
Abstract
Aim
Globally, hypertension is one of the main threats to public health and a significant risk factor predisposing individuals to various cardiovascular conditions. Hypertension in the young is particularly complex and challenging. Accumulating evidence has implicated that low birth weight is vital for elevated blood pressure, and birth weight was negatively correlated with blood pressure. However, fewer studies with conflicting results have addressed the associations between birth weight and blood pressure in children and adolescents, and there is no relevant research conducted in the NHANES population. The principal objective of this project was to investigate the relationship between birth weight and blood pressure in children and adolescents in NHANES.
Methods
A total of 7600 subjects aged 8 to15 were enrolled in the present study from the National Health and Nutrition Examination Survey (NHANES) 2007–2018. Outcome variables were systolic blood pressure(SBP) and diastolic blood pressure(DBP). Birth weight was regarded as an independent variable. EmpowerStats software and R (version 3.4.3) were performed to examine the association between birth weight and SBP or DBP.
Results
Birth weight was negatively correlated with SBP in the fully-adjusted model(β = -0.02, 95%CI: -0.04 to -0.04, p = 0.0013), especially in non-Hispanic White (β = -0.03, 95%CI: -0.06 to -0.00,p = 0.0446), aged between 13 to 15(β = -0.03, 95%CI: -0.04 to -0.01, p = 0.0027), and male individuals(β = -0.03, 95%CI: -0.05 to -0.01, p = 0.0027). However, there was no unidirectional association between birth weight and DBP in the fully adjusted model(β = -0.01, 95%CI: -0.03 to 0.02, p = 0.5668) and in sub-analysis. An inverted U-shaped and J-shaped relationship was uncovered between birth weight and DBP in those aged 13 or above and Mexican Americans, respectively. The inflection point calculated by a recursive algorithm of birth weight in these groups was all 105 oz.
Conclusions
The current study identified that birth weight was negatively related to SBP but not significantly related to DBP in children and adolescents aged 8 to 15, highlighting different potential mechanisms behind high SBP and high DBP in the young. However, an inverted U-shaped and J-shaped relationship between birth weight and DBP was observed, suggesting that targeted intervention measures should be taken for different groups of people rather than generalizations.
Similar content being viewed by others

Introduction
Hypertension, a global threat to human health, substantially increases the risk of cardiovascular diseases and is a prominent contributor to mortality with more than 1 billion cases [1, 2]. Along with the improvement in the social economy and the aging of the population, the incidence of hypertension is rising at an alarming rate. In China, the prevalence of hypertension is 23.2% [3], while in the United States, the situation may be even more critical [4]. Notably, recent studies have also shown that high BP in adolescents and children is also a worrisome concern [5,6,7]. The United States is burdened with an increased incidence of hypertension in children and adolescents constantly, seriously hindering the development and health of the young [6, 8, 9].
Hypertension is a multifactorial disorder with complex mechanisms and numerous causes arising from the interplay of lifestyles, living conditions, and genetic factors [10, 11]. In addition, accumulating evidence has implicated that birth weight is a vital element for elevated blood pressure, implying that adverse effects in early life may be another etiology of hypertension. Various observational studies have detected an inverse relationship between birth weight and blood pressure [12,13,14]. For instance, Al Salmi I et al. [12] revealed in their study that birth weight was reversely associated with both SBP and DBP in a representative Austrian population. Consistent with the previous findings, a cross-sectional study in China suggested that low birth weight was related to an increased hypertension risk in adolescent girls, irrespective of BMI [13].
However, the current research on the relationship between birth weight and blood pressure is partly controversial and even completely contradictory [15,16,17]. Lai C et al. [16] found a U-shaped relationship between birth weight and blood pressure, especially SBP. They believed that birth weight and blood pressure were unidirectional but a complex relationship that is affected by a combination of various factors. Moreover, a sizeable Mendelian randomization analysis failed to detect an inverse relationship between birth weight and blood pressure [15]. Another similar study on birth weight and blood pressure in rural subjects also highlighted this issue [17].
Additionally, fewer studies with conflicting results have addressed the associations between birth weight and blood pressure in children and adolescents, and there is no relevant research conducted in the NHANES population. Therefore, we proposed this study to investigate the relationship between birth weight and blood pressure in NHANES, which has tremendous clinical implications for promoting the health of adolescents and reducing the risk of cardiovascular disease in adulthood.
Methods
Study population
The National Health and Nutrition Examination Survey (NHANES), a population-based survey conducted by the National Center for Health Statistics (NCHS), is a publicly used data set used to record the health status and related personal and lifestyle characteristics of all civilians in the United States. A multi-stage, complex clusters, probabilistic sample design is used for data acquisition and analysis to achieve a nationally representative rather than a simple random sample from the general US population [18]. In particular, the Centers for Disease Control and Prevention (CDC) is responsible for preparing and disseminating data files to provide full access to the data [19]. The present study analyzed the NHANES data collected from 2007 to 2018, which contained cross-sectional socio-demographic, dietary, and medical records obtained by questionnaires, standard physical examinations, and laboratory tests conducted in authoritative laboratories.
A total of 9094 subjects aged between 8–15 were enrolled in the primary analysis. The inclusion criteria were subjects who had self-reported birthweight with valid blood pressure records. We adhered to the following exclusion criteria:(1) individuals with missing birth weight or with invalid information; (2) those without blood pressure records;(3) those with self-reported severe diseases such as cancer and any other congenital diseases. The final sample size for analysis was 7600, after excluding the participants as mentioned above. The NCHS Ethics Review Committee supports this study, and each subject also signed a written informed consent [20].
Variables
Blood pressure, including SBP and DBP, and birth weight were treated as dependent and independent variables, respectively. Proxy-reported birth weight data are only available for individuals aged 15 and under. Birth weight was recorded in pounds and ounces and converted into ounces in the final analysis. According to the World Health Organization (WHO) definition, low birth weight means that the birth weight is less than 2,500 g [21], which is about 88.2 oz. Therefore, we divide the research objects into two groups(< 88.2 oz and > = 88.2 oz).
In addition, the following variables were collected and analyzed in the current study: age, race/ethnicity, gender, the ratio of family income to poverty, height, weight, body mass index (BMI), waist circumference, triglyceride (TG), total cholesterol (TC), LDL-cholesterol (LDL), plasma fasting glucose (FBG), uric acid (UA), creatinine (Cr), blood urea nitrogen (BUN) and glycohemoglobin. Also, associated risk factors, including the mother's age when the child was born, were also collected and analyzed. As BMI in the young varies with gender and age, we calculate age- and sex-specific BMI to evaluate weight status by using height and weight measurements gathered from the physical examination [22]. We defined overweight and obesity by using CDC criteria, which define overweight as age- and sex-specific BMI ≥ 85th percentile and obesity as BMI ≥ 95th percentile [23].
Blood pressure measurement procedure: After all subjects rested quietly for at least 5 min in the Mobile Inspection Center (MEC), the appropriate cuff was selected according to the size of the subject's upper arm. Three consecutive blood pressure readings will be obtained once the participant's maximum inflation level (MIL) is determined. If the measurement is interrupted or incomplete, or invalid, a fourth reading will be undertaken. An average value of all valid readings was served as the final blood pressure.
Missing value management: We excluded subjects with missing independent or dependent variables. The missing continuous variables were replaced by the median. The missing categorical variables were regarded as a separate group.
Any detailed information about the variables acquisition process is described at www.cdc.gov/nchs/nhanes/.
Statistical analyses
We used the weighted analysis to obtain national representation following the NCHS Analysis Recommendation. The continuous variables were characterized by mean ± standard deviation, or median and interquartile range when appropriate. The categorical variables were presented as a percentage(%). The P-value was calculated using a weighted chi-squared test for categorical variables and a linear regression model for continuous variables. The association between birth weight and blood pressure, including SBP and DBP, was analyzed using multivariable linear regression. To further analyze the relationship between birth weight and SBP as well as DBP, we used the following three models: Model 1: No adjustment for variables; Model 2: Gender, age, and race/ethnicity were adjusted; Model 3: All underlying covariates including sex, age, race/ethnicity, ratio of family income to poverty, height, weight, BMI, waist circumference, TG, TC, LDL, FBG, UA, Cr, BUN, glycohemoglobin and mothers' age when born were adjusted.
In addition to further data research, we subsequently performed subgroup analysis stratified by age, gender, and race/ethnicity. A weighted generalized additive model and a smooth curve fitting were conducted to address nonlinearity afterward. When nonlinearity was uncovered, we first calculated the vital inflection point using a recursive algorithm and then conducted a weighted two-piecewise linear regression model on both sides of the inflection point. The statistical analyses were performed using R software (version 3.4.3, http://www.Rproject.org) and EmpowerStats software (http://www.empowerstats.com). The results would be considered to be statistically significant if a two-sided p-value of < 0.05.
Results
Weighted characteristics, including socio-demographic and laboratory data of 7600 responders in the present study, are reported and summarized in Table 1. Among all the research objects, the average was 11.54 ± 2.31 years old. Overall, the proportion of males was slightly higher than females: 51.06% were boys, and 48.94% were girls. A higher proportion non-Hispanic White subjects were included in the study(54.67%) compared with non-Hispanic Black(13.90%) and Mexican Americans (14.90%), and other race/ethnicity(16.54%). In comparison to those with a birth weight less than 88.2 oz, the SBP was much lower in those with heavier birth weights, while DBP was equal in the two groups. Pulse, height, weight, mother's age when born, and the ratio of family income to poverty were all of great statistical significance between the two groups. In addition, those with a birth weight more than 88.2 oz tend to have a high proportion of obesity in their later life when compared to those with a birth weight less than 88.2 oz(24.60% vs. 18.50%). Detailed descriptions of the participants in the study are listed in Table 1.
A clear inverse relationship can be observed between birth weight and SBP in the fully-adjusted model(β = -0.02, 95%CI: -0.04 to -0.04, p = 0.0013). In sub-analysis stratified by gender, age, race/ethnicity, this negative association was more obvious in males(β = -0.03, 95%CI: -0.05 to -0.01, p = 0.0027), and age > = 13 years old(β = -0.03, 95%CI: -0.04 to -0.01, p = 0.0027) and in non-Hispanic White (β = -0.03, 95%CI: -0.06 to -0.00,p = 0.0446) (Table2, Fig. 1).

Relationship between birth weight and SBP. a Each black point represents a sample. b The red line represents the smooth curve fit between variables. In comparison, blue bands represent the 95% CI. Sex, age, race/ethnicity, ratio of family income to poverty, height, weight, BMI, waist circumference, TG, TC, LDL, FBG,UA, Cr, BUN, glycohemoglobin and mothers' age when born were adjusted
Contrastingly and unexpectedly, there was no linear association between birth weight and DBP in the fully adjusted model(β = -0.01, 95%CI: -0.03 to 0.02, p = 0.5668) and sub-analysis stratified by gender, age, race/ethnicity(Table 3, Fig. 2).

Association between birth weight and DBP. a Each black point represents a sample. b The red line represents the smooth curve fit between variables. In comparison, blue bands represent the 95% CI. Sex, age, race/ethnicity, ratio of family income to poverty, height, weight, BMI, waist circumference, TG, TC, LDL, FBG,UA, Cr, BUN, glycohemoglobin and mothers' age when born were adjusted
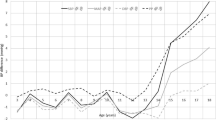
Furthermore, we performed a weighted generalized additive model and a smooth curve fitting stratified by age, gender, and race/ethnicity to detect the nonlinear relation between birth weight and SBP as well as DBP and further confirm the results (Fig. 3,4,5,6,7,8). An inverted U-shaped and J-shaped relationship was uncovered between birth weight and DBP in those aged 13 or above and Mexican Americans, respectively (Fig. 4, Fig. 8). According to the smoothing plot, we further performed a two-piecewise linear regression model to address birth weight's threshold effect on DBP. The inflection point calculated by a recursive algorithm of birth weight in these groups was all 105 oz (Table 4).

The relationship between birth weight and SBP, stratified by age

The association between birth weight C and DBP, stratified by age

The relationship between birth weight and SBP, stratified by gender

The association between birth weight C and DBP, stratified by gender

The relationship between birth weight and SBP, stratified by race/ethnicity

The association between birth weight C and DBP, stratified by race/ethnicity
Discussion
The present study utilized the population-based cross-sectional resources of NHANES to detect the correlation between birth weight and blood pressure in general children and adolescents aged 8 to 15, which, to our knowledge, was the first time to examine such a relationship in this population. We adjusted the socioeconomic conditions, physical measurement indicators, mother's age when born, and common predisposing risk factors for hypertension for all the participants. The major finding to emerge from the current study was that birth weight was negatively correlated with SBP even after adjusting for the relevant covariates, especially in White, aged between 13 to 15, and male individuals. However, there was no unidirectional relationship between birth weight and DBP. A somewhat unexpected finding is that for individuals aged between 13 to 15 and Mexican Americans, birth weight and DBP showed an inverted U-shaped relationship and an inverted J-shaped relationship, respectively.
Globally, hypertension, responsible for the increasing burden of disease, is one of the main threats to public health and a significant risk factor that predisposes individuals to various cardiovascular conditions [1, 24]. Hypertension in the young is particularly complex and challenging because it is demonstrated an increased risk of developing cardiovascular disorders later in adulthood [8, 25, 26]. As we all know, hypertension is a multifactorial disorder involving the combined effect of environment and genes with an unsatisfactory controlling rate [10, 11]. Continuing to explore the etiology of hypertension, especially in adolescence and childhood, has significant implications for preventing disease progression and improving global health. Low body weight, an indicator of congenital development dysplasia or an adverse intrauterine environment, has recently been thought to be widely implicated in high blood pressure and other cardiovascular diseases [27, 28].
Barker et al. [29] first proposed the hypothesis of birth weight and later cardiovascular risk in adulthood. A large number of subsequent studies also confirmed the conclusions of the predecessors [30,31,32,33]. A Mendelian randomized study aimed at elucidating complex underlying biological mechanisms further corroborated previously published work [30]. The study identified a causal relationship between low birth weight and susceptibility to cardiovascular disease and diabetes, independent of adult obesity or high blood pressure. Recently, studies have further indicated that birth weight had a negative relationship with blood pressure, and low birth weight might lead to the risk of late increased blood pressure in adulthood [12,13,14, 28, 34, 35]. In agreement with earlier findings, the negative correlation between birth weight and SBP was also uncovered in children and adolescents even after adjusting for other relevant confounders, including the mother's age when born that may possess an elevation in blood pressure in the present study.
The following underlying mechanism may be involved in the reverse relationship between birth weight and blood pressure. Firstly, low birth weight caused by fetal dysplasia is a significant cause of increased blood pressure in later life. Low birth weight is considered an essential surrogate indicator of a poor and adverse intrauterine environment [36, 37]. Later, scholars advanced this theory to integrate the critical role of the kidney, indicating that the decrease in the number of nephrons at birth was a significant cause for diseases such as hypertension and coronary heart disease in adolescents and adulthood [12, 16, 38, 39]. In 2003, the kidney collected by Hughson M et al. [40] through autopsy confirmed that people with low birth weight had fewer nephrons, providing further evidence for the reverse association between birth weight and blood pressure. In addition, the developmental origin theory may further explain the negative relationship between birth weight and blood pressure, which believed that cardiovascular diseases originate from intrauterine development, not just traditional acquired [41].
Nevertheless, some studies have questioned the relationship between birth weight and blood pressure, and some scholars even draw contradictory conclusions [15,16,17, 42]. Inadequate adjustment of related variables and nonrepresentative study samples are the main reasons that may contribute to discrepant results [43]. Our research object is the nationally representative NHANES, and after adjusting BMI, weight, height, waist circumference, and common risk factors for high blood pressure such as FBG and blood lipids, this negative correlation between birth weight and SBP still exists. Moreover, we performed a subgroup analysis of different groups, and the same conclusions could be drawn.
Previous findings have revealed that birth weight was identified to be associated inversely with DBP in adults [12] and adolescents [44]. This negative correlation, conversely, has not been replicated in children and adolescents in the current research. Our findings suggested a nonidentical relationship between birth weight and DBP, which may imply that the influence of birth weight on DBP may be the result of a combination of multiple factors, including growth restriction in utero and acquired factors. Similar to our findings, an analysis of data from a census in six major urban areas in China showed that birth weight did not influence DBP [16]. Since China is a predominantly agricultural country, the objects of this study mainly collected from urban areas without rural regions, so the sample may not be nationally representative. The NHANES data used in our research is a typical nationally representative database based on demographic characteristics. We found this nonlinear relationship between birth weight and DBP and that the effect persisted after adjusting for potential confounding factors. Unlike SBP, DBP is not affected by birth weight, highlighting different potential mechanisms behind high SBP and high DBP in the young [16, 45]. As a result, more animal models and clinical studies are required to explain this relationship between birth weight and DBP in our observations.
In addition, we found that among participants at the age of 13 to 15 years and Mexican Americans, there was an inverted U-shaped and inverted J-shaped relationship between birth weight and blood pressure. Furthermore, these trends were not observed in those younger than 13, which may be related to different physical growth manner after the age of 13, such as changes in adolescent hormones, which requires further confirmation. Previous studies have found that different groups of people had different responses to blood pressure. For example, Keller G et al. [46] analyzed 10 patients with essential hypertension who died unexpectedly and found that White had significantly fewer nephrons. Our cross-sectional study found that birth weight and DBP formed a reverse J-shaped relationship in Mexican Americans. Specifically, when the birth weight was less than 105 oz, the effect on DBP was little. While the birth weight was greater than 105 oz, the diastolic blood pressure decreased by 1.06 mmHg for every ounce increase in birth weight. Additionally, our study also implies that for those aged 13 to 15, a birth weight less than 105 oz may contribute to an elevation in blood pressure.
To conclude, the current study identified that birth weight was negatively related to SBP but not significantly related to DBP in children and adolescents aged 8 to 15 during the NHANES 2007–2018. However, we observed an inverted U-shaped association between birth weight and DBP, with low and high levels being related to lower DBP in individuals aged 13 to 15. In addition, our current study indicates a reverse J characteristic curve between birth weight and DBP in Mexican Americans. It is well known that even a slight rise in blood pressure can increase the long-term risk of target organ damage and cardiovascular disease. Therefore, it is imperative to tease out the etiology of hypertension in the young and find potential preventive measures. Our findings have a number of profound implications in clinical practice. In the first place, our research supports the view that using precision medical measures to improve prenatal nutrition and growth to intervene in low-weight fetuses may improve cardiovascular fitness in adulthood. Secondly, for infants with low birth weight, standardized monitoring of blood pressure and timely intervention, such as nutrition and diet adjustments, may help reduce the risk of hypertension, exceptionally high SBP. Lastly, birth weight has different effects on DBP for different groups of people, suggesting that targeted intervention measures should be taken rather than generalizations.
Nevertheless, this study still has the following primary deficiencies. First, this is a cross-sectional study, and the birth weight data reported by the agency may have some recall bias. Second, there is a lack of dynamic information regarding the impact of birth weight on adolescents' blood pressure. Finally, the absence of data about underlying confounding factors such as gestational age, puberty development, physical activities, and other unidentified prognostic factors was another flaw of the study. Our findings should be interpreted with caution, given the above limitations. Prospective studies examining infants and tracking their blood pressure in adulthood to verify the causal effect of birth weight on hypertension are imperative and urgent.
Availability of data and materials
The data used to support the findings of this study are available from corresponding author upon request.
References
Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, Amann M, Anderson HR, Andrews KG, Aryee M, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet (London, England). 2012;380(9859):2224–60.
Lawes CM, Vander Hoorn S, Rodgers A. Global burden of blood-pressure-related disease, 2001. Lancet (London, England). 2008;371(9623):1513–8.
Li M, Zhan A, Huang X, Hu L, Zhou W, Wang T, Zhu L, Bao H, Cheng X. Positive association between triglyceride glucose index and arterial stiffness in hypertensive patients: the China H-type Hypertension Registry Study. Cardiovasc Diabetol. 2020;19(1):139.
Liu B, Sun Y, Xu G, Rong S, Zhang J, Du Y, Snetselaar LG, Robinson JG, Wallace RB, Bao W. Long-Term Trends in Hypertension and Elevated Blood Pressure Among U.S. Adults, 1999 to 2016. J Am College Cardiol. 2018;72(17):2089–91.
Yang L, Yang L, Zhang Y, Xi B. Prevalence of Target Organ Damage in Chinese Hypertensive Children and Adolescents. Front Pediatr. 2018;6:333.
Chen X, Wang Y. Tracking of blood pressure from childhood to adulthood: a systematic review and meta-regression analysis. Circulation. 2008;117(25):3171–80.
Gartlehner G, Vander Schaaf EB, Orr C, Kennedy SM, Clark R, Viswanathan M. Screening for Hypertension in Children and Adolescents: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA. 2020;324(18):1884–95.
Hardy ST, Sakhuja S, Jaeger BC, Urbina EM, Suglia SF, Feig DI, Muntner P. Trends in Blood Pressure and Hypertension Among US Children and Adolescents, 1999–2018. JAMA Netw Open. 2021;4(4):e213917.
Flynn JT, Kaelber DC, Baker-Smith CM, Blowey D, Carroll AE, Daniels SR, de Ferranti SD, Dionne JM, Falkner B, Flinn SK, et al. Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and Adolescents. Pediatrics. 2017;140(3):e20171904.
Caillon A, Paradis P, Schiffrin EL. Role of immune cells in hypertension. Br J Pharmacol. 2019;176(12):1818–28.
Di Raimondo D, Buscemi S, Musiari G, Rizzo G, Pirera E, Corleo D, Pinto A, Tuttolomondo A. Ketogenic Diet, Physical Activity, and Hypertension-A Narrative Review. Nutrients. 2021;13(8):2567.
Al Salmi I, Hannawi S. Birth weight is inversely correlated with blood pressure: population-based study. J Hypertens. 2020;38(11):2205–14.
Wang X, Dong Y, Zou Z, Ma J, Yang Z, Gao D, Li Y, Nguyen MT. Low Birthweight Is Associated with Higher Risk of High Blood Pressure in Chinese Girls: Results from a National Cross-Sectional Study in China. Int J Environ Res Public Health. 2019;16(16):2898.
Dior UP, Karavani G, Bursztyn M, Paltiel O, Calderon-Margalit R, Friedlander Y, Youssim I, Manor O, Hochner H. Birth Weight and Maternal Body Size as Determinants of Blood Pressure at Age 17: Results from the Jerusalem Perinatal Study Cohort. Matern Child Health J. 2021;25(1):162–71.
Zheng Y, Huang T, Wang T, Mei Z, Sun Z, Zhang T, Ellervik C, Chai JF, Sim X, van Dam RM, et al. Mendelian randomization analysis does not support causal associations of birth weight with hypertension risk and blood pressure in adulthood. Eur J Epidemiol. 2020;35(7):685–97.
Lai C, Hu Y, He D, Liang L, Xiong F, Liu G, Gong C, Luo F, Chen S, Wang C, et al. U-shaped relationship between birth weight and childhood blood pressure in China. BMC Pediatr. 2019;19(1):264.
Monyeki K, Kemper H, Mogale A, Hay L, Sekgala M, Mashiane T, Monyeki S, Sebati B. Association between Blood Pressure and Birth Weight among Rural South African Children: Ellisras Longitudinal Study. Int J Environ Res Public Health. 2017;14(9):974.
Fain JA. NHANES. Diabetes Educ. 2017;43(2):151.
Ahluwalia N, Dwyer J, Terry A, Moshfegh A, Johnson C. Update on NHANES Dietary Data: Focus on Collection, Release, Analytical Considerations, and Uses to Inform Public Policy. Advances in nutrition (Bethesda, Md). 2016;7(1):121–34.
Frediani JK, Naioti EA, Vos MB, Figueroa J, Marsit CJ, Welsh JA. Arsenic exposure and risk of nonalcoholic fatty liver disease (NAFLD) among U.S. adolescents and adults: an association modified by race/ethnicity, NHANES 2005–2014. Environ health. 2018;17(1):6.
Sema A, Tesfaye F, Belay Y, Amsalu B, Bekele D, Desalew A. Associated Factors with Low Birth Weight in Dire Dawa City, Eastern Ethiopia: A Cross-Sectional Study. Biomed Res Int. 2019;2019:2965094.
Skinner AC, Ravanbakht SN, Skelton JA, Perrin EM, Armstrong SC. Prevalence of Obesity and Severe Obesity in US Children, 1999–2016. Pediatrics. 2018;141(3):e20173459.
Kuczmarski RJ, Ogden CL, Guo SS, Grummer-Strawn LM, Flegal KM, Mei Z, et al. 2000 CDC Growth Charts for the United States: methods and development. Vital Health Stat 11. 2002;(246):1–190.
Grassi G. Assessment of sympathetic cardiovascular drive in human hypertension: achievements and perspectives. Hypertension. 2009;54(4):690–7.
Tran AH, Urbina EM. Hypertension in children. Curr Opin Cardiol. 2020;35(4):376–80.
Anyaegbu EI, Dharnidharka VR. Hypertension in the teenager. Pediatr Clin North Am. 2014;61(1):131–51.
Knop MR, Geng TT, Gorny AW, Ding R, Li C, Ley SH, Huang T. Birth Weight and Risk of Type 2 Diabetes Mellitus, Cardiovascular Disease, and Hypertension in Adults: A Meta-Analysis of 7 646 267 Participants From 135 Studies. J Am Heart Assoc. 2018;7(23):e008870.
Raghuraman RP, Duffy D, Carroll VA, Manyonda I, Antonios TF. Oxygen therapy in premature low birth weight infants is associated with capillary loss and increases in blood pressure: a pilot study. J Hum Hypertens. 2020;34(4):278–85.
Barker DJ, Bull AR, Osmond C, Simmonds SJ. Fetal and placental size and risk of hypertension in adult life. BMJ (Clinical research ed). 1990;301(6746):259–62.
Zanetti D, Tikkanen E, Gustafsson S, Priest JR, Burgess S, Ingelsson E. Birthweight, Type 2 Diabetes Mellitus, and Cardiovascular Disease: Addressing the Barker Hypothesis With Mendelian Randomization. Circulation Genomic and precision medicine. 2018;11(6):e002054.
Nomura K, Kido M, Tanabe A, Nagashima K, Takenoshita S, Ando K. Investigation of optimal weight gain during pregnancy for Japanese Women. Sci Rep. 2017;7(1):2569.
Stillerman KP, Mattison DR, Giudice LC, Woodruff TJ. Environmental exposures and adverse pregnancy outcomes: a review of the science. Reproductive sciences (Thousand Oaks, Calif). 2008;15(7):631–50.
Tilling K, Davies N, Windmeijer F, Kramer MS, Bogdanovich N, Matush L, Patel R, Smith GD, Ben-Shlomo Y, Martin RM. Is infant weight associated with childhood blood pressure? Analysis of the Promotion of Breastfeeding Intervention Trial (PROBIT) cohort. Int J Epidemiol. 2011;40(5):1227–37.
Smal JC, Uiterwaal CS, Bruinse HW, Steendijk P, van Bel F. Inverse relationship between birth weight and blood pressure in growth-retarded but not in appropriate for gestational age infants during the first week of life. Neonatology. 2009;96(2):86–92.
Mu M, Wang SF, Sheng J, Zhao Y, Li HZ, Hu CL, Tao FB. Birth weight and subsequent blood pressure: a meta-analysis. Arch Cardiovasc Dis. 2012;105(2):99–113.
Javaid MK, Prieto-Alhambra D, Lui LY, Cawthon P, Arden NK, Lang T, Lane NE, Orwoll E, Barrett-Conner E, Nevitt MC, et al. Self-reported weight at birth predicts measures of femoral size but not volumetric BMD in eldery men: MrOS. J Bone Miner Res. 2011;26(8):1802–7.
Telerant A, Dunietz GL, Many A, Tauman R. Mild Maternal Obstructive Sleep Apnea in Non-obese Pregnant Women and Accelerated Fetal Growth. Sci Rep. 2018;8(1):10768.
Coats LE, Davis GK, Newsome AD, Ojeda NB, Alexander BT. Low Birth Weight, Blood Pressure and Renal Susceptibility. Curr Hypertens Rep. 2019;21(8):62.
Brenner BM, Garcia DL, Anderson S. Glomeruli and blood pressure. Less of one, more the other? Am J Hypertension. 1988;1(4):335–47.
Hughson M, Farris AB 3rd, Douglas-Denton R, Hoy WE, Bertram JF. Glomerular number and size in autopsy kidneys: the relationship to birth weight. Kidney Int. 2003;63(6):2113–22.
Barker DJ. The origins of the developmental origins theory. J Intern Med. 2007;261(5):412–7.
Mann KD, Basterfield L, Wright C, Parkinson K, Reilly JK, Reilly JJ, Adamson AJ, Pearce MS. Birth weight and adolescent blood pressure measured at age 12 years in the Gateshead Millennium Study. J Dev Orig Health Dis. 2019;10(6):621–6.
Edvardsson VO, Steinthorsdottir SD, Eliasdottir SB, Indridason OS, Palsson R. Birth weight and childhood blood pressure. Curr Hypertens Rep. 2012;14(6):596–602.
de Beer M, Vrijkotte TG, Fall CH, van Eijsden M, Osmond C, Gemke RJ. Associations of Infant Feeding and Timing of Weight Gain and Linear Growth during Early Life with Childhood Blood Pressure: Findings from a Prospective Population Based Cohort Study. PLoS ONE. 2016;11(11):e0166281.
Pietrobelli A, Agosti M, Zuccotti G. Putting the Barker Theory into the Future: Time to Act on Preventing Pediatric Obesity. Int J Environ Res Public Health. 2016;13(11):1151.
Keller G, Zimmer G, Mall G, Ritz E, Amann K. Nephron number in patients with primary hypertension. N Engl J Med. 2003;348(2):101–8.
Acknowledgements
The authors appreciate the time and effort given by participants during the data collection phase of the NHANES project.
Funding
This work was funded by the National Natural Science Foundation of China (No.82160072) and the Science and Technology Support Project of Enshi Prefecture Science and Technology Bureau (No.D20210024).
Author information
Authors and Affiliations
Contributions
All authors made a significant contribution to the work reported, whether that is in the study design, acquisition of data, statistics analysis; HR and YSX took part in drafting, revising or critically reviewing the article; YHL is the article’s guarantor; All authors read and approve the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was granted ethical approval by the National Center for Health Statistics (NCHS). The study was carried out following the ethical standards of the responsible committee on human experimentation and with the 1975 Helsinki Declaration and its later amendments. Furthermore, written informed consent was received from each subject.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no conflicts of interest to disclose, financially or otherwise.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Huang, R., Yang, S. & Lei, Y. Birth weight influences differently on systolic and diastolic blood pressure in children and adolescents aged 8–15. BMC Pediatr 22, 278 (2022). https://doi.org/10.1186/s12887-022-03346-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-022-03346-7