
Abstract
Background
Since the onset of the COVID-19 pandemic, SARS-CoV-2 has evolved into independent new forms, variants of concern (VOCs). While epidemiological data showed increased transmissibility of VOCs, their impact on clinical outcomes is less clear. This study aimed to investigate the differences between the clinical and laboratory features of children infected with VOCs.
Methods
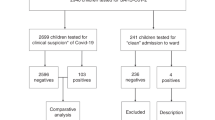
This study included all cases with SARS-CoV-2-positive nasopharyngeal swabs obtained from patients referred to Children’s Medical Center (CMC), an Iranian referral hospital, between July 2021 and March 2022. The inclusion criteria for this study included all patients, regardless of age, who had a positive test anywhere in the hospital setting. Exclusion criteria for the study included those whose data was obtained from non-hospital outpatient settings, or referred from another hospital. The SARS-CoV-2 genome area encoding the S1 domain was amplified and sequenced. The type of variant in each sample was identified based on the mutations in the S1 gene. Demographic characteristics, clinical data, and laboratory findings were collected from the patient’s medical records.
Results
This study included 87 pediatric cases with confirmed COVID-19, with a median age of 3.5 years (IQR: 1-8.12). Data from sequencing reveals the type of variants as 5 (5.7%) alpha, 53 (60.9%) Delta, and 29 (33.3%) Omicron. The incidence of seizure was higher in patients with Alpha and Omicron infection compared to the Delta group. A higher incidence of diarrhea was reported in Alpha-infected patients, and a higher risk of disease severity, distress, and myalgia was associated with Delta infection.
Conclusion
Laboratory parameters did not mostly differ among the patients infected with Alpha, Delta, and Omicron. However, these variants may manifest different clinical features. Further studies with larger sample sizes are required to fully understand the clinical manifestations of each variant.
Similar content being viewed by others


Background
The coronavirus disease 2019 (COVID-19) is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which was first reported in Wuhan city, China, in December 2019 [1]. As of May 2022, the pandemic had caused more than 510 million cases and 6 million deaths, making it one of the deadliest in history. In Iran, the first case of COVID-19 was identified in Qom city in February 2020. Since the first confirmed case, the number of cases has risen and resulted in more than 7 million cases infected and 140 thousand deaths [2].
COVID-19 can cause mild to severe illness; its clinical manifestations include fever, cough, shortness of breath, and in more severe cases, pneumonia, kidney failure, and eventually death. Apart from respiratory symptoms, gastrointestinal manifestations, including vomiting, diarrhea, constipation, and abdominal pain, are also common in COVID-19 patients [3, 4].
In children, SARS-CoV-2 infection has mostly resulted in mild or even asymptomatic infection [5,6,7,8,9]. However, a condition termed multisystem inflammatory syndrome in children (MIS-C) has emerged with the clinical manifestation of multi-organ involvement and occurred at a much-increased frequency compared to previous years [10,11,12,13,14].
The genomics analysis using next-generation sequencing (NGS) indicates that SARS-CoV-2 is an enveloped single-strand positive-sense RNA (+ ssRNA)- with a genome length of ∼ 30 kilobases encoding 9860 amino acids (aa) [15, 16]. The genome has 11 coding regions that can encode structural and non-structural proteins [17]. The main structural proteins include spike (s), envelope (E), membrane (M), and nucleocapsid (N). The S protein with a length of 1273 aa is one of the most important viral proteins that mediates receptor binding and virus entry. It has two major domains: S1 and S2. The S1 is responsible for receptor recognition and attachment, while S2 mediates cell fusion [18].
Genome sequence data have been extensively used to track the evolution of SARS-CoV-2 [19]. Most of the mutations of functional importance occur in S protein and can affect host tropism and viral transmission [20, 21]. Specific mutations in the S1 subunit of the S protein are considered genomic characteristics of variants of concern (VOCs) [22]. In October 2021, World Health Organization defines four VOCs: B.1.1.7 (Alpha) [23], B.1.351 (Beta) [24], P.1 (Gamma) [25], and B.1.617.2 (Delta) [26]. As of December 2021, a new VOC, B.1.1.529 (Omicron) variant, has been detected and has spread globally [27].
Each variant harbors several mutations. The Alpha-variant harbors N501Y and P681R mutations. The Beta-variant harbors these mutations with the addition of the E484K and K417N mutations. The Delta-variant has several spike mutations including T19R, G142D, E156G/Δ 157–158, L452R, T478K and D950N [28]. Omicron-variant harbors multitude of mutations (more than 30) in the spike gene, which increase the concerns of enhanced infectivity and immune escape ability [29].
Although there should be evidence of increased transmissibility, virulence, or immunity for a lineage to be classified as a VOC [30], the impact of the evolution on clinical outcomes, especially in children, is yet to be fully understood. Therefore, in this study, we analyzed the S1 domain sequencing data obtained from pediatric patients to investigate the frequency of VOCs and the relation between the variants and laboratory and clinical data in children.
Materials and methods
Patient selection
This study obtained ethical approval from Tehran University of Medical Sciences, Tehran, Iran (IR.TUMS.CHMC.REC.1400.092).
This study included all cases with SARS-CoV-2-positive nasopharyngeal swabs obtained from patients referred to Children’s Medical Center (CMC), an Iranian referral hospital, between July 2021 and March 2022. CMC is one of the most experienced sub-specialized hospitals in Iran, with nearly 20 specialty and sub-specialty wards and a monthly turnover rate of more than 35,000 outpatients and 2500 inpatients, offer high quality and specialized therapeutic services to neonates, infants and children throughout country.
Inclusion criteria for this study included all patients, regardless of age, who had a positive test anywhere in the hospital setting. Exclusion criteria for the study included those whose data was obtained from non-hospital outpatient settings, or referred from another hospital.
All cases were diagnosed with SARS-CoV-2 infection using a reverse transcription polymerase chain reaction (RT-PCR) assay of nasopharynx specimens, as previously described [10], or with MIS-C according to the Centers for Disease Control and Prevention (CDC) definition [31]. The following variables were collected: patient gender and age, symptoms at admission, comorbidities, severity of disease, laboratory parameters, ICU need, and mortality. All patients’ parents or guardians signed informed consent forms.
A severe COVID-19 diagnosis will require at least one of the following conditions: SpO2 93% (90% in premature infants), PaO2 60 mmHg, PaCO2 > 50 mmHg, a respiratory rate of 70/min (≤ 1 year) and 50/min (more than one year), or lung infiltrates > 50%; respiratory failure demanding respiratory support, septic shock development, or critical organ failure demanding intensive care unit (ICU) care [32]. The lab results were obtained from the patient’s medical records.
Laboratory tests including leukocyte, neutrophil, and lymphocyte counts, hemoglobin, platelet count, C-reactive protein (CRP), erythrocyte sedimentation rates (ESR), d-dimer, blood urea, serum creatinine, liver enzymes, fibrinogen, ferritin, lactate dehydrogenase, creatine phosphokinase, sodium, potassium, calcium, phosphorus, magnesium, albumin, procalcitonin, prothrombin time, partial thromboplastin time, and international normalized ratio, vitamin D, CK-MB, D-dimer, and troponin were assessed using the laboratory reference values.
All symptoms, including COVID-19 symptoms, were documented at the time of admission (e.g., fever, cough, conjunctivitis, shortness of breath, abdominal pain, vomiting or diarrhea, tachypnea, chest pain, headache, myalgia, rash, and seizure).
Molecular reaction After viral RNA extraction using High Pure Viral Nucleic Acid kit (Roche, Germany) according to the manufacturer’s instruction, and cDNA synthesis was accomplished.
using PrimeScript RT reagent kit (taKaRa, Japan) [33]. the cDNAs were subsequently used in routine PCR reactions, utilizing the specific primers targeting RBD domain (RBD_S_F: 5′- GGGCAAACTGGAAAGATTGCTGA-3′; RBD_S_R: 5′-TGTGTACAAAAACTGCCATATTGCA–3′). Amplification was performed in a mixture consisting of 2.5 µl of the 10X PCR buffer, 0.5 µL of 100 mM MgCl2, 2.5 units of Taq DNA polymerase, 0.5 µL of 50 µM dNTP, 0.5 µL of 10 pMol of each primer, 1 µl of cDNA (final concentration 2 ng/µL) and DNase-, RNase-free deionized water to a final volume of 25 µl. Cycling conditions were carried out as follows: initial denaturation at 95º C for 5 min, followed by 30 cycles including denaturation for 45 s at 95º C, annealing for 45 s at 60º C and extension for 45 s at 72º C and a single final extension at 72º C for 5 min. The PCR products were sent to be sequenced by the Sanger protocol (Bioneer, South Korea).
Bioinformatics and statistical analysis
Full-length SARS-CoV-2 gene sequences were obtained from the NCBI GenBank database and the GISAID EpiFlu database (http://www.GISAID.org). This study screened and analyzed genome sequences with mutations in the S protein RBD. MAFFT version 7 online serve with default parameters (https://mafft.cbrc.jp/alignmeloadnt/server/) and BioEdit were used to align the sequences, and the Wuhan-Hu-1 (NC 045512) strain serving as a reference.
The sequencing result was analyzed as a FASTA file using the GISAID software algorithm. SPSS (Statistical Package for the Social Sciences) version 13.0 software was used for statistical analysis (SPSS Inc.). All categorical variables were represented numerically and as percentages. Means, standard deviations, medians, and interquartile ranges were used to describe normally and non-normally distributed data (IQR). To compare normally distributed, non-normally distributed continuous, and categorical variables, parametric tests (t-test and ANOVA), nonparametric tests (Mann–Whitney and Kruskal–Wallis), and the Pearson χ2 test (or Fisher exact test, when necessary) were used, respectively. Significance was considered at p < 0.05.
Results
A total of 87 pediatric cases were included in the present study. The median age of the patients was 3.5 years (range: 8 days to 14 years, IQR: 1-8.12 years). Underlying conditions were found in 28 cases including cardiovascular diseases (n = 9), cerebral palsy (n = 3), esophageal atresia (n = 2); and hydrocephalus, autoimmune encephalitis, autoimmune hepatitis, talasemia major, inflammatory bowel disease, cystic fibrosis, acute lymphocytic leukemia, asthma, cirrhosis, seizure, diabetes, brain tumor, neurodevelopmental disorder, Glanzmann thrombasthenia (n = 1). The proportions of patients requiring ICU admission and respiratory support were 11.5% and 4.3%, respectively. The proportions of individuals with serious COVID-19 illness were 25.3%, and 8 cases (9.2%) had MIS-C. Remdesivir therapy for COVID-19 was reported in 14 patients (16.1%). In this study, the mortality rate was 2.3% (Table 1).
Sequence analysis
Of 87 patients, 5 (5.7%) were determined to be infected with the Alpha variant based on the analysis of the S1 mutations. Also, 53 (60.9%) and 29 (33.3%) cases were infected with Delta and Omicron variants, respectively. Sequence alignment of spike RBD of SARS-CoV-2 variants showed that the alpha variant had 3 common mutations T716I, P681H and A570D, the last one was reported in all 5 patients. The delta type in this study had 4 common mutations namely D614G, T478K, L452R, and 9681R, and the vast majority (51 cases, 96.2%) had all the first three cases and 39 cases had the last mutation (73.6%). While the omicron type had 3 mutations N679K, E484K and Q498R, the first one was common in all 29 cases and the second in 25 cases (about 86%) and the last in about half of the patients with omicron (15 people, 51.7%) reported. It should be noted that all 87 investigated patients had the D614G mutation.
The median days of hospital stay were 5 days (range 1 to 46 days, IQR:3–6 day). The Delta variant showed a higher risk of disease severity compared to other variants (p value = 0.015). The proportions of patients requiring ICU admission during the Delta and Alpha period were higher, but the differences were not statistically significant. The main clinical symptoms include fever (85.9%) and cough (47.6%). Most of the clinical characteristics did not differ between the Alpha, Delta, and Omicron variant-infected patients, as detailed in Table 1.
Fever was common clinical symptoms in all peaks. Gastrointestinal symptoms, including diarrhea and vomiting were the highest symptoms in Alpha variant period.
Among all cases, 13 (15.3%) presented with seizures. The incidence of seizure was higher in patients with Alpha and Omicron infection compared to the Delta group (p value = 0.028). Myalgia was only found in Delta variant-infected patients (7.5%). Respiratory distress was significantly higher in those who infected with Delta variant (p < 0.0001).
Laboratory data did not differ between the variants, except for CRP and troponin levels (Table 2). Although a higher troponin level was found in the Omicron group, it was still in the normal range.
Discussion
Since the onset of the pandemic, SARS-CoV-2 has developed various mutations in different countries, some of which resulted in more virulent and treatment-resistant strains [34]. Mutations in S protein are of great interest since this protein is one of the main targets for drugs and vaccines against SARS-CoV-2. Therefore, continuous monitoring of S protein in each region can provide valuable data for disease prevention and treatment in that country [35]. In this study, we aim to: first, identify the type of the SARS-CoV-2 variant in children with COVID-19 based on the S1 mutations; second, investigate the relationship between the SARS-CoV-2 variant and the clinical features.
Based on the result of this study, most of the children (60.9%) were infected with the Delta variant. The second most dominant variant was Omicron (33.3%), and only a few (5.7%) patients had an Alpha variant infection. No patients were infected with Beta or Gamma variants. However, these data are specific to the time studied, which was between the Delta and Omicron surges in Iran. Among the mutations identified in this study, D614G mutation, which is considered to be a common global mutation, was reported in all samples. Also, in another study in India, it was observed in 81.66% of the sequenced genome [36]. Also, in the study of Dolci et al., a total of 32 children with SARS-CoV-2, half of whom were girls, with an average age of 1.4 years (range: 1 day to 13 years) were included in the study. Amino acid substitution D614G was detected in all isolated viral strains. One Delta and Omicron type was detected in 7 (21.8%) isolates and 1 (3.1%) case, respectively [37].
Our study shows that the laboratory data did not differ between the variants, except for troponin, which was higher in patients with Omicron infection. However, the mean level of troponin was still in the normal range. .
In this study, severe disease, distress, and myalgia were more frequent in Delta-infected patients. Ong et al. conducted a study on 829 patients infected with Alpha, Beta, and Delta variants. Their results showed that there is a possible correlation between the Delta infection and severe COVID-19, increased viral load, and prolonged viral shedding in respiratory samples [38]. In another study by Deng et al., it was shown that mild status is more prevalent with Omicron compared to Delta (50.0% vs. 22.1%, P value < 0.001) [39]. In addition, the result of a study by Wang et al. indicates that first-time infection with Omicron is associated with less severe symptoms compared to first-time infection with Delta [40].
Based on our results, children with an Alpha infection had a higher incidence of diarrhea. Jain et al. [41] compared the clinical symptoms of patients with MIS-C in Children during the first and second surges (original/Alpha) and third surge (Delta). Their results showed that children infected with original/Alpha had a higher incidence of intubation compared to Delta-infected children (16% vs. 0%, p value: 0.009), but gastrointestinal symptoms were not different between the two groups. The lack of difference in gastrointestinal symptoms might be due to the study design since the MIS-C patients mainly present gastrointestinal signs and symptoms [42].
In conclusion, our study enhances the current knowledge concerning the differences between VOCs in the case of signs and symptoms. There were not many differences between the Alpha, Delta, and Omicron variants in laboratory data. However, the analysis of clinical symptoms reveals that Delta is associated with the increased severity of illness, myalgia, and distress, while diarrhea was reported more in Alpha-infected patients. One limitation of our study is a small sample size which can cause missing the statistically significant differences in clinical presentation with VOCs. Further research with larger sample sizes is required to gain a full understanding of the differences in laboratory and clinical data between the VOCs.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
All data is already released and that any accession numbers/web links are available (www.ncbi.nlm.nih.gov/genbank/), and that all web links and accessions allow access to public data. The datasets generated and/or analyzed during the current study are available in MAFFT version 7 online serve with default parameter (https://mafft.cbrc.jp/alignment/server/). Spike amino mutations were analyzed and calculated with BioAider V1.334 using Wuhan-Hu-1 (NC_045512) strain.
Abbreviations
- COVID-19:
-
Coronavirus disease 19
- SARS-CoV-2:
-
Severe acute respiratory syndrome coronavirus 2
- RT-PCR:
-
Reverse Transcription polymerase chain reaction
- MIS-C:
-
Multisystem inflammatory syndrome in children
- NGS:
-
Next-generation sequencing
- VOCs:
-
Variants of concern
- CRP:
-
C-reactive protein
- ESR:
-
Erythrocyte sedimentation rates
References
Wu F, Zhao S, Yu B, Chen Y-M, Wang W, Song Z-G, et al. A new coronavirus associated with human respiratory disease in China. Nature. 2020;579(7798):265–9.
Worldmeter. Coronavirus Disease 2019 (covid-19) Cases [Available from: https://www.worldometers.info/coronavirus/.
Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA. 2020;323(11):1061–9.
Pan L, Mu M, Yang P, Sun Y, Wang R, Yan J et al. Clinical characteristics of COVID-19 patients with digestive symptoms in Hubei, China: a descriptive, cross-sectional, multicenter study. Am J Gastroenterol. 2020;115.
Viner RM, Mytton OT, Bonell C, Melendez-Torres G, Ward J, Hudson L, et al. Susceptibility to SARS-CoV-2 infection among children and adolescents compared with adults: a systematic review and meta-analysis. JAMA Pediatr. 2021;175(2):143–56.
Tsankov BK, Allaire JM, Irvine MA, Lopez AA, Sauve LJ, Vallance BA, et al. Severe COVID-19 infection and pediatric comorbidities: a systematic review and meta-analysis. Int J Infect Dis. 2021;103:246–56.
Preston LE, Chevinsky JR, Kompaniyets L, Lavery AM, Kimball A, Boehmer TK, et al. Characteristics and disease severity of US children and adolescents diagnosed with COVID-19. JAMA Netw open. 2021;4(4):e215298–e.
Dewi R, Kaswandani N, Karyanti MR, Setyanto DB, Pudjiadi AH, Hendarto A, et al. Mortality in children with positive SARS-CoV-2 polymerase chain reaction test: Lessons learned from a tertiary referral hospital in Indonesia. Int J Infect Dis. 2021;107:78–85.
Velásquez SR, Jacques L, Dalal J, Sestito P, Habibi Z, Venkatasubramanian A, et al. The toll of COVID-19 on african children: a descriptive analysis on COVID-19-related morbidity and mortality among the pediatric population in sub-saharan Africa. Int J Infect Dis. 2021;110:457–65.
Mamishi S, Pourakbari B, Mehdizadeh M, Navaeian A, Eshaghi H, Yaghmaei B, et al. Children with SARS-CoV-2 infection during the novel coronaviral disease (COVID-19) outbreak in Iran: an alarming concern for severity and mortality of the disease. BMC Infect Dis. 2022;22(1):1–10.
Riphagen S, Gomez X, Gonzalez-Martinez C, Wilkinson N, Theocharis P. Hyperinflammatory shock in children during COVID-19 pandemic. The Lancet. 2020;395(10237):1607–8.
Toubiana J, Poirault C, Corsia A, Bajolle F, Fourgeaud J, Angoulvant F et al. Kawasaki-like multisystem inflammatory syndrome in children during the covid-19 pandemic in Paris, France: prospective observational study. BMJ. 2020;369.
Verdoni L, Mazza A, Gervasoni A, Martelli L, Ruggeri M, Ciuffreda M, et al. An outbreak of severe Kawasaki-like disease at the italian epicentre of the SARS-CoV-2 epidemic: an observational cohort study. The Lancet. 2020;395(10239):1771–8.
Whittaker E, Bamford A, Kenny J, Kaforou M, Jones CE, Shah P, et al. Clinical characteristics of 58 children with a pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2. JAMA. 2020;324(3):259–69.
Lu I-N, Muller CP, He FQ. Applying next-generation sequencing to unravel the mutational landscape in viral quasispecies. Virus Res. 2020;283:197963.
Kim D, Lee J-Y, Yang J-S, Kim JW, Kim VN, Chang H. The architecture of SARS-CoV-2 transcriptome. Cell. 2020;181(4):914–21. e10.
Saha I, Ghosh N, Maity D, Sharma N, Sarkar JP, Mitra K, Infection. Genet Evol. 2020;85:104457.
Zhang J, Xiao T, Cai Y, Chen B. Structure of SARS-CoV-2 spike protein. Curr Opin Virol. 2021;50:173–82.
Dellicour S, Durkin K, Hong SL, Vanmechelen B, Martí-Carreras J, Gill MS, et al. A phylodynamic workflow to rapidly gain insights into the dispersal history and dynamics of SARS-CoV-2 lineages. Mol Biol Evol. 2021;38(4):1608–13.
Johnson BA, Xie X, Kalveram B, Lokugamage KG, Muruato A, Zou J et al. Furin cleavage site is key to SARS-CoV-2 pathogenesis. BioRxiv. 2020.
Starr TN, Greaney AJ, Hilton SK, Ellis D, Crawford KH, Dingens AS, et al. Deep mutational scanning of SARS-CoV-2 receptor binding domain reveals constraints on folding and ACE2 binding. Cell. 2020;182(5):1295–310. e20.
Team EE. Updated rapid risk assessment from ECDC on the risk related to the spread of new SARS-CoV-2 variants of concern in the EU/EEA–first update. Eurosurveillance. 2021;26(3):2101211.
Leung K, Shum MH, Leung GM, Lam TT, Wu JT. Early transmissibility assessment of the N501Y mutant strains of SARS-CoV-2 in the United Kingdom, October to November 2020. Eurosurveillance. 2021;26(1):2002106.
Makoni M. South Africa responds to new SARS-CoV-2 variant. The Lancet. 2021;397(10271):267.
Faria NR, Mellan TA, Whittaker C, Claro IM, Candido DdS, Mishra S, et al. Genomics and epidemiology of the P. 1 SARS-CoV-2 lineage in Manaus, Brazil. Science. 2021;372(6544):815–21.
Singh J, Rahman SA, Ehtesham NZ, Hira S, Hasnain SE. SARS-CoV-2 variants of concern are emerging in India. Nat Med. 2021;27(7):1131–3.
Viana R, Moyo S, Amoako DG, Tegally H, Scheepers C, Althaus CL, et al. Rapid epidemic expansion of the SARS-CoV-2 Omicron variant in southern Africa. Nature. 2022;603(7902):679–86.
Fibke CD, Joffres Y, Tyson JR, Colijn C, Janjua NZ, Fjell C et al. Spike Mutation Profiles Associated With SARS-CoV-2 Breakthrough Infections in Delta Emerging and Predominant Time Periods in British Columbia, Canada. Front Public Health. 2022:2038.
Ou J, Lan W, Wu X, Zhao T, Duan B, Yang P, et al. Tracking SARS-CoV-2 Omicron diverse spike gene mutations identifies multiple inter-variant recombination events. Signal Transduct Target Therapy. 2022;7(1):1–9.
Mascola JR, Graham BS, Fauci AS. SARS-CoV-2 viral variants—tackling a moving target. JAMA. 2021;325(13):1261–2.
Mamishi S, Movahedi Z, Mohammadi M, Ziaee V, Khodabandeh M, Abdolsalehi MR et al. Multisystem inflammatory syndrome associated with SARS-CoV-2 infection in 45 children: a first report from Iran. Epidemiol Infect. 2020;148.
Mahmoudi S, Mehdizadeh M, Badv RS, Navaeian A, Pourakbari B, Rostamyan M, et al. The coronavirus disease 2019 (COVID-19) in children: a study in an iranian children’s Referral Hospital. Infect drug Resist. 2020;13:2649.
Mamishi S, Esslami GG, Mohammadi M, Abdolsalehi MR, Sadeghi RH, Mahmoudi S, et al. Detection of SARS-CoV-2 antibodies in pediatric patients: an iranian referral hospital-based study. Hum Antibodies. 2021;29(3):217–23.
Toyoshima Y, Nemoto K, Matsumoto S, Nakamura Y, Kiyotani K. SARS-CoV-2 genomic variations associated with mortality rate of COVID-19. J Hum Genet. 2020;65(12):1075–82.
Schrörs B, Riesgo-Ferreiro P, Sorn P, Gudimella R, Bukur T, Rösler T, et al. Large-scale analysis of SARS-CoV-2 spike-glycoprotein mutants demonstrates the need for continuous screening of virus isolates. PLoS ONE. 2021;16(9):e0249254.
Abbasi J. Researchers tie severe immunosuppression to chronic COVID-19 and virus variants. JAMA. 2021;325(20):2033–5.
Dolci M, Signorini L, Cason C, Campisciano G, Kunderfranco P, Pariani E, et al. Circulation of SARS-CoV-2 variants among children from November 2020 to January 2022 in Trieste (Italy). Microorganisms. 2022;10(3):612.
Ong SWX, Chiew CJ, Ang LW, Mak T-M, Cui L, Toh MPH et al. Clinical and virological features of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) variants of concern: a retrospective cohort study comparing B. 1.1. 7 (Alpha), B. 1.351 (Beta), and B. 1.617. 2 (Delta). Clinical Infectious Diseases. 2021.
Deng H, Lin H, Mai Y, Liu H, Chen W. Clinical features and predictive factors related to liver injury in SARS-CoV-2 Delta and Omicron variant-infected patients. Eur J Gastroenterol Hepatol. 2022:101097.
Wang L, Berger NA, Kaelber DC, Davis PB, Volkow ND, Xu R. Comparison of outcomes from COVID infection in pediatric and adult patients before and after the emergence of Omicron. MedRxiv. 2022.
Jain PN, Acosta S, Annapragada A, Checchia PA, Moreira A, Muscal E et al. Comparison of Laboratory and Hemodynamic Time Series Data Across Original, Alpha, and Delta Variants in Patients With Multisystem Inflammatory Syndrome in Children. Pediatr Crit Care Med. 2022:101097.
Walker DM, Tolentino VR. COVID-19: the impact on pediatric emergency care. Pediatr Emerg Med Pract. 2020;17:1–27. (Suppl 6 – 1.
Acknowledgements
We thank all the hospital staff members, especially Ms. Raheleh Ghasemi, for their effort in collecting the information that was used in this study, all the patients who consented to donate their data for analysis, and the medical staff members who are on the front line caring for patients.
Funding
This study was supported by a grant (grant number: 1400-1-149-53238) from Tehran University of Medical Sciences to Professor Setareh Mamishi.
Author information
Authors and Affiliations
Contributions
Shima Mahmoudi, Babak Pourakbari and Setareh Mamishi participated in the research design. Reihaneh H. Hosseinpour Sadeghi performed experimental tests. Sepideh Benvari wrote the first draft of manuscript. Babak Pourakbari, Shima Mahmoudi, Reihaneh Hosseinpour Sadeghi, Mohammad Reza Abdolsalehi, Mohammad Ali Shahbabaie, Fatemeh Jalali, Fatemeh Safari, and Amene Navaeian contributed to data acquisition and data interpretation. Shima Mahmoudi contributed to the statistical analysis and revising of the manuscript. All authors reviewed and approved the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was conducted in accordance with the principles outlined in the Declaration of Helsinki and was approved by the Ethics Committee of Tehran University of Medical Sciences, Tehran, Iran (IR.TUMS.CHMC.REC.1400.092). In addition, informed consent was obtained from the legal guardian of all the subjects.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mahmoudi, S., Pourakbari, B., Benvari, S. et al. Clinical and laboratory features of SARS-CoV-2 variants across multiple rounds of pandemic waves in hospitalized children in an Iranian referral hospital. BMC Pediatr 23, 241 (2023). https://doi.org/10.1186/s12887-023-04042-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-023-04042-w