
Abstract
Background
Necrotizing enterocolitis (NEC) is a serious gastrointestinal disease, primarily affects preterm newborns and occurs after 7 days of life (late-onset NEC, LO-NEC). Unfortunately, over the past several decades, not much progress has been made in its treatment or prevention. This study aimed to analyze the risk factors for LO-NEC, and the impact of LO-NEC on short-term outcomes in very preterm infants (VPIs) with a focus on nutrition and different onset times.
Method
Clinical data of VPIs were retrospectively collected from 28 hospitals in seven different regions of China from September 2019 to December 2020. A total of 2509 enrolled VPIs were divided into 2 groups: the LO-NEC group and non-LO-NEC group. The LO-NEC group was divided into 2 subgroups based on the onset time: LO-NEC occurring between 8 ~ 14d group and LO-NEC occurring after 14d group. Clinical characteristics, nutritional status, and the short-term clinical outcomes were analyzed and compared among these groups.
Results
Compared with the non-LO-NEC group, the LO-NEC group had a higher proportion of anemia, blood transfusion, and invasive mechanical ventilation (IMV) treatments before NEC; the LO-NEC group infants had a longer fasting time, required longer duration to achieve the target total caloric intake (110 kcal/kg) and regain birthweight, and showed slower weight growth velocity; the cumulative dose of the medium-chain and long-chain triglyceride (MCT/LCT) emulsion intake in the first week after birth was higher and breastfeeding rate was lower. Additionally, similar results including a higher proportion of IMV, lower breastfeeding rate, more MCT/LCT emulsion intake, slower growth velocity were also found in the LO-NEC group occurring between 8 ~ 14d when compared to the LO-NEC group occurring after 14 d (all (P < 0.05). After adjustment for the confounding factors, high proportion of breastfeeding were identified as protective factors and long fasting time before NEC were identified as risk factors for LO-NEC; early feeding were identified as protective factors and low gestational age, grade III ~ IV neonatal respiratory distress syndrome (NRDS), high accumulation of the MCT/LCT emulsion in the first week were identified as risk factors for LO-NEC occurring between 8 ~ 14d. Logistic regression analysis showed that LO-NEC was a risk factor for late-onset sepsis, parenteral nutrition-associated cholestasis, metabolic bone disease of prematurity, and extrauterine growth retardation.
Conclusion
Actively preventing premature birth, standardizing the treatment of grade III ~ IV NRDS, and optimizing enteral and parenteral nutrition strategies may help reduce the risk of LO-NEC, especially those occurring between 8 ~ 14d, which may further ameliorate the short-term clinical outcome of VPIs.
Trial registration
ChiCTR1900023418 (26/05/2019).
Similar content being viewed by others


Background
Necrotizing enterocolitis (NEC) is a serious digestive tract disease which occurs more frequently in very preterm infants (VPIs) during the neonatal period. According to the data of several systematic reviews [1, 2], the incidence of NEC is 7% and the mortality is 20%~30% in premature infants with a birth weight of 500 ~ 1500 g, and there has been no evident improvement in these statistics in recent years. A study enrolling 10,823 VPIs from 57 tertiary neonatal intensive care units (NICUs) of the Chinese Neonatal Network in 2019 showed that the survival rate of VPIs was 95.4%, and the incidence of NEC was 4.9%; notably, the incidence of NEC increased with decreasing gestational age [3]. In 90% cases, NEC occurred in VPIs with a gestational age of < 32 weeks [4]. The risk factors for NEC vary with the time of onset. Short et al. [5]. Proposed an onset time of ≤ 7 days after birth to represent early-onset NEC (EO-NEC) and an onset time of > 7 days after birth as late-onset NEC (LO-NEC). Considering the small amount of enteral nutrition in the early postnatal period, the causes of EO-NEC are mostly related to perinatal factors, such as asphyxia and intrauterine infection. Conversely, LO-NEC is closely related to high-risk factors in the NICU, such as improper feeding, intestinal flora imbalance, long fasting time, and late-onset infection [6]. Most NEC cases occur 13 ~ 23 days after birth, which represents LO-NEC [2]. There is a paucity of data on the related factors of those cases occurring between 8 ~ 14 days after birth, which also belong to LO-NEC. Therefore, analyzing the high-risk factors for LO-NEC with different onset times to prevent the occurrence of NEC has immense guiding significance in clinical practice.
In terms of nutrition, we explored the high-risk factors for LO-NEC and its impact on the short-term clinical outcomes among VPIs through a retrospective analysis of the clinical data from 28 Chinese NICUs in our study. We hope the findings will help further optimize the treatment strategy for premature infants in the NICU, particularly with improving the nutrition management, reducing the incidence of LO-NEC, and providing a theoretical basis for improving the short-term prognosis of VPIs with LO-NEC.
Methods
Study design and sample
The data used in this study were sourced from a prospective multicenter study that involved the influencing factors of extrauterine growth restriction (EUGR) in VPIs from different regions of China (clinical trial registry: www.chictr.org.cn; registration number: ChiCTR1900023418; date of first registration: 26/05/2019). The study was approved by the Ethics Committee of the Women and Children’s Hospital, School of Medicine, Xiamen University (No. KY-2019-016). In this study, the clinical data of VPIs in the NICU were collected from 28 tertiary first-class hospitals in 20 provinces of China between September 2019 and December 2020.
Inclusion criteria
Infants born with a gestational age (GA) of < 32 weeks or birth weight (BW) of < 1500 g who were admitted to the participating NICUs within 24 h of birth were included.
Exclusion criteria
We excluded infants who (1) had a congenital malformation or metabolic disease; (2) died or whose treatment was interrupted, followed by discharge from the hospital because of parents’ wishes or financial constraints; (3) had a hospitalization period of < 2 weeks; (4) had incomplete medical record information; (5) had EO-NEC.
Study dataset
Depending on whether LO-NEC occurred, VPIs who met the criteria were divided into 2 groups: LO-NEC group and non-LO-NEC group. The LO-NEC group was divided into 2 subgroups based on the onset time: LO-NEC occurring between 8 ~ 14d group and LO-NEC occurring after 14d group. Demographic and clinical data were collected for the following parameters: perinatal information (e.g., GA, BW, the use of antenatal steroids, mode of delivery, the Apgar score at 5 min, and maternal complications during pregnancy); nutrition-related data, including breastfeeding, use of breast milk fortifier, fasting time, weight growth velocity (GV), and parenteral nutrition; and short-term clinical outcomes, such as severe intraventricular hemorrhage (IVH; grade 3 or 4), periventricular leukomalacia (PVL), moderate and severe bronchopulmonary dysplasia (BPD), parenteral nutrition-associated cholestasis (PNAC), and stage 3 through 5 retinopathy of prematurity (ROP) in either eye. Data for diseases and interventions in the LO-NEC group were collected before the occurrence of NEC.
Study definitions
Late-onset NEC
NEC defined as Bell stage II or greater according to established criteria [7]. The onset time of > 7 days after birth was defined as LO-NEC [5]. In this study, after removing excluded cases (as described above), infants diagnosed as having confirmed NEC (≥ stage II) with an onset time of > 7 days after birth were included in the LO-NEC group, and the remaining infants were enrolled in the non-LO-NEC group.
Definitions related to nutrition management
(1) Early feeding was defined as starting feeding within 24 h of birth. (2) High proportion of breastfeeding was defined as breastfeeding accounting for more than 50% of the total enteral feeding during hospitalization. (3) The average weight GV (after regaining BW, g/kg/day) = [1000 × ln(Wn/W1)]/(Dn - D1). Wn: The weight of the infant at the day of discharge (g); W1: The weight of the infant on the first day after delivery (g); Dn: Length of hospitalization in days (d); and D1: the length of regaining BW in days (d) [8].
Definitions related to diseases (including short-term outcomes)
(1) Hemodynamically significant patent ductus arteriosus (hsPDA) was defined as a patent ductus arteriosus catheter diameter of > 1.5 mm, left atrial diameter/aortic diameter of ≥ 1.4, or left ventricular end-diastolic diameter/aortic diameter of ≥ 2.1 accompanied by one of the following clinical manifestations: heart murmur, tachycardia (sustained ≥ 160 beats/min), increased respiration, increased pulse pressure (> 25 mmHg), hypotension, flushing, or cardiac dilation [9]. (2) The diagnostic criteria of early-onset sepsis (EOS) and late-onset sepsis (LOS; including clinical and diagnosis criteria) were based on the Expert Consensus on the Diagnosis and Treatment of Neonatal Sepsis (2019 Edition) [10]. (3) The EUGR evaluation criteria refer to the Fenton growth curve published in 2013 [11]. ① The evaluation criteria for percentile were as follows: VPI with a weight below the 10th percentile at the time of discharge or 36 weeks of corrected gestational age; ② A change in the z-score (Δz value) of weight by more than 1 between two points (discharge/36 weeks of corrected gestational age and birth). (4) Moderate and severe BPD, severe IVH (grade 3 or 4), and stage 3–5 ROP in either eye were diagnosed as per standard definitions and the published literature [12,13,14]. (5) Finally, diagnoses of grade III–IV neonatal respiratory distress syndrome (NRDS), PNAC, PVL, metabolic bone disease of prematurity (MBDP), and anemia were established by referring to Practical Neonatology (5th edition) [15].
Statistical methods
The counting data rate (%) indicated that a comparison between groups was performed using χ2 test. The Kolmogorov–Smirnov test was used to evaluate whether the measurement data conformed to the normal distribution. Normally distributed measurement data were expressed as ± s, and the two independent samples t-test was used for between-group comparisons, whereas non-normally distributed measurement data were expressed as M (Q1, Q3). The rank-sum test was used for between-group comparisons. Multivariate analysis was performed using binary/triple logistic regression analysis and linear regression analysis. All statistical analyses were conducted using a software program (SPSS, version 26.0; IBM, Armonk, NY, USA), with statistical significance evaluated using two-sided P values at the 5% testing level.
Results
General information
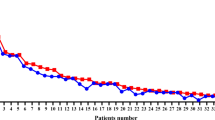
A total of 2600 preterm infants with a GA of < 32 weeks were admitted during the study period. After excluding 86 cases with incomplete medical information and 5 EO-NEC cases, the remaining 2509 infants enrolled in the analysis included 212 cases (8.4%) in the LO-NEC group and 2297 cases (91.6%) in the non-LO-NEC group (Fig. 1). Among LO-NEC VPIs, 47 cases were received surgical treatment, and 165 cases were received conservative treatment. Clinical characteristics of the LO-NEC VPIs with these two treatment methods were presented in Supplementary Table 1. The median age of VPIs in the LO-NEC group was 14 days (11,19); 60.4% of them were 8 ~ 14 days old, and 39.6% were > 14 days old (Fig. 2).

Subject enrollment and selection flow chart

Numbers of participants according to age of late-onset necrotizing enterocolitis
Comparison of perinatal characteristics
Compared with infants in the non-LO-NEC group, those in the LO-NEC occurring between 8 ~ 14d group had a lower GA (29.8 weeks vs. 30.1 weeks) and those in the LO-NEC occurring after 14 d group had a lower BW (1260.0 g vs. 1340.0 g); furthermore, the LO-NEC group had a higher proportion of anemia, blood transfusion, and invasive mechanical ventilation (IMV) treatments before NEC. The 3 groups did not significantly differ in other perinatal factors, such as mode of delivery, male:female ratio, multiple births, percentage of small for gestational age (SGA) infants, full-course antenatal steroids, maternal complications (e.g., gestational diabetes mellitus and hypertensive disorder complicating the pregnancy), and underlying disease (e.g., EOS, grade III ~ IV NRDS, and hsPDA) (all P > 0.05; Table 1).
Comparison of nutritional status
Compared with infants in the non-LO-NEC group, those in the LO-NEC group took longer to reach 110 kcal/(kg·d) total caloric intake had a longer fasting time; those in the LO-NEC occurring between 8 ~ 14d group took longer to regain BW (10.5 days vs. 9.0 days; all P < 0.05). Furthermore, infants in the LO-NEC occurring between 8 ~ 14d group had a lower breastfeeding rate, lower GV, and higher cumulative dose of medium-chain and long- chain triglyceride (MCT/LCT) emulsion in the first week after birth than those in the LO-NEC occurring after 14 d group and the non-LO-NEC group. The 3 groups did not significantly differ in terms of other nutritional factors, such as breast milk volume on addition of human milk fortifier, days for full human milk fortifier (HMF), cumulative dose of amino acids, cumulative dose of SMOF® (soybean oil, medium-chain triglycerides, olive oil, and fish oil) lipid emulsion, and cumulative caloric intake in the first week after birth (P > 0.05; Table 2).
Multivariate logistic regression analysis of the risk factors for LO-NEC in VPIs
Although univariate analysis revealed no significant differences in the incidence of early feeding among 3 groups (P = 0.762), it was still included in the multivariate regression analysis considering its protective effects against NEC [16]. After adjusting for factors that may affect LO-NEC, multivariate analysis showed that high proportion of breastfeeding (aOR: 0.25, 95%CI: 0.10 ~ 0.78; aOR: 0.53, 95%CI: 0.08 ~ 0.89) were identified as protective factors and long fasting time before NEC (aβ: -4.65, 95%CI: -6.02~-2.14; aβ: -3.32, 95%CI: -5.18~-2.07) were identified as risk factors for LO-NEC; early feeding (aOR: 0.42, 95%CI: 0.14 ~ 0.84; aOR: 0.28, 95%CI: 0.19 ~ 0.77) were identified as protective factors and low gestational age (aβ: -1.98, 95%CI: -5.64~-0.45), grade III ~ IV neonatal respiratory distress syndrome (NRDS) (aOR: 3.32, 95%CI: 1.76 ~ 6.45), high accumulation of the MCT/LCT emulsion in the first week (aβ: -3.44, 95%CI: -7.19~-1.16; aβ: -3.59, 95%CI: -6.45~-2.76) were identified as risk factors for LO-NEC occurring between 8 ~ 14d (Table 3).
Multivariate logistic regression analysis of LO-NEC for short-term outcomes in VPIs
Univariate analysis found that the incidence of LOS, MBDP, PNAC, and EUGR was statistically significantly different between the two groups (all P < 0.05; Table 4). After adjusting for confounding factors that may affect the clinical outcomes, multivariate regression analysis showed that the risk of LOS was 1.5 times higher in the LO-NEC group than in the non-LO-NEC group (aOR = 1.527, 95% CI: 1.049 ~ 2.221, P < 0.001), the risk of MBDP was 2.6 times higher in the LO-NEC group than in the non-LO-NEC group (aOR = 2.613, 95% CI: 1.363 ~ 5.008, P = 0.002), the risk of PNAC was 2.3 times higher in the LO-NEC group than in the non-LO-NEC group (aOR = 2.350, 95% CI: 1.616 ~ 3.416, P < 0.001), and the risk of EUGR was 1.6 times higher in the LO-NEC group than in the non-LO-NEC group (aOR = 1.613, 95% CI: 1.114 ~ 2.337, P < 0.001; Table 5).
Discussion
LO-NEC is one of the main causes of death in premature infants one week after birth [17]. The early clinical manifestations and X-ray imaging results of NEC are often nonspecific, and the progress is rapid. By the time its diagnosis is established, the condition is often serious and generally presents with intestinal necrosis and perforation, which require surgical treatment. Many of the survivors present with short bowel syndrome, which can widely be complicated with intestinal stenosis, PNAC, EUGR, and other short-term adverse prognoses and even with neurocognitive dysfunction in the long term. Therefore, the prevention of this disease is the most critical, and to this end, it is necessary to recognize the high-risk factors for NEC early and intervene promptly, which can greatly improve the clinical outcome of premature infants.
At present, LO-NEC is considered to result from multiple factors which are mainly related to an altered intestinal barrier immune response to feeding and the developing microbiome in premature infants; LO-NEC development can also be attributed to hypoxia, hemodynamic instability, and infection [1, 18]. In our study, compared to the non-LO-NEC group, the LO-NEC group had a higher incidence of anemia, although there was no difference after adjustment. Anemia can impair splanchnic perfusion, resulting in tissue hypoxia. Anemia can also impair the normal maturation of vascular autoregulation in the premature intestine, predisposing to ischemic injury, and possibly, NEC [19]. Therefore, the early prevention and treatment of anemia is encouraged in the NICU. Potential means of preventing anemia include delayed cord clamping and methods for limiting phlebotomy losses.
This study confirmed that low GA and grade III ~ IV NRDS were high-risk factors for LO-NEC occurring between 8 ~ 14d. A lower GA with a higher incidence of grade III ~ IV NRDS is associated with intestinal immaturity and vulnerability to various pathological factors, consequently leading to NEC [20]. In VPIs with grade III ~ IV NRDS, immature lungs have damaged gas exchange function and intestinal tissue oxygenation disorder, which lead to NEC. In our study, all grade III-IV NRDS patients have received IMV treatment. Compared to the LO-NEC group occurring after 14 d, higher proportion of grade III ~ IV NRDS and longer IMV duration were found in the LO-NEC group occurring between 8 ~ 14d. It has been hypothesized that indwelling endotracheal tube may compromise the infants’ mucosal barriers increasing the risk of infection [21]. Moreover, variations in intrathoracic pressure during IMV had a major impact and affect systemic venous return, right ventricular preload, left ventricular preload, right ventricular afterload, left ventricular afterload and myocardial contracility, which may affect blood supply to the intestine and consequently increase the risk of NEC [22].
A long fasting time may lead to intestinal mucosal atrophy, intestinal dysfunction, abnormal intestinal flora colonization, and excessive intestinal inflammatory response in premature infants, which are high-risk factors for NEC [23]. Notably, enteral feeding can prevent intestinal atrophy, enhance mucosal adaptability, and stimulate intestinal movement and growth. This study shows that early feeding is a protective factor against LO-NEC occurring between 8 ~ 14d. A prospective randomized controlled trial showed that VPIs given trophic feeding within 24 h of birth had faster body weight growth and that this approach helped prevent NEC [16]. In agreement with previous studies, the present study also confirmed that breastfeeding was a protective factor for LO-NEC. The protective effect of breastfeeding on NEC reportedly has a dose–effect relationship. Lapidaire et al. confirmed that every 10% increase in breast milk intake was associated with a ~ 12% reduction in the incidence of NEC [24]. Miller et al. [25]. also reported a more evident protective effect when the intake of breast milk was ≥ 50% of the total intake. However, the overall breastfeeding ratio in this study was not high because most NICUs in China did not receive breast milk during the COVID-19 pandemic; this may also explain the incidence of LO-NEC being slightly higher in this study (8.4%) than in other studies (7.0%) [2].
The results of this study showed that a higher cumulative dose of the MCT/LCT emulsion in the first week was a risk factor for LO-NEC occurring between 8 ~ 14d; however, the cumulative dose of SMOF did not statistically significantly differ between the two groups. Some investigators have pointed out that the use of lipid emulsion impairs monocyte, lymphocyte, and neutrophil functions, and these changes seemed to be related to the quantity and rate of lipid administration; conversely, the use of n-3 fatty acids (represented by SMOF) produces less immunosuppressive eicosanoids [26]. A major finding of a previous study was that compared to the standard dose of intravenous lipid emulsion (starting from 0.5 g/kg/day−1 and gradually increased by 1 g/kg/day to a maximum of 3.5 g/kg/day), a restricted dose of intravenous lipid emulsion (1 g/kg/day) significantly increased the rate of bacterial clearance in preterm infants with blood stream infections [27]. A significant increase in the levels of n-6 long-chain polyunsaturated fatty acids (LCPUFAs), proinflammatory lipid metabolites, such as arachidonic acid-containing glycerophospholipids, and eicosanoids, such as prostaglandin A2 (PGA2), was observed in the intestinal tissue of NEC pigs [28]. The MCT/LCT emulsion contains a high proportion of ω-6 LCPUFAs (ω-6:ω-3 = 7:1). ω-6 Arachidonic acid (AA), a metabolite of LCPUFA, is a precursor of inflammatory mediators. It can catalyze the formation of PG and TBX via cyclooxygenase, reduce and weaken the phagocytosis of neutrophils, promote oxidative stress injury, increase the production of inflammatory mediators, and damage the vascular endothelial system and immunosuppression [29], thus resulting in an increased risk of NEC. In addition, ω-6 LCPUFAs metabolize to produce a strong vasoconstrictor, TXA2, whereas the vasodilator PGI2 is significantly reduced; these changes constrict the blood vessels and form thrombi in severe cases [25, 29], thus affecting intestinal blood flow and inducing NEC. This study also confirmed that early feeding was a protective factor for LO-NEC occurring between 8 ~ 14d, whereas a long fasting time was a risk factor for LO-NEC. A long fasting time and late feeding of VPIs will inevitably increase the cumulative dose of the MCT/LCT emulsion ingested intravenously in the first week, which may further increase the risk of NEC. Therefore, enteral nutrition should be started as soon as possible to minimize the dosage of the MCT/LCT emulsion in the first week. Notably, giving SMOF lipid emulsion with less ω-6 LCPUFAs may be beneficial to reduce the incidence of LO-NEC. Similarly, regarding nutrition aspects, lower early feeding rate and breastfeeding rate, more MCT/LCT emulsion intake, slower growth velocity were found in the LO-NEC group occurring between 8 ~ 14d when compared to the LO-NEC group occurring after 14 d. These results may suggest that nutrition plays a role in affecting the timing of NEC occurrence, which is worth further exploration.
NEC occurring in VPIs may increase the risk of short-term adverse outcomes. Shah et al. [30]. reported that NEC was associated with an increased risk of ROP, BPD, and PVL. Compared with the non-LO-NEC group, our study found that the incidence of EUGR, LOS, PNAC, and MBDP in the LO-NEC group was 1.6, 1.5, 2.4, and 2.6 times higher, respectively. A foreign study has pointed out that more than half of NEC premature infants have EUGR [31]. A recent domestic study also confirmed that the risk of development of EUGR was 5 times higher in very low-birth-weight infants with confirmed NEC, regardless of whether it was treated surgically [32]. The reasons were considered to be related to delayed feeding, longer fasting time, slower GV, longer time to regain BW, longer time to reach total enteral nutrition, and longer time to reach a total caloric intake of 110 kcal/kg/d in the LO-NEC group. Less nutrient intake and malabsorption caused by short bowel syndrome or intestinal stenosis after intestinal resection also increase the incidence of EUGR [33]. Due to NEC, the parenteral nutrition (PN) time is prolonged with decreased intestinal peristalsis, which may lead to intestinal flora translocation through the damaged intestinal wall, causing bacteria and toxins to invade, which leads to an increased risk of LOS. In addition, endotoxin invades the portal venous system, leading to the activation of liver Kupffer cells in the early stage, which results in hepatocyte damage and cholestasis [34]. A study using a mouse model found that when there was intestinal injury and the PN time was prolonged, which lead to hepatocyte injury and PNAC occurrence, neither the intestinal injury nor the PN prolongation alone was sufficient to trigger the above results, suggesting that the combined effect of intestinal injury and PN prolongation led to the occurrence of PNAC [35]. NEC and PNAC in premature infants delayed establishment of enteral nutrition, and a PN time of > 4 weeks are reportedly high-risk factors for MBDP [36].
This study had several limitations. First, this study lacks information regarding some important aspects, such as chorioamnionitis during pregnancy, delayed cord clamping, hypoxic events, impaired placental function, and the use of probiotics. These confounding factors may have influenced the clinical outcomes. Second, the data presented here come from a prospective multicenter study on factors influencing VPIs-EUGR in China, which excluded patients who died at the initial stage and during hospitalization. Therefore, the effect of NEC on death as a clinical outcome was not studied. Finally, nutrition management strategies of each center are slightly different, particularly enteral nutrition, and therefore, the research results may be biased.
Conclusion
The results of this study showed that long fasting time, high cumulative dose of the MCT/LCT emulsion in the first week, and low GA with grade III–IV NRDS were the risk factors for LO-NEC in VPIs, especially those occurring between 8 ~ 14d; conversely, early feeding and breastfeeding were protective factors. Therefore, it is necessary to actively prevent premature birth, standardize the treatment of grade III ~ IV NRDS and optimize enteral and PN strategies, which may help reduce the incidence of LO-NEC and may further reduce the risk of clinical adverse outcomes, such as EUGR, LOS, PNAC, and MBDP.
Availability of data and materials
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- NEC:
-
Necrotizing enterocolitis
- EO-NEC:
-
Early-onset NEC
- LO-NEC:
-
Late-onset NEC
- VPIs:
-
Very preterm infants
- MCT/LCT:
-
Medium-chain and long-chain triglyceride
- NRDS:
-
Neonatal respiratory distress syndrome
- NICUs:
-
Neonatal intensive care units
- EUGR:
-
Extrauterine growth restriction
- GA:
-
Gestational age
- BW:
-
Birth weight
- GV:
-
Growth velocity
- IVH:
-
Intraventricular hemorrhage
- PVL:
-
Periventricular leukomalacia
- BPD:
-
Bronchopulmonary dysplasia
- PNAC:
-
Parenteral nutrition-associated cholestasis
- ROP:
-
Retinopathy of prematurity
- hsPDA:
-
Hemodynamically significant patent ductus arteriosus
- EOS:
-
Early-onset sepsis
- LOS:
-
Late-onset sepsis
- PMA:
-
Postmenstrual age
- NRDS:
-
Neonatal respiratory distress syndrome
- MBDP:
-
Metabolic bone disease of prematurity
- SGA:
-
Small for gestational age
- HMF:
-
Human milk fortifier
- SMOF:
-
Soybean oil, medium-chain triglycerides, olive oil, and fish oil
- LCPUFAs:
-
Long-chain polyunsaturated fatty acids
- PGA2:
-
Prostaglandin A2
- AA:
-
Arachidonic acid
- PG:
-
Prostaglandin
- TBX:
-
Thromboxane
- TXA2:
-
Thromboxane A2
- PGI2:
-
Prostaglandin-I-2
- PN:
-
Parenteral nutrition
- HDCP:
-
Hypertensive disorder complicating pregnancy
- IMV:
-
Invasive mechanical ventilation
References
Jones IH, Hall NJ. Contemporary outcomes for infants with necrotizing enterocolitis - a systematic review. J Pediatr. 2020;220:86–92e3.
Neu J, Walker WA. Necrotizing enterocolitis. N Engl J Med. 2011;364:255–64.
Cao Y, Jiang S, Sun J, Hei M, Wang L, Zhang H, et al. Assessment of neonatal Intensive Care Unit practices, Morbidity, and Mortality among very Preterm infants in China. JAMA Netw Open. 2021;4:e2118904.
Samuels N, van de Graaf RA, de Jonge RCJ, Reiss IKM, Vermeulen MJ. Risk factors for necrotizing enterocolitis in neonates: a systematic review of prognostic studies. BMC Pediatr. 2017;17:1–9.
Short SS, Papillon S, Berel D, Ford HR, Frykman PK, Kawaguchi A. Late onset of necrotizing enterocolitis in the full-term infant is associated with increased mortality: results from a two-center analysis. J Pediatr Surg. 2014;49:950–3.
Yee WH, Soraisham AS, Shah VS, Aziz K, Yoon W, Lee SK, et al. Incidence and timing of presentation of necrotizing enterocolitis in preterm infants. Pediatr. 2012;129:e298–304.
Bell MJ, Ternberg JL, Feigin RD, Keating JP, Marshall R, Barton L, et al. Neonatal necrotizing enterocolitis. Therapeutic decisions based upon clinical staging. Ann Surg. 1978;187:1–7.
Patel AL, Engstrom JL, Meier PP, Kimura RE. Accuracy of methods for calculating postnatal growth velocity for extremely low birth weight infants. Pediatrics. 2005;116:1466–73.
Jain A, Shah PS. Diagnosis, evaluation, and management of patent ductus arteriosus in preterm neonates. JAMA Pediatr. 2015;169:863–72.
Subspecialty Group of Neonatology, the Society of Pediatric, Chinese Medical Association. Professional Committee of Infectious Diseases, Neonatology Society, Chinese Medical Doctor Association. Expert consensus on the diagnosis and management of neonatal sepsis (version 2019). Chin J Pediatr. 2019;57:252–7.
Fenton TR, Kim JH. A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatr. 2013;13:59.
Jobe AH. Bancalari E.Bronchopulmonary dysplasia.Am. J Respir Crit Care Med. 2001;163:1723–9.
Papile LA, Burstein J, Burstein R, Koffler H. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm. J Pediatr. 1978;92:529–34.
Chiang MF, Quinn GE, Fielder AR, Ostmo SR, Paul Chan RV, Berrocal A, et al. International classification of retinopathy of Prematurity, Third Edition. Ophthalmology. 2021;128:e51–68.
Shao XM, Ye HM, Qiu XS. Practice of neonatology. 5th ed. Beijing: People’s Medical Publishing House; 2018. p.368,380,510,575,632,855,860,951,1025.
Bozkurt O, Alyamac Dizdar E, Bidev D, Sari FN, Uras N, Oguz SS. Prolonged minimal enteral nutrition versus early feeding advancements in preterm infants with birth weight < = 1250 g: a prospective randomized trial. J Matern Fetal Neonatal Med. 2022;35:341–7.
Patel RM, Kandefer S, Walsh MC, Bell EF, Carlo WA, Laptook AR. Causes and timing of death in extremely premature infants from 2000 through 2011. N Engl J Med. 2015;372:331–40.
Flahive C, Schlegel A, Mezoff EA. Necrotizing enterocolitis: updates on morbidity and mortality outcomes. J Pediatr. 2020;220:7–9.
Maheshwari A, Patel RM, Christensen RD. Anemia, red blood cell transfusions, and necrotizing enterocolitis. Semin Pediatr Surg. 2018;27:47–51.
McPherson C, Wambach JA. Prevention and treatment of respiratory distress syndrome in Preterm neonates. Neonatal Netw. 2018;37:169–77.
Gitau K, Ochieng R, Limbe M, Kathomi C, Orwa J. The incidence and modifiable risk factors for necrotizing enterocolitis in preterm infants: a retrospective cohort study. J Matern Fetal Neonatal Med. 2023;36:2253351.
Lamia B, Molano LC, Muir JF, Cuvelier A. Cardiopulmonary interactions in the course of mechanical ventilation. Rev Mal Respir. 2016;33:865–76.
Patwardhan G, Soni A, Rachwani N, Kadam S, Patole S, Pandit A. Factors Associated with Time to full feeds in Preterm very low Birth Weight infants. J Trop Pediatr. 2018;64:495–500.
Lapidaire W, Lucas A, Clayden JD, Clark C, Fewtrell MS. Human milk feeding and cognitive outcome in preterm infants: the role of infection and NEC reduction. Pediatr Res. 2022;5:1207–14.
Miller J, Tonkin E, Damarell RA, McPhee AJ, Suganuma M, Suganuma H, et al. A systematic review and meta-analysis of human milk feeding and morbidity in very low birth weight infants. Nutrients. 2018;10(6):707.
Garnacho Montero J, Shou J, Ortiz Leyba C, Jiménez Jiménez FJ, Daly JM. Lipids and immune function. Nutr Hosp. 1996;11:230–7.
Shouman B, Abdel-Hady H, Badr RI, Hammad E, Salama MF. Dose of intravenous lipids and rate of bacterial clearance in preterm infants with blood stream infections. Eur J Pediatr. 2012;171:811–6.
Yakah W, Singh P, Brown J, Stoll B, Burrin D, Premkumar MH, et al. Parenteral lipid emulsions induce unique ileal fatty acid and metabolomic profiles but do not increase the risk of necrotizing enterocolitis in preterm pigs. Am J Physiol Gastrointest Liver Physiol. 2021;320:G227–239.
Innes JK, Calder PC. Omega-6 fatty acids and inflammation. Prostaglandins Leukot Essent Fat Acids. 2018;132:41–8.
Shah J, Singhal N, Da Silva O, Rouvinez-Bouali N, Seshia M, Lee SK, et al. Intestinal perforation in very preterm neonates: risk factors and outcomes. J Perinatol. 2015;35:595–600.
Chin LK, Doan J, Teoh YS, Stewart A, Forrest P, Simm PJ. Outcomes of standardised approach to metabolic bone disease of prematurity. J Paediatr Child Health. 2018;54:665–70.
Multicenter Study Collaborative Group for Evaluation of Outcomes in Very Low Birth Weight Infants. Risk factors for extrauterine growth retardation in very low birth weight infants: a multicenter study. Chin J Pediatr. 2020;58:653–60.
Hong CR, Fullerton BS, Mercier CE, Morrow KA, Edwards EM, Ferrelli KR, et al. Growth morbidity in extremely low birth weight survivors of necrotizing enterocolitis at discharge and two⁃year follow⁃up. J Pediatr Surg. 2018;53:1197–202.
Raba AA, O’Sullivan A, Semberova J, Martin A, Miletin J. Are antibiotics a risk factor for the development of necrotizing enterocolitis-case-control retrospective study. Eur J Pediatr. 2019;178:923–8.
El Kasmi KC, Anderson AL, Devereaux MW, Fillon SA, Harris JK, Lovell MA, et al. Toll-like receptor 4-dependent Kupffer cell activation and liver injury in a novel mouse model of parenteral nutrition and intestinal injury. Hepatology (Baltimore, Md). 2012;55:1518–28.
Faienza MF, D’Amato E, Natale MP, Grano M, Chiarito M, Brunetti G, et al. Metabolic bone disease of Prematurity: diagnosis and management. Front Pead. 2019;7:143.
Acknowledgements
We would like to thank all participants of the Chinese Multicenter EUGR Collaborative Group, which consisted of: Department of Neonatology, Women and Children’s Hospital, School of Medicine, Xiamen University, Xiamen, Fujian, China (Kun Yao Hong, Yao Zhu, Wei Shen, Li-Xia Tang, Zhi Zheng, and Xin-Zhu Lin); Department of Neonatology, The Third Affiliated Hospital of Guangzhou Medical University, Guangzhou, Guangdong, China (Fan Wu, Qian-Xin Tian, and Qi-Liang Cui); Department of Pediatrics, Shengjing Hospital of China Medical University, Shenyang, Liaoning, China (Jian Mao, Yuan Yuan, and Ling Ren); Department of Neonatology, Guiyang Maternity and Child Health Hospital/Guiyang Children’s Hospital, Guiyang, Guizhou, China (Ling Liu, Bi-Zhen Shi and Yu-Mei Wang); Department of Pediatrics, Peking University Third Hospital, Beijing, China (Yan-Mei Chang, Jing-Hui Zhang, and Xiao-Mei Tong); Department of Neonatology, Children’s Hospital of Fudan University, Shanghai, China (Rong Zhang, Yan Zhu); Department of Neonatology, Maternal and Child Hospital of Guangdong Province, Guangzhou, Guangdong, China (Xiu-Zhen Ye, Jing-Jing Zou); Department of Neonatology, General Hospital of Ningxia Medical University, Yinchuan, Ningxia, China (Yin-Ping Qiu, Yu-Huai Li, and Bao-Yin Zhao); Department of Neonatology, Children’s Hospital of Hebei Province, Shijiazhuang, Hebei, China (Shu-Hua Liu and Li Ma); Department of Neonatology, Children’ Hospital of Nanjing Medical University, Nanjing, Jiangsu, China (Ying Xu and Rui Cheng); Department of Neonatology, The First Hospital of Jilin University, Changchun, Jilin, China (Wen-Li Zhou and Hui Wu); Department of Neonatology, Quanzhou Maternity and Children’s Hospital, Quanzhou, Fujian, China (Zhi-Yong Liu and Dong-Mei Chen); Department of Pediatrics, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, China (Jin-Zhi Gao, Jing Liu, and Ling Chen); Department of Neonatology, Liaocheng People’s Hospital, Liaocheng, Shandong, China (Cong Li, Chun-Yan Yang, and Ping Xu); Department of Neonatology, the Affiliate Hospital of Inner Mongolia Medical University, Hohhot, Inner Mongolia, China (Ya-Yu Zhang, Si-Le Hu, and Hua Mei); Department of Neonatology, Suzhou Municipal Hospital, Suzhou, Jiangsu, China (Zu-Ming Yang, Zong-Tai Feng, and San-Nan Wang); Department of Neonatology, The Third Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, China (Er-Yan Meng, Li-Hong Shang, and Fa-Lin Xu); Department of Neonatology, Chengdu Women’ and Children’s Central Hospital, School of Medicine, University of Electronic Science and Technology of China, Chengdu, Sichuan, China (Shaoping Ouand Rong Ju); Department of Neonatology, Hunan Children’s Hospital, Changsha, Hunan, China (Gui-Nan Li and Juan Yi); Department of Neonatology, People’s Hospital of Xinjiang Uygur Autonomous Region, Urumqi, Xinjiang, China (Long Li and Yong-Qiao Liu); Department of Neonatology, Guangzhou Women and Children’s Medical Center, Guangzhou, Guangdong, China (Zhe Zhang and Mei-Gui Wu); Department of Neonatology, Shanghai Children’s Medical Center, Shanghai, China (Fei Bei and Ye Liu); Department of Neonatology, Children’s Hospital of Chongqing Medical University, Chongqing, China (Chun Deng and Hui-Jie Yang); Department of Neonatology, The First People’s Hospital of Yulin, Yulin, Guangxi, China (Ping Suand Shi-Feng Chen); Department of Neonatology, the People’s Hospital of Baoji, Baoji, Shanxi, China (Ling-Ying Luo and Lin-Lin Wang); Department of Pediatrics, Affiliated Hospital of Qingdao University, Qingdao, Shandong, China (Xiao-Hong Liu and Li-Hua Yan); Departments of Neonatology, Shandong Provincial Hospital Affiliated to Shandong First Medical University, Jinan, Shandong, China (Li-Jun Wang and Xiao-Kang Wang); and Departments of Neonatology, Xi’an Children’s Hospital, Xi’an, Shanxi, China (Shu-Qun Yu and Qiao-Mian Zhu). This study was also supported by Project of Clinical key specialty of Fujian Province (Specialty in neonatology).
Funding
This study was supported by Guidance Project of Xiamen Medical and Health in 2019 (3502Z20199077) and Guidance Project of Xiamen Medical and Health in 2021 (3502Z20214ZD1225).
Author information
Authors and Affiliations
Consortia
Contributions
XZL,XMT, and KYH conceptualized and designed the study. KYH,YZ,FW,JM,LL,RZ,YMC,WS,LXT,XZY,YPQ,LM,RC,HW,DMC,LC,PX,HM,SNW,FLX,RJ,ZZ, and the other consortium members (the Chinese Multicenter EUGR Collaborative Group) carried out the clinical data collection. KYH,YZ,FW,JM,LL, and RZ analyzed and interpreted the clinical data. KYH and YZ wrote the first draft of this manuscript. XZL,XMT, and KYH reviewed and revised the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The research protocol was approved by the Ethics Committee of Women and Children’s Hospital affiliated to Xiamen University/Xiamen Maternal and Child Health Hospital (Batch number KY-2019-016). All procedures performed in studies involving human participants were in accordance with the ethics standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethics standards. The parents of all study participants provided written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hong, KY., Zhu, Y., Wu, F. et al. The role of nutrition in analysis of risk factors and short-term outcomes for late-onset necrotizing enterocolitis among very preterm infants: a nationwide, multicenter study in China. BMC Pediatr 24, 172 (2024). https://doi.org/10.1186/s12887-024-04611-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-024-04611-7