
Abstract
Background
Traditional measurement of vaccine coverage can mask the magnitude of timely uptake of vaccine. Hence, the optimal measurement of timeliness is unclear due to variations in vaccine schedule among countries in the world. In Ethiopia, Oral Polio Virus (OPV), Pentavalent, Tetanus, H. influenza type B, Hepatitis B, and Pneumonia-Conjugate Vaccine (PCV) are basic vaccines which are taken at birth, six weeks, ten weeks, and fourteen weeks respectively. Despite its importance, information is scarce about on-time vaccination in the study area. Therefore, this study aimed to assess prevalence and factors associated with on-time vaccination among children of age 12–23 months in Boricha district, Sidama Ethiopia, in 2019.
Methods
A community based survey was conducted in Boricha district, Sidama region Ethiopia from January 1–30 in 2019. Study participants were selected using stratified multistage sampling technique. Kebeles were stratified based on residence. First, Kebeles were selected using random sampling. Then, systematic random sampling was employed to reach each household. Data were collected using structured and interviewer administered questionnaire. Logistic regression analysis was employed to identify factors associated with timely vaccination. Then, independent variables with p-value < 0.25 in COR were fitted further into multivariate logistic regression analysis model to control the possible cofounders. AOR with 95% CI and p-value < 0.05 was computed and reported as the level of statistical significance.
Results
From a total of 614 study participants, only 609 study participants have responded to questions completely making a response rate of 99.2%. Prevalence of timeliness of vaccination was 26.8% (95% CI: 25, 28) in this study. Factors like children of women with formal education (AOR = 5.3, 95%CI,2.7, 10.4), absence of antenatal care visit (AOR = 4.2,95%CI, 1.8,9.8), home delivery (AOR = 6.2,95%CI,4.0,9.3), lack of postnatal care (AOR = 3.7,95%CI,1.1,13.3), and lack of information about when vaccines completion date (AOR = 2.0, 95% CI,1.13,3.8) were factors influences timely vaccination among children of age 12–23 months.
Conclusion
Prevalence of on-time vaccination among children of age 12–23 months is lower than national threshold. Therefore, sustained health education on vaccination schedule and reminder strategies should be designed and implemented. Furthermore, maternal and child health care services should be enhanced and coordinated to improve on-time uptake of vaccine.
Similar content being viewed by others

Background
Globally, the performance of vaccination programs has been assessed through vaccine coverage indicators. It is the proportion of children who have received a vaccine by a benchmark age, or number of doses of vaccine for a particular antigen in the specific age group regardless of the timing of administration [1]. Although vaccination coverage and defaulting are useful metrics, there can be substantial disparities between these measures and measures that consider timing of vaccine administration [2]. Vaccination coverage and timeliness of vaccine are related but separate issues. High level of vaccine coverage can sometimes mask the low level of vaccine timeliness [3]. Maintaining high-quality expanded immunization program is challenging, with non-attendance and delays to vaccination appointments in developing countries [4, 5]. Consequently, timely vaccination is the pivotal action during infancy, as trans-placental immunity decreases rapidly after birth [6].
Based on the World Health Organization (WHO) report, vaccine coverage indicator has failed to show on-time vaccine coverage [7]. According to WHO recommendation, timely vaccination indicates when a child completes age-appropriate vaccination [8]. Several studies also revealed that despite high vaccine coverage in most countries, there is substantial gap on the timely administration of childhood vaccination with substantial delay in age-appropriate vaccine [9,10,11].
Globally, the Expanded Program of Immunization (EPI) agenda was planned by applying WHO standards to give the primary vaccination series to at least 90% of children [12]. Ethiopia launched the EPI program in 1980. Currently, vaccines are provided for 11 antigens at birth, six weeks, ten weeks, fourteen weeks and nine months [13]. Although vaccines are provided freely in Ethiopia, the total vaccine coverage was still 49.9% in 2016 [14]. This is well below the target of 95% coverage of fully immunized infants set by the Health Sector Transformation Plan (HSTP) by 2020 [15, 16]. Regarding the overall timeliness of vaccination, the coverage was increased from 18% in 2014 to 22% in 2016 [17]. Particularly, Diphtheria Tetanus Pertussis (DTP1) (63.8%), Oral Polio Vaccine (OPV1) (63.1%), and measles (68.5%) were delayed for more than one month beyond WHO recommended schedule [18].
Currently, the timing of vaccine administration has received increasing attention when the level of vaccination coverage is close to that needed for protective herd immunity [19, 20]. Vaccine timeliness is critical in Sub-Saharan African countries since most of the causes of child deaths are vaccine preventable diseases [5]. It is used to observe active response, minimize individual vulnerability, and prevent disease outbreaks within societies in a given country [21].
Previous studies have revealed that untimely vaccination of measles poses a threat to susceptible children [2, 3]. Besides, previous studies highlighted that vaccine timeliness is a crucial indicator to understand population-level disease susceptibility [15, 16]. Therefore, age appropriate vaccine coverage has to be achieved to control and eliminate vaccine-preventable infectious diseases [19, 22, 23].
Previous study in Ethiopia showed that socio-demographic, maternal health service and health institution factors were associated with delay or early vaccination of children. For example, women’s educational status, wealth index, and women who used maternal and child health services were positive predictors of on-time vaccination. On the contrary, older caregivers, distant health institutions,and vaccinations at health post were protective against on-time vaccine coverage [24]. Marked child immunization differentials are also observed by community and ethnic group effects suggest that further targeting of health activities could be efficient and effective [25]. Although studies have measured the full vaccination coverage, studies on timely vaccination are rare in Sub- Saharan Africa [26, 27]. Specifically, a few previous studies were conducted about timeliness of vaccination in different parts of Ethiopia; most of them were conducted either at urban settings or at the national level [24, 28,29,30]. Local contextual policy planning should be mandatory for achieving the national expanded programe of immunization target. However, information is limited about the timeliness of vaccinations in Sidama, Ethiopia. Therefore, this study aimed to assess the prevalence of incomplete immunization status and factors among children 12–23 months of age in Boricha, South Ethiopia, in 2019.
Methods
Study design, period and setting
Community based cross-sectional study was conducted in Boricha district, Sidama region, Ethiopia from January 1–30, 2019. Boricha is one of 36 districts in Sidama region, in Ethiopia. It is 32 km away from Hawassa, the capital city of Sidama regional state. It is divided into 43 Kebeles (lowest administrative units in Ethiopia). There are 39 rural and 4 urban Kebeles in Boricha. Based on 2007 Ethiopian Central Statistical Agency (CSA) report the total population of the district was estimated as 317,605 in 2011. From this population, 16,452 were children of age 12–23 months. There were 10,132 infants in the district. A total of 50 public health institutions have provided vaccine freely in Boricha. These include 1 district hospital, 10 health centers, and 39 health posts. The health service coverage of the district was estimated as 85% for the total population.
Population
All children in the age range of 12–23 months who had at least single exposure of vaccination and permanently resided (lived for more than six months) in Boricha district were the source population. Children aged 12–23 months had at least single exposure a vaccination, lived in the selected households of selected Kebeles, and presented during data collection period were the study population in this study. All children of age 12–23 months, who were permanent resident of selected Kebeles, and whose mother / Guardians / were voluntary for consent, were included. On the contrary, children in 12–23 months whose mothers were seriously ill and, whose mothers or legal guardian refused to give consent were excluded from this study.
Sample size determination and sampling technique
The minimum sample size was calculated using a single population proportion formula. Furthermore, sample size determination considered the following key factors: Power, precision, baseline proportion of timeliness of vaccine, quality and cost of the study. Therefore, sample size was determined using the following assumptions: Proportion of timely vaccination of 41.2% from Ethiopian Demographic Health Survey (EDHS) analysis of vaccine timeliness of South Ethiopia [31], 95% confidence level, and 5% margin of error, a design effect of 1.5 and 10% non-response rate. Thus, standard Cochran formula (n = z2pq/d2) was used to compute the initial sample size. Plugging the values of above assumptions into formula, n = 1.962*(0.41) (0.59)/ (0.05)2. As a result, we have calculated as 372 sample size. Next, by considering sample size compensation factor of design effect of 1.5 and adding 10% non-response rate. The final sample size was computed as 614 for this study. The calculated sample sizes for factors associated with vaccine timeliness were lower compared with sample size calculated to prevalence of vaccine timeliness. Therefore, data were collected on a total of 609 children. Multi-stage stratified sampling strategy was employed to get actual study participants in the study. First, all Kebeles were stratified using residence as urban and rural Kebeles. Then, sample Kebeles were selected proportionally within each stratum. From a total of 39 Kebeles, 1 urban and 9 rural Kebeles were selected. List of households with children aged 12–23 months was utilized as the sampling frame from the registration book of health extension workers in each health posts. Then, systematic random sampling was applied to select sample households. Finally, simple random sampling technique was utilized to select a child for households which contain more than one child. If no one answered at a household, a revisit was conducted before the household was labelled as a non-respondent.
Data collection tools and procedures
Data were collected using structured, and interviewer administered questionnaire. The questionnaire was adapted from EDHS questionnaire. It included the following three parts: socio-demographic characteristics, information about vaccination completeness, and information about maternal health service utilization. Data were collected by 10 BSC Nurses who are fluent Sidama-afoo; local language. Two health officers supervised the data collection process daily. Problems, which were raised during data collection period, were solved through discussion at the end of every day.
Study variables
Timeliness of vaccination is the outcome variable in this study. It is a binary outcome variable. A woman/guardian/ was asked to show vaccine card or/and recall the time of birth of the child and her child vaccination appointment. Then, the vaccine schedule was compared with the vaccine card for inconsistency. If there was delay or early vaccination from WHO standard recommendation, timely vaccination was absent, and recoded as ‘0’, otherwise,’1’. The explanatory variables included in the analysis of this study were socio-demographic characteristics, vaccine information related factors, and maternal health services utilization. Socio-demographic variables were the following factors: Age, educational status, occupation, place of residence, marital status, monthly income level and family size. Child and maternal health service related factors consisted antenatal visit, place of delivery, postnatal care, child birth order and sex of a child. Information related variables were: Awareness vaccine preventable disease, vaccine protects from illness, session needed for full vaccination, age of children to begin vaccine, age of children to complete vaccine, importance of vaccine for child health and vaccine can cause health problem.
Operational definitions
Full vaccination
Was defined as the child vaccination status once an infant has received all recommended vaccines included in the national schedule: A dose of Bacilli Chalmette Guerin (BCG); three doses of Oral Polio Vaccine (OPV); three doses each of Pentavalent and Pneumococcal Conjugate Vaccine (PCV); one dose of Inactivated Polio Vaccine (IPV); two doses of rotavirus and one dose of measles vaccines by the age of 12 months [32, 33].
Vaccine timeliness
Was defined as vaccine dose administered within four days prior [27, 33] and within four weeks after the recommended age-specific vaccine according to national immunization schedule [23, 27, 34]. Table 1 of this study indicates that on-time full vaccination was also defined as all vaccine doses administered within four days prior [27, 33], and within four weeks after the recommended age specified in the national immunization schedule. Otherwise, it was not considered as on-time full vaccination if at least one vaccine dose was given early, late or missed at all [27, 34, 35] (see Table 1).
Kebele
Is the smallest administrative unit in Ethiopia which consists of around 2000 households. It is much similar unit to sub-district in other countries [36].
Data quality control
Questionnaire was initially prepared in English and translated into Sidama-afoo (local language) and back to English, by language experts to ensure its consistency. Training was given for data collectors and supervisors for two days. Pre-testing was conducted on 5% of sample size in Kebeles which were not included in actual study to check consistency and any ambiguity of the questionnaire a week back of actual data collection. Then, any deviation identified during pretest was checked again and rephrased or re-adjusted accordingly. Data completeness was checked by the supervisor daily and weekly by the principal investigator for completeness and missing data.
Data analysis
Data were entered into Epi-data version 4.4, exported and analyzed using SPSS version 22. Data coding and cleaning was conducted before formal analysis. Descriptive analysis was carried out by frequency tables, graphs and charts. Chi-square test was performed to identify association between the outcome and independent variables. 12 variables were found to have association (P-value < 0.05). After necessary logistic regression assumption was checked, binary logistic regression was fitted and 10 variables were found to be associated with timeliness of vaccine (p-value < 0.25). Then, these variables were further fitted into multivariate logistic regression analysis to control possible cofounders. Finally, only six variables were found to be associated significantly in multivariate logistic regression analysis model. Hosmer Lemeshow goodness of fit test was used to check goodness of fit of the model, and it was good fit. Binary logistic regression was done to identify candidate variables that can be fitted into multivariable logistic regression analysis model. Statistical significance of variables at final model was declared at p-value less than 0.05 and 95% CI of Adjusted Odds Ratio (AOR). Finally, Hosmer–Lemeshow goodness of fit test was used to estimate the goodness of fit of the adjusted final model [37]. All cases were analyzed except the non-respondent in this study.
Multicollinearity and interaction effect
The presence of multicollinearity was checked among independent variables using Variance Inflation Factor (VIF) at cut off point of 10 [38]. Accordingly, multicollinearity between variables was found to be VIFs < 2. Moreover, the tolerance of all variables was greater than 0.1 which indicates no meaningful multicollinearity in this study.
Results
Socio-demographic characteristics
Table 2 presents the socio-demographic characteristics of study participants of this study. From the total of 614 study subjects, six hundred nine (609) study participants have responded questions completely making a response rate of 99.2%. Non-respondents were examined for their main reason for loss of on time vaccination and found not related with timeliness of vaccine. The mean age of study subjects was 28.2 ± 5.1 years. Furthermore, the mean age of children was 17.2 ± 3.3 months. More than half (57.0%) of children were females. From the total study participants, 242(39.7%) study participants were illiterate. Most (94.5%) of the study participants resided in rural area. Nearly all (98.4%) study participants were married. More than half (53.2%) of the study participants earn less than 9.2 USD per month. Most of (95.4%) the study participants were Sidama ethnic group. Majorities (89.5%) of the study participants were Protestants. Five-hundred (82.3%) of the study participant were housewives in this study (see Table 2).
Information about vaccination
Based on the report of Table 3, nearly all (99%) care givers had heard about vaccination and vaccine preventable diseases. Nearly all participants (91.3%) had awareness about vaccine can protect disease. In addition, most (93.6%) of the participants knew the benefit of vaccine for healthy child. Only 35(5.8%) of the participants mentioned more than five vaccine preventable diseases. On the contrary, half (50.4%) of the participants knew that the age of children to begin vaccination is at 45th day of birth. Besides, majorities nearly four out of five (78.3%) of the study participants identified the end date of child vaccination (see Table 3).
Maternal health service utilization
Table 4 presented the maternal health service utilization, two-hundred-eighty (46%) did not have history of antenatal care visit. About 22.1% of them had at least three visits during their pregnancy of the child selected for this study. More than half (59.9%) of the primary caretakers did not get postnatal care service for the current child. Among children ever born by the mothers, majorities (60.8%) of children were from 3–4 birth order. Two-third (57%) of children was born at health institutions (see Table 4).
Proportion of timely vaccination
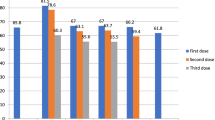
Prevalence of timely vaccination was 26.8% (95%CI: 25%, 29%) in the study area. From a total of 614 study participants, 609 children aged 12–23 months gave full response making a response rate of 99.2%. Majorities 494(81.1%) of the study participants had vaccination card which indicated complete vaccination. Figure 1 highlights proportion of delayed vaccine time in this study. The most defaulted vaccine was measles (21.7%) followed by PCV3 (17.9%). A total of 10.8% of the children did not take BCG vaccine. Besides, OPV1 was the least defaulted vaccine (7.6%). Besides, measles was the most defaulted vaccine (24.2%) followed by PCV3 vaccines (20.5%). Nearly (26.8%) of the children aged 12–23 months were incompletely vaccinated by card and history from mothers of children (see Fig. 1).

Deviation from national vaccine schedule among children of age 12–23 months, Boricha district, South Ethiopia, in 2022
Reasons for timely vaccination
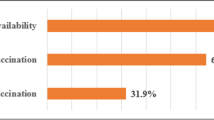
According to Table 5 description of reasons for delayed vaccination, most (45.4%) of the study participants have explained that lack of information for next dose was their main reason. Inconvenient vaccination time (39.3%) and shortage of vaccines in health institutions (32.5%) are the remain major significant problems (see Table 5).
Factors associated with timely vaccination
Of the 12 variables that were statistically associated with timely vaccination in unadjusted analyses, six remained significant in multivariable analyses. Specifically, compared with women without formal education, women with formal education had 5.3 times more chance of having timely vaccination (AOR = 5.3, 95%CI, 2.7, 10.4). Furthermore, children whose mother without previous antenatal care had 4.3 fold higher odds of untimely vaccination than their counterparts (AOR = 4.2, 95%CI, 1.9, 9.8). The chance of late /early/ vaccination among children of age 12–23 months who was born at home was higher than their counterparts (AOR = 6.2, 95%CI, 4.0, 9.3). The likelihood of dropouts from vaccine schedule among children whose mother (caregiver) who had no postnatal care visit was 3.7 times more than their counterparts (AOR = 3.7, 95%CI, 1.2, 13.3). The odd of timeliness of vaccination among children whose mothers can not identified the time of completion of vaccine was twofold higher than their counterparts (AOR = 2.0, 95% CI, 1.2, 3.8). The chance of timely vaccination among children whose mother had three sessions needed for complete vaccination was 2.1 times higher than those of women with four sessions (AOR = 2.1, 95% CI, 1.2, 3.3) (see Table 6).
Discussion
Apart from measurement of total vaccine coverage, vaccine timeliness should be the key EPI indicator to measure vaccine efficacy and effectiveness. To design and implement vaccine policy and programs, contextual local studies are needed to inform the target of intervention. Hence, we have tried to highlight the prevalence and factors associated with vaccine timeliness among children of age 12–23 months in Boricha Sidama Ethiopia in 2019.
Accordingly, timeliness of vaccination among children aged 12–23 months was found to be 26.8% (95%CI: 25%, 29%) in this study. Our finding highlights that it is far behind the national target [32]. The possible explanation might be associated with the presence of vaccine misinformation, challenge in the supply chain system related to COVID-19 infection or due to fragility of the study setting because of conflict and migration. Furthermore, parents/guardians/of children might hesitate take their children for vaccination into health institutions because of fear of side effects, excessive waiting time, rumors about vaccine and fear of injection [39, 40].
When comparing our results to those of older studies, it must be pointed out that this finding is less than findings of studies done in Gondar city, Northwest Ethiopia (31.9%) [24], and Addis Ababa (55.9%), Ethiopia [29]. We have verified that differences in place of residents could result in variation of socio-demographic characteristics, access to health care and attention. In Ethiopia, urban areas historically have easier access to health services and better transportation available, whereas rural health centers may face challenges with vaccine shortages, cold chain maintenance, attrition of the health care work force, and density of clinics relative to urban areas [41]. This result goes beyond the previous report of the study North West Ethiopia (68%) [24]. The possible reason might be due to effective mentorship of vaccine program, better commitment of health extension workers and better awareness about vaccine in community.
Regarding factors associated with timely vaccination, children whose mothers were uneducated were more chance of getting timely of vaccination than their counterparts. This is consistent with findings previous studies conducted in Gondar city, Northwest, Ethiopia [42] and Tigray, North Ethiopia [43]. This might be due to low level of understanding about the benefits of vaccination, low chance of exposure and difficulty to interpret and low perceived impact of vaccine completeness. Besides, low education level can hinder the caregiver’s communication with health workers and might influence caregiver’s awareness to seek and take advantage of public health services including child vaccination. Finally, educated women may choose health care services that generate better health. This may be because education may provide greater knowledge of the health care utilization and the ability to respond to new knowledge more rapidly [44,45,46].
Children of women who did not attend antenatal care were more likely to default from vaccine schedule than their counterparts. This finding is similar with findings of studies conducted in Gondar city, Northwest Ethiopia [42], and Debre-Lebanon, Central Ethiopia [47]. This consistency can be explained by the fact that pregnant women who attend prenatal care can be counseled and reminded the vaccine schedule. Moreover, utilization of subsequent health service such as delivery in the health institution, postnatal care, family planning and expanded programme of immunization can be advocated at antenatal care visit.
Antenatal care visit at a health institution during pregnancy can have better chance of taking one or more tetanus toxoid vaccine which creates further opportunities to obtain adequate information to discuss vaccines and vaccine-preventable diseases and to encourage adherence to vaccine schedules [48,49,50]. On-time vaccination was found to be higher among children whose mothers attended postnatal care than their counterparts. This find is in line with previous study conducted in Kenya [35]. The possible explanation could be due to strong counseling about vaccine schedule and provision of vaccine card among women during postnatal visit and service integration of postnatal care with EPI. Furthermore, the fact that most caregivers are females than males indicate that males have less chance to be involved during prenatal care, child birth and postnatal care. Therefore, they might have less chance of knowledge about vaccination. Furthermore, the have more social pressure.
Mothers who gave birth at home were more likely to default from the vaccination schedule than their counterparts. A similar pattern of result was obtained the study done in the west Shewa zone [42]. The possible reason for this consistency might be due to lack of information about the benefits and time of the vaccine during childbirth and immediate postnatal care. Furthermore, women who gave birth at home might be exposed to wrong cultural perceptions and practice about disease prevention for children than vaccine. Children of women who did not know a vaccine protect children from illness were more likely to take delayed vaccine than their counterparts. This result ties well with previous study done in West Shewa, Ethiopia [42]. The possible explanation might be that, as women did not have awareness about vaccine protection against illness, they could not complete vaccines. Moreover, special preparation and planning revisit programs may be done when women are aware of complication of incomplete vaccination. A similar conclusion was reached that lack of access to information and knowledge about, by whom, where, and when children should be vaccinated were significantly associated with defaulting from completion of children vaccinated [51, 52].
Children of caregivers who did not know the importance of vaccine had more chance of taking an untimely vaccine than their counterparts. Our result was broadly in line with finding of studies done in Hawassa zuria [53], Sinana district, South East of Ethiopia [54]. The possible rationale could be due to caregivers that could not change their health-seeking behavior to vaccinate their children unless they are well informed and correct their misconception. Children whose caregivers were know that the maximum number of vaccine dose is three doses were more likely to delay from on-time vaccination than caregivers who know four doses for completing vaccine. The basic finding is consistent to the findings of previous studies [31, 55, 56]. The probable explanation could be due to the fact that lack of clear information from health providers about timing of vaccination until completion of vaccine doses.
Limitation of the study
This study had a number of strengths. First, it addresses important public health problem through community based study yielding accurate estimate. Moreover, it filled the gap by assessing the problem in most affected rural children. An apparent limitation of the method is that it cannot prove the causal relationship between the outcome and explanatory variables. Further, this study suffers from the limitation of recalling bias.
However, we ascertained vaccination outcomes objectively from expanded programe of immunization cards and expanded programe of immunization registers of health facilities, and we restricted the analysis to children of age 12–23 months to minimize recalling bias. Another limitation of this study had could not assess distance from health facilities. Lastly, this study cannot show the separate analysis of cases who seek vaccines lately or early. Further research should be done using qualitative methods to explore more about women perceptions health provider and stakeholder opinions and contextual assessment about on-time vaccination in the study area. Besides, future studies should make disaggregate analyses for a late and early vaccine.
Conclusion
To conclude, the proportion of timely vaccination among children was lower than the national threshold. Uneducated women, history of absence in antenatal care visit, children who gave birth at home, mothers without postnatal care visits and lack of information about the benefits of vaccination and number of sessions needed for full vaccination were statistically significant with delays in timely vaccination of children aged 12–23 months. Therefore, efforts should be strengthened to expand maternal health services. Furthermore, strong awareness creation should be intensified not only for vaccine coverage but also for on time vaccination based on national schedule.
Public health implication
The results of this study can be a benchmark for policy makers mainly situated at regionally. They can be well informed about strengthening and integrating vaccine information into maternal health services such as antenatal, delivery and postnatal care.
Availability of data and materials
For those who are interested; the datasets of this study could be accessed from the corresponding author on reasonable request.
Abbreviations
- AOR:
-
Adjusted Odds Ratio
- CI:
-
Confidence Interval
- EDHS:
-
Ethiopian Demographic and Health Survey
- EFY:
-
Ethiopian Fiscal Year
- FMOH:
-
Federal Ministry of Health
- NGO:
-
Nongovernmental Organization
- OR:
-
Odds Ratio
- BCG:
-
Baccilus Calmet Gullerian
References
Luman ET, et al. Timeliness of childhood vaccinations in the United States: days undervaccinated and number of vaccines delayed. JAMA. 2005;293(10):1204–11.
Dayan GH, et al. Assessment of delay in age-appropriate vaccination using survival analysis. Am J Epidemiol. 2006;163(6):561–70.
Hull BP, McIntyre PB. Timeliness of childhood immunisation in Australia. Vaccine. 2006;24(20):4403–8.
Babirye JN, et al. Timeliness of childhood vaccinations in Kampala Uganda: a community-based cross-sectional study. PLoS ONE. 2012;7(4): e35432.
Machingaidze S, Wiysonge CS, Hussey GD. Strengthening the expanded programme on immunization in Africa: looking beyond 2015. PLoS Med. 2013;10(3): e1001405.
de Cock C, et al. Use of apps to promote childhood vaccination: systematic review. JMIR Mhealth Uhealth. 2020;8(5): e17371.
Feldstein LR, et al. School-based delivery of routinely recommended vaccines and opportunities to check vaccination status at school, a global summary, 2008–2017. Vaccine. 2020;38(3):680–9.
Maman K, et al. The value of childhood combination vaccines: from beliefs to evidence. Hum Vaccin Immunother. 2015;11(9):2132–41.
Mutua MK, et al. Fully immunized child: coverage, timing and sequencing of routine immunization in an urban poor settlement in Nairobi Kenya. Trop Med Health. 2016;44(1):1–12.
Scott S, et al. Coverage and timing of children’s vaccination: an evaluation of the expanded programme on immunisation in the Gambia. PLoS ONE. 2014;9(9): e107280.
Fadnes LT, et al. Is vaccination coverage a good indicator of age-appropriate vaccination? A prospective study from Uganda. Vaccine. 2011;29(19):3564–70.
Negussie A, et al. Factors associated with incomplete childhood immunization in Arbegona district, southern Ethiopia: a case – control study. BMC Public Health. 2016;16(1):27.
Kinfe Y, Gebre H, Bekele A. Factors associated with full immunization of children 12–23 months of age in Ethiopia: A multilevel analysis using 2016 Ethiopia Demographic and Health Survey. PLoS ONE. 2019;14(11): e0225639.
Control, C.f.D and Prevention. Ten great public health achievements--United States, 1900–1999. MMWR. Morb Mortal Wkly Rep. 1999;48(12):241–243.
Dombkowski KJ, Lantz PM, Freed GL. The need for surveillance of delay in age-appropriate immunization. Am J Prev Med. 2002;23(1):36–42.
Rodewald L, et al. Immunization performance measurement in a changing immunization environment. Pediatrics. 1999;103(Supplement_1):889–897.
Demographic E. Health survey: Addis Ababa. Ethiopia and Calverton, Maryland, USA: Central statistics agency and ORC macro, 2011. 2011.
Ndiritu M, et al. Immunization coverage and risk factors for failure to immunize within the Expanded Programme on Immunization in Kenya after introduction of new Haemophilus influenzae type b and hepatitis b virus antigens. BMC Public Health. 2006;6(1):1–8.
Lernout T, et al. Timeliness of infant vaccination and factors related with delay in Flanders. Belgium Vaccine. 2014;32(2):284–9.
Saini V, et al. Timeliness and completeness of routine childhood vaccinations in children by two years of age in Alberta Canada. Can J Public Health. 2017;108(2):e124–8.
Organization WH. Reaching every district (RED): A guide to increasing coverage and equity in all communities in the African Region. 2017.
Kiely M, et al. Impact of vaccine delays at the 2, 4, 6 and 12 month visits on incomplete vaccination status by 24 months of age in Quebec Canada. BMC Public Health. 2018;18(1):1–15.
Mbengue MAS, Mboup A, Ly ID, Faye A, Camara FBN, Thiam M, Ndiaye BP, Dieye TN, Mboup S. Vaccination coverage and immunization timeliness among children aged 12-23 months in Senegal: a Kaplan-Meier and Cox regression analysis approach. Pan Afr Med J. 2017;27(Suppl 3).
Mekonnen ZA, et al. Timely completion of vaccination and its determinants among children in northwest, Ethiopia: a multilevel analysis. BMC Public Health. 2020;20(1):1–13.
Kiros G-E, White MJ. Migration, community context, and child immunization in Ethiopia. Soc Sci Med. 2004;59(12):2603–16.
Akmatov MK, Mikolajczyk RT. Timeliness of childhood vaccinations in 31 low and middle-income countries. J Epidemiol Community Health. 2012;66(7):e14–e14.
Schoeps A, et al. Socio-demographic determinants of timely adherence to BCG, Penta3, measles, and complete vaccination schedule in Burkina Faso. Vaccine. 2013;32(1):96–102.
Boulton ML, et al. Vaccination timeliness among newborns and infants in Ethiopia. PLoS ONE. 2019;14(2): e0212408.
Masters NB, et al. Vaccine hesitancy among caregivers and association with childhood vaccination timeliness in Addis Ababa Ethiopia. Hum Vaccin Immunother. 2018;14(10):2340–7.
Wagner AL, Tefera YA, Gillespie BW, Carlson BF, Boulton ML. Vaccine coverage, timeliness and delay estimated from regional and national cross-sectional surveys in Ethiopia, 2016. Pan Afr Med J. 2021;39(1).
Tadesse H, Deribew A, Woldie M. Predictors of defaulting from completion of child immunization in south Ethiopia, May 2008–A case control study. BMC Public Health. 2009;9(1):1–6.
Health, F.M.o. Ethiopia National Expanded Programme on Immunization, Comprehensive Multi-Year Plan 2011–2015. Federal Minisitry Of Health Addis Ababa, Ethiopia. 2010.
Kroger AT, Atkinson WL, Marcuse EK, Pickering LK. General recommendations on immunization; recommendations of the advisory committee on immunization practices (ACIP). 2006.
Hu Y, et al. Completeness and timeliness of vaccination and determinants for low and late uptake among young children in eastern China. Hum Vaccin Immunother. 2014;10(5):1408–15.
Adetifa IM, et al. Coverage and timeliness of vaccination and the validity of routine estimates: Insights from a vaccine registry in Kenya. Vaccine. 2018;36(52):7965–74.
Samia Z. Ethiopian national population and housing census. Addis Ababa: Ethiopian central statistics agency. 2007;308.
Hosmer Jr. DW, Lemeshow S, Sturdivant RX. Applied logistic regression (Vol. 398). Wiley; 2013.
Hamaker EL, et al. Model selection based on information criteria in multilevel modeling. Handbook of advanced multilevel analysis. 2011. p. 231-255.
Napolitano F, D’Alessandro A, Angelillo IF. Investigating Italian parents’ vaccine hesitancy: A cross-sectional survey. Hum Vaccin Immunother. 2018;14(7):1558–65.
Bianco A, et al. Parent perspectives on childhood vaccination: How to deal with vaccine hesitancy and refusal? Vaccine. 2019;37(7):984–90.
Lakew Y, Bekele A, Biadgilign S. Factors influencing full immunization coverage among 12–23 months of age children in Ethiopia: evidence from the national demographic and health survey in 2011. BMC Public Health. 2015;15(1):1–8.
Fadnes LT, et al. Vaccination coverage and timeliness in three South African areas: a prospective study. BMC Public Health. 2011;11(1):1–12.
Gebremeskel TG, et al. Magnitude and associated factors of delayed vaccination among children aged11-23 months in, Tigray, Ethiopia, 2018. Hum Vaccin Immunother. 2021;17(10):3831–7.
Grossman M. Education and nonmarket outcomes. Handbook Econ Educ. 2006;1:577–633.
Lindeboom M, Llena-Nozal A, van Der Klaauw B. Parental education and child health: Evidence from a schooling reform. J Health Econ. 2009;28(1):109–31.
Bloom SS, Wypij D, Das Gupta M. Dimensions of women’s autonomy and the influence on maternal health care utilization in a north Indian city. Demography. 2001;38(1):67–78.
Dejene H, et al. Vaccination Timeliness and Associated Factors Among Children Age 12–23 Months in Debrelebanos District of North Shewa Zone, Oromia Regional State, Ethiopia. Front Pediatrics. 2022;1229.
D’Alessandro A, et al. Vaccination knowledge and acceptability among pregnant women in Italy. Hum Vaccin Immunother. 2018;14(7):1573–9.
Danchin MH, et al. Vaccine decision-making begins in pregnancy: Correlation between vaccine concerns, intentions and maternal vaccination with subsequent childhood vaccine uptake. Vaccine. 2018;36(44):6473–9.
Rosso A, et al. Knowledge and attitudes on pediatric vaccinations and intention to vaccinate in a sample of pregnant women from the City of Rome. Vaccine. 2019;37(14):1954–63.
Bugvi AS, et al. Factors associated with non-utilization of child immunization in Pakistan: evidence from the Demographic and Health Survey 2006–07. BMC Public Health. 2014;14(1):1–7.
Dubé E, et al. Vaccine hesitancy: an overview. Hum Vaccin Immunother. 2013;9(8):1763–73.
Birhan Y, et al. Predictors of Immunization Defaulting Among Children Age 12–23 Months in Hawassa Zuria District of Southern Ethiopia: Community Based Unmatched Case Control Study. Int J Public Health Sci. 2014;3(3):7191.
Legesse E, Dechasa W. An assessment of child immunization coverage and its determinants in Sinana District Southeast Ethiopia. BMC Pediatrics. 2015;15(1):1–14.
Mohammed H, Atomsa A. Assessment of child immunization coverage and associated factors in Oromia regional state, eastern Ethiopia. Sci Technol Arts Res J. 2013;2(1):36–41.
Odusanya OO, et al. Determinants of vaccination coverage in rural Nigeria. BMC Public Health. 2008;8(1):1–8.
Acknowledgements
We are grateful to almighty God. We also extend our appreciation to Hawassa University, College of Medicine and Health Science, Department of Public Health, study participants, data collectors, Supervisors, Boricha District Health Office, Yirba Primary hospital manager, Boricha district Health Centers.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
BT conceived and designed the study, developed the data collection instruments, performed the statistical analysis and wrote first version of the manuscript. YT and AY design the study, participated in analysis and drafted the report. All authors critically revised and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All methods followed were in accordance with the ethical standards of the Helsinki Declaration). The study was approved by the Institutional Review Board (IRB) of Hawassa University, College of Medicine and Health Science. A formal letter was written to Boricha district health office for permission. Written informed consent was obtained from each mother / guardian/ of each child. Participants were asked to enroll and were told that they had the right not to respond to questions that they did not want to and could stop at any point in the survey if they wanted. The data was de-identified, de-linked and stored in a secure location.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Questionnaires.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Negash, B.T., Tediso, Y. & Yoseph, A. Predictors of timeliness of vaccination among children of age 12–23 months in Boricha district, Sidama region Ethiopia, in 2019. BMC Pediatr 23, 409 (2023). https://doi.org/10.1186/s12887-023-04234-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-023-04234-4