels among children with T1D.
Paediatric care for T1D is complex as there are a range of developmental stages to consider. For younger children (< 14 years) care tends to be family orientated, as they lack the maturity to self-manage their care delivery and planning [5], whereas, adolescents are encouraged to take on more responsibility for self-management as they approach adulthood [7]. Successful outcomes require a psychosocial approach with education and support from clinical teams for the child and their family, to empower and motivate them to effectively manage the treatment 24-h a day, seven days a week, and through life events. Commonly, models of care for paediatric T1D involve routine outpatient clinic visits every 3–4 months with a multidisciplinary team (MDT) [8, 9]. Regular consultations are usually undertaken face-to-face with the child and family, with between visit communication initiated by families/carers as needed [10]. MDT care typically includes specialist doctors and nurses, diabetes educators, dieticians and psychologists, and has been proposed as an effective way of providing care to increase safe levels of glycaemia [11]. A model of care involving an MDT approach is one where professionals bring their skills and expertise from a range of disciplines for a combined team effort that responds to the individual child and family needs. Team members typically collaborate to discuss the patient and family and develop shared care plans. Although several implementation barriers have been identified to adoption of such models, including time constraints, inaccessibility, cost and conflicting recommendations from different providers, this approach has the potential to strengthen clinical care and improve health outcomes, especially when it is consumer focused and involves shared-decision making between the provider and patient [12]. Although the International Society for Pediatric and Adolescent Diabetes (ISPAD) guidelines provide evidence based recommendations for care [13], it is not known whether these are being implemented in practice. Additionally, there have been no systematic reviews to describe current models of care, nor a synthesis of current evidence for the effectiveness of models of care for T1D. It is unclear how the effectiveness of models of care has been conceptualised and, in examining these models, what types of study designs have been used and which outcomes have been measured.
Our group recently conducted a systematic review on models of care for individuals with T1D transitioning from paediatric to adult health care [14]. We identified a gap in the evidence about the implementation determinants and the sustainability of models of care, with few studies applying longitudinal designs to measure long-term outcomes. Given this gap in the transition context, a synthesis of evidence about the implementation determinants and sustainability of non-transitional models of care for T1D is needed.
This review aims, first, to map the scope of implemented models of care for children living with T1D, to describe the model components, how and to what extent these contribute to improved health, psychosocial and health services outcomes. Second, we aim to synthesise evidence about factors associated with implementation and sustainability of effective models of care to inform future adoption of successful models at scale and in different contexts.
Methods
Review protocol
The studies in this review were identified in the results of a concurrent review that reports on models of care for transitioning young adults living with T1D [14]. As such, the methodology sections are similar. The systematic review was guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Systematic Reviews (PRISMA) guidelines [15] and follows a registered protocol (CRD42021262727) which is available here: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=262727.
Search methods
The review team met with a medical librarian to design the search strategy. Four databases were searched: Scopus, Medline, CINAHL, and EMBASE on 6th June 2021 and updated on 11th November 2022. An example of the search strategy is provided in Supplemental File 1. Search limits were applied to include to publications in English, published from January 2010 to November 2022. Snowballing techniques identified other relevant publications in the reference list of included studies and these were screened according to the inclusion and exclusion criteria.
Inclusion and exclusion criteria
We included peer-reviewed articles and reviews describing the intervention of a person centred model of care implemented in high income countries [16], and patients under the age of 18 years diagnosed with T1D. Studies that described telehealth, in addition to describing other model components, that was facilitated and delivered by MDT approaches or innovative diabetes education were included. Studies had to report on health related and/or psychosocial outcomes, and/or experiences from the perspective of the health provider, health consumer, and/or caregiver.
Studies that were published prior to 2010, in a language other than English, were conducted in a low- or middle-income country, focused on transitional care of T1D, Type 2 diabetes or maternal health interventions or clinical interventions, e.g., clinical trials involving drugs or specific equipment were excluded. Other reasons for exclusion were commentaries, publications of opinion or perspective, letters to the editor, editorials, and conference abstracts. We also excluded studies that discussed routine consultations through telehealth without a description of a broader model of care.
Study selection
The reference details for articles returned from search results were downloaded to a folder and duplicates were removed and exported into Rayyan, an electronic literature screening program [17]. Ten percent were screened independently by IM and MS, and a separate sample of 10% were screened by YZ and IM. For the updated searches, all title/abstract and full text screening was undertaken independently by two reviewers (AC, GD). Any disagreements among reviewers were resolved by discussion with the whole review team. The full text of selected studies was then examined. Studies were excluded if they failed to meet the inclusion criteria on full-text screening.
Data extraction and synthesis
A custom data extraction workbook was created in Microsoft Excel. The workbook underwent pilot testing on five articles, and adjustments were made as necessary to accommodate the different types of data reported in the articles. Four reviewers (AC, MS, NH, RL) systematically extracted the data, and any discrepancies among the reviewers were resolved through discussion. The relevant information extracted included: specific publication details such as authors, year published, country; design, methods and setting; patient details such as age, gender, race/ethnicity, socio- economic status, mean duration of diabetes, and insurance status; description of the model of care, their components, staffing, resources, and setting; a description of usual care, outcomes related to health, psychosocial aspects, or health service use, the utilisation of an implementation framework, and the determinants, enablers, barriers, and adoption of the model into practice (Table 2). Common themes, features specific to the model, and categories of outcomes were extracted by the research team.
Results
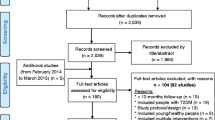
The search for primary studies yielded 1951 results (CINAHL: 727, EMBASE: 572, Medline: 446, Scopus: 205; identified from other sources: 1). Among these, 361 duplications were removed. After screening 1590 title/abstracts, 1313 papers were excluded as they did not meet the inclusion criteria. Two hundred and seventy studies underwent full text review and a further 258 papers were excluded. Nineteen primary studies were included for data extraction and synthesis, as shown in Fig. 1. Interrater reliability scores (Cohen’s kappa) [18] were all above k = 0.6, which is considered a “good” inter-rater reliability score.

PRISMA flow chart describing the study selection process
Quality assessment
Methodological quality was appraised using the Mixed Methods Appraisal Tool (MMAT) [19]. To ensure consistency, two investigators (AC and RL) appraised 10% of the articles independently. Twelve of the 19 studies reported a quantitative non-randomised design and included a representative sample and complete outcome data [9, 11, 20,21,22,23,24,25,26,27,28,29], however, two of these studies did not account for confounders [9, 29]. There were six randomised controlled trials that reported appropriate randomisation and complete outcome data [8, 10, 30,31,32,33], however, outcome assessors were not blinded, potentially introducing a bias. One study reported a qualitative design that adopted an appropriate approach, adequate data collection and substantiated interpretation [34]. We did not exclude any studies based on quality assessment. See Supplemental File 2 for further detail.
Scope of models
Most studies (13/19, 68%) were from the USA [8,9,10, 20,21,22, 24, 26, 27, 30, 31, 33, 34]. The remaining studies were from Australia (4/19, 22%) [11, 23, 25, 28], Canada (1/19, 5%) [29], and Denmark (1/19, 5%) [32], (Table 1). Most studies were conducted using quantitative methodologies (12/19, 63%) [9, 11, 20,21,22,23,24,25,26,27,28,29], a third used randomised controlled trial designs (6/19, 32%) [8, 10, 30,31,32,33], and there was one qualitative study (1/19, 5%) [34]. The models of care described in the 19 included papers were comprised of several components such as MDT care, shared decision making, capacity building and education for self-care, remote monitoring, and outreach support (Table 1).
Model components
Although there was often overlap among the components (e.g., MDT, shared care and outreach), common components and approaches to care provision were identified as demonstrated in Fig. 2. These included MDT care, shared decision making, capacity building and education to support self-care, outreach support and mentoring and integrated care where technology such as a paging system was used as an enabler.

Components of T1D paediatric models of care
Multidisciplinary team care, education and capacity building for self care
MDT care was a central model component across 13 studies (68%). Teams provided T1D care in different contexts including in hospital settings, outpatient clinics, outreach services or via telemedicine. MDTs were comprised of medical staff such as paediatric emergency medicine physicians, paediatric endocrinologists, primary healthcare providers as well as nurse practitioners, mental health nurses, dieticians, pharmacists, and patients. MDT model components and the work of MDTs often included education for patients and providers [20, 27]; shared medical appointments that involved the child living with T1D, their caregivers and multiple healthcare providers [9]; capacity building for patient self-care and education [8, 24, 26, 30]; education and remote monitoring in outreach and rural settings [10, 11]; and support between clinic visits from diabetes nurse educators for patients residing in rural settings [28]. The structure and work of the MDT models was variable with no model being described in the same way. Examples include MDTs implementing and embedding evidence-based treatment guidelines into their practice for patients with diabetic ketoacidosis (DKA) [20]; a Spanish speaking MDT involved in shared medical appointments (SMA) for Latino children with T1D [27], and an MDT model where individuals and caregivers participated in SMAs involving education and clinical care [9]. Another MDT was involved in weekly review of outpatient data uploaded from an activity monitor, insulin pump and glucose sensor [10].
Capacity building for self-care included family education programs comprised of education initiatives offered to patients and families in diabetes clinics. A key component was the exploration and identification of self-management barriers that subsequently lead to solutions such as the design and delivery of tailored self-management education resources [8, 30, 33], and coping skills programs [34]. These included tailored delivery of resources to help families improve diabetes management [8], training sessions on cognitive behavioural skills and relapse prevention to improve maintenance of safe glycaemic levels [30], and training in insulin pump usage and the basal bolus regimen [24]. Others described accessible, co-ordinated, family-centred care [26], individualised treatment plans for patients to improve glycaemic maintenance and quality of life, and group support to increase knowledge about T1D, goal setting, and glucose pattern recognition [21]. Additionally, identification of child and family psychosocial issues enabled the development of a stepped care model where the intensity of clinical intervention was matched to each case as needed [29]. Concerns were discussed and addressed among the individuals living with T1D, their caregiver and the care team [29].
Shared decision making
A shared decision making model was described by Hatherly et al. (2011) [23], where paediatric endocrinologists from large metropolitan hospitals provide outreach and travel to rural and regional sites to integrate care with a primary health care provider and patients, to empower patient/family relationships with specialist physicians, nurses and dieticians, providing care that includes self-reflection and the development of life skills [32]. Integrated care with technology as an enabler included real-time mobile health technology that shares patient blood glucose data with their parents, and clinic-based healthcare providers facilitated shared decision making [31].
Outreach support
Outreach support often involved digital and remote monitoring and was described in three studies (16%) [22, 25, 28]. Outreach rural services included a visiting medical specialist who attended routine medical appointments at three-month intervals and follow up by allied health teams or diabetes nurse educators between appointments [28]. In a study in regional and remote Western Australia, all patients are offered 24-h, 7 days-a-week telephone support with an in-hospital or outreach team, and four visits from a metropolitan-based outreach team per year [25]. Triaging in remote settings was undertaken using a paging system that families could access [22].
Model outcomes and effectiveness
Many different outcomes were measured and reported in the 19 included studies. Outcomes could be grouped under the broad categories of health, psychosocial, satisfaction, cost, hospital admissions, regimen adherence and other (Table 2).
Table 3 presents the evidence for effectiveness based on the outcomes, stratified by model components.
Glycaemic control was the most frequently reported health outcome. Five studies (26%), involving MDT, education and capacity building for self-care, reported significant improvements in glycaemic control associated with the model of care [8, 11, 27, 30, 33]. Three studies (16%) reported no change in HbA1c levels indicating that the model of care was comparable to routine care [9, 10, 21]. Two studies (11%) reported a significant reduction in DKA and hospital admissions [20, 24], another two studies (11%) reported comparable insulin regimen adherence compared with usual care [30, 33], one study (5%) showed an increase in insulin pump usage for Latino patients [27], and one study (5%) reported comparable insulin pump usage compared to usual care [9] (Table 3).
For studies describing shared care and decision making, the evidence for health benefits was mixed. Two studies (11%) reported no change in HbA1c levels (perceived benefit) [23, 32], one study (5%) reported short term benefits at three months but this effect was not replicated at six months [31]. One study (5%) reported an increase in HbA1c across 18 months compared to baseline [29]. Compared with usual care, four studies (21%) describing outreach support and mentoring, reported comparable health outcomes including similar levels of HbA1c [25, 35], and episodes of severe hypoglycaemia [25, 28], or DKA [22, 25] (Table 3).
Quality of life and psychosocial outcomes are important measures of the effectiveness of care; however, benefits were not consistently reported. For MDT, education and capacity building for self-care models three studies (16%) reported improved quality of life [11, 21, 30], one (5%) reported better communication [21], and three (16%) reported improved satisfaction for caregivers [30] and patients [27, 34]. Three studies (16%) reported improved quality of life [29], greater support from a diabetes educator [23], and improved motivation [32]. For outreach support, one study (5%) reported an increased number of rural clinic visits [28].
Two studies (11%) compared healthcare costs for MDT, education and capacity building for self-care models with usual care [9, 20], with one reporting a decrease in ED charges because of decreased presentations of DKA [20]. A further study showed a reduction in the negative impact of T1D on factors such as school attendance and finances for families involved in medical care in their homes compared to usual care [26].
Implementation determinants and model sustainability
None of the 19 studies mentioned implementation frameworks or theories to guide their adoption of multidisciplinary models of care. Twelve studies (63%) discussed implementation enablers, and 11 (58%) reported barriers to implementation (Table 4). For models incorporating MDT, education, or capacity building for self-care, the reported enablers included: group-based sessions, [8] care managed by a single facilitator [8, 11], a small team [11], adequate provider to patient ratio [24], integration into existing clinics [33], close collaboration between primary care doctors and the diabetes team in hospital [26], and adopting a multicultural approach [27]. Barriers included length of program being too long for patients to engage with consistently [30], low frequency of sessions [8], lack of skilled staff to cover periods of leave [11], low health literacy of patients and caregivers [26], and a lower drive among older children (> 12 years) to undertake diabetes related education [27].
For models that included outreach support, the enablers included having a dedicated and well-trained team [22], the adoption of a MDT approach [25] that is consistent and cohesive, and coupled with effective communication [28]. In one study, support between routine consultations was facilitated by 24-hour phone access to the diabetes team [25]. Access to clinics for those living in remote regions was a reported barrier by one study [28].
For models using shared care and decision making and integration of care, a reported enabler was having all the model components working well together [21]. A barrier was a lack of access to 24-hour ambulatory care and inequitable access for families of lower socio-economic status due to higher costs [23].
In the assessment of the sustainability of the models or care, three of 19 studies (16%) measured outcomes at two years [20, 27, 33], and five (26%) measured outcomes two years or longer after model implementation [11, 22, 24, 28, 29] (Table 1). Four of these studies (21%) did not mention sustainability of the model of care after implementation, although outcomes were measured [20, 27, 29, 33]. The remaining studies presented evidence for model sustainability by measuring outcomes once across a period of time [11, 22, 24, 28]. Several barriers and enablers associated with the sustainability of the models of care were described (Table 4).
Discussion
Our evidence synthesis identified a variety of implemented innovative models of care for T1D, with an MDT approach most frequently reported. The key components of the models included MDTs, shared medical appointments, shared decision making, capacity building for self-care, outreach support and mentoring and integrated care enabled by technology such as telehealth consultations and interactive educational programs delivered online or by teleconference.
The literature shows enormous variety of outcome measures reported across studies, which makes it difficult to synthesise evidence of benefits across different models. For example, some reported benefits in terms of improved maintenance of glycaemic levels [10, 21, 27, 30], and increased insulin pump usage, while others reported no improvements in health outcomes [29, 31, 32].
Improved psychosocial outcomes, including quality of life were consistently reported for models that included shared care, decision making, and integrated care [23, 29, 32]. These benefits are consistent with previous studies on integrated care models for other conditions such as chronic kidney disease [36], cancer survival [37], and mental illness [38]. It remains uncertain, however, whether improvements, or lack of improvements, can be directly attributed to the innovative model of care or its components, because of the differing models in use, and the large variety of outcome tools and measures being used across studies. Versloot et al. (2022) [29] for example, applied both a general measure of quality of life and a diabetes-specific measure of quality of life, showing that effects were stronger when the diabetes-specific measure was used [29]. This suggests that a greater consistency and standardisation of diabetes specific outcome measures may be needed to improve the reliability of evidence synthesis across studies and settings in the future.
Outreach support had previously been reported to contribute to positive health behaviors for adults living with diabetes [39], and for the provision of social support and capacity for skill building among people living with chronic conditions in rural areas [40]. Consistent with our findings, these positive outcomes are enabled by technology – usually a combination of telephone and online support, in addition to face-to-face consultations as previously described in a model of care for children living with medical complexity [41].
Over half of the studies reported on the implementation determinants of the model of care, however none used implementation science frameworks or theories to guide their work. Commonly reported enablers of successful model of care implementation included communication and team cohesiveness [9, 11, 21, 22, 25,26,27,28, 33]. These findings are consistent with those reported in other studies of paediatric integrated care models [41], and by adult consumers and providers commenting on integrated care models [42]. A review conducted by Bradford et al. (2016) [43] reported that establishing clear, efficient processes to support teams to manage care is important for the successful implementation and sustainability of models of care [43].
The key barriers identified for patient engagement with T1D models of care included program intensity requiring frequent engagement or long educational sessions [30], difficulties in accessibility due to connectivity problems for online components [39], or additional travel and cost for families living in rural regions [28]. This suggests that groups developing new models of care may benefit with closer engagement and co-design with end-users before launching new models of care or programs for T1D. Limited availability of skilled staff when team members were on leave also limited access [11], suggesting the need for adequate human resource planning and staff training when implementing new models of care.
Short follow-up periods after implementation limited assessment of the evidence for models’ sustainability. Nine (47%) of studies were evaluated at 12 months post implementations, and the follow-up period was not reported in two studies (11%). Only eight studies (42%) measured outcomes two years or longer after implementation, the longest follow-up period being six years [28]. For example, a rural MDT model of care that offered education and support showed significant benefits for glycaemic management and quality of life measures every 12 months for 3 years [11]. These findings are consistent with the known gaps in evidence for the sustainability of health programs [44], including for models of care for chronic health conditions [45]. Understanding the determinants of successful model of care implementation and sustainability should be a research priority to inform future T1D models of care development and co-design, as well as informing strategies for implementation and scaling up. For example, the Consolidated Framework for Implementation Science Research (CFIR) [46] and the Integrated Sustainability Framework (ISF) [45] provide comprehensive, flexible frameworks underpinned by robust theoretical grounding that lends itself to the study of implementation and sustainability of models of care while taking account of specific internal and external contexts [46].
Strengths and limitations of the current review
Applying the PRISMA guidelines, a rigorous multi-step team-based study selection process, a comprehensive search of four international academic databases and adhering to a registered protocol are all methodological strengths of this study. Most studies were from the USA and were conducted in large metropolitan settings which limits the generalisability of findings to other settings. Other limitations include selecting only articles written in English and from high income countries, and omitting grey literature may have impacted the comprehensiveness of results. Grey literature may be particularly important in this area as models of care may be reported in “in-house” service reports or evaluations that are not submitted for peer review and publication in journals. Additionally, our search criteria focused on implemented T1D models of care, and did not focus on other ways of driving improved health outcomes for T1D based on population registries or networks, for example the Swedish paediatric diabetes quality registry, SWEDIABKIDS [47] or the SWEET global network [48]. Future reviews should consider including grey literature and the impacts of registry data to drive improvements in health outcomes for T1D. Due to the wide heterogeneity of study methodologies, analysis methods, and outcome measures we were not able to pool data, and synthesis was challenging, limiting the generalisability of our findings. Other limitations included small sample sizes [21], limited scope [34], and single site models [10, 20,21,22, 24, 30, 31].
Conclusions
The evidence for the effectiveness, acceptability and sustainability of paediatric T1D models of care is currently limited and inconsistent, although a pattern is emerging. Across three broad categories of model components, that include an MDT approach, some studies reported benefits for children living with T1D, including improved glycaemic management, although other studies reported no benefit. Several psychosocial benefits such as improved quality of life and motivation were reported, especially for shared care models, but again some studies reported no benefit. Barriers to accessing these models by patients/families included program intensity, time commitment required, cost and location. Enhanced communication and team cohesiveness were reported as important enablers for effective care delivery. There is a need for greater consistency of outcome measures to enable more robust evidence synthesis across studies and contexts. We also identified a need to adopt longitudinal study designs with larger sample sizes and longer follow-up periods to better understand model of care sustainability. Future studies should be guided by robust theoretical frameworks to study implementation determinants and sustainability of T1D models of care.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Gregory GA, Robinson TI, Linklater SE, Wang F, Colagiuri S, de Beaufort C, et al. Global incidence, prevalence, and mortality of type 1 diabetes in 2021 with projection to 2040: a modelling study. Lancet Diabetes Endocrin. 2022;10(10):741–60.
Atkinson MA, Eisenbarth GS, Michels AW. Type 1 diabetes. Lancet. 2014;383(9911):69–82.
Patterson CC, Dahlquist G, Harjutsalo V, Joner G, Feltbower RG, Svensson J, et al. Early mortality in EURODIAB population-based cohorts of type 1 diabetes diagnosed in childhood since 1989. Diabetologia. 2007;50(12):2439–42.
Stene LC. Gaps in life expectancy for people with type 1 diabetes. Diabetologia. 2016;59(6):1150–2.
Peters A, Laffel L, Group ADATW. Diabetes care for emerging adults: recommendations for transition from pediatric to adult diabetes care systems: a position statement of the American diabetes association, with representation by the American College of osteopathic family physicians, the American Academy of pediatrics, the American association of clinical endocrinologists, the American osteopathic association, the centers for disease control and prevention, children with diabetes, the endocrine society, the International Society for pediatric and adolescent diabetes, juvenile diabetes research Foundation international, the National Diabetes education program, and the pediatric endocrine society (formerly Lawson Wilkins pediatric endocrine society). Diabetes Care. 2011;34(11):2477–85.
Barrett EJ, Liu Z, Khamaisi M, King GL, Klein R, Klein BE, et al. Diabetic microvascular disease: an endocrine society scientific statement. J Clin Endocrinol Metab. 2017;102(12):4343–410.
Cameron FJ, Garvey K, Hood KK, Acerini CL, Codner E. ISPAD clinical practice consensus guidelines 2018: diabetes in adolescence. Pediatr Diabetes. 2018;19(Suppl 27):250–61.
Fiallo-Scharer R, Palta M, Chewning BA, Rajamanickam V, Wysocki T, Wetterneck TB, et al. Impact of family‐centered tailoring of pediatric diabetes self‐management resources. Pediatr Diabetes. 2019;20(7):1016–24.
Wan W, Nathan AG, Reid MW, Majidi S, Fogel JL, Raymond JK, et al. The Economic Evaluation of Team Clinic—Group Approach to a care model of early adolescents with type 1 diabetes. J Pediatr Health Care. 2022;36(5):430–7.
Gandrud L, Altan A, Buzinec P, Hemphill J, Chatterton J, Kelley T, et al. Intensive remote monitoring versus conventional care in type 1 diabetes: a randomized controlled trial. Pediatr Diabetes. 2018;19(6):1086–93.
Goss PW, Paterson MA, Renalson J. A ‘radical’new rural model for pediatric diabetes care. Pediatr Diabetes. 2010;11(5):296–304.
Powell W, Corathers PD, Raymond S, Streisand J. New approaches to providing individualized diabetes care in the 21st century. Curr Diabetes Rev. 2015;11(4):222–30.
International Society for Pediatric and Adolescent Diabetes. ISPAD. Accessed on 23. Oct 2023. https://www.ispad.org/page/About.
Zurynski Y, Carrigan A, Meulenbroeks I, Sarkies MN, Dammery G, Halim N, et al. Transition models of care for type 1 diabetes: a systematic review. *Joint first authors. BMC Health Serv Res. 2023;23(1):779.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. 2021;88:105906.
Organization for Economic Co-operation and Development. Country Classification 2021 [ https://www.oecd.org/trade/topics/export-credits/documents/2021-cty-class-en-(valid-from-18-08-2021).pdf.
Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan—a web and mobile app for systematic reviews. Syst Rev. 2016;5(1):1–10.
McHugh ML. Interrater reliability: the kappa statistic. Biochem Med. 2012;22(3):276–82.
Hong QN, Gonzalez-Reyes A, Pluye P. Improving the usefulness of a tool for appraising the quality of qualitative, quantitative and mixed methods studies, the mixed methods Appraisal Tool (MMAT). J Eval Clin Pract. 2018;24(3):459–67.
Bergmann KR, Abuzzahab MJ, Arms J, Cutler G, Vander Velden H, Simper T et al. A quality improvement initiative to reduce hospitalizations for low-risk diabetic ketoacidosis. Pediatrics. 2020;145(3).
Floyd BD, Block JM, Buckingham BB, Ly T, Foster N, Wright R, et al. Stabilization of glycemic control and improved quality of life using a shared medical appointment model in adolescents with type 1 diabetes in suboptimal control. Pediatr Diabetes. 2017;18(3):204–12.
Franklin BE, Crisler SC Jr, Shappley R, Armour MM, McCommon DT, Ferry RJ Jr. Real-time support of pediatric diabetes self-care by a transport team. Diabetes Care. 2014;37(1):81–7.
Hatherly K, Smith L, Overland J, Johnston C, Brown-Singh L, Waller D, et al. Glycemic control and type 1 diabetes: the differential impact of model of care and income. Pediatr Diabetes. 2011;12(2):115–9.
Ilkowitz JT, Choi S, Rinke ML, Vandervoot K, Heptulla RA. Pediatric type 1 diabetes: reducing admission rates for diabetes ketoacidosis. Qual Manag Health Care. 2016;25(4):231.
Joshi KK, Haynes A, Smith G, Jones TW, Davis EA. Comparable glycemic outcomes for pediatric type 1 diabetes patients in metropolitan and non-metropolitan regions of Western Australia: a population‐based study. Pediatr Diabetes. 2018;19(3):486–92.
Katz ML, Laffel LM, Perrin JM, Kuhlthau K. Impact of type 1 diabetes mellitus on the family is reduced with the medical home, care coordination, and family-centered care. J Pediatr. 2012;160(5):861–7.
Pascual AB, Pyle L, Nieto J, Klingensmith GJ, Gonzalez AG. Novel, culturally sensitive, shared medical appointment model for hispanic pediatric type 1 diabetes patients. Pediatr Diabetes. 2019;20(4):468–73.
Simm PJ, Wong N, Fraser L, Kearney J, Fenton J, Jachno K, et al. Geography does not limit optimal diabetes care: use of a tertiary centre model of care in an outreach service for type 1 diabetes mellitus. J Paediatr Child Health. 2014;50(6):471–5.
Versloot J, Saab H, Minotti SC, Ali A, Ma J, Reid RJ et al. An integrated care model to support adolescents with diabetes-related quality of life concerns: an intervention study. Can J Diabetes. 2022.
Ellis DA, Carcone AI, Naar-King S, Rajkumar D, Palmisano G, Moltz K. Adaptation of an evidence-based diabetes management intervention for delivery in community settings: findings from a pilot randomized effectiveness trial. J Pediatr Psychol. 2019;44(1):110–25.
Hannon TS, Yazel-Smith LG, Hatton AS, Stanton JL, Moser EA, Li X, et al. Advancing diabetes management in adolescents: comparative effectiveness of mobile self‐monitoring blood glucose technology and family‐centered goal setting. Pediatr Diabetes. 2018;19(4):776–81.
Husted GR, Thorsteinsson B, Esbensen BA, Gluud C, Winkel P, Hommel E, et al. Effect of guided self-determination youth intervention integrated into outpatient visits versus treatment as usual on glycemic control and life skills: a randomized clinical trial in adolescents with type 1 diabetes. Trials. 2014;15(1):1–12.
Nansel TR, Iannotti RJ, Liu A. Clinic-integrated behavioral intervention for families of youth with type 1 diabetes: randomized clinical trial. Pediatrics. 2012;129(4):e866–73.
Herbert LJ, Sweenie R, Kelly KP, Holmes C, Streisand R. Using qualitative methods to evaluate a family behavioral intervention for type 1 diabetes. J Pediatr Health Care. 2014;28(5):376–85.
Walker AF, Haller MJ, Gurka MJ, Morris HL, Bruggeman B, Miller K, et al. Addressing health disparities in type 1 diabetes through peer mentorship. Pediatr Diabetes. 2020;21(1):120–7.
Scherpbier-de Haan ND, Vervoort GM, van Weel C, Braspenning JC, Mulder J, Wetzels JF, et al. Effect of shared care on blood pressure in patients with chronic kidney disease: a cluster randomised controlled trial. Br J GenPract. 2013;63(617):e798–806.
Shad A, Myers SN, Hennessy K. Late effects in cancer survivors:the shared care model. Curr Onc Rep. 2012;14(2):182–90.
Kelly BJ, Perkins DA, Fuller JD, Parker SM. Shared care in mental illness: a rapid review to inform implementation. Int J Ment. 2011;5(1):1–12.
Ingram M, Gallegos G, Elenes J. Diabetes is a community issue: the critical elements of a successful outreach and education model on the U.S.-Mexico border. Prev Chronic Dis. 2005;2(1):A15–A.
Lauckner HM, Hutchinson SL. Peer support for people with chronic conditions in rural areas: a scoping review. Rural Remote Health. 2016;16(1):1–14.
Altman L, Breen C, Ging J, Burrett S, Hoffmann T, Dickins E et al. Dealing with the hospital has become too difficult for us to do alone–developing an Integrated Care Program for Children with Medical Complexity (CMC). Int J Integr Care. 2018;18(3).
Carrigan A, Roberts N, Clay-Williams R, Hibbert P, Austin E, Pulido DF et al. What do consumer and providers view as important for integrated care? A qualitative study. BMC Health Serv Res. 2023;23(1).
Bradford NK, Caffery LJ, Smith AC. Telehealth services in rural and remote Australia: a systematic review of models of care and factors influencing success and sustainability. Rural Remote Health. 2016;16(4):1–23.
Zurynski Y, Herkes-Deane J, Holt J, McPherson E, Lamprell G, Dammery G, et al. How can the healthcare system deliver sustainable performance? A scoping review. BMJ Open. 2022;12(5):e059207.
Shelton RC, Cooper BR, Stirman SW. The sustainability of evidence-based interventions and practices in public health and health care. Annu Rev Public Health. 2018;39:55–76.
Damschroder LJ, Reardon CM, Widerquist MAO, Lowery J. The updated Consolidated Framework for Implementation Research based on user feedback. Implement Sci. 2022;17(1):1–16.
Peterson A, Hanberger L, Åkesson K, Bojestig M, Andersson Gäre B, Samuelsson U. Improved results in paediatric diabetes care using a quality registry in an improvement collaborative: a case study in Sweden. PLoS ONE. 2014;9(5):e97875.
SWEET Pediatric Diabetes. Accessed on 23. Oct 2023. https://www.sweet-project.org/.
Acknowledgements
A review describing similar methodologies has been published in BMC Health Services Research [14].
Funding
This work was funded by the JDRF Australia [5_SRA_2021_1088_m-X]. The funding source played no role in the design, collection, analysis, or interpretation of the data or in the decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Contributions
YZ, ED, TJ and JB designed the research. YZ, AC, MS, IM, GD, NH, and RL conducted the research. AC and YZ analysed the data and drafted the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not required as a review article.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it.The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Carrigan, A., Meulenbroeks, I., Sarkies, M. et al. Benefits, implementation and sustainability of innovative paediatric models of care for children with type 1 diabetes: a systematic review. BMC Pediatr 24, 502 (2024). https://doi.org/10.1186/s12887-024-04945-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-024-04945-2