
Abstract
Background
The cut-off date in the education system causes a relative age difference, with developmental advantages for children who are born on the “early side” of the cut-off date and disadvantages for those born later, which is known as the relative age effect (RAE). Very few studies have examined whether there is a RAE on the development of fundamental movement skills (FMSs) in preschool children, and no studies have been conducted in China. The purpose of this study is to identify whether a RAE exists on FMS in Chinese preschool children, comparing RAEs according to gender and age.
Methods
From a total of 378 invited preschool children regularly registered at one Chinese kindergarten, a total of 288 healthy and typically developing preschoolers (4.33 ± 0.84 years-old; 56.6% boys) were included in this study. All children were required to take part in anthropometry and FMS assessments. Analysis of covariance (ANCOVA) was applied to examine the difference in each of the FMS items across quarter categories, year and gender groups, controlling for body mass index (BMI).
Results
For the overall sample, the data show the significant main effects on the quarter of birth factor in locomotor skills (LC; F (3, 265) = 2.811, p = 0.04, ηp2 = 0.031), object control skills (OB; F (3, 265) = 6.319, p = 0.04, ηp2 = 0.031), and total test score (TTS; F (3, 265) = 5.988, p = 0.001, ηp2 = 0.063). There were also significant differences in the age effect on all the domains of FMS (FLC (2, 265) = 100.654, p < 0.001, ηp2 = 0.432; FOB (2, 265) = 108.430, p < 0.001, ηp2 = 0.450; FTTS (2, 265) = 147.234, p < 0.001, ηp2 = 0.526) but a gender effect only in LC (F (1, 265) = 20.858; p < 0.001; ηp2 = 0.073). For gender and quarter of birth groups, RAEs in LC only exists in girls. Moreover, regarding age and quarter of birth factors, RAEs are only found at younger ages.
Conclusions
This study suggests the existence of RAEs in the FMS of Chinese preschool children. Teachers need to be aware of the effect of RAEs on the FMS when approaching development, evaluation, and teaching approaches in preschools.
Similar content being viewed by others


Background
To ensure equal education, school systems specify cut-off dates for entry to each grade, to provide a more adequate and uniform educational process for all [1, 2]. The Chinese education system generally sets 31 August as the deadline for a grade to enroll. However, age groupings that impose cut-off dates promote relative age differences. There is an age difference of almost 12 months between the oldest and youngest participants in any age group [3, 4]. This variation among children grouped in the same cohort is commonly referred to as the “relative age” and its subsequent implications are known as the “relative age effect (RAE)” [5, 6]. Earlier studies have shown that young people who demonstrated an eminent performance tended to be born early in their birth year [7, 8]. Subsequent research has shown that the relationship between RAEs and academic performance appears consistent across subjects, with early RAEs appearing to persist throughout education [5, 9, 10].
Theoretical support for the existence of RAEs rests on the Maturation-selection hypothesis, the Matthew effect (the rich get richer and the poor get poorer), the Pygmalion effect (the greater the expectation placed on an individual is, the greater the result that individual will attain), and the Galatea effects (once expectations are placed upon an individual, that individual typically acts congruently with those expectations) [11, 12]. In this regard, relatively older children have maturational, physical, cognitive and emotional advantages over their younger peers within the same age group [2, 4]. The potential biases in evaluation, selection and accrued exercise experiences may negatively affect younger children in the same age group [13]. Worryingly, however, it was observed that students disadvantaged by RAE were disproportionately referred for psychiatric support and generally exhibited greater health problems [14, 15]. Thompson found that the most disturbing consequence of RAEs was that those born later in the year had a higher suicide rate than their earlier-born peers. RAEs were identified as a new factor in suicide among young people [16]. Morrow and Navarro found that RAEs were a risk factor for attention deficit hyperactivity disorder (ADHD) and developmental coordinator disorder (DCD) [17, 18].
Physical Education (PE) is an important part of education that plays critical role in the lifelong development of children. Motor development is one of the goals of PE and a critical element of quality PE classes [2, 19]. PE classes must provide all children with the acquisition of sufficient motor competence to be able to access a wide range of physical-sport activities throughout their lives [6]. Acquiring adequate motor competence during childhood is essential for a child’s physical, socioemotional, and cognitive development[18]. Lack of motor competence can have lasting negative effects, such as developmental delay [18, 20, 21]. In particular, preschool-age children are particularly sensitive; thus, this period is fundamental for the development of motor competence. For preschool children, the learning and acquisition of fundamental movement skills (FMSs) is essential for the development of motor competence [2, 22]. FMS is defined as basic learned movement patterns that do not occur naturally and are suggested to be foundational for more complex physical and sporting activities, including locomotor, object control, and stability skills [23]. These FMS are important to young children because proficiency in FMS is associated with various behaviour and health benefits [24] that can continue to adolescence and adulthood [25].
Regarding FMS, physical maturity may give older children an advantage that is mistaken for superior ability. To date, very few studies have examined whether there is a RAE on the development of FMS in preschool children. To the author’s knowledge, there are no studies on the RAE of FMS in preschool children in China. Navarro-Patón [2] found that a RAE was present among 4-year-old children but not 5-year-old children. However, in another study, Navarro-Patón [26] found that RAEs were present in aiming and catching, balance, and total test scores among 5-year-old children. Meanwhile, Imamoglu [27] only found RAEs in boys’ leap and girls’ side gallop skills in different age groups of 5 to 6-year-old children. In addition, the findings on RAE of FMS are inconclusive, as some researchers indicate that children born in the first quarter of the year or near the cut-off date have better motor competence [2, 3, 6, 26, 28], and others indicate the inverse results [29]. The evidence from current studies is too weak to support the consistent findings regarding RAEs on FMS. These ambiguous results may be due to individual differences in the development of motor competence resulting from age and gender effects [3, 30]. Given that preschool children acquire FMS through quality instruction, feedback and encouragement, which typically occur in PE settings, examining whether RAEs influences the performance of FMS is important [31,32,33]. Clarifying the role of RAEs in FMS could provide evidence and teaching strategies in response to the consequences of lower relative age, avoiding unconscious bias in teaching and evaluation and maximizing children’s movement potential [6, 28].
As a consequence, the following research questions are formulated: Are there any differences in FMS proficiency levels among preschool children according to the quarter of birth, age, and gender? Does a RAE exist in the FMS of children of different genders and ages? Based on the above, the purpose of this study is to investigate RAEs on the FMS of preschool children from China (Shanghai), and we hypothesized that FMS, measured by the Test of Gross Motor Development-2nd edition (TGMD-2) [34], would be higher in preschool children born in the early quarter of the school years than in those born in the later quarter.
Methods
Study design and participants
For the development of this research, a cross-sectional study was conducted in Yangpu District, Shanghai, China. The variables of FMS were the dependent variables, and the quarter of birth was the independent variable, with children compared according to gender and age.
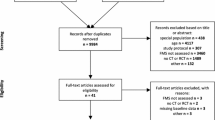
This study focuses on preschool children with typical motor development. Children with physical and intellectual disorders that affect motor development were excluded from this study. A total of 378 healthy preschool children (3–5 years) regularly registered at one kindergarten was invited to participate in this study. Of these, 355 participants and their parents consented to participate by signing an informed consent document, while others declined for personal reasons (participation rate: 93.9%). Ultimately, 288 participants completed the study assessment and provided a valid date of birth.
Procedures and assessments
All participants were required to participate in anthropometric assessments including measurements of weight and height. Weight (kg) and height (cm) were assessed without shoes and with the participants wearing lightweight clothes. Height (in centimeter) and body mass (in kilograms) were recorded to the nearest centimeter and 100 g, respectively, using a stadiometer (Jianmin CVS5, Beijing, China) and electronic weighing scales (Jianmin CVS5, Beijing, China) from which body mass index (BMI) was calculated (kg/m2). All anthropometric measures were taken twice but not consecutively. The average value of the two measurements was used in the analyses.
Prior to the FMS assessment, each participant was required to participate in a warm-up (approximately 6 min) organized by one research staff member. FMS assessment was administered using the TGMD-2 by trained research students. The TGMD-2 is a widely used assessment for children aged 3–10 years [34, 35]. Specifically, the TGMD-2 consists of two domains: locomotor (run, jump, leap, hop, gallop and slide) and object control (overarm throw, stationary strike, kick, catch, underhand roll and stationary dribble). Participants completed the test in a group (5–8 children) in kindergarten playgrounds. One trained research staff member provided a silent demonstration of the skill to be tested to the participants before the formal test. All children performed a familiarization trial of each skill followed by two performance trials, as recommended in the TGMD-2 handbook, taking approximately 45–55 min per group [34]. Children’s performances on each skill were videotaped for assessment.
During the two trials for each skill, components were marked as being absent (scored 0) or present (scored 1), with the exception of three skills. For the throw and strike hip/trunk rotation was scored as differentiation (2), block (1) or no rotation (0), whilst the catch identified a successful attempt as being caught cleanly with hands/fingers (2) or trapped against body/chest (1). The FMS comprehensive score was obtained by adding the test results of two tests of all skill components. Meanwhile, the scores of the locomotor and object-control were calculated as the sum of the skill scores in each subscale. All analyses were completed by a single trained assessor. Two independent raters completed the assessment, and the interrater reliability (intraclass coefficient, ICC) of 12 skills ranged from 0.41 to 0.72.
Relative age effect (RAE)
Participants’ information was retrieved from the individual profile archive of the kindergarten and information on birthdate, including birth year, month and day. Therefore, based on the birth year, participants were divided into three age groups: 3 years old, 4 years old and 5 years old. Furthermore, within each year group and based on the birthdate, 4 quarter groups were created based on China’s kindergarten registration/enrolment policy (starting at the school year cut-off date of 31 August). Commensurate with recent work by Sandercock et al. [36], Birch et al. [28] and Jarvis[13], the year was divided into quarters (labelled: Q1, Q2, Q3, and Q4), with quarter 1 (Q1) corresponding to the period of 1 September through 30 November, quarter 2 (Q2) from 1 December to 30 February, quarter 3 (Q3) from 1 March to 31 May, and quarter 4 (Q4) from 1 June to 31 August.
Statistical analysis
Differences in each of the FMS items across quarter categories, year group (3 years, 4 years, 5 years) and gender were examined using a series of analyses of covariance (ANCOVAs) controlling for BMI [28]. A post hoc analysis using least significance difference (LSD) adjustments was performed where any significant interactions and main effects were found. The effect size was calculated by partial eta squared (ηp2), and small, moderate and large effects corresponded to values equal to or greater than 0.001, 0.059, and 0.138, respectively [37]. Statistical analysis was performed using SPSS 26.0 (IBM, Chicago, IL, USA). p < 0.05 was considered to indicate significance.
Results
A total of 288 healthy preschool children (mean age of 4.33 years old (± 0.84)) were evaluated, of which 163 (56.6%) were boys and 125 (43.4%) were girls. Sixty-seven children were 3 years old, 102 were 4 and 119 were 5. The distribution of the participants was as follows: quarter 1 [n = 48 (16.7%)], quarter 2 [n = 78 (27.1%)], quarter 3 [n = 79 (27.4%)] and quarter 4 [n = 83 (28.8%)]. Table 1 shows the frequencies of preschool children based on gender, age and the quarter of birthdate.
The results of the ANCOVA regarding locomotor skills (LC), object control skills (OB), and total test score (TTS) indicate a significant main effect of the birthdate quarter (FLC (3, 265) = 2.811, p = 0.04, ηp2 = 0.031; FOB (3, 265) = 6.319, p = 0.04, ηp2 = 0.031; FTTS (3, 265) = 5.988, p = 0.001, ηp2 = 0.063), with LC and TTS scores being higher in those born in the first quarter (Fig. 1). For the age factor, main effects were found for LC, OB, and TTS, with higher scores in 5-year-old preschool children (FLC (2, 265) = 100.654, p < 0.001, ηp2 = 0.432; FOB (2, 265) = 108.430, p < 0.001, ηp2 = 0.450; FTTS (2, 265) = 147.234, p < 0.001, ηp2 = 0.526) (Fig. 2). However, for the gender factor, a main effect in the gender effect is only found by LC, with higher scores in girls (F (1, 265) = 20.858; p < 0.001; ηp2 = 0.073) (Fig. 3).

Quarter of birth according to skill scores. LC: Locomotor skills; OB: Object control skills; TTS: Total test score. Note: * p < 0.05 different between quarters; ** p < 0.001 different between quarters

Total skill scores according to age. LC: Locomotor skills; OB: Object control skills; TTS: Total test score. Note: ** p < 0.001 different between quarters

Total skill scores according to gender. LC: Locomotor skills; OB: Object control skills; TTS: Total test score. Note: ** p < 0.001 different between boys and girls; nsp > 0.05 no significant differences
Regarding the comparison by pairs, for gender (Table 2), regarding the LC, significant differences were found between boys and girls in quarters 1 (p = 0.007) and 2 (p = 0.032), with higher scores in girls. Regarding the age group (Table 3), in terms of LC, OB, and TTS, statistically significant differences were also found between 3-, 4-, and 5-year-old, with 5-year-old children demonstrating an advantage in each quarter.
In the pairwise analysis based on the quarter of birth (Table 2), regarding the LC, only a significant difference was found in total preschool children between Q1 and Q4 (Q1 > Q4, p = 0.018). In the OB, differences were found between those born in Q1 vs. Q4 (Q1 > Q4, p = 0.029), Q2 vs. Q4 (Q2 > Q4, p = 0.008) and Q3 vs. Q4 (Q3 > Q4, p = 0.014). In the TTS, significant differences were found between Q1 and Q4 (Q1 > Q4, p = 0.007), Q2 and Q4 (Q2 > Q4, p = 0.007) and Q3 and Q4 (Q3 > Q4, p = 0.041).
In the pairwise analysis based on gender and the quarter of birth (Table 2), regarding the LC, significant differences were only found in girls between Q1 and Q4 (Q1 > Q4, p = 0.004); and between Q1 and Q3 (Q1 > Q3, p = 0.028). Regarding the OB of girls, differences were found between those born in Q3 vs. Q4 (Q3 > Q4, p = 0.049), and boys were significantly different between Q2 vs. Q4 (Q2 > Q4, p = 0.008). In the TTS, significant differences were found in girls between Q1 and Q4 (Q1 > Q4, p = 0.008), and differences were found in boys between Q2 and Q4 (Q2 > Q4, p = 0.031).
In the pairwise analysis based on age and the quarter of birth (Table 3), regarding the LC, significant differences were only found in 4-year-old preschool children between Q1 and Q2 (Q1 > Q2, p = 0.009). In the OB of 3-year-old preschool children, there were significant differences between Q2 and Q4 (Q2 > Q4, p = 0.027). In 4-year-olds, there were significant differences between Q1 and Q2 (Q1 > Q2, p = 0.011) and between Q1 vs. Q3 (Q1 > Q3, p = 0.008). In the TTS, significant differences were found in 3-years-old preschool children between Q2 vs. Q4 (Q2 > Q4, p = 0.026). In 4-years-olds, there are significant differences between Q1 vs. Q2 (Q1 > Q2, p = 0.001), and between Q1 and Q3 (Q1 > Q3, p = 0.009).
Discussions
This study is the first to evaluate the RAE on FMS in preschool children in China. We hypothesized that LC, OB and TTS, as measured by the TGMD-2, would be higher in preschool children born from September to November (Quarter 1) of the previous year than in those born from June to August (Quarter 4).
Our results show that a RAE exists in every skill domain studied (i.e., LC, OB and TTS). TTS improves as relative age increases in preschool children, as those who were born in the first quarter obtained higher scores than those born in the second, third and fourth quarters. In LC and OB tests, the differences between the quarters of birthdate were significant. This is not in agreement with the findings Imamoglu’s study [27] but coincides with the results of present studies on motor competence [2, 3, 26]. This result may be because motor competence improves as children biologically mature and grow [2, 38]. Additionally, relatively older children are likely to be physically stronger, have greater skill development experience and to be more psychologically mature than relatively younger children, which is a consequence of being born at different times within the school year [4, 39]. In fact, scientific evidence reports better skill performance and physical fitness among older children than in their younger counterparts [2, 40].
The data obtained in our research indicate no statistically significant differences between boys and girls in TTS and OB, but significant differences between Q1 and Q2 were found in LC. Overall, girls’ TTS scores were is higher than boys’ scores, except for in Q2. Except for in Q3, the OB score of boys was generally higher than that of girls. Regarding LC, girls scored higher than boys, although the gender difference was not significant in Q3 and Q4. This observation could be related to gender differences and skill characteristics. Girls can perform better in LC than boys due to the types of activities, opportunities and options presented at this age group [35]. Girls often prefer to participate in more diverse physical activities, such as dancing, aerobics and rhythmic gymnastics [13, 28]. Boys tend to gain greater exposure to object control skills than girls and typically receive greater encouragement, support, opportunities in PE and participate in sports at home, in school and in the broader community [13]. The influence of gender on LC, OB and TTS is inconclusive, particularly among young children. Some studies have shown that report boys perform better on TTS, especially on OB [41, 42], while others indicate that gender is unrelated to TTS [43]. Nonetheless, our findings should be interpreted cautiously as children present substantial TTS variabilities, even at young ages.
Regarding the gender and quarter of the birth groups, a RAE is only found in LC among the girls. The possible reasons for this phenomenon are as follows: due to the type of stereotyped activities or gender role models [28], girls are more likely to participate in LC activities. Based on the Pygmalion effect [12, 44], teachers and parents unconsciously and mistakenly have higher expectations for relatively older girls through physical maturity in LC, which may manifest as RAEs. Boys often prefer to participate in sports related to object control skills, such as basketball and soccer [13]. In general, teachers’ and parents’ expectations of boys are relatively lower regarding LC, and the Pygmalion effect does not seem to be present in boys. In addition, the Garratt effect further indicates that once children are under high expectations, they will usually conform to these expectations by adopting measures such as hard practice and increasing practice time to reflect their self-belief in their high potential [44]. Thus, girls have RAEs in LC skills, but boys do not. Nonetheless, our explanation may not be strongly compelling owing to some uncontrollable factors, such as study design. Further research is needed to explain and refine the findings.
Furthermore, the data presented in the current study indicate that statistically significant age differences are found between 3-, 4-, and 5-year-old children in LC, OB and TTS. Thus, FMS improves as the age of the group advances. The age differences reported in the present study are congruent with those reported elsewhere [45,46,47]. Moreover, the presence of RAEs was found in both the OB and TTS of 3- and 4-year-old children but only in the LC of 4-year-olds. LC plays a more basic role in FMS and is the most basic ability for all children to participate in sports. Meanwhile, based on the phases and stages of motor development [48], those 2–3 years of age are at the initial stage of FMS, the LC is at a relatively low level, and the difference between children in different birthdate quarters is not obvious. Therefore, RAEs have not yet appeared in the LC of 3-year-old children. Our main results suggest that RAE is not present in 5-year-old children. This is in agreement with Navarro-Patón’s studies in which RAE was significant among 4-year-old but not 5-year-old children[2]. The possible reason for this is that younger children’s physical development changes quickly and greatly [4]. In fact, some researchers have found that in preschoolers, 3-month difference in birthdate time can account for up to 8% of their life, while in 11-year-olds it accounts for approximately 2% [4, 49]. Based on Seefeldt’s Windows Barrier theory[50], this effect may be because children reach the maturity plateau of FMS at this age. Therefore, the birthdate quarter difference is more prominent in the younger age group, and RAEs are more likely to occur. It also seems that the RAE on FMS does not exist at age 5, possibly because of the ‘proficiency barrier’, but further research is warranted to verify this observation. This finding also indicates that the development of FMS is of great importance in early childhood. As long as the proficiency barrier is broken, specialized skills can be better developed. The guidance of FMS and the creation of a motor development–conducive environment for children should be strengthened in preschool.
Our research emphasizes that preschool children grouped in the same class year may demonstrate different FMS levels within a period as short as one quarter (3 months), particularly among younger children. The results of this study contribute to the understanding that the cut-off age is an important factor in the acquisition of skills in all areas of children’s development (physical, motor, cognitive, etc.) [14, 51]. The presence of RAEs must be individually considered and compensated for in the sports needs of preschoolers, as younger students may achieve the same level as their older peers in the future[52]. The key issue is that children may demonstrate different levels of FMS in the same grade simply because they are relatively younger. Teachers need to approach comparisons of FMS in preschoolers in the same grade with caution.
From the perspective of motor development, RAE should be considered when teaching and evaluating preschool children in the same school year, for example, grouping preschool children according to their biological and nonchronological age, and applying corrective adjustments to PE assessments with relative age [2, 6]. Furthermore, physical education sessions should be designed and implemented based on children’s motor competence levels, and personalized teaching strategies should be established [3]. There is also a need to pay attention to the learning participation of children at relatively younger ages. All children can learn how to move and experience the enjoyment of moving to ensure lifelong engagement. One approach to achieving this is to adopt a mastery motivational climate in physical education settings, which has shown great promise with respect to motivating children to learn their FMS [53, 54].
Study limitations
Although the current study is the first to investigate the RAE on FMS in preschool children, especially in a Chinese sample, some inherent limitations should be mentioned in explaining our research findings. One major concern is that the cross-sectional study design used in our study cannot establish the true cause-and-effect association between the RAE and FMS. Another limitation is the relatively small sample size, as the study was is restricted to one Chinese preschool, and specific context bias cannot be disregarded. Moreover, the absence of children born in the first quarter in the 3-year-old sample is another limitation; thus, the generalizability of the research findings might be limited. The third limitation is that this study does not account for maturity variables as covariates. Thus, we cannot exclude bias in the research findings. Future studies are encouraged to address these limitations and obtain more robust evidence for the relationship between RAEs and FMS in early childhood.
Conclusions
RAEs have a significant effect on FMS in Chinese preschool children. Those children born in Q1 achieve better scores in FMS than those born in Q4 (i.e., LC, OB and TTS). Meanwhile, we found that RAEs in the LC only exist in girls, RAEs in the OB mainly exist in boys, and RAEs are more likely to occur in younger-age preschool children. Further studies are encouraged to explore the relative age effect on FMS in Chinese preschool children by gender and school grade. Moreover, more interventions and longitudinal studies may be needed to clarify and reduce RAEs on FMS in preschool children.
Data Availability
The datasets analyzed in this study are available from the corresponding author on reasonable request.
Change history
27 April 2023
A Correction to this paper has been published: https://doi.org/10.1186/s12887-023-04002-4
Abbreviations
- RAE:
-
Relative Age Effect
- FMS:
-
Fundamental Movement Skill
- LC:
-
Locomotor skills
- OB:
-
Object control skills
- TGMD-2:
-
Test of Gross Motor Development-2nd edition
- BMI:
-
Body Mass Index
- Q1:
-
Quarter 1
- Q2:
-
Quarter 2
- Q3:
-
Quarter 3
- Q4:
-
Quarter 4
- ANCOVA:
-
Analysis of covariance
- SEM:
-
Standard Error of Mean.
References
Gutierrez D. Review of relative age effects and potential ways to reduce them in sport and education. Retos Nuevas tendencias en Educación Física, Deporte y Recreación 2013, 23:51–63.
Navarro-Paton R, Mecias-Calvo M, Fernandez JER, Arufe-Giraldez V. Relative Age Effect on Motor Competence in Children Aged 4–5 Years.Children-Basel2021, 8(2).
Navarro Paton R, Arufe-Giráldez V, Sanmiguel-Rodríguez A, Mecías M. Differences on Motor Competence in 4-Year-Old Boys and Girls Regarding the Quarter of Birth: Is There a Relative Age Effect? Children 2021, 8:141.
Cupeiro R, Rojo-Tirado M, Cadenas-Sanchez C, Artero E, Peinado A, Labayen I, Dorado C, Arias N, Moliner-Urdiales D, Vidal-Conti J, et al. The relative age effect on physical fitness in preschool children. J Sports Sci. 2020;38:1–10.
Aune TK, Ingvaldsen R, Vestheim O, Bjerkeset O, Dalen T. Relative Age Effects and Gender Differences in the National Test of Numeracy: A Population Study of Norwegian Children.Frontiers in Psychology2018,9.
Mecias-Calvo M, Arufe-Giraldez V, Cons-Ferreiro M, Navarro-Paton R. Is It Possible to Reduce the Relative Age Effect through an Intervention on Motor Competence in Preschool Children?Children-Basel2021, 8(5).
Pintner R, Forlano G. The birth month of eminent men. J Appl Psychol. 1934;18:178–88.
Musch J, Grondin S. Unequal competition as an impediment to Personal Development: a review of the relative age effect in Sport. Dev Rev. 2001;21:147–67.
Massey A, Elliott G, Ross E. Season of birth, sex and success in GCSE English, mathematics and science: some long-lasting effects from the early years? Res Papers Educ. 1996;11:129–50.
Aune TK, Pedersen A, Ingvaldsen R, Dalen T. Relative Age Effect and Gender Differences in Physical Education Attainment in Norwegian Schoolchildren.Scandinavian Journal of Educational Research2016,61.
Hancock D, Adler A, Côté J. A proposed theoretical model to explain relative age effects in sport. Eur J sport Sci. 2013;13:630–7.
Langham-Walsh E, Gottwald V, Hardy J. Relative age effect? No “flipping” way! Apparatus dependent inverse relative age effects in elite, women’s artistic gymnastics. PLoS ONE. 2021;16:e0253656.
Jarvis S, Rainer P, Ganesh S. Fundamental Movement Proficiency of Welsh Primary School Children and the Influence of the Relative Age Effect on Skill Performance - Implications for Teaching. Education 3–13 2022.
Dutil C, Tremblay M, Longmuir P, Barnes J, Belanger K, Chaput J-P. Influence of the relative age effect on children’s scores obtained from the Canadian assessment of physical literacy.BMC Public Health2018,18.
Goodman R, Gledhill J, Ford T. Child psychiatric disorder and relative age within school year: Cross sectional survey of large population sample. BMJ (Clinical research ed). 2003;327:472.
Thompson A, Barnsley R, Dyck R. A new factor in youth suicide: the relative age effect. Can J psychiatry Revue canadienne de psychiatrie. 1999;44:82–5.
Morrow RL, Garland EJ, Wright JM, Maclure M, Taylor S, Dormuth CR. Influence of relative age on diagnosis and treatment of attention-deficit/hyperactivity disorder in children. CMAJ. 2012;184(7):755–62.
Navarro Paton R, Pueyo Villa S, Martín Ayala J, Martí M, Mecías M. Is quarter of Birth a risk factor for developmental coordinator disorder in Preschool Children? Int J Environ Res Public Health. 2021;18:5514.
Bund A, Scheuer C. Changes in Childhood and Adolescence: Current Challenges for Physical Education. 2017.
Roth K, Ruf K, M O, Ahnert SM, Schneider J, Joisten W, Formerly Graf C, Hebestreit H. Is there a secular decline in preschool children? Scand J Med Sci Sports. 2009;20:670–8.
Gabbard C. Lifelong Motor Development, 8th edition; 2021.
Clark J, Metcalf JS. The Mountain of Motor Development: A Metaphor.Motor Development: Research and Review: Vol 22002:62–95.
Barnett L, Stodden D, Cohen K, Smith J, Lubans D, Lenoir M, Iivonen S, Miller A, Laukkanen A, Dudley D et al. Fundamental Movement Skills: An Important Focus.Journal of Teaching Physical Education2016,35.
Lubans D, Morgan P, Cliff D, Barnett L. Fundamental Movement Skills in children and adolescents. Sports Med (Auckland NZ). 2010;40:1019–35.
Robinson L, Stodden D, Barnett L, Lopes V, Logan S, Rodrigues L, D’Hondt E. Motor Competence and its Effect on Positive Developmental Trajectories of Health.Sports medicine (Auckland, NZ)2015,45.
Navarro-Paton R, Lago-Ballesteros J, Arufe-Giraldez V, Sanmiguel-Rodriguez A, Lago-Fuentes C, Mecias-Calvo M. Gender Differences on Motor Competence in 5-Year-Old Preschool Children Regarding Relative Age.International Journal of Environmental Research and Public Health2021, 18(6).
İmamoğlu M, Ziyagil M. The role of relative age effect on fundamental movement skills in boys and girls. 2017, 4:84.
Birch S, Cummings L, Oxford SW, Duncan MJ. EXAMINING RELATIVE AGE EFFECTS IN FUNDAMENTAL SKILL PROFICIENCY IN BRITISH CHILDREN AGED 6–11 YEARS. J strength conditioning Res. 2016;30(10):2809–15.
Lopes V, Silva R, Seabra A, Morais F. Estudo do nível de desenvolvimento da coordenação motora da população escolar (6 a 10 anos de idade) da Região Autónoma dos Açores. Revista Portuguesa de Ciências do Desporto 2003, 2003.
Kokštejn J, Musalek M, Tufano J. Are sex differences in fundamental motor skills uniform throughout the entire preschool period?PLoS ONE2017,12.
Wainwright NN, Goodway JD, John AA, Edwards KA, Piper KA. Examining the impact of SKIP training for teachers on children’s motor development in the Foundation Phase. J Sport Exerc Psychol. 2017;39:101–S102.
Brian A, Goodway JD, Logan JA, Sutherland S. SKIPing with teachers: an early years motor skill intervention. Phys Educ Sport Pedagogy. 2017;22(3):270–82.
Brian A, Goodway JD, Logan JA, Sutherland S. SKIPing with Head Start Teachers: influence of T-SKIP on object-control skills. Res Q Exerc Sport. 2017;88(4):479–91.
Ulrich DA. Test of gross motor development-2. 2000.
Bolger LE, Bolger LA, O’Neill C, Coughlan E, O’Brien W, Lacey S, Burns C, Bardid F. Global levels of fundamental motor skills in children: a systematic review. J Sports Sci. 2021;39(7):717–53.
Sandercock G, Taylor M, Voss C, Ogunleye A, Cohen D, Parry D. Quantification of the Relative Age Effect in Three Indices of Physical Performance.Journal of strength and conditioning research / National Strength & Conditioning Association2013,27.
Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Lawrence Erlbaum Associates, Publishers.; 1988.
Cadenas-Sanchez C, Martínez-Téllez B, Sánchez-Delgado G, Mora-Gonzalez J, Castro-Piñero J, Löf M, Ruiz J, Ortega F. Assessing physical fitness test in preschool children: feasibility, reliability and practical recommendations for the PREFIT battery.Journal of Science and Medicine in Sport2016,19.
Helsen W, Winckel J, Williams A. The relative age effect in youth soccer across Europe. J Sports Sci. 2005;23:629–36.
De Miguel-Etayo P, Gracia-Marco L, Ortega F, Intemann T, Foraita R, Oja L, Barba G, Michels N, Tornaritis M, Molnár D, et al. Physical fitness reference standards in european children: the IDEFICS study. Int J Obes. 2014;38(Suppl 2):57–66.
Barnett L, Beurden E, Morgan P, Brooks L, Beard J. Gender differences in Motor Skill Proficiency from Childhood to Adolescence: a longitudinal study. Res Q Exerc Sport. 2010;81:162–70.
Iivonen S, Sääkslahti AK. Preschool children’s fundamental motor skills: a review of significant determinants. Early Child Development and Care. 2014;184(7):1107–26.
Barnett L, Hinkley T, Okely AD, Salmon J. Child, family and environmental correlates of children’s motor skill proficiency. J Sci Med Sport. 2013;16(4):332–6.
Wattie N, Schorer J, Baker J. The Relative Age Effect in Sport: A Developmental Systems Model.Sports medicine (Auckland, NZ)2014, 45.
Saraiva L, Rodrigues L, Cordovil R, Barreiros J. Influence of age, sex and somatic variables on the motor performance of pre-school children.Annals of human biology2013,40.
Livesey D, Coleman R, Piek J. Performance on the Movement Assessment Battery for children by australian 3- to 5-year-old children. Child Care Health Dev. 2007;33:713–9.
Ecevit R, Şahin M. RELATIONSHIP BETWEEN MOTOR SKILLS AND SOCIAL SKILLS IN PRESCHOOL CHILDREN.European Journal of Education Studies2021,8.
Goodway JD. Understanding Motor Development: Infants, Children, Adolescents, Adults (8th ed.). 2020.
Cobley S, Abraham C, Baker J. Relative age effects on physical education attainment and school sport representation. Phys Educ Sport Pedagogy. 2008;13:267–76.
Brian A, Getchell N, True L, De Meester A, Stodden DF. Reconceptualizing and Operationalizing Seefeldt’s proficiency barrier: applications and future directions. Sports Med. 2020;50(11):1889–900.
Khajooei M, Wochatz M, Baritello O, Mayer F. Effects of shoes on children’s fundamental motor skills performance. Footwear Sci. 2020;12(1):55–62.
Navarro J-J, García J, Olivares P. The relative age effect and its influence on academic performance. PLoS ONE. 2015;10(10):e0141895.
Johnson JL, Rudisill ME, Hastie P, Wadsworth D, Strunk K, Venezia A, Sassi J, Morris M, Merritt M. Changes in Fundamental Motor-Skill performance following a Nine-Month Mastery Motivational Climate intervention. Res Q Exerc Sport. 2019;90(4):517–26.
Kelly L, Connor S, Harrison A, Ni Cheilleachair N. Effects of an 8-week school-based intervention programme on Irish school children’s fundamental movement skills.Physical Education and Sport Pedagogy2020,26.
Acknowledgements
Thanks, are sincerely given to all the preschool children, parents and teachers at the participating schools for their excellent cooperation during the data collection.
Funding
This study is supported by grants from the Shanghai Science and Technology Planning Project (No.21010503700) and Shanghai Key Laboratory of Human Performance (Shanghai University of Sport, No.11DZ2261100).
Author information
Authors and Affiliations
Contributions
KL contributed to data analysis and writing the manuscript. YC and SC originated the research idea supervised data collection and critically reviewed the manuscript. SL and XS contributed to collecting data. JM, CM and MD contributed to critically reviewed the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study survey was also approved by Institution of Review Board at Shanghai University of Sport. Procedures performed in studies were in accordance with national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. All the children and their parents voluntarily participated in this study with the parent’s signed informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, K., Chen, S., Ma, J. et al. The relative age effect on fundamental movement skills in Chinese children aged 3–5 years. BMC Pediatr 23, 150 (2023). https://doi.org/10.1186/s12887-023-03967-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-023-03967-6