
Abstract
Background
Evidence suggests that the interactive effects of physical activity, screen-time and sleep are stronger than independent effects of these behaviors on pediatric obesity. However, this hypothesis has not been fully examined among samples of young school-aged children. The aim of this study is to determine the association of weight status with meeting the physical activity, screen-time, and sleep guidelines, independently and concurrently, among 2nd grade children.
Methods
The Texas School Physical Activity and Nutrition Project collected parent-reported physical activity, screen-time, and sleep, and measured body height and weight on a statewide representative weighted sample (n = 320,005) of children. Weighted multivariable logistic regressions were used to assess associations of weight status (classified using age- and sex-specific body weight [kg]/height [m]2, based on International Obesity Task Force cutoffs) with meeting the physical activity, screen-time, and sleep guidelines, while controlling for relevant covariates (age, sex, race/ethnicity, comorbidities etc.).
Results
A greater proportion of healthy weight children (9.9%) met the physical activity, screen-time, and sleep guidelines concurrently compared to children who are thin (3.3%), or children with overweight (5.7%), obese (3.5%), and morbid obesity (1.0%). Children who were thin (adjusted odds ratio [aOR]:0.40, 95% confidence interval [CI]: 0.10, 1.50), overweight (aOR = 0.75, CI: 0.33, 1.70), obese (aOR = 0.53, CI: 0.15, 1.81), and morbidly obese (aOR = 0.10, CI: 0.02, 0.28) had lower odds of concurrently meeting the guidelines compared to children with healthy weight.
Conclusions
Among this representative sample of Texas children, weight status was associated with meeting physical activity, screen-time, and sleep guidelines. Future studies should aim to evaluate causal relations between these behaviors and weight status.
Similar content being viewed by others


Introduction
Short sleep duration, physical inactivity, and increased screen-time are independent risk factors for childhood obesity [1,2,3,4,5]. The combination of these deleterious behaviors influences childhood obesity status to a greater degree than what is observed of each behavior independently [6, 7]. In light of these findings, the American Academy of Pediatrics and World Health Organization established evidence-based guidelines which recommend that children accumulate at least 60 minutes of moderate intensity aerobic physical activity (PA) per 24 hours, limit their screen-time to less than 2 hours, and sleep for 9–11 hours (aged 6–13 years) [1, 8, 9]. However, recent studies have reported that a majority of children do not meet the guideline recommendations, and the prevalence of independently meeting the guidelines is decreasing globally [10,11,12].
Among children and adolescents in the United States (U.S.), 23, 33, and 86% independently meet the PA, screen-time, and sleep guidelines, respectively [13]. Only 12.9% of all U.S. children aged 6–11 years and 5% of U.S. high school adolescents aged 12–17 years meet all three of the guidelines concurrently [13, 14]. The lack of U.S. children concurrently meeting guidelines is of growing concern. Childhood obesity prevalence has increased nationally from 5.2% in 1974 to 19.3% in 2018 [15]. Of particular concern, the prevalence of childhood obesity in the state of Texas is among the highest in the U.S. In 2019 it was reported that 17.3% of Texas children have obesity [16]. Nearly 20 years ago, Perez and colleagues [17] found that Texas children who did not concurrently meet the PA guidelines (20–30 minutes of vigorous- to moderate- intensity activity on at least 3 or 5 days in the past week, respectively) and screen-time guidelines (2 hours or less per day) had higher odds of obesity (boys: odds ration [OR]: 1.40, 95% confidence interval [CI]: 1.01, 1.94; girls: OR: 1.26, 95% CI: 0.78, 2.04) than those who were normal weight. Other studies have also demonstrated independent associations between physical activity, sedentary behaviors, and sleep [4, 13, 14] with weight status in children, however, there remains a limited understanding of the health implications of concurrently engaging in recommended levels of these behaviors with various health outcomes. In particular, the level of understanding on this topic remains scant among population-based samples of young school-aged U.S. children.
Therefore, the aim of this study is to determine whether weight status is associated with meeting the PA, screen-time, and sleep guidelines, independently and concurrently, among a statewide representative sample of 2nd grade children in Texas. We hypothesize that children with unhealthy weight will be associated with lower odds of achieving the PA, screen-time, and sleep guidelines, independently and concurrently, compared to children with healthy weight. The results from this study will help in developing more knowledge and awareness on the association between 24-hour cycle behaviors and pediatric obesity [18].
Methods
Study design, data source and participants
This cross-sectional study was reported and all methods were carried out in accordance to the Strengthening the Report of Observational studies in Epidemiology (STROBE) guidelines [19]. This analysis was conducted using 2015–2016 survey data collected by the Texas School Physical Activity and Nutrition (SPAN) Project. A full description of the Texas SPAN study design and participants is available elsewhere [20]. Briefly, Texas SPAN is a cross-sectional, statewide representative, school-based cluster survey administered annually since 2000. Texas SPAN is designed to measure prevalence of obesity, nutrition, PA, sleep, screen-time, and other health behaviors among 2nd, 4th, 8th, and 11th grade children in Texas. The current study included 2nd grade children (n = 320,005) who participated in Texas SPAN during the 2015–2016 school year. Written child assent and informed consent were obtained from all Texas SPAN participants and primary caregivers to use their data for research purposes. This study was reviewed and approved by the Committee for the Protection of Human Subjects at the University of Texas Health Science Center at Houston (UTHealth) (HSC-SPH-00-056), the Texas Department of State Health Services Institutional Review Board (IRB# 04–062), and local school district review committees.
Measures
The primary exposure of interest was body weight status. Standard protocols were used to measure and record height and weight among the participants. Body mass index (BMI) was calculated using body weight in kilograms divided by the square of height in meters. Weight status was further classified by age and sex healthy (BMI: 18.5–24.99), thin (BMI: < 18.5), overweight (BMI: 25.00–29.99), obesity (BMI: 30.00–39.99), and morbid obesity (BMI: > 35.00), according to International Obesity Task Force (IOTF) definitions [21].
The primary outcome variables of interest were meeting the PA, screen-time, and sleep guidelines, independently and concurrently. The participating child’s primary caregiver was asked to report on their child. PA behavior was assessed by reporting the total number of days in the last week the child performed activity that increased his/her heart rate and made him/her breathe hard some of the time for a total of at least 60 minutes. Those participants reporting 7-days of PA as described were considered to have met the PA guideline [8]. Screen-time behaviors were assessed by asking how many hours per day the child usually spends watching TV, DVDs, movies or using a computer, tablet/iPad® or Smartphone® away from school. The hours for each screen-based activity were summed. Children having less than 2 hours total of screen-time per day were considered to have met the screen-time guideline. Sleep was assessed by asking parents how many hours of sleep their child usually gets per night. Those children reporting 9–11 hours of sleep per night were considered to have met the sleep guideline [1, 8, 22]. The PA, screen-time, and sleep questions were adapted (for parent proxy report) from the Youth Risk Behavior Surveillance System (YRBSS) questionnaires and have been shown to demonstrate acceptable reliability [23].
Potential covariates that are known to be associated with weight status included in the analysis were caregiver-reported demographic characteristics (e.g. age [years]; sex; race/ethnicity [non-Hispanic White, non-Hispanic Black, Hispanic/Latinx, and other]; financial assistance (yes/no); healthy food preference (always, sometimes, or never); comorbidities [yes/no] including physical limitations, asthma, diabetes, attention deficit hyperactivity disorder, autism spectrum disorder), and parent BMI [continuous] [24,25,26,27,28].
Statistical analysis
The proportions and 95% confidence intervals (CI) of weight status were estimated in sex strata by potential covariates (e.g., age, sex, race/ethnicity, financial assistance, healthy food preference, comorbidities, and parent BMI). Multiple logistic regressions in sex stratum were adjusted for potential covariates and used to calculate weighted relative odds of independently and concurrently meeting the PA, screen-time, and sleep guidelines based on child weight status. All statistical analyses were conducted in STATA 15.1 (Stata Statistical Software: Release 15, StataCorp LLC, College Station, TX).
Results
Sample demographic and health characteristics are presented in Table 1. Among Texas 2nd grade children, nearly two-thirds (58.5%) had a healthy weight status, 4.7% were thin, 17.38% were overweight, 9.3% had obesity, and 9.6% had morbid obesity. The majority were 7 years of age (62.3%), Hispanic/Latinx (56.4%) ethnicity, and received financial assistance (70.3%). Asthma was the most common comorbidity (14.4%) followed by attention deficit hyperactivity disorder (7.8%), physical limitations (3.2%), autism spectrum disorder (0.9%), and diabetes (0.4%).
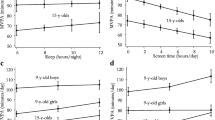
The prevalence of children who independently met the PA, screen-time, and sleep guidelines differed by weight status and gender (Table 2). Specifically, 4.9% (95% CI: 2.3, 10.2) of girls with morbid obesity met the PA guideline, compared to 24.5% (95% CI: 19.7, 29.9) of girls with healthy weight. Among boys, 15.8% (95% CI: 8.6, 27.2) of boys with obesity met the PA guideline, compared to 27.5% (95% CI: 23.0, 32.6) of boys with healthy weight. For screen-time and sleep, results followed a similar pattern overall and by sex. The prevalence of meeting the guidelines concurrently was lowest among those children classified as having obesity and morbid obesity (overall and by sex), with the exception of boys with thin weight status (2.2, 95% CI: 0.3, 18.2). Overall, 3.5% (95% CI: 1.2, 10.0) and 1.0% (95% CI: 0.3, 2.9) of children with obesity and morbid obesity met the guidelines concurrently, compared to 9.9% (95% CI: 6.9, 14.1) of children with healthy weight. Among girls with obesity and morbid obesity, 3.5% (95% CI: 1.1, 11.3) and 1.1% (95% CI: 0.3, 4.1) concurrently met the guidelines, compared to 8.3% (95% CI: 5.5, 12.3) of girls with healthy weight. Meanwhile, 3.6% (95% CI: 0.6, 18.2) of boys with obesity and 0.08% (95% CI: 0.1, 5.9) of boys with morbid obesity concurrently met the guidelines, compared to 11.3% (95% CI; 6.8, 18.2) of boys with healthy weight.
The adjusted odds ratio (aOR) of meeting the PA, screen-time, and sleep guidelines among Texas 2nd grade children, after controlling for age, race/ethnicity, financial assistance, comorbidities, and parent BMI, are presented overall and by sex in Table 3. There were significant associations with having obesity and morbid obesity and independently meeting the PA guideline. Specifically, girls with morbid obesity had 0.16 (95% CI: 0.05, 0.47) and girls with obesity had 0.37 (95% CI: 0.18, 0.77) times the odds of meeting the PA guideline compared to girls with healthy weight. For boys, those classified as having morbid obesity and obesity had 0.42 (95% CI: 0.18, 0.97) and 0.41 (95% CI: 0.18, 0.92) times the odds of meeting the PA guidelines, respectively, compared to boys with healthy weight.
Children with obesity and morbid obesity of both sexes were less likely to concurrently meet the guidelines than children with healthy weight. Specifically, girls with morbid obesity had lower odds (aOR: 0.52, 95% CI: 0.13, 2.05) of achieving the PA and screen-time guidelines concurrently compared to girls with healthy weight. Further, girls with morbid obesity had 0.08 (95% CI: 0.19, 0.33) times the odds of achieving all three of the guidelines concurrently compared to girls with healthy weight. Boys with morbid obesity had 0.09 (95% CI: 0.03, 0.27) times the odds of meeting the sleep and screen-time guidelines concurrently.
Discussion
This study found that weight status and sex are associated meeting the PA, screen-time, and sleep guidelines, independently and concurrently. The prevalence of meeting the PA guideline was over three times higher among boys with morbid obesity compared to girls with morbid obesity. There are several potential explanations for the observed sex difference. In a prospective study of children aged 8 to 12 years, boys were found to be 19% more physically active than girls and these differences were attributed to less extracurricular sport participation, less parental support, and less perceived competence in physical education in girls compared to boys [29]. In other studies of younger children (aged 4 to 6 years and 9 to 11 years, respectively), boys have been found to be more physically active compared to girls, regardless of obesity status [30, 31]. Conversely, nearly half of girls with morbid obesity met the screen-time guidelines compared to less than 10% of boys with morbid obesity. Thirty one percent of girls with morbid obesity and 2.4% of boys with morbid obesity met the screen-time and sleep guidelines. Despite these differences, a similar proportion of boys and girls met all three guidelines concurrently, suggesting that while prevalence of concurrently meeting guidelines is of concern among all children, different problematic movement behavior patterns may be at play among male versus female children. Overall, children with healthy weight had the highest prevalence of meeting any of the guidelines, independently and concurrently, compared to children with unhealthy weight. Similar trends were observed when evaluating the odds of meeting any of the guidelines by weight status. For instance, none of the boys with unhealthy weight were more likely to meet any combination of the guidelines than boys with healthy weight with the exception of thin boys more likely to meet sleep and screen-time guidelines concurrently. Similarly, none of the girls with unhealthy weight were more likely to meet certain guidelines, independently and concurrently, compared to girls with healthy weight with the exception of thin girls and girls with morbid obesity more likely to meet sleep and screen-time guidelines concurrently. Most notably, girls with morbid obesity were nearly 2 times more likely to meet the screen-time guidelines independently, and the sleep and screen-time guidelines concurrently, compared to girls with healthy weight. This demonstrates the importance of studying and evaluating adherence to the guidelines concurrently by sex. Further, these results contribute to a limited body of research that suggests that meeting the PA, screen-time, and sleep guidelines concurrently may have an important relationship with pediatric obesity [6, 17, 18].
Overall, these results align with previous findings from population-based samples of U.S. adolescents, which reported that a very small proportion (5%) of students met all of the guidelines concurrently, [14] and those who do not meet the guidelines were more likely to have obesity.17 However, participants in our analysis were younger (2nd grade) than those included in similar studies [14, 17], which is important given the challenges and deleterious health outcomes related to early-onset morbid obesity in childhood. Similar to the current study’s findings, Laurson et al. [7] concluded that the relationship between weight status and meeting all of the guidelines appeared to be associated in a graded manner where those with the unhealthiest weight status had the lowest odds of meeting all of the guidelines. Overall, the literature suggests that adherence to the PA, screen-time, and sleep guidelines among children differs across sexes, and that these behaviors are associated with weight status.
The prevalence of children independently meeting the guidelines provided interesting findings. In particular, it appears that the low prevalence of meeting all of the guidelines concurrently was primarily driven by the inclusion of meeting the PA guidelines, rather than meeting the sleep or screen-time guidelines. For example, among children with healthy weight (boys and girls), 32.0% met the sleep and screen-time guidelines concurrently. When adherence to the PA guideline was added to the combination, the proportion of children meeting all of the guidelines dropped to 9.9%. This was consistently observed across all weight status categories and for both sexes when evaluated per strata. This may help explain the mechanisms by which children with obesity and morbid obesity are less likely to meet all three guidelines concurrently. Social norms (e.g., lower levels of adult support and self-conscious of body/looks when physically active) and psychological barriers (e.g., lack of interest, fear of being teased/chosen last, lack of energy/willpower/motivation) may disproportionately increase the barriers to meeting the physical activity guidelines for children with obesity and morbid obesity compared to children with healthy weight [32,33,34].
This study is not without limitations. First, the measures for the primary outcomes of interest, adherence to the PA, screen-time, and sleep guidelines, were reported by the child’s primary caregiver, which has mixed evidence of agreement compared to self-report in children [35, 36]. However, children in our study were very young (2nd grade) and the child’s primary caregiver report might be preferable in this age group. Future studies could aim to use objective PA and sleep measurement tools such as accelerometers, however the guidelines were developed using self-report measures which could indicate that measuring adherence to the guidelines with objective measurement tools is incorrect [37]. Although there is evidence of associations between screen-time, pediatric obesity [38], and other health outcomes [39] some of the guidelines (e.g., American Academy of Pediatrics) have removed previous screen-time recommendations due to potential weaknesses of screen-time measures, which include lack of evidence for a clear threshold of time and determining if screen-time is a proxy measure for sedentary behavior [40,41,42]. Even though screen-time measures have potential weaknesses, systematic reviews continue to report moderately strong evidence of association between screen-time and obesity and suggest more evidence is needed to inform guidelines [40]. Finally, given the cross-sectional design of this study, we are unable to make conclusions regarding the temporal associations between pediatric weight status and meeting the guidelines. Despite these limitations, a strength of this study is the large sample size which is state-representative and includes more low-income and diverse populations than the representative U.S. population. Additionally, our study used direct measurement of height and weight to calculate child BMI, which has been found to be more accurate than self-reported BMI [43].
Conclusion
Finally, this study added to our understanding of how pediatric body weight status is associated with a 24-hour cycle of behaviors. Importantly, most studies to this point on this young of a population have only focused on a single behavior in isolation, thereby ignoring the inherent displacing effect of the behaviors on each other, and potential interactive effects of multiple behaviors occurring simultaneously. To our knowledge, this is the first study to report the association between concurrently meeting the PA, screen-time, and sleep guidelines with weight status in a population-based sample of young school-aged children. Although the results of this analysis indicate that PA in particular is strongly related to body weight status in this age group, future studies should strive to consider PA, sleep and sedentary behaviors both independently and concurrently in studies of their effects on pediatric obesity and other related health outcomes.
The results of this study should raise awareness to the potential magnitude of not adhering recommendations for 24-hour cycle of physical behaviors in pediatric populations and should inform future research to consider the interrelation of adherence to the PA, screen-time, and sleep guidelines when evaluating pediatric obesity. We found that adherence to the PA guidelines is much lower than adherence to the screen-time or sleep guidelines, therefore intervening on the PA guideline adherence may provide the most benefit. The difference in likelihood between concurrently meeting the guidelines and weight statuses suggests increased attention should be given to adherence to the guidelines in children with unhealthy weight compared to children with healthy weight.
Availability of data and materials
The datasets used and/or analysed during the current study are not publicly available due to concerns about analysis quality and consistency but are available from the corresponding author on reasonable request.
Abbreviations
- PA:
-
Physical activity
- U.S.:
-
United States
- SPAN:
-
School Physical Activity and Nutrition
- BMI:
-
Body mass index
- IOTF:
-
International Obesity Task Force
- CI:
-
Confidence intervals
- aOR:
-
Adjusted odds ratio
- STROBE:
-
Strengthening the Report of Observational studies in Epidemiology
References
Tremblay MS, Carson V, Chaput JP, Connor Gorber S, Dinh T, Duggan M, et al. Canadian 24-hour movement guidelines for children and youth: an integration of physical activity, sedentary behaviour, and sleep. Appl Physiol Nutr Metab Physiol Appl Nutr Metab. 2016;41(6 Suppl 3):S311–27.
Taheri S. The link between short sleep duration and obesity: we should recommend more sleep to prevent obesity. Arch Dis Child. 2006;91(11):881–4.
Janssen I, LeBlanc AG. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int J Behav Nutr Phys Act. 2010;7(1):40.
Cappuccio FP, Taggart FM, Kandala NB, Currie A, Peile E, Stranges S, et al. Meta-analysis of short sleep duration and obesity in children and adults. Sleep. 2008;31(5):619–26.
Tremblay MS, LeBlanc AG, Kho ME, Saunders TJ, Larouche R, Colley RC, et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth. Int J Behav Nutr Phys Act. 2011;21(8):98.
Saunders TJ, Gray CE, Poitras VJ, Chaput JP, Janssen I, Katzmarzyk PT, et al. Combinations of physical activity, sedentary behaviour and sleep: relationships with health indicators in school-aged children and youth. Appl Physiol Nutr Metab Physiol Appl Nutr Metab. 2016;41(6 Suppl 3):S283–93.
Laurson KR, Lee JA, Gentile DA, Walsh DA, Eisenmann JC. Concurrent associations between physical activity, screen time, and sleep duration with childhood obesity. ISRN Obes. 2014;2014:204540.
Expert Committee Recommendations Regarding the Prevention, Assessment, and Treatment of Child and Adolescent Overweight and Obesity: Summary Report | American Academy of Pediatrics. Available from: https://pediatrics.aappublications.org/content/120/Supplement_4/S164. Cited 2021 Jun 14
Bull FC, Al-Ansari SS, Biddle S, Borodulin K, Buman MP, Cardon G, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. 2020;54(24):1451–62.
Guthold R, Stevens GA, Riley LM, Bull FC. Global trends in insufficient physical activity among adolescents: a pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc Health. 2020;4(1):23–35.
Bucksch J, Sigmundova D, Hamrik Z, Troped PJ, Melkevik O, Ahluwalia N, et al. International trends in adolescent screen-time behaviors from 2002 to 2010. J Adolesc Health Off Publ Soc Adolesc Med. 2016;58(4):417–25.
Loprinzi PD, Davis RE. Recent temporal trends in parent-reported physical activity in children in the United States, 2009 to 2014. Mayo Clin Proc. 2016;91(4):477–81.
Friel CP, Duran AT, Shechter A, Diaz KM. U.S. Children meeting physical activity, screen time, and sleep guidelines. Am J Prev Med. 2020;59(4):513–21.
Knell G, Durand CP, Kohl HW III, Wu IHC, Pettee GK. Prevalence and likelihood of meeting sleep, physical activity, and screen-time guidelines among US youth. JAMA Pediatr. 2019;173(4):387–9.
Fryar CD, Carroll MD, Afful J. Prevalence of overweight, obesity, and severe obesity among children and adolescents aged 2–19 years: United States, 1963–1965 through 2017–2018. NCHS Health E-Stats. 2020.
State Obesity Data. The State of Childhood Obesity. Available from: https://stateofchildhoodobesity.org/states/. Cited 2021 Jul 20
Pérez A, Hoelscher DM, Springer AE, Brown HS, Barroso CS, Kelder SH, et al. Physical activity, watching television, and the risk of obesity in students, Texas, 2004-2005. Prev Chronic Dis. 2011;8(3):A61.
Dulloo AG, Miles-Chan JL, Montani JP. Nutrition, movement and sleep behaviours: their interactions in pathways to obesity and cardiometabolic diseases. Obes Rev Off J Int Assoc Study Obes. 2017;18(Suppl 1):3–6.
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344–9.
Pérez A, Hoelscher D, Frankowski R, Day R, ES L. Statistical design, sampling weights and weight adjustments of the school physical activity and nutrition (SPAN) population-based surveillance 2009-2010 study. JSM Proceedings, Statistics in Epidemiology. Washington, DC. American Statistical Association; 2010. p. 3397–404.
Cole TJ, Lobstein T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr Obes. 2012;7(4):284–94.
Strasburger VC, Wilson BJ, Jordan AB. Children, adolescents, and the media: SAGE Publications; 2013. p. 673.
Brener ND, Kann L, Kinchen SA, Grunbaum JA, Whalen L, Eaton D, et al. Methodology of the youth risk behavior surveillance system. MMWR Recomm Rep Morb Mortal Wkly Rep Recomm Rep. 2004;53(RR-12):1–13.
Isong IA, Rao SR, Bind MA, Avendaño M, Kawachi I, Richmond TK. Racial and ethnic disparities in early childhood obesity. Pediatrics. 2018;141(1) Available from: https://pediatrics.aappublications.org/content/141/1/e20170865. Cited 2021 Aug 25.
Bolton K, Kremer P, Rossthorn N, Moodie M, Gibbs L, Waters E, et al. The effect of gender and age on the association between weight status and health-related quality of life in Australian adolescents. BMC Public Health. 2014;14(1):898.
Halford JCG, Boyland EJ, Cooper GD, Dovey TM, Smith CJ, Williams N, et al. Children’s food preferences: effects of weight status, food type, branding and television food advertisements (commercials). Int J Pediatr Obes IJPO Off J Int Assoc Study Obes. 2008;3(1):31–8.
Erhart M, Herpertz-Dahlmann B, Wille N, Sawitzky-Rose B, Hölling H, Ravens-Sieberer U. Examining the relationship between attention-deficit/hyperactivity disorder and overweight in children and adolescents. Eur Child Adolesc Psychiatry. 2012;21(1):39–49.
Fradkin C, Wallander J, Elliott M, Tortolero S, Cuccaro P, Schuster M. Associations between socioeconomic status and obesity in diverse, young adolescents: variation across race/ethnicity and gender. Health Psychol Off J Div Health Psychol Am Psychol Assoc. 2014;34(1):1–9.
Telford RM, Telford RD, Olive LS, Cochrane T, Davey R. Why are girls less physically active than boys? Findings from the LOOK longitudinal study. Plos One. 2016;11(3):e0150041.
Vale S, Trost S, Ruiz JJ, Rêgo C, Moreira P, Mota J. Physical activity guidelines and preschooler’s obesity status. Int J Obes. 2013;37(10):1352–5.
Page A, Cooper AR, Stamatakis E, Foster LJ, Crowne EC, Sabin M, et al. Physical activity patterns in nonobese and obese children assessed using minute-by-minute accelerometry. Int J Obes. 2005;29(9):1070–6.
Zabinski MF, Saelens BE, Stein RI, Hayden-Wade HA, Wilfley DE. Overweight children’s barriers to and support for physical activity. Obes Res. 2003;11(2):238–46.
Jodkowska M, Oblacińska A, Nałęcz H, Mazur J. Perceived barriers for physical activity in overweight and obese adolescents and their association with health motivation. Dev Period Med. 2017;21(3):248–58.
Stankov I, Olds T, Cargo M. Overweight and obese adolescents: what turns them off physical activity? Int J Behav Nutr Phys Act. 2012;9(1):53.
Mack JW, McFatrich M, Withycombe JS, Maurer SH, Jacobs SS, Lin L, et al. Agreement between child self-report and caregiver-proxy report for symptoms and functioning of children undergoing cancer treatment. JAMA Pediatr. 2020;174(11):e202861.
Martin SR, Zeltzer LK, Seidman LC, Allyn KE, Payne LA. Caregiver-child discrepancies in reports of child emotional symptoms in pediatric chronic pain. J Pediatr Psychol. 2020;45(4):359–69.
Troiano RP, McClain JJ, Brychta RJ, Chen KY. Evolution of accelerometer methods for physical activity research. Br J Sports Med. 2014;48(13):1019–23.
Fang K, Mu M, Liu K, He Y. Screen time and childhood overweight/obesity: a systematic review and meta-analysis. Child Care Health Dev. 2019;45(5):744–53.
Lissak G. Adverse physiological and psychological effects of screen time on children and adolescents: literature review and case study. Environ Res. 2018;164:149–57.
Stiglic N, Viner RM. Effects of screentime on the health and well-being of children and adolescents: a systematic review of reviews. BMJ Open. 2019;9(1):e023191.
LeBlanc AG, Katzmarzyk PT, Barreira TV, Broyles ST, Chaput JP, Church TS, et al. Correlates of Total sedentary time and screen time in 9–11 year-old children around the world: the international study of childhood obesity, lifestyle and the environment. Plos One. 2015;10(6):e0129622.
Dumuid D. Screen time in early childhood. Lancet Child Adolesc Health. 2020;4(3):169–70.
Elgar FJ, Stewart JM. Validity of self-report screening for overweight and obesity. Evidence from the Canadian community health survey. Can J Public Health Rev Can Sante Publique. 2008;99(5):423–7.
Acknowledgements
Not applicable.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The (co) authors would like to acknowledge and offer our sincere gratitude to all the participating school districts, schools, families, research staff, and state-wide partners who contributed to the success of Texas SPAN. This study was funded by the Texas Department of State Health Services with funds from the Title-V Maternal and Child Health Block Grant to Texas, Centers for Disease Control and Prevention Health and Human Services Block Grant, and the Michael and Susan Dell Foundation through the Michael and Susan Dell Center for Healthy Living. The Texas Department of State Health Services collaborated with the Michael and Susan Dell Center for Healthy Living to design the study, and this article was written with a coauthor from the Texas Department of State Health Services. The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement, by Texas DSHS, HRSA, HHS, or the U.S. Government.’
Author information
Authors and Affiliations
Contributions
GB, RB, NR, DH, DB, and GK were responsible for the concept and design of the study, analysis of the data, and revision of the manuscript. GB, RB, and GK were responsible for interpretation of the data and drafting the manuscript. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Written child assent and informed consent were obtained from all Texas SPAN participants and primary caregivers to use their data for research and publication purposes. All methods were carried out in accordance with the Declaration of Helsinki. This study was reviewed and approved by the Committee for the Protection of Human Subjects at the University of Texas Health Science Center at Houston (UTHealth) (HSC-SPH-00-056), the Texas Department of State Health Services Institutional Review Board (IRB# 04–062), and local school district review committees.
This study was reported, and methods were carried out in accordance to the Strengthening the Report of Observational studies in Epidemiology (STROBE) guidelines.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Bejarano, G., Brayton, R.P., Ranjit, N. et al. Weight status and meeting the physical activity, sleep, and screen-time guidelines among Texas children: results from a population based, cross-sectional analysis. BMC Pediatr 22, 428 (2022). https://doi.org/10.1186/s12887-022-03488-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-022-03488-8