
Abstract
Background
To investigate serum irisin levels in girls at different developmental status and explore the significance of irisin for the diagnosis of central precocious puberty (CPP) in girls.
Methods
In this cross-sectional study 111 girls were enrolled, including 43 cases of CPP, 44 cases of peripheral precocious puberty (PPP) and 24 cases of girls with normal sexual development as controls. The data on age, weight and height, measured blood levels of luteinizing hormone (LH), follicle stimulating hormone (FSH), estradiol, and irisin were collected. Pelvic Doppler ultrasound was performed to evaluate uterine length, transverse diameter, anteroposterior diameter. The girls were divided into non-CPP group and CPP group according to gonadotropin-releasing hormone (GnRH) stimulation test.
Results
Serum irisin levels were significantly higher in CPP group than in PPP group and normal control group. Serum irisin level was positively correlated with basal LH level, basal FSH level, peak LH level, peak LH /FSH ratio, uterine volume, bone age, and bone age index. The area under the curve, cut-off value, sensitivity and specificity of serum irisin were 0.958, 219.255 pg/ml, 100% and 80.6%. The combined diagnosis of CPP in girls by serum irisin and serum basal LH combined with uterine volume had an AUC, sensitivity, and specificity of 0.994, 97.6%, and 100%, superior to that of the single index.
Conclusions
Serum irisin level in girls with CPP is significantly increased. An irisin combined index could help the diagnosis of CPP in girls.
Similar content being viewed by others

Introduction
Precocious puberty refers to the rapid development of internal and external genital organs and the appearance of secondary sexual characteristics before the age of 8 years for girls and 9 years for boys [1]. In the latest precocious puberty diagnosis and treatment guideline in China, the age is defined as 7.5 years old for girls [2]. Based on whether the hypothalamic-pituitary-gonadal axis (HPGA) function is activated, precocious puberty can be classified into central precocious puberty (CPP), peripheral precocious puberty (PPP) and incomplete precocious puberty [1]. The causes of PPP include tumors with abnormal secretion of sex hormones, gonadotropin-secreting tumors, exposure or ingestion of exogenous sex hormones, gene mutations affecting sex hormone production, adrenocortical adenomas, adrenal malignancies, and special syndromes such as Mc-Cune-Albright syndrome. CPP is a common pediatric endocrine disease, which seriously affects the physical and mental health of children. In recent years, the incidence of precocious puberty has been reported to be increasing worldwide, and the age of onset is also higher than before [3,4,5,6,7,8].
The gonadotropin-releasing hormone (GnRH) provocation test is the gold standard for the diagnosis of CPP [1], but it requires repeated blood sampling, which increases the pain of the children and the economic burden of the parents, and is not easy to be carried out in the outpatient clinic. Therefore, exploring a simple screening method for CPP has become one of the research hotspots in the field of pediatric endocrinology. Irisin is a newly discovered myogenic factor [9]. FNDC5 is the precursor of irisin and is mainly expressed in the muscles, especially in skeletal muscles, while its expression level is low in the kidney, liver and lung [10]. In addition, FNDC5 is mainly expressed in the proximal pituitary. The expression of FNDC5 and irisin in the HPGA axis correlates with developmental and metabolic status and is expressed in a sex-specific manner. Irisin promotes GnRH expression to participate in the regulation of the reproductive system [11, 12]. Irisin was investigated in CPP, but its levels in PPP have not yet been investigated. Therefore, this study aimed to investigate serum irisin in control and girls with CPP and PPP, and to develop an index based on irisin levels for the diagnosis of CPP.
Methods
Subjects
This was a cross-sectional study and the sample size was calculated by G-power software. Eighty-seven girls with precocious puberty who attended the pediatric endocrinology clinic of Huai’an First Hospital affiliated with Nanjing Medical University from May 2022 to June 2023 were selected as the study subjects, and 24 girls with normal sexual development during the same period were used as controls. None of the girls were being treated during this study. Inclusion criteria for precocious puberty: girls with breast development before the age of 8 years. Exclusion criteria: (1) precocious thelarche, pubic hair appears early, simple early menarche; (2) previous use of drugs affecting the HPGA axis; (3) poor adherence to the doctor’s instructions. All enrolled children and their parents were fully informed about the study and gave informed consent, and the study was approved by the Ethics Committee of Huai’an First Hospital affiliated with Nanjing Medical University (KY-2023-068-01).
Data collection
Height, weight, waist circumference (WC), hip circumference, body mass index (BMI) were measured by trained professionals, and height-for-age z-scores (HAZ), weight-for-age z-scores (WAZ) and BMI-for-age z-scores (BAZ) were calculated with the help of the WHO AhthroPlus (version 1.0.4) software [13]. Bone age index (BAI) was calculated as (bone age- actual age) /actual age. Breast staging was based on the Tanner criteria [14]. Serum levels of basal gonadotropin (Gn), estradiol, prolactin (PRL), insulin like growth factor 1 (IGF-1) were measured using electrochemiluminescence immunoassay analyzer with matching kits (Roche). Greulich & Pyle standardized atlas was used to determine bone age. Uterine volume, ovarian volume, number of follicles, and uterine length were assessed by an experienced sonographer with specialized training.
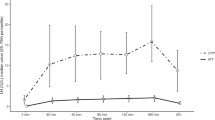
Girls were divided into the CPP group and the PPP group according to the results of GnRH stimulation test: basal values of serum Gn were determined before the stimulation test, and triptorelin acetate (Dabiga, 0.1 mg/branch, Phylin Pharmaceutical Co., Ltd. Germany) was injected subcutaneously with 2.5 µg/kg, maximum 100 µg, and 2 ml of venous blood was withdrawn sequentially at 15, 30, 60, and 90 min after the injection to determine the levels of serum Gn (Immune chemiluminescence method).
ELISA
The girls fasted for 12 h, and the venous blood was drawn at 8:00 a.m. under a quiet state; the blood samples were centrifuged at 3000 r/min for 10 min. The serum samples were stored at -80℃ in a special refrigerator for specimens. The serum irisin level was determined by ELISA kit (Qiaoyi Company, Anhui, China; cat No: JEN-017).
Data analysis
SPSS 25.0 software was used for data analysis. Qualitative information was expressed as percentages, and the chi-square test was used to compare two groups. Continuous variables with normal distribution were expressed as mean ± standard deviation (SD), independent sample t-test was used for comparison of two groups, one-way ANOVA was used for comparison of three groups, and Pearson correlation analysis was used for correlation analysis. Non-normally distributed continuous variables were expressed as median (quartile) [M (P25, P75 )], Man- Whitney U test was used for two-group comparisons, Kruskal-Wallis H test was used for three-group comparisons, and correlation analyses were performed using Spearman rank correlation analysis. Receiver operator characteristic curve (ROC) was plotted, and logistic regression was used to explore the role of single versus combined indicators in the diagnosis of CPP. P < 0.05 was considered significant difference, and two-sided tests were used for all tests.
Results
General information in three groups of girls
A total of 43 CPP girls, 44 PPP girls and 24 girls with normal sexual development were included. There were significant differences in age, height, WAZ, weight, HAZ, BMI and BAZ among the three groups of girls (P < 0.05); there were significant differences in waist circumference, hip circumference, bone age, BAI, IGF-1, basal LH, basal FSH, estradiol, testosterone, uterine volume, ovary volume, peak LH, peak LH /FSH ratio and glucose between CPP and PPP groups (P < 0.05), but there were no significant differences in PRL, peak FSH, total cholesterol (TC) and triglycerides (TG) (P > 0.05, Table 1). The tanner stages and the percentage of children in each stage were shown in Table 2. CPP and PPP groups had complete data, and normal control group had data on age, height, and weight.
Comparison of serum irisin levels in three groups of girls
The detectable rates of serum irisin in CPP group, PPP group, and normal control group were 95.35%, 70.45%, and 79.17%, and mean irisin level in CPP group 568.61(404.42,1157.14) pg/ml was higher than that in PPP group 118.74(76.81,202.86) pg/ml and normal control group 100.76(52.89,160.75) pg/ml (P < 0.05). There was no significant difference in mean irisin level between PPP group and normal control group (P > 0.05, Fig. 1).

Comparison of irisin levels in CPP group, PPP group and normal control group (N)
Correlation analysis of serum irisin with age, height, weight, blood sex hormones, bone age index and uterine volume in three groups of girls
Spearman’s correlation analysis of serum irisin and general clinical data of girls suggested that serum irisin level of girls was positively correlated with age, height, HAZ, weight, WAZ, BMI, waist circumference, hip circumference and bone age, BAI, basal LH and FSH, peak LH, peak LH/FSH ratio, estradiol, IGF-1, uterine volume, but was negatively correlated with total cholesterol (TG) (P < 0.05, Fig. 2). No statistical significance was found in the correlation with BAZ, prolactin, peak FSH, ovarian volume, glucose, and triglycerides (P > 0.05, Fig. 2). CPP group had 43 girls, PPP group had 44 girls and normal control group had 24 girls. CPP and PPP groups had complete data, and normal control group had data on age, height, weight and irisin.

Correlation analysis between irisin and other clinical data
Multifactor logistic regression analysis
Whether GnRH stimulation test results were diagnosed as CPP or not was the dependent variable, and multivariate Logistic regression analysis was performed for 43 girls in CPP group and 44 girls in PPP group. There was no significant covariance for the respective variables (VIF < 5). By multifactor regression analysis we established regression model Y = -11.582 + 0.014* irisin + 2.934* serum basal LH + 3.929 * uterine volume (Table 3).
ROC curve analysis of serum irisin level and uterine volume in the diagnosis of precocious puberty in girls
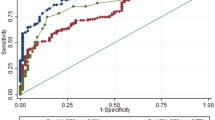
ROC curve analysis was performed for 43 girls in CPP group and 44 girls in PPP group. to compare the value of serum irisin level and uterine volume for the diagnosis of CPP in girls. The sensitivity and specificity of basal LH ≥ 0.3 U/L in the diagnosis of CPP were 85.4% and 93.5%, respectively. The cutoff level of irisin at 219.255 pg/ml had a high AUC and sensitivity for the diagnosis of CPP.
Serum irisin had a high AUC and sensitivity, and serum LH basal value and uterine volume had a high specificity (Table 4). By multifactor regression analysis we established regression model Y = -11.582 + 0.014* irisin + 2.934* serum basal LH + 3.929 * uterine volume. The above indicators were used as the combined indicators for the diagnosis of CPP, and the ROC curve analysis was performed with the combined index Y. The AUC, sensitivity, and specificity of the model combined with auxiliary diagnosis of CPP were 0.994, 97.6%, and 100%, respectively, which were better than those of single index (Fig. 3). Therefore, the combination of the above three indicators had the highest efficiency in the diagnosis of CPP, and the difference was significant (P < 0.05).

ROC curve of serum irisin, uterine volume and combined indexes for the diagnosis of CPP in girls. ROC curves were based on the analysis of 43 girls in CPP group and 44 girls in PPP group
Discussion
Sexual development is controlled by the hypothalamic-pituitary-gonadal axis, which is inhibited in childhood and activated by complex regulatory mechanisms to mark the onset of puberty [15]. Abnormal sexual development such as precocious puberty causes a series of harms to children, such as early menarche in girls, premature epiphyseal closure, which affects the lifelong height, and even psychosocial and behavioral problems such as anxiety and depression [16, 17]. Recent studies have shown that early menarche increases the incidence of postmenopausal breast cancer and the risk of type 2 diabetes and cardiovascular disease [18,19,20]. Epidemiological studies have shown that early puberty in women or men is associated with a higher incidence of diseases of the reproductive system, endocrine system, circulatory system, digestive system and nervous system [21, 22]. Therefore, early diagnosis and treatment of precocious puberty have important significance.
Currently, basal LH levels are usually used in clinical practice to assess HPGA activity. The European guideline consensus update suggests that HPGA initiation can be determined when the basal luteinzing hormone (LH) value is greater than 0.83 [23]. However, GnRH provocation test is still required to clarify the type of precocious puberty in most children [24]. However, the results of GnRH stimulation test are affected by obesity and other factors, and false-negative phenomenon may occur in the clinic. Therefore, there is an urgent need to develop diagnosis methods of precocious puberty that are not affected by obesity and other factors.
It has been shown that irisin levels are associated with puberty, and irisin levels are significantly correlated with Tanner staging [25, 26]. The irisin precursor, type III fibronectin component-containing protein 5 (FNDC5), is mainly expressed in the proximal pituitary gland, and is upregulated during puberty to promote the expression of LH and follicle-stimulating hormone (FSH) [27]. In present study, serum irisin levels were significantly higher in girls with CPP than in girls with PPP and normal sexual development, suggesting that irisin level may be useful for the initial screening of precocious puberty.
A growing number of studies have shown that obese children are prone to precocious puberty, and basal LH levels and peak LH excitation in obese girls are significantly lower than in girls with normal BMI [28, 29]. BMI is correlated with body fat and is not affected by height. In present study, we found that serum irisin levels did not correlate with BAZ in girls with CPP. Therefore, irisin may exclude the interference of obesity in the diagnosis of CPP. Uterine volume and serum Gn levels are known to be helpful in the diagnosis of precocious puberty, but the reliability is not good and the interference of factors such as obesity cannot be excluded. In this study, serum irisin, serum basal LH and uterine volume were combined to diagnose CPP in girls, which were better than a single index.
This study showed a high correlation between irisin and bone age and BAI. Irisin can be higher secondarily to the higher bone age of CPP girls, as Irisin and bone age have the higher correlation among the variables studied. Recent evidences suggest that irisin is involved in the regulation of bone state [30]. Bone age examination is known to be radioactive and cannot be repeated in a short period of time. We will further study the relationship between irisin and bone age in CPP and PPP groups in order to reduce the exposure of radioactive substances in the treatment of children with precocity.
Conclusion
Although this study has limitations as a single-center study with a small number of cases, and we did not monitor the changes of irisin levels during the follow-up of CPP treatment, our study was the first report on the use of irisin combined index to diagnose CPP. Our results demonstrate that serum irisin level has no correlation with BAZ value, and can improve the diagnosis of CPP when it is combined with serum basal LH and uterine volume.
Data availability
All data are available upon request to correspondence authors.
References
Bradley SH, Lawrence N, Steele C, Mohamed Z. Precocious puberty. BMJ. 2020;368:l6597.
The Chinese medical. Association branch of pediatrics of the genetic metabolic endocrine group, the journal pediatrics editorial board. Expert consensus on the diagnosis and treatment of central precocious puberty (2022). Chin J Pediatr. 2023;61(1):16–22.
Kang S, Park MJ, Kim JM, et al. Ongoing increasing trends in central precocious puberty incidence among Korean boys and girls from 2008 to 2020. PLoS ONE. 2023;18(3):e0283510.
Bräuner EV, Busch AS, Eckert-Lind C, et al. Trends in the incidence of central precocious puberty and normal variant puberty among children in Denmark, 1998 to 2017. JAMA Netw Open. 2020;3(10):e2015665.
Eckert-Lind C, Busch AS, Petersen JH, et al. Worldwide secular trends in Age at Pubertal Onset assessed by breast development among girls: a systematic review and Meta-analysis. JAMA Pediatr. 2020;174(4):e195881.
Li H, Yu G, Duan H, Fu J, et al. Changes in children’s Healthcare visits during coronavirus Disease-2019 pandemic in Hangzhou, China. J Pediatr. 2020;224:146–9.
Street ME, Ponzi D, Renati R, et al. Precocious puberty under stressful conditions: new understanding and insights from the lessons learnt from international adoptions and the COVID-19 pandemic. Front Endocrinol (Lausanne). 2023;14:1149417.
Wang X, Yao Z, Liu D, Yu C, Li H. Current and future therapies for abnormal early embryogenesis with assisted reproductive technology. Biocell. 2022;46(8):1803–6.
Boström P, Wu J, Jedrychowski MP, et al. A PGC1-α-dependent myokine that drives brown-fat-like development of white fat and thermogenesis. Nature. 2012;481(7382):463–8.
Wahab F, Shahab M, Behr R, Hypothesis. Irisin is a metabolic trigger for the activation of the neurohormonal axis governing puberty onset. Med Hypotheses. 2016;95:1–4.
Jiang Q, Zhang Q, Lian A, Xu Y. Irisin stimulates gonadotropins gene expression in tilapia (Oreochromis niloticus) pituitary cells. Anim Reprod Sci. 2017;185:140–7.
Anastasilakis AD, Polyzos SA, Saridakis ZG, et al. Circulating irisin in healthy, young individuals: day-night rhythm, effects of food intake and exercise, and associations with gender, physical activity, diet, and body composition. J Clin Endocrinol Metab. 2014;99(9):3247–55.
WHO Multicentre Growth Reference Study Group. WHO Child Growth standards based on length/height, weight and age. Acta Paediatr Suppl. 2006;450:76–85.
Marshall WA, Tanner JM. Variations in pattern of pubertal changes in girls. Arch Dis Child. 1969;44(235):291–303.
Abreu AP, Kaiser UB. Pubertal development and regulation. Lancet Diabetes Endocrinol. 2016;4(3):254–64.
Kaplowitz PB. Update on precocious puberty: who should be treated? Adv Pediatr. 2020;67:93–104.
Huang H, Liu L, Su S, et al. Self-consciousness and depression in precocious pubertal children. J Int Med Res. 2021;49(5):3000605211020227.
Lan B, Lv D, Yang M, Sun X, Zhang L, Ma F. Psychological distress and quality of life in Chinese early-stage breast cancer patients throughout chemotherapy. J Natl Cancer Cent. 2022;2(3):155–61.
Ding R, Xiao Y, Mo M, Zheng Y, Jiang YZ, Shao ZM. Breast cancer screening and early diagnosis in Chinese women. Cancer Bio Med. 2022;19(4):450–67.
Day FR, Elks CE, Murray A, et al. Puberty timing associated with diabetes, cardiovascular disease and also diverse health outcomes in men and women: the UK Biobank study. Sci Rep. 2015;5:11208.
Li Y, Hao C, Chen W, Meng Q. Analysis of specific lipid metabolites in cord blood of patients with gestational diabetes mellitus. Biocell. 2022;46(6):1565–73.
Pai LF, Wang DS, Hsu WF, et al. New insights into precocious puberty and ADHD: a nationwide cohort study. Pediatr Res. 2022;92(6):1787–94.
Bangalore Krishna K, Fuqua JS, et al. Use of Gonadotropin-releasing hormone analogs in children: update by an International Consortium. Horm Res Paediatr. 2019;91(6):357–72.
Wood CL, Lane LC, Cheetham T, Puberty. Normal physiology (brief overview). Best Pract Res Clin Endocrinol Metab. 2019;33(3):101265.
Reinehr T, Elfers C, Lass N, et al. Irisin and its relation to insulin resistance and puberty in obese children: a longitudinal analysis. J Clin Endocrinol Metab. 2015;100(5):2123–30.
Elizondo-Montemayor L, Mendoza-Lara G, Gutierrez-DelBosque G, et al. Relationship of circulating irisin with body composition, physical activity, and Cardiovascular and Metabolic disorders in the Pediatric Population. Int J Mol Sci. 2018;19(12):3727.
Wahab F, Khan IU, Polo IR, et al. Irisin in the primate hypothalamus and its effect on GnRH in vitro. J Endocrinol. 2019;241(3):175–87.
Shi L, Jiang Z, Zhang L. Childhood obesity and central precocious puberty. Front Endocrinol (Lausanne). 2022;13:1056871.
Zhao C, Tang Y, Cheng L. Diagnostic value of LH Peak Value of the GnRH stimulation test for girls with precocious puberty and its correlation with body Mass Index. Comput Math Methods Med. 2022;2022:4118911.
Colaianni G, Sanesi L, Storlino G, et al. Irisin and Bone: from Preclinical studies to the evaluation of its circulating levels in different populations of human subjects. Cells. 2019;8(5):451.
Acknowledgements
Not applicable.
Funding
This study was supported by Scientific Research Fund of Jiangsu Maternal and Child Health Association (No. FYX202213).
Author information
Authors and Affiliations
Contributions
JW, YT, GC, MY, QG, YW performed the experiments, WZ designed and supervised the study. All authors read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All enrolled children and their parents were fully informed about the study and gave informed consent, and the study was approved by the Ethics Committee of Huai’an First Hospital affiliated with Nanjing Medical University (KY-2023-068-01).
Consent for publication
Not applicable.
Competing interests
All authors report no conflicts of interest in this work.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, J., Tang, Y., Chen, G. et al. Irisin combined index to diagnose central precocious puberty in girls: a cross-sectional study. BMC Pediatr 24, 275 (2024). https://doi.org/10.1186/s12887-024-04743-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-024-04743-w