
Abstract
Background
The breastfeeding rate in China is lower than that in many other countries and the extent of adoption of the “Feeding Recommendations for Preterm Infants and Low Birth Weight Infants” guideline in NICUs remains unclear.
Method
A web-based survey about the current status of human milk feeding and enteral feeding practices at NICUs was sent to all China Neonatal Network’s cooperation units on September 7, 2021, and the respondents were given a month to send their responses.
Results
All sixty NICUs responded to the survey, the reply rate was 100%. All units encouraged breastfeeding and provided regular breastfeeding education. Thirty-six units (60.0%) had a dedicated breastfeeding/pumping room, 55 (91.7%) provided kangaroo care, 20 (33.3%) had family rooms, and 33 (55.0%) routinely provided family integrated care. Twenty hospitals (33.3%) had their own human milk banks, and only 13 (21.7%) used donor human milk. Eight units (13.3%) did not have written standard nutrition management guidelines for infants with body weight < 1500 g. Most units initiated minimal enteral nutrition with mother’s milk for infants with birth weight ˂1500 g within 24 h after birth. Fifty NICUs (83.3%) increased the volume of enteral feeding at 10–20 ml/kg daily. Thirty-one NICUs (51.7%) assessed gastric residual content before every feeding session. Forty-one NICUs (68.3%) did not change the course of enteral nutrition management during drug treatment for patent ductus arteriosus, and 29 NICUs (48.3%) instated NPO for 1 or 2 feeds during blood transfusion.
Conclusion
There were significant differences in human milk feeding and enteral feeding strategies between the NICUs in CHNN, but also similarities. The data obtained would be useful in the establishment of national enteral feeding guidelines for preterm infants and quality improvement of cooperation at the national level.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
Human milk (HM) is the most ideal source of nutrition for newborns, especially preterm infants, on account of its short-term benefits, such as reducing the risk of necrotizing enterocolitis (NEC), sepsis, chronic lung disease(CLD), and mortality, and its long-term benefits, such as improving long-term neurodevelopment [1]. Apart from its medical advantages, HM feeding also has economic advantages [2]. Lactation onset is often delayed after premature delivery, and as a result, preterm infants receive an insufficient amount of milk during the first few critical days of life [3]. Donor human milk (DHM) and preterm formula are used as supplements when MOM is insufficient, and DHM is preferred over preterm formula as it is better in terms of nutritional composition and biological value [4, 5].
Therefore, the World Health Organization and the American Society for Parenteral Nutrition have emphasized the use of HM in preterm infants in their guidelines for the nutritional management of preterm/low-birth-weight infants [6]. Similarly, China issued “Feeding Recommendations for Preterm Infants and Low Birth Weight Infants” in 2009, according to which mother’s own milk (MOM) was recommended as the first choice for preterm infants [7]. Following these guidelines, the breastfeeding rate in China’s NICUs increased from 23% in 2009 to 58.2% in 2018 [8]. However, the breastfeeding rate is still far lower than that in other countries [9]. Furthermore, the situation of implementation of “Feeding Recommendations for Preterm Infants and Low Birth Weight Infants” for each NICU was still unclear. Therefore, the purpose of this study was to examine and compare the status of HM feeding and enteral feeding strategies in China’s level 3 NICUs. This is the first national-level survey on this topic in China, so the data obtained would be useful in the establishment of national enteral feeding guidelines for preterm infants and quality improvement of cooperation at the national level.
Methods
Survey methods
On September 7, 2021, a prospective, cross-sectional, web-based survey was sent to the director or representative of 60 level 3 NICUs participating in the Chinese Neonatal Network (CHNN).The CHNN is the first national neonatal network and has the largest geographically representative cohort from NICUs in China. It was officially put into operation on January 1, 2019. CHNN hospitals are tertiary referral hospitals with Grade A level 3 NICUs authorized by the Health Administration of China and have recognized expertise in caring for high-risk neonates.
The survey contained questions about the current status of HM feeding and enteral feeding strategies,and the unit director or representative was responsible for completing the survey and was instructed to provide answers based on common unit-level practice rather than their personal opinions/practice alone. The questionnaire, which consisted of single-choice, multiple-choice, and open-ended questions, gathered information about the demographic features of the unit, HM feeding characteristics, presence of a milk bank or access to DHM, initiation and advancement of enteral feeding, and indications for and the use of human milk fortifier (HMF), among other data(see supplementary materials). The deadline for submitting the filled-in surveys was October 7, 2021.
Data collection and analysis
Participants were enrolled between September 7 and October 7,2021. A link to the online questionnaire was sent through WeChat. Participants only needed to fill in the basic information for the NICUs and no personal information was attached to the data. All questions had to be completed before submission, duplicate responses were verified and eliminated.
The survey results were collected online and all analyses were conducted using Microsoft Excel. The demographic information was described by median (interquartile range,1–3). Descriptive results are expressed as numbers and percentage (%).
Results
Sixty NICUs responded to the survey: 14 (23.3%) were from children’s hospitals; 23 (38.3%) maternity hospitals; and 23 (38.3%) general hospitals. The median number of beds in these units was 100, and the median number of neonates hospitalized in 2020 was 3000, including 907 premature infants, 140 very-low-birth weight (VLBW) infants, and 148 infants of gestational age < 32 weeks (Table 1).
Education about breastfeeding
All 60 units encouraged breastfeeding at their NICUs. Parents were educated about breastfeeding before delivery at 26 units (43%), at the time of neonate admission at 57 units (95%), or during hospitalization at 57 units (95%). The staff involved in breastfeeding education included neonatal physicians at 51 units (85%), obstetricians at 21 units (36%), nurses in neonatal units at 60 units (100%), and nurses at human milk banks (HMBs) at 17 units (28%). The content and mode of communication of breastfeeding education for parents are shown in Table 2. Most of the units would repeat the breastfeeding instructions to the parents before neonatal discharge from the hospital (Table 2).
Feeding with mother’ own milk
Out of the 60 units, 36 (60.0%) had a dedicated breastfeeding/pumping room for mothers. Only 2 units (3.3%) did not accept MOM during neonatal hospitalization, and 36 units (61.7%) did not routinely pasteurize MOM after collection. Further, 55 units (91.7%) provided kangaroo care (KC), 20 units (33.3%) had family rooms, and 33 units (55.0%) routinely carried out family integrated care (FICare, parents spent ≥ 6 h per day in the NICU and provided non-medical care for their infants under the close supervision of the FICare nurse).
Donor human milk and human milk bank
Twenty of the hospitals (33.3%) established their own HMB, and the sources of operating funds for the HMB were social funding at 4 hospitals (20%), hospital funding at 15 (75%), and own unit funding at 14 (70%). All the HMBs provided their services for free, for both donors and recipients of DHM.
Only 13 units (21.7%) were licensed to use DHM. The main reasons for using DHM were to reduce the risk of NEC and support mother’s breastfeeding. The most common reason for not using DHM was the lack of a license. DHM was most frequently used in cases of extremely/very low birth weight infants, feeding intolerance, and intestinal malabsorption (Table 3).
Enteral feeding strategies
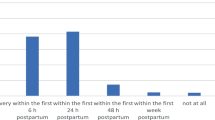
Eight units (13.3%) did not have any standardized protocol for nutrition management for infants with body weight < 1500 g. Twenty-nine units (48.3%) initiated minimal enteral nutrition (MEN,involves feeding with low volumes of 12–24 ml/kg/day in the first week of life) for infants with birth weight < 1500 g within 24 h after birth, and used fresh mother’ milk. However, 13 units (21.7%) used < 1250 g body weight as the criterion for initiating MEN, 13 units (21.7%) used < 1000 g and 5 units (8.3%) used < 750 g (Fig. 1A and B). The duration of MEN ranged from 24 to 144 h (Fig. 1C).

Minimum enteral nutrition practices at NICUs. A Infants that require minimal enteral nutrition after birth; B Time at which minimal enteral nutrition was started after birth for infants with body weight < 1500 g; C Duration of minimal enteral nutrition for premature infants
Most of the NICUs increased the volume of enteral feeding at the rate of 10–20 ml/kg daily (Fig. 2A) and discontinued parenteral nutrition when the enteral volume reached ≥ 120 ml/kg daily (Fig. 2B). HMF was added when enteral volume reached 80–100 ml/kg daily in most units(80%), at the ratio of 1:50 (HMF to human milk) as initial dosage(58.3%) (Fig. 2C and D).

Enteral feeding and human milk fortifier at NICUs. A Rate at which the volume of enteral nutrition was increased in premature infants; (B) Volume of enteral nutrition required to discontinue parenteral nutrition; (C) Volume of enteral nutrition before the use of human milk fortifier was initiated; (D) Ratio of human milk fortifier at the time of initiation
At 31 NICUs (51.7%), gastric residual content was examined before every feeding episode (Fig. 3A). At 41 NICUs (68.3%), the course of enteral nutrition management was not changed during treatment for patent ductus arteriosus(PDA)(Fig. 3B). At 29 NICUs (48.3%), enteral feeding was stopped for 1 or 2 feeds during blood transfusion to prevent NEC (Fig. 3C).

Gastric residual content and changes in feeding strategy. A Time point for assessment of gastric residual content; B Changes in enteral feeding strategies during drug treatment for patent ductus arteriosus; C Enteral feeding changes during blood transfusion
Discussion
Nutrition is important to standardize among different NICUs, even in terms of long-term outcomes. For example, the prevention of extra-uterine growth retardation (EUGR) in preterm infants through nutritional strategies is of extreme importance, as the achievement of adequate growth has been associated with a better neurodevelopmental outcome through childhood [10], although there is still no consensus regarding the best definition of EUGR to use to predict neurological outcome [11].
This is the first comprehensive study to investigate human milk feeding and enteral feeding practices in NICUs from all districts in mainland China. As evident in the survey responses, we found significant variations but also similarities in the status of human milk feeding and enteral feeding strategies among the examined NICUs. In general, all the NICUs encouraged breastfeeding, and breastfeeding education was provided by nurses in the neonatal units. The content of breastfeeding education covered benefits of breastfeeding, collection,storage,and transport of breast milk,kangaroo care, how to keep lactation,feedback of breastfeeding. Breastfeeding information was provided via channels such as oral instruction, video, paper materials,bedside education,WeChat or SMS platform and others. During the recent COVID-19 pandemic, parental visitation practices were suspended at many NICUs in China but once the pandemic was brought under control, most NICUs restarted their previous parental visitation policies. At most NICUs, communication about breastfeeding with parents was implemented online or through face-to-face meetings at least once a week. Further, at the majority of the hospitals (58 NICUs, 96.7%), MOM was obtained during neonatal hospitalization.
The present findings showed significant variations between the NICUs with regard to the provision of family rooms and FICare, the use of DHM, and enteral feeding strategies.55 NICUs (91.7%) provided KC. Accordingly, previous studies have documented that most NICUs in China were aware of the benefits of KC [12, 13]. Compared to the high rates of implementation of KC, family rooms were provided in only 20 NICUs (33.3%) and only 33 units (55.0%) routinely provided FICare. Family rooms are known to be beneficial for both infants and parents, as they improve weight gain, promote breastfeeding after NICU discharge, reduce parental stress and anxiety, as well as reduce the incidence of health-assistance related infections [14]. Additionally, FICare in Chinese NICUs was found to be associated with reduced hospital length of stay, medical expenditures, and rates of adverse outcomes [15]. Therefore, in the future, NICUs in China should promote FICare vigorously.
Since the first HMB was established in Guangzhou in 2003, 20 HMBs have been established in China so far. All these HMBs provide their services free of charge to both donors and recipients of DHM. However, the cost of running HMBs is quite high [16] and is almost entirely borne by the local hospitals, as shown by our findings. This is also one of the reasons for the small number of HMBs in China. Therefore, it is necessary to find alternate sources of funds for HMBs in China. In China, both parents and medical workers’ attitude about DHM is positive [17,18,19], but in our survey, only 13 units (21.7%) used DHM. The most common reason for not using DHM was the lack of a license. This highlights the need to improve the process of using DHM in China.In the 7 units that established an HMB but did not use DHM, the reason was because the banks were awaiting for their licensing.Therefore, they could only manage and use MOM in the HMB.
Our study highlights the diversity of recommended feeding practices in NICUs across China. While most of the units initiated MEN for infants with birth weight < 1500 g (48.3%), the criteria for initiating MEN varied considerably across the remaining units. The optimal duration of MEN is still under debate [20, 21], and this was also reflected in the results of our study. With regard to feed volume, we found that most units (83.3%) increased enteral feeding intake by 10 to 20 ml/kg daily. A Cochrane review compared daily feed intake increments of 15 to 20 ml/kg versus 30 to 35 ml/kg and concluded that more rapid advancement did not increase the risk of NEC, mortality, or interruption of feeds [22]. Further, previous studies reported that early fortification (< 40 ml/kg daily) was safe and well tolerated [23]. In the present study, we found a significant variation in both the recommended timing of initiation and the recommended initial volume of HMF. Another international survey-based study also reported large variations in the timing of initiation and volume of HMF at initiation [24]. Given these variations in enteral feeding strategies and the previous findings, national-level guidelines should recommend standardized enteral feeding and human milk fortification strategies for NICUs in China.
Routine assessment of gastric residual content was reported by 31 units (51.7%).A previous study indicated that the omission of gastric residual evaluation increased the delivery of enteral nutrition as well as improved weight gain and led to earlier hospital discharge [25]. This suggests that the NICUs in China should probably change the previous practice.A previous study reported that feeding during pharmacological PDA closure in preterm neonates was not associated with delay to reach full feeds, NEC incidence, or gastric residuals; nonetheless, feeding management of this population should be carefully evaluated [26]. Our study showed that 41 units (68.3%) did not make any changes in their enteral feeding regimen during drug treatment for PDA. Further, feeding during blood transfusions may increase the risk for mesenteric ischemia and the development of transfusion-related NEC in preterm infants [27]. In the present study, 29 units (48.3%) instated stop feeding for 1 or 2 feeds during blood transfusion, but 15 units (25.0%) reported that did not introduce any changes and only closely monitored the situation.
There are some limitations to this study. As with other surveys, a responder bias could not be ruled out, and the responses may, potentially, not be representative of the practices of the unit. We also did not evaluate whether the variation in feeding practices are associated with infant growth and outcomes such as NEC.
Conclusion
There were significant differences in human milk feeding and enteral feeding strategies between the NICUs in CHNN, but also similarities. Establishing national-level feeding guidelines for preterm and low birth weight infants and quality improvement of cooperation at the national level are needed. This is the first national-level survey on this topic in China, so the data obtained would be useful in the establishment of national enteral feeding guidelines for preterm infants and quality improvement of cooperation at the national level.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author upon request.
References
Reena OF, Rashmi K, James D. A quality improvement project to decrease human milk errors in the NICU. Pediatrics. 2017;139(2):e20154451.
Tricia JJ, Aloka LP, Harold RB. Economic benefits and costs of human milk feedings: a strategy to reduce the risk of prematurity-related morbidities in very-low-birth-weight infants. Adv Nutr. 2014;5(2):207–12.
Corpeleijn WE, Kouwenhoven SM, Paap MC. Intake of own mother’s milk during the first days of life is associated with decreased morbidity and mortality in very low birth weight infants during the first 60 days of life. Neonatology. 2012;102(4):276–81.
Capriati T, Goffredo BM, Argentieri M, De Vivo L, Bernaschi P, Cairoli S, Laureti F, Reposi MP, Marino D, Benedetti S, Diamanti A. A Modified Holder Pasteurization Method for Donor Human Milk: Preliminary Data. Nutrients. 2019;11(5):1139.
Committee on Nutrition, Section on Breastfeeding, Committee on Fetus and Newborn. Donor human milk for the high-risk infant: Preparation, safety, and usage options in the United States. Pediatrics. 2017;139(1):e20163440.
Agostoni C, Buonocore G, Carnielli VP. Enteral nutrient supply for preterm infants: Commentary from the European Society of Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition. J Pediatr Gastroenterol Nutr. 2010;50(1):85–91.
Editorial Board of Chinese Journal of Pediatrics, Sub specialty Groups of Neonatology and Child Health Care, & The Society of Pediatrics Chinese Medical Association. Feeding recommendations for preterm infants and low birth weight infants. Zhonghua Er Ke Za Zhi. 2009;47(7):508–10.
Yuanyuan Y, Hong L. Breastfeeding in hospitalised preterm infants: A survey from 18 tertiary neonatal intensive care units across mainland China. J Paediatr Child Health. 2020;56(9):1432–7.
Henry CL, Paul SK, Nancy EW. A quality improvement project to increase breast milk use in very low birth weight infants. Pediatrics. 2012;130(6):e1679–87.
Giannì ML, Roggero P, Garbarino F, Bracco B, Fumagalli M, Agosti M, Mosca F. Nutrition and growth in infants born preterm from birth to adulthood. Early Hum Dev. 2013;89(Suppl 2):S41–4.
De Rose DU, Cota F, Gallini F, Bottoni A, Fabrizio GC, Ricci D, Romeo DM, Mercuri E, Vento G, Maggio L. Extra-uterine growth restriction in preterm infants: Neurodevelopmental outcomes according to different definitions. Eur J Paediatr Neurol. 2021;33:135–45.
Yao Z, Qingqi D, Binghua Z. Neonatal intensive care nurses’ knowledge and beliefs regarding kangaroo care in China: a national survey. BMJ Open. 2018;8(8):e021740.
Bo Z, Zhiying D, Yingxi Z. Intermittent kangaroo mother care and the practice of breastfeeding late preterm infants: results from four hospitals in different provinces of China. Int Breastfeed J. 2020;15(1):64.
O’Brien K, Robson K, Bracht M. Effectiveness of Family Integrated Care in neonatal intensive care units on infant and parent outcomes: a multicentre, multinational, cluster-randomised controlled trial. Lancet Child Adolesc Health. 2018;2(4):245–54.
Mingyan H, Xiangyu G, Ying L. Family Integrated Care for Preterm Infants in China: A Cluster Randomized Controlled Trial. J Pediatr. 2021;228:36–43.
Daili C, Kunkun Z, Guangjun Y. Cost Analysis of Operating a Human Milk Bank in China. J Hum Lact. 2020;36(2):264–72.
Ce T, Yamin L, Lee S. Lactating Women’s Knowledge and Attitudes About Donor Human Milk in China. J Hum Lact. 2021;37(1):52–61.
Na Z, Junyan L, Xinwen L. Factors associated with postpartum women’s knowledge, attitude and practice regarding human milk banks and milk donation: a cross-sectional survey. Midwifery. 2020;91: 102837.
Rui Y, Danqi C, Qingqi D. The effect of donor human milk on the length of hospital stay in very low birthweight infants: a systematic review and meta-analysis. Int Breastfeed J. 2020;15(1):89.
Jessie M, Lauren Y, William M. Delayed introduction of progressive enteral feeds to prevent necrotising enterocolitis in very low birth weight infants. Cochrane Database Syst Rev. 2014;12:CD001970.
Ozlem B, Evrim AD, Duygu B. Prolonged minimal enteral nutrition versus early feeding advancements in preterm infants with birth weight ≤1250 g: a prospective randomized trial. J Matern Fetal Neonatal Med. 2022;35(2):341–7.
Oddie SJ, Young L, McGuire W. Slow advancement of enteral feed volumes to prevent necrotising enterocolitis in very low birth weight infants. Cochrane Database Syst Rev. 2017;8(8):CD001241.
Beth G, Carmel TC, Cathie H. Does early compared to late fortification of human milk for preterm infants improve clinical outcomes? J Paediatr Child Health. 2019;55(7):867–72.
Klingenberg C, Embleton ND, Jacobs SE. Enteral feeding practices in very preterm infants: An international survey. Arch Dis Child Fetal Neonatal Ed. 2012;97:F56-61.
Leslie AP, Michael W, Roberto MT. Effect of Gastric Residual Evaluation on Enteral Intake in Extremely Preterm Infants: A Randomized Clinical Trial. JAMA Pediatr. 2019;173(6):534–43.
Martini S, Aceti A, Galletti S, Beghetti I, Faldella G, Corvaglia L. To Feed or Not to Feed: A Critical Overview of Enteral Feeding Management and Gastrointestinal Complications in Preterm Neonates with a Patent Ductus Arteriosus. Nutrients. 2019;12(1):83.
Terri M, Cassandra DJ, Niki K. Feeding preterm infants during red blood cell transfusion is associated with a decline in postprandial mesenteric oxygenation. J Pediatr. 2014;165(3):464–71.
Acknowledgements
The authors gratefully acknowledge all site investigators of the China Neonatal Network (CHNN) for their participation in this survey.
Funding
This study was supported by the Nanjing Medical Science and Technology Development Foundation (grant number ZKX19045); the "Specialized Diseases Cohort" Program of Nanjing Medical University (grant number NMUC2020037); and the Six Talent Peaks Project in Jiangsu Province (grant number LGY2019008).
Author information
Authors and Affiliations
Contributions
Xiaoshan Hu and Junjie Lu conceptualized and designed the study, drafted the initial manuscript,and approved the final manuscript as submitted. Shuping Han and Xiaohui Chen conceptualized and designed the study, conducted data analysis, drafted the initial manuscript. Jun Zhang, Min Zhang and Zhangbin Yu participated in data collection and sorting, and reviewed and revised the manuscript. Shoo K. Lee prepared the data and initial analysis, critically reviewed the manuscript and approved the final manuscript as submitted. All the authors have read and approved the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The ethical approval was waived by Medical Ethics Committee of Nanjing Maternity and Child Health Hospital as the study did not involve access to private patient data or alterations of feeding practices.Every participant was inquired the willingness to join this survey and informed consent was obtained. All methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hu, X., Lu, J., Zhang, J. et al. Survey on human milk feeding and enteral feeding practices for very-low-birth-weight infants in NICUs in China Neonatal Network. BMC Pediatr 23, 75 (2023). https://doi.org/10.1186/s12887-023-03862-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-023-03862-0