
Abstract
Backgrounds
The Autism spectrum disorder (ASD) prevalence has increased significantly over the past two decades. This review summarizes the current knowledge of the association between the early life growth of head circumference (HC), weight, and height with ASD in infants.
Methods
PubMed, Scopus, Science Direct, and Google Scholar databases were searched up to November 2021 using relevant keywords. All original articles are written in English evaluating the early life growth of HC, weight, and height in infants with ASD were eligible for the present review.
Results
Totally, 23 articles involving 4959 infants were included in this review. Of 13 studies that evaluated HC of infants at birth, 10 studies (83.33%) showed that the HC at the birth of autistic children was similar to that of the average found in the control group. Among 21 studies that evaluated the HC and weight status in infants, 19 studies (90.47%) showed that autistic children had larger HC and weight than the control group or abnormal acceleration of head growth during infancy. Height growth of infants was investigated in 13 studies, of which 10 cases (76.92%) reported that infants with ASD were significantly longer than control groups. Most of he included studies had a good quality.
Conclusions
The findings suggest that in infants with ASD, without the contribution of birth growth factors and sex of the child, the growth of HC, weight, and height probably was faster than in infants with normal development, in early life. Therefore, these measurements might be useful as initial predictive biomarkers for the risk of developing ASD.
Similar content being viewed by others

Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental condition influencing one in 59 children in the world. Along with behavior problems, ASD is accompanied with sleep complications, seizures, gastrointestinal difficulties, and mental health concerns that can intensely affect the quality of life of children and their families [1]. Intellectual disability or low verbal ability were also reported in around one-third of children with ASD [1]. Timely identification of developmental disorders is vital to the well-being of children. American Academy of Pediatrics (AAP) suggests that developmental surveillance and standardized screening tests be considered for ASD at 18 and 24 months of age, at every health supervision visit [2].
The precise cause of ASD is mostly unknown [3]. According to evidence, multiple risk factors including genetic, environmental, immunological, and perinatal factors may contribute to the ASD pathogenesis [3,4,5,6]. On the other hand, both genetics and environmental factors early in development have role in the etiology of autism [7]. However, some of the evidence supporting a significant contribution of environmental factors to autism risk [6]. Features of autism may be detected in early childhood, but the diagnosis of autism is usually not made until much later [5]. Recently, ASD detection strategies focus on early risk markers and growth abnormalities during the early years of life have often been paid attention, to in this direction [8,9,10].
Growth assessments and standard growth patterns are the gold standard diagnostic tests by which clinicians evaluate the health and physical and emotional well-being of a child. Height, weight, and head circumference (HC) are the main components of anthropometry for infants and toddlers less than two years of age [11]. Reliable sequential anthropometric assessments can help recognize underlying medical, nutritional, or social problems in infants and children [12].
Poor growth during infancy or childhood may contribute to adverse health outcomes in adults [13, 14], hence prevention of growth retardation at these periods of life may have both short- and long-term health advantages [15, 16]. On contrary, several observational investigations have indicated that early life (under two years) accelerated or too fast growth may adversely contribute to long-term health outcomes such as increasing the risk of obesity and chronic diseases [17,18,19]. In preterm infants, the growth acceleration may be beneficial for later neurodevelopment [17], but it may affect contradictory in healthy term infants. Recently, infancy growth accelerated has become a major focus of research.
Increased body growth, including weight and height, during infancy, has been suggested as a feature of ASD by several studies [9, 20]. In addition, macrocephaly and abnormal acceleration in head growth during the early stages of postnatal development have been proposed as a discerning feature of ASD, by some other investigations [21, 22]. However, the findings were inconsistent across the studies and it is not yet definitively known whether accelerated HC and body growth during infancy are associated with ASD incidents. Moreover, most studies have focused on the physical growth in older children and adolescents with ASD. Best to our knowledge, there is no comprehensive study to review systematically the association between early life growth of HC, weight, and height with ASD incidents in infants. Therefore, the present study was performed to summarize the existing literature regarding the association between early life growth of HC, weight, and height with ASD incidents in infants.
Methods
The protocol of this study was approved and registered by the Research Vice-Chancellor of Tabriz University of Medical Sciences (ethical code: IR.TBZMED.REC.1400.1243).
Search strategy
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Supplementary Table 1) [23]. Electronic databases of PubMed, ScienceDirect, Scopus, and Google Scholar were searched without date restrictions until November 2021, using the following keywords: “weight OR height OR length OR head circumference OR growth OR nutritional status” AND “early life OR first year of life OR early growth” AND “autism spectrum disorders OR ASD OR autism OR autistic” AND “children OR infants OR infancy”. We defined the early life as the first 2 years of life. Moreover, to ensure the inclusion of all eligible studies, a separate search was conducted through Google, and also the reference lists of the included studies were reviewed. The search strategy is shown in Supplementary Table 2.
Articles screening and selection criteria
The extracted studies were saved in an EndNote software and duplicate studies were removed. To identify studies with the correct scope for the current review, the remaining articles were screened in two stages by two independent reviewers (SK and RMG). At first, the titles and abstracts of all the articles were checked. Then, full-text of the remained articles was scrutinized to ensure the suitability of the study for inclusion in this review. Finally, original English-language articles that meted the eligibility criteria were selected. All clinical and observational studies that addressed the early life (ages < 2 years) growth of HC, weight, and height in infants with ASD were eligible for inclusion in this study. Reviews, abstracts, conference papers, editorials, book chapters, posters, letters, thesis, animal, and generic studies were not included. Studies that measured the association between prenatal head growth that was estimated by sonography and postnatal autistic traits were excluded. Studies that measured the association of growth factors and autistic traits in ages > 2 years were excluded. Articles that studied other autistic traits (e.g., oral motor coordination and muscle tone) in early life (case study) and used patients with two or more neurodevelopmental disorders were also excluded. Then, the full texts of the screened articles were critically and separately analyzed for eligibility.
Data extraction
The extracted data from the eligible studies were following: the authors’ name; year of publication; study design and location; the number of participants; mean age and gender of participants; mean HC, weight, and height at birth; percent of macrocephaly; findings concerning the early life growth of HC, weight, and height in infants with ASD.
Articles quality assessment
The assessment of each included study quality was done using the Newcastle-Ottawa scales [24]. Assessment is based on three sections of the comparability, selection, and the exposure or outcome of the groups. The adopted Newcastle-Ottawa scale score for cross-sectional studies is maximum of 10 points and if the overall score was within 7 to 10 points, the study has good quality [24, 25]. The Newcastle-Ottawa scale score is maximum of 9 points for case-control studies and if the overall score was within 6 to 9 points, the study has good quality [24, 26].
Results
Study selection
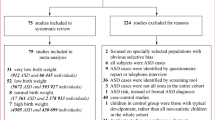
The process of search and study selection (PRISMA diagram) of this systematic review is showed in Fig. 1. Totally, 504 potential articles were retrieved through searching of PubMed (n = 79), Google Scholar (n = 601), Scopus (n = 93) and ScienceDirect (n = 51) databases. Following the elimination of duplicate articles, 473 studies remained for additional screening. Of these, 442 studies were excluded in the first stage of screening based on the title and abstract of the articles. During critical analysis, 31 articles were screened of which 8 articles were excluded because of non-availability of full text (n = 1), being out of the studied life stage (fetal period) (n = 1) [27], studying autism in combination with Fragile X Syndrome (n = 1) [28], were at ages > 2 years (n = 2) [29, 30], did not measure growth factors during the first year (n = 1) [31], were on high-risk children for ASD (siblings of a child with ASD) (n = 1) [32], and were unrelated (n = 1). Finally, 23 articles were included in the current systematic review.

PRISMA diagram for the process of the search and study selection
Quality of articles
As presented in Supplementary Tables 3 and 4, the quality of each included study was assessed using the Newcastle-Ottawa scales for cross-sectional and case-control studies resulting in the mean scores of 7.6 and 7.5, respectively (Supplementary Tables 3 and 4). These findings indicated that the included studies had a good quality. The most of studies had enough sample sizes and represented infants of the wider community thus scoring well in the selection domain. Scores about the comparability domain were relatively good due to all of the reviewed studies did not adjust all potentially important confounders.
Characterizes of the included studies
The main characteristics of the included studies are shown in Table 1. Of 23 included studies, 16 studies had a retrospective design that used medical records, and 7 studies were conducted prospectively. Both genders had been included in 19 studies, but in 4 cases, it had only been restricted to males. A total of 4959 autistic children were included in this study.
Relationship between early life HC growth with ASD
In all, 21 studies assessed the status of HC growth in ASD infants that of which 13 cases reported information regarding HC in children at birth. 83.33% of the studies (10 of 13) showed that the HC at the birth of autistic children was similar to that of the average found in the control group, two cases indicated smaller HC, and one study reported a larger HC in ASD infants than in control groups. Among 21 studies that evaluated the HC status in infants, 19 studies (90.47%) showed that autistic children had larger HC or abnormal acceleration of HC growth than the control group. In 12 cases of the included studies, the percent of macrocephaly (HC > 97th percentile or HC > 2 standard deviations (SD)) in ASD infants ranged from 1.2 to 53% that these results were consistent with standard macrocephaly rates according to CDC norms and only in two studies were more than standard values. Nineteen studies were conducted on both sexes, of which 14 studies (73.68%) reported similar results between males and females, and three studies showed greater mean HC in males than females.
Relationship between early life weight gain with ASD
Six studies reported data about the birth weight of ASD infants, of which five cases showed no significant difference between ASD and typically developed infants. One study revealed that the birth weight of autistic infants was lower than that in the control group. Twenty-one studies assessed the weight status of children during the infancy period, of which 19 cases (90.47%) demonstrated that weight growth was significantly greater in ASD groups compared with controls. Of studies conducted on both genders (n = 19), all of them reported similar findings in males and females, only one case indicated higher weight gain in boys rather than in girls, during infancy.
Relationship between early life length growth with ASD
Regarding height at birth, five studies indicated a similar height in ASD and control infants. Thirteen studies investigated the height growth of children during the infancy period, of which 10 cases (76.92%) reported that infants with ASD were significantly longer than control groups. Among studies that included both genders, one case indicated larger height in boys rather than in girls, and the other remaining reported similar results in both sexes.
Discussion
The findings of the present study showed that rapid growth of weight, height, and HC during infancy was associated with an enhanced risk of ASD developing. The previous research also emphasis the importance of assessing neonatal anthropometric measures such as weight and HC growth [33,34,35]. Some studies confirm the validity of HC growth as a potential biomarker of normal and abnormal early child development [35, 36]. Recently, it has been reported that an abnormality in factors such as hormone levels, metabolism, and growth or neurotrophic factors may predispose a subject to overall acceleration of growth as well as ASD [22, 36, 37]. Neurotrophins abnormalities, which regulate the metabolism of glucose, may cause accelerated growth in HC and body size [38] and also improve neuronal growth and survival [39]. Liu et al. [40] performed a comprehensive systematic review on the changes in peripheral neurotrophic factors in autistic children and revealed strong evidence that the levels of brain-derived neurotrophic factor (BDNF), nerve growth factor (NGF), and vascular endothelial growth factor (VEGF) in peripheral blood of autistic children were higher than those in healthy controls, establishment the evidence that neurotrophic factors play critical roles in ASD onset and/or development. However, they found no significant associations between neurotrophin-3 (NT-3) or neurotrophin-4 (NT-4) and ASD [40]. It has been reported that overgrowth of the brain volume in early ASD children is largely due to the augmented proliferation of neural progenitor cells [43]. Neurotrophic factors have a positive role in the embryonic neural progenitor cells proliferation [42]. Importantly, the BDNF level is temporally regulated during development that has been shown to be required for the proper development and functions of neuronal [43]. Therefore, it is likely that in the early life of ASD children, abnormal regulation of BDNF cause the subsequent long-term changes in structure and function of the brain, such as accelerating its growth. BDNF has also similar effects in other psychiatric disorders [44].
According to the previous evidence, abnormal secretion of some hormones, such as adiponectin, leptin, ghrelin, insulin, and IGF-1 may cause changes in the growth process, especially in early life, and may be associated with the risk of autism [45,46,47,48,49,50]. Adipokines, cytokines secreted mostly by adipose tissue, may have a widespread effect and function on brain health [51]. Rodrigues et al. found significant changes in the adipokines plasma levels in ASD patients [52]. Many adipokines such as interleukin-8 [53], interleukin-6 (IL-6) [54], IL-10 [55], leptin [56], tumor necrosis factor-alpha (TNF-α) [57], omentin [58], resistin, and adiponectin [59] have been shown to be associated with ASD. Adiponectin is an adipocyte-derived circulating protein that based on recent evidence may have a role in the pathophysiology of autism [60]. Fujita-Shimizu et al. indicated that the serum levels of adiponectin were significantly lower in the individuals with autism than in normal subjects [61]. However, the role of adiponectin on the early life growth of autistic infants is not clear.
Leptin is another hormone whose abnormality in its release may be contributed to the association between rapid growth and ASD. Recent works found elevated plasma leptin levels in children with autism compared to typically developing controls [52, 62, 63]. There are some reasons for the involvement of leptin in the neuropathology of ASD. Leptin can cross the blood-brain barrier through active transport [64]. Moreover, it has been reported that proinflammatory cytokines can mediate the rapid postnatal growth of ASD [65]. Raghavan et al. indicated the mediating effect of leptin in extremely rapid weight gain during infancy in ASD children [56]. Although they did not analyze HC, weight is the strongest predictor of HC during most of the infancy [22]. In agreement with this, animal models showed that rapid catch-up growth in early childhood is connected with leptin resistance [66]. Beyond leptin’s role in weight gain of postnatal, this pleiotropic cytokine has an essential function in the neurodevelopment regulation of including neural differentiation, promoting migration of neuronal lineage cells to the cortical plate, synaptic plasticity, and neuron excitability, [62, 63, 67].
It is well known that ghrelin has a significant role in the growth and development of infants [68,69,70]. Al-Zaid et al. showed that the plasma levels of ghrelin were significantly decreased in the autism group compared with healthy controls and revealed also a significant negative association between ghrelin and HC [50]. It is intriguing the fact that autistic children despite low ghrelin levels have increased weight; this could be suggesting a drastic disturbance in the central processing of these peripheral signals. The involvement of many other hormones which may have functions in body weight management is another possible explanation [50].
Insulin-like growth factor-1 (IGF-1) is a neurotrophin that regulates somatic growth and metabolism and myelination and brain growth [71]. Lower plasma IGF-1 and growth hormone-binding protein (GHBP) was observed in autistic children [46], and IGF-1 levels were positively correlated with HC [46]. Li et al. also demonstrated that the ASD group had a significantly lower serum level of IGF- 1 and IGFBP (IGF binding protein)-3 than the control group [72]. The beneficial effects of IGF-1 for treating ASD are due to the potent effects of IGF-1 on synaptic maintenance, function, and plasticity. Based on these findings, the reduction in serum IGF-1 levels in early childhood may be associated with the development of ASD, but the mechanism of the association between decreased IGF-1 levels and increased HC, weight, and height in infants with autism has not yet been elucidated. Abnormal regulation of some hormones such as BDNF, IGF-1, leptin, and ghrelin may be associated with the accelerated growth of infants. However, genes related to head circumference and behavioral development, such as PTEN, might have a role in ASD [73,74,75]. Fu et al. revealed that some of the PTEN variant and ASD genetic background affected genes involved in neurogenesis, neural development, and synapse signaling and contribute to cellular features consistent with ASD associated with macrocephaly [74]. Moreover, mutations in the regulator genes of mTORC1 result in ASD-like phenotypes through the disruption of the mTORC1-mediated signaling [75].
Macrocephaly is one of the most common physical findings was achieved in autistic individuals [76]. Reported rates of macrocephaly in autistic children vary, with an average rate of 20%. However, 83.3% of the studies included in this review showed that autistic children at or shortly after birth usually did not have macrocephaly and had a similar HC percentile distribution as the general population. Therefore, an abnormal acceleration in head growth during the earliest stages of postnatal development, independent of macrocephaly, may be a risk factor related with the development of ASD [21].
Timely evaluation and early detection of ASD among young children should be an important public health goal [77] because evidence showed that early treatment and services for ASD links with improved outcomes [40, 78, 79]. It should be considered that the findings were obtained from the studies with various follow-up times and different time points for assessing growth and outcomes and were concluded from retrospective and prospective data. Moreover, racial difference between the infants may be have a role in these findings. Nevertheless, early life assessment of anthropometric measures is suggested.
Limitation of the study
Since growth factors had been measured at various time points of infancy across the studies, we were not able to carry out a meta-analysis. Moreover, the majority of the included studies not reported the criteria that were used for the diagnosis of the ASD infants. The sample sizes of the included studies also were low so, generalizing it to all ASD populations should be done with caution. Some environmental factors such as socioeconomic status of ASD infants’ families may contributed to growth and developmental changes in ASD children. However, this issue has not been considered in the included studies in this review.
Conclusions
More than 91% of the studies included in this systematic review revealed that rapid growth of HC, weight, or height during infancy probably was associated with the risk of ASD. Therefore, these measurements might be helpful as initial predictive biomarkers for the risk of developing ASD. In addition, these measurements may be a useful and cost-effective method in helping to diagnose the risk of ASD in situations where there isn’t access to magnetic resonance imaging technology. However, these measures are not replaceable with aspects that neuroimaging exams can achieve. Long-term prospective cohort studies are required to determine the association between accelerated growth in the early life and ASD risk.
Data Availability
Data are available from the corresponding author upon reasonable request.
References
Practice Guidelines; Autism Spectrum Disorder. Updated guidelines from the American Academy of Pediatrics. Am Fam Physician. 2020;102(9):629–31. https://www.aafp.org/pubs/afp/issues/2020/1115/p629.pdf.
Centers for Disease Control and Prevention. (.gov); Recommendations and Guidelines; Autism Spectrum Disorder (ASD); American Academy of Pediatrics (AAP), January 2020 https://www.cdc.gov/ncbddd/autism/hcp-recommendations.html.
Moore GS, Kneitel AW, Walker CK, Gilbert WM. Xing GJAjoo, gynecology. Autism risk in small-and large-for-gestational-age infants. 2012;206(4):314. e1-. e9.
Limperopoulos CJCip. Autism spectrum disorders in survivors of extreme prematurity. 2009;36(4):791–805.
Wang L, Wang B, Wu C, Wang J, Sun M. Autism spectrum disorder: neurodevelopmental risk factors, Biological mechanism, and Precision Therapy. Int J Mol Sci. 2023;24(3):1819.
Chaste P, Leboyer M. Autism risk factors: genes, environment, and gene-environment interactions. Dialogues in clinical neuroscience. 2022.
Höfer J, Hoffmann F, Kamp-Becker I, Poustka L, Roessner V, Stroth S, Wolff N, Bachmann CJ. Pathways to a diagnosis of autism spectrum disorder in Germany: a survey of parents. Child Adolesc Psychiatry Mental Health. 2019;13(1):1–0.
Campbell DJ, Chang J, Chawarska KJJotAAoC, Psychiatry A. Early generalized overgrowth in autism spectrum disorder: prevalence rates, gender effects, and clinical outcomes. 2014;53(10):1063–73. e5.
Grandgeorge M, Lemonnier E, Jallot NJAP. Autism spectrum disorders: head circumference and body length at birth are both relative. 2013;102(9):901–7.
Schrieken M, Visser J, Oosterling I, van Steijn D, Bons D, Draaisma J et al. Head circumference and height abnormalities in autism revisited: the role of pre-and perinatal risk factors. 2013;22(1):35–43.
Casadei K, Kiel JJS. Anthropometric measurement. 2020.
Gupta PM, Wieck E, Conkle J, Betters KA, Cooley A, Yamasaki S et al. Improving assessment of child growth in a pediatric hospital setting. 2020;20(1):1–10.
Johnson RC. Schoeni RFJTBjoea, policy. The influence of early-life events on human capital, health status, and labor market outcomes over the life course. 2011;11(3).
Adair LS, Fall CH, Osmond C, Stein AD, Martorell R, Ramirez-Zea M et al. Associations of linear growth and relative weight gain during early life with adult health and human capital in countries of low and middle income: findings from five birth cohort studies. 2013;382(9891):525–34.
Singhal AJL-bbbtsots. Should we promote catch-up growth or growth acceleration in low-birthweight infants? 2015;81:51–60.
Barnett WSJTfoc. Long-term effects of early childhood programs on cognitive and school outcomes. 1995:25–50.
Singhal, AJAoN. Metabolism. Long-term adverse effects of early growth acceleration or catch-up growth. 2017;70(3):236–40.
Yim HE, Yoo KHJPN. Early life obesity and chronic Kidney Disease in later life. 2015;30(8):1255–63.
Gluckman PD, Hanson MA, Cooper C, Thornburg KLJNEJM. Effect of in utero and early-life conditions on adult. Health and Disease. 2008;359(1):61–73.
de Vinck-Baroody O, Shui A, Macklin EA, Hyman SL, Leventhal JM, Weitzman CJAP. Overweight and obesity in a sample of children with autism spectrum disorder. 2015;15(4):396–404.
Dementieva YA, Vance DD, Donnelly SL, Elston LA, Wolpert CM, Ravan SA, et al. Accelerated head Growth in Early Development of Individuals with Autism. 2005;32(2):102–8.
Mraz KD, Green J, Dumont-Mathieu T, Makin S, Fein DJJCN. Correlates of head circumference growth in infants later diagnosed with autism spectrum disorders. 2007;22(6):700–13.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. 2009;62(10):e1–e34.
Peterson J, Welch V, Losos M, Tugwell PJOOHRI. The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. 2011;2(1):1–12.
Herzog R, Álvarez-Pasquin M, Díaz C, Del Barrio JL, Estrada JM. Gil ÁJBph. Are healthcare workers’ intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. 2013;13(1):1–17.
Stang AJEjoe. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. 2010;25(9):603–5.
Aydin E, Tsompanidis A, Chaplin D, Hawkes R, Allison C, Hackett G, Austin T, Padaigaitė E, Gabis LV, Sucking J, Holt R. Fetal brain growth and infant autistic traits. medRxiv. 2021 Oct 18:2021–10.
Chiu S, Wegelin JA, Blank J, Jenkins M, Day J, Hessl D, Tassone F, Hagerman R. Early acceleration of head circumference in children with fragile x syndrome and autism. J Dev Behav Pediatr. 2007;28(1):31–5.
de Vinck-Baroody O, Shui A, Macklin EA, Hyman SL, Leventhal JM, Weitzman C. Overweight and obesity in a sample of children with autism spectrum disorder. Acad Pediatr. 2015;15(4):396–404.
Courchesne E, Karns CM, Davis HR, Ziccardi R, Carper RA, Tigue ZD, Chisum HJ, Moses P, Pierce K, Lord C, Lincoln AJ. Unusual brain growth patterns in early life in patients with autistic disorder: an MRI study. Neurology. 2001;57(2):245–54.
Courchesne E, Campbell K, Solso S. Brain growth across the life span in autism: age-specific changes in anatomical pathology. Brain Res. 2011;1380:138–45.
Keehn B, Wagner JB, Tager-Flusberg H, Nelson CA. Functional connectivity in the first year of life in infants at-risk for autism: a preliminary near-infrared spectroscopy study. Front Hum Neurosci. 2013;7:444.
Taylor RW, Haszard JJ, Meredith-Jones KA, Heath AL, Galland BC, Gray AR, Fortune S, Sullivan T, Adebowale T, Taylor BJ. Rapid infant weight gain or point‐in‐time weight status: which is the best predictor of later obesity and body composition?. Obesity. 2023.
Coronado R, Giraldo J, Macaya A, Roig M. Head circumference growth function as a marker of neurological impairment in a cohort of microcephalic infants and children. Neuropediatrics. 2012 Aug;29:271–4.
Dupont C. The Predictive Value of Head Circumference Growth during the First Year of Life on Child Traits in Early Childhood.
Ohta H, Nordahl CW, Iosif AM, Lee A, Rogers S, Amaral DGJA. Increased surface area, but not cortical thickness, in a subset of young boys with autism spectrum disorder. 2016;9(2):232–48.
Chawarska K, Campbell D, Chen L, Shic F, Klin A. Chang JJAogp. Early Generalized Overgrowth in boys with Autism. 2011;68(10):1021–31.
Nockher WA, Renz HJCCA. Neurotrophins in clinical diagnostics: pathophysiology and laboratory investigation. 2005;352(1–2):49–74.
Rogers SJ, Estes A, Lord C, Munson J, Rocha M, Winter J et al. A multisite randomized controlled two-phase trial of the early start Denver Model compared to treatment as usual. 2019;58(9):853–65.
Liu S-H, Shi X-J, Fan F-C, Cheng YJS. Peripheral blood neurotrophic factor levels in children with autism spectrum disorder: a meta-analysis. 2021;11(1):1–9.
Piven J, Elison JT, Zylka MJJMP. Toward a conceptual framework for early brain and behavior development in autism. 2017;22(10):1385–94.
Numakawa T, Odaka H, Adachi NJI. Actions of brain-derived neurotrophic factor and glucocorticoid stress in neurogenesis. 2017;18(11):2312.
Mori T, Shimizu K, Hayashi MJN. Differential expression patterns of TrkB ligands in the macaque monkey brain. 2004;15(16):2507–11.
Shi XJ, Du Y, Li XS, Yao CQ, Cheng Y. Effects of brain-derived neurotrophic factor (BDNF) on the Schizophrenia model of animals. J Psychiatr Res. 2022;156:538–46.
Quan L, Zhao Y, Yi J, Shi X-D, Zhong Y, Liu LJMBD. Serum adiponectin levels are reduced in autism spectrum disorder and association with severity of symptoms. 2021;36(3):491–8.
Vanhala R, Turpeinen U, Riikonen RJDM, Neurology C. Low levels of insulin-like growth factor-I in cerebrospinal fluid in children with autism. 2001;43(9):614–6.
Mills JL, Hediger ML, Molloy CA, Chrousos GP, Manning-Courtney P, Yu KF et al. Elevated levels of growth‐related hormones in autism and autism spectrum disorder. 2007;67(2):230–7.
Garofoli F, Mazzucchelli I, Angelini M, Klersy C, Ferretti VV, Gardella B, et al. Leptin levels of the perinatal period shape offspring’s weight trajectories through the First. Year of Age. 2022;14(7):1451.
Cioana M, Michalski B, Fahnestock MJAR. Insulin-like growth factor and insulin‐like growth factor receptor expression in human idiopathic autism Fusiform Gyrus tissue. 2020;13(6):897–907.
Al-Zaid FS, Alhader AA, Al-Ayadhi, LYJSr. Altered ghrelin levels in boys with autism: a novel finding associated with hormonal dysregulation. 2014;4(1):1–5.
Arnoldussen IA, Kiliaan AJ, Gustafson DRJEN. Obesity and Dementia: adipokines interact with the brain. 2014;24(12):1982–99.
Rodrigues DH, Rocha NP, da Cunha Sousa LF, Barbosa IG, Kummer A, Teixeira ALJN. Changes in adipokine levels in autism spectrum disorders. 2014;69(1):6–10.
Singh S, Yazdani U, Gadad B, Zaman S, Hynan LS, Roatch N et al. Serum thyroid-stimulating hormone and interleukin-8 levels in boys with autism spectrum disorder. 2017;14(1):1–7.
Yang C-J, Liu C-L, Sang B, Zhu X-M, Du Y-JJN. The combined role of serotonin and interleukin-6 as biomarker for autism. 2015;284:290–6.
Jyonouchi H, Geng L, Streck DL, Dermody JJ, Toruner GAJJN. MicroRNA expression changes in association with changes in interleukin-1ss/interleukin10 ratios produced by monocytes in autism spectrum disorders: their association with neuropsychiatric symptoms and comorbid conditions (observational study). 2017;14(1):1–14.
Raghavan R, Zuckerman B, Hong X, Wang G, Ji Y, Paige D et al. Fetal and infancy growth pattern, cord and early childhood plasma leptin, and development of autism spectrum disorder in the Boston birth cohort. 2018;11(10):1416–31.
Ghaffari MA, Mousavinejad E, Riahi F, Mousavinejad M, Afsharmanesh MRJN. Increased serum levels of tumor necrosis factor-alpha, resistin, and visfatin in the children with autism spectrum disorders: a case-control study. 2016;2016.
Yürümez E, Uğur Ç, Sertçelik MJP, Psychopharmacology C. The assessment of serum omentin levels of children with autism spectrum disorder and attention-deficit/hyperactivity disorder. 2018;28(3):268–75.
Prosperi M, Guiducci L, Peroni DG, Narducci C, Gaggini M, Calderoni S et al. Inflammatory biomarkers are correlated with some forms of regressive autism spectrum disorder. 2019;9(12):366.
Maeda N, Funahashi T, Matsuzawa Y, Shimomura IJA. Adiponectin, a unique adipocyte-derived factor beyond hormones. 2020;292:1–9.
Fujita-Shimizu A, Suzuki K, Nakamura K, Miyachi T, Matsuzaki H, Kajizuka M et al. Decreased serum levels of adiponectin in subjects with autism. 2010;34(3):455–8.
Blardi P, de Lalla A, Ceccatelli L, Vanessa G, Auteri A, Hayek JJN. Variations of plasma leptin and adiponectin levels in autistic patients. 2010;479(1):54–7.
Ashwood P, Kwong C, Hansen R, Hertz-Picciotto I, Croen L, Krakowiak P et al. Brief report: plasma leptin levels are elevated in autism: association with early onset phenotype? 2008;38(1):169–75.
Banks WAJP. The many lives of leptin. 2004;25(3):331–8.
Pylipow M, Spector LG, Puumala SE, Boys C, Cohen J, Georgieff, MKJTJop. Early postnatal weight gain, intellectual performance, and body mass index at 7 years of age in term infants with intrauterine growth restriction. 2009;154(2):201–6.
Coupe B, Grit I, Hulin P, Randuineau G, Parnet PJPO. Postnatal growth after intrauterine growth restriction alters central leptin signal and energy homeostasis. 2012;7(1):e30616.
Harvey J, Solovyova N, Irving AJP. Leptin and its role in hippocampal synaptic plasticity. 2006;45(5):369–78.
Savino F, Liguori SA, Fissore MF, Oggero R, Silvestro L, Miniero RJJ et al. Serum ghrelin concentration and weight gain in healthy term infants in the first year of life. 2005;41(5):653–9.
Yis U, Öztürk Y, Sisman AR, Uysal S, Soylu ÖB, Büyükgebiz BJTT. The relation of serum ghrelin, leptin and insulin levels to the growth patterns and feeding characteristics in breast-fed versus formula-fed infants. 2010;52(1):35.
Savino F, Grassino E, Fissore MF, Guidi C, Liguori SA, Silvestro L et al. Ghrelin, motilin, insulin concentration in healthy infants in the first months of life: relation to fasting time and anthropometry. 2006;65(2):158–62.
Scheepens A, Möderscheim TA, Gluckman PDJHRP. The role of growth hormone in neural development. 2005;64(Suppl. 3):66–72.
Li Z, Xiao G-Y, He C-Y, Liu X, Fan X, Zhao Y et al. Serum levels of insulin-like growth factor-1 and insulin-like growth factor binding protein-3 in children with autism spectrum disorder. 2022;24(2):186–91.
Cummings K, Watkins A, Jones C, Dias R, Welham A. Behavioural and psychological features of PTEN mutations: a systematic review of the literature and meta-analysis of the prevalence of autism spectrum disorder characteristics. J Neurodevelopmental Disorders. 2022;14(1):1–27.
Fu S, Bury LA, Eum J, Wynshaw-Boris A. Autism-specific PTEN p. Ile135Leu variant and an autism genetic background combine to dysregulate cortical neurogenesis. Am J Hum Genet. 2023;110(5):826–45.
Thomas SD, Jha NK, Ojha S, Sadek B. mTOR signaling disruption and its Association with the development of Autism Spectrum Disorder. Molecules. 2023;28(4):1889.
Kanner LJNc. Autistic disturbances of affective contact. 1943;2(3):217–50.
Johnson CP, Myers SMJP. Identification and evaluation of children with autism spectrum disorders. 2007;120(5):1183–215.
Reichow B, Barton EE, Boyd BA, Hume KJC. Early intensive behavioral intervention (EIBI) for young children with autism spectrum disorders (ASD). 2012(10).
Rogers SJ, Estes A, Lord C, Vismara L, Winter J, Fitzpatrick A et al. Effects of a brief early start Denver Model (ESDM)–based parent intervention on toddlers at risk for autism spectrum disorders: a randomized controlled trial. 2012;51(10):1052–65.
Constantino JN, Majmudar P, Bottini A, Arvin M, Virkud Y, Simons P et al. Infant head growth in male siblings of children with and without autism spectrum disorders. 2010;2(1):39–46.
Courchesne E, Carper R, Akshoomoff NJJ. Evidence of brain overgrowth in the first year of life in autism. 2003;290(3):337–44.
Dawson G, Munson J, Webb SJ, Nalty T, Abbott R, Toth KJB. Rate of head growth decelerates and symptoms worsen in the second year of life in autism. 2007;61(4):458–64.
Fukumoto A, Hashimoto T, Ito H, Nishimura M, Tsuda Y, Miyazaki M, et al. Growth of head Circumference in Autistic Infants during the First year of life. 2008;38(3):411–8.
Fukumoto A, Hashimoto T, Mori K, Tsuda Y, Arisawa K, Kagami SJB, et al. Head Circumference and body Growth in Autism Spectrum Disorders. 2011;33(7):569–75.
Gillberg C, De Souza LJDM, Neurology C. Head circumference in autism, Asperger syndrome, and ADHD: a comparative study. 2002;44(5):296–300.
Hazlett HC, Poe M, Gerig G, Smith RG, Provenzale J, Ross A et al. Magnetic resonance imaging and head circumference study of brain size in autism: birth through age 2 years. 2005;62(12):1366–76.
Kral TV, Chittams J, Bradley CB, Daniels JL, DiGuiseppi CG, Johnson SL et al. Early life influences on child weight outcomes in the study to explore early development. 2019;23(4):954–62.
McKeague IW, Brown AS, Bao Y, Hinkka-Yli-Salomäki S, Huttunen J. Sourander AJBp. Autism with intellectual disability related to dynamics of head circumference growth during early infancy. 2015;77(9):833 – 40.
Mraz KD, Dixon J, Dumont-Mathieu T, Fein DJJCN. Accelerated head and body growth in infants later diagnosed with autism spectrum disorders: a comparative study of optimal outcome children. 2009;24(7):833–45.
Muratori F, Calderoni S, Apicella F, Filippi T, Santocchi E, Calugi S et al. Tracing back to the onset of abnormal head circumference growth in Italian children with autism spectrum disorder. 2012;6(1):442–9.
Rommelse NN, Peters CT, Oosterling IJ, Visser JC, Bons D, van Steijn DJ et al. A pilot study of abnormal growth in autism spectrum disorders and other childhood psychiatric disorders. 2011;41(1):44–54.
Surén P, Stoltenberg C, Bresnahan M, Hirtz D, Lie KK, Lipkin WI et al. Early growth patterns in children with autism. 2013;24(5):660.
Torrey EF, Dhavale D, Lawlor JP, Yolken, RHJBp. Autism and head circumference in the first year of life. 2004;56(11):892–4.
van Daalen E, Swinkels SH, Dietz C, van Engeland H, Buitelaar JKJPN. Body length and head growth in the first year of life in autism. 2007;37(5):324–30.
Webb SJ, Nalty T, Munson J, Brock C, Abbott R, Dawson GJJCN. Rate of head circumference growth as a function of autism diagnosis and history of autistic regression. 2007;22(10):1182–90.
Acknowledgements
The authors are grateful for the financial support of the Research Vice-Chancellor of Tabriz University of Medical Sciences, Tabriz, Iran.
Funding
This work was supported by the Research Vice-Chancellor of Tabriz University of Medical Sciences, Tabriz, Iran (grant number: 68636).
Author information
Authors and Affiliations
Contributions
SK, MA, and RMG have made substantial contributions to the conception and design of this study. Dr. SK and RMG conducted the search and extracted the data and RMG wrote the first draft of the manuscript; and Dr. SK and Dr. MA commented on previous versions of the manuscript. FHK conducted the quality assessment of the included articles. All authors read and approved the final content.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The protocol of this study was approved and registered by the Ethical Committee of Tabriz University of Medical Sciences (ethical code: IR.TBZMED.REC.1400.1243).
Consent for publication
Not Applicable.
Competing interests
The authors declare no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Molani-Gol, R., Alizadeh, M., Kheirouri, S. et al. The early life growth of head circumference, weight, and height in infants with autism spectrum disorders: a systematic review. BMC Pediatr 23, 619 (2023). https://doi.org/10.1186/s12887-023-04445-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-023-04445-9