
Abstract
Background
Malnutrition is a critical public health issue that has been related to a significant increase in mortality and morbidity rates. Despite the fact that children are expected to benefit from home gardening products, their nutritional condition in Ethiopia, particularly in the planned study region, is not thoroughly monitored. Therefore the purpose of this is to determine the nutritional status of 6–59 months of age children between households with and without home gardening practices at Zege.
Methods
A community based comparative cross-sectional study was conducted among paired mothers with 6–59 month children from February to March 2020. Data were collected using questionnaire and anthropometric measurement tools. Binary logistic regression models were used. A-p-value < 0.05 was used as cutoff point to declare statistically significant variables with the outcome variable.
Result
Stunting and wasting among children aged 6–59 months was high and did not show significant variation between households practicing home gardening (stunting 46.1%, at 95%, CI: 40.6–51.3 and wasting 9.1%, at 95% CI: 6.2–12.7) and not practiced home gardening (stunting 50.3%, at 95% CI: 44.5–55.8 and wasting 10.1%, 95% CI: 6.8–13.8). Having low dietary diversity (AOR = 2.7; 95% CI: 1.9–3.9), Being male (AOR = 2.1; 95% CI: 1.4–3), feeding frequency < 3/day (AOR = 1.7; 95% CI: 1.1–2.4), and presence of diarrhea (AOR = 2.6; 95% CI: 1.4–4.6) were predictors of stunting. Unprotected-drinking water (AOR = 2.1; 95% CI: 1.0–4.2), not fully-immunized (AOR = 2.6; 95% CI: 1.3–5.1) and being female (AOR = 2.4; 95% CI: 1.3–4.6) were predictors for child wasting.
Conclusion
stunting and wasting are highly prevalent in both home gardening and non- home gardening households’ children of the community. Promoting diversified diet, protected water source, vaccinating children, access to a healthy environment and integrated with the access of nutrition education programs are vital interventions to improve nutrition.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Introduction
Malnutrition, defined as being either undernourished or over nourished, is a serious public-health issue that has been linked to a significant increase in the risk of mortality and morbidity [1]. Child malnutrition causes a delay in physical growth and motor development, lower intellectual quotient (IQ), greater behavioral problems, a lack of skills, susceptibility to contracting diseases, chronic illnesses in adulthood which can have an intergenerational effects, [2, 3]. Wasting, stunting, and underweight are defined as Z-scores less than − 2 standard deviations of weight for height, height for age, and weight for age, respectively [4].
Globally, 150.8 million under the age of five children were stunted, and 50.5 million children were wasted [5]. Malnutrition is an underlying cause for nearly half (45%) of child deaths, particularly in low socioeconomic communities, with more than 7 million women suffering from complications due to vitamin A deficiency and causing deaths in 6–8 percent of the children under the age of five in Africa and Asia [6]. Furthermore, the, overall under-5 mortality rate due to malnutrition was 55 deaths per 1,000 live births [7]. Under nutrition remains a major public health concern in developing countries, as a result of a combination of poor dietary consumption, infection such as diarrhea, household food insecurity, and poor sanitation practices [8]. Malnutrition is one of the most serious public health issues in Ethiopia, and one of the world's largest [9]. Stunting is extremely common in Ethiopia, ranging from (49% in Tigre to 14% in Addis Ababa), and wasting has varying figures in different parts of the country, reaching up to 21 percent in Afar [10, 11].
Despite the achievements in agricultural productivity, access to basic health services and education around the worldwide, the progress of malnutrition especially under nutrition reduction has been characterized by poor nutritional outcomes and lag in measures of social and economic progress [12]. Similarly the 2018 Global Nutrition Report finds again that the problem of malnutrition remains severe, the world is falling short of its goals, and that malnutrition in all its forms remains unacceptably high across all regions of the world [13].
Multiple strategies are required to address the issue of malnutrition, food production and food security, and home gardening practice is one of nutrition sensitive intervention systems in many developing countries and is widely used as a remedy to alleviate hunger and malnutrition [14]. Evidences suggests that home garden food production played a role in improving household dietary intake and income earning, lowering the proportion of under-five malnutrition, and increasing women’s involvement in household decision making [15,16,17,18]. Furthermore, despite the Ethiopian government's development of a Food and Nutrition Policy (FNP), a National Nutrition Program (NNP), and the Sequta Declaration to end all forms of malnutrition in children under the age of five, malnutrition remains a public health problem [19,20,21].
Inadequate food intake, food insecurity, inadequate child care, illness such as diarrhea and other infections, lack of sanitation, low maternal education, low socioeconomic status, low Dietary Diversity Score (DDS), and rural residency are all risk factors for child malnutrition [7, 22,23,24].
Despite the fact that there is information on the effects of home gardening on child nutrition, well-organized and documented evidences are lacking in Ethiopia. One reason for this evidence scarcity could be the country's limited use of home gardening practices, particularly in the proposed study area.
This study is aimed to compare the nutritional status and associated factors among children aged 6–59 months between HHs with and without home gardening practice in rural town of Bahir Dar city administration Zege North West Ethiopia.
Methods and materials
Study setting and Period
The study was conducted in Zege, from February 10th to March 10th /2020. Zege is one of the Bahr-Dar city administrations rural satellite town found 32 km far from Bahir Dar, the capital of Amara National Regional state. Zege peninsula is found around religious area and households didn’t have enough farm lands for production of diversified croups [25].
Based on 2019 population projection given from Bahir Dar city administration, the current population size of Zege is 10,083 (Male 4041, Female 6042). For administrative purpose Zege has 03 Keble’s and 2142 total HHS, 709 with home gardening and1433 without home gardening. Zege has 01 health centers and 03 health posts and each of health facility giving health care service to the population of Zege and nearby population [26].
Study design and populations
A Community based comparative cross-sectional study was used to determine nutritional status of children aged 6–59 months and its associated factors between Households with and without home gardening at Zege rural town of Bahr-Dar city administrations northwest Ethiopia. All care givers and 6–59 month of age children with and without home gardening were included in the study.
Sample size determination
The required sample size of the study was determined by using double population proportion formula by considering the following assumption.95% confidence level,80% power, of the study, P1 and P2 the prevalence of stunting in home gardening and non-home gardening populations, respectively.
p1 = prevalence of stunting of under five children with home garden 41% from previous study (South Ethiopia) [27] P2 = prevalence of stunting of under five children without home garden 52.5% from previous study (East Gojam) [8]. Finally, by taking 10% non-response rate the total sample size was 647.
Sampling technique and sampling procedure
First, Kebeles (the smallest administrative unit in the country) in the district were stratified based on home gardening status (home garden user and non-home garden users and non-irrigation users). The total number of 6–59 months old children in each kebeles were taken from the respective households using the registration book at health posts. Then, the calculated sample size (648), 324 for each group were selected using simple random sampling (computer generating method) technique whenever there were two or more under- five children, in the house, the youngest child was selected in order to avoid recall bias.
Data collection tools and procedures
Different types of tools and measurements were implemented to collect the required data. Structured interviewer administered questionnaire was developed by reviewing different literature. The questionnaire has sections like socio-demographic, and/or socioeconomic characteristics, nutrition related, wash related, health related factors and anthropometric measurements. After HHs who have 6–59 months of age children were selected from health posts, then data collectors were go to house to house for interview. Four clinical nurses and two health officer were assigned for data collection and supervisor respectively.
Weight and height of children were taken using the standard anthropometric measurement procedures outlined in the measurement guide prepared by the Food and Nutrition Technical Assistance (FANTA) project in 2007 [28]. Body weight was measured using portable weighing scale in light clothing with no jackets or coats, shoes, and additional clothing to the nearest 0.1 kg. For child less than two or unable to stand was the difference between weight of the mother caring the child and the weight of the mother alone on a new calibrated portable scale. Weighing scale was calibrated before and after any measurement. Height of children was measured using a portable stadiometer with no shoes; the shoulders, buttocks, and the heels touched the vertical stand with the head in Frankfurt plane to the nearest 0.1 cm. Children with 6–23 months of age, recumbent length the nearest to 1 mm and for children 24- 59 months of age, standing height to the nearest 0.1 cm was measured.
Both height and weight was recorded with two decimal places. Age of each child was also collected from the mother and counter-checked using vaccination cards or other forms of informal recording. All anthropometric measurements were taken twice, and the average of the two measurements were calculated and recorded.
Dietary diversity of children
A 24-h recall method (from sun rise to sun rise) was used to assess dietary diversity practices. It was based on the mother’s recall of foods given to her child in the previous24 hours prior to the interview date. Then, minimum dietary diversity was estimated using information collected from the24-hour dietary recall. Minimum dietary diversity was fulfilled if a child had received four or more food groups from the seven WHO food groups in the last 24 h preceding the survey. Seven food groups included were grains, roots, and tubers; legumes and nuts; dairy products (milk, yogurt, and cheese); flesh foods (meat, fish, poultry, and liver/organ meats); eggs; vitamin rich fruits and vegetables; and other fruits and vegetables [29].
Food security status of the households
determined based on nine standard Household Food Insecurity Access Scale (HFIAS) questions that were developed for this purpose by Food and Nutrition Technical Assistance (FANTA) [30].
Wealth index of the households
Was determined using the Principal Component Analysis (PCA) by considering latrine, water source, household assets, live-stock, and agricultural land ownership. Quintiles of the wealth score was created to categorize households as poor, medium and rich [31].
Data quality control
To maintain the quality of data, first, standardized data collection tools were developed in English and translated to Amharic (local language) for data collection then back to English for consistency. Pretest was done on 5% of the total sample size in other sites in order to evaluate the developed questioner. Weighing scale was calibrated before each measurement using known weight and all anthropometric measurements were taken twice, and the average of the two measurements were calculated and recorded. Two-day training was given for data collectors and supervisor prior to the actual data collection time on the selection procedure of study participants, purpose of the study, on the steps how they can give the necessary information for the participants when they start data collection. The supervisor and principal investigator were supervised and checked the completeness and quality of data daily. During data collection, questionnaires were reviewed and checked for completeness by the supervisor and principal investigators and the necessary feedback was offered to the data collectors in the next morning.
Data processing and analysis
The collected data was coded, entered and cleaned using Epi data version 3.02 and exported to SPSS version 23 for analysis. Descriptive statistics like frequency, percentage and mean were carried out for different variables. The association between two populations was cheeked using chi square test. Bi variable logistic regression analysis was used to know the crude association between each independent variables and outcome variable (stunting and wasting) and crude odds ratio was taken. Then variables which was associated with the dependent variable in bi-variable analysis with p value < 0.2 was included in the models of multivariable logistic regression analysis with backward likelihood ratio approach. Anthropometric data were converted in to indices and indicators using WHO Anthro software. P-value less than 0.05 in multivariable logistic regression analysis were used to conclude the presence of statistically significant association between different predictor variables with outcome variable (stunting and wasting). The strength of statistically association was measured by adjusted odds ratio at 95% confidence level.
Ethical consideration
Ethical clearance was obtained from ethical Review Board of Bahir Dar University College of Medicine and Health Sciences (CMHS/ IRB 01–008) and zonal health department and selected kebele through formal letter. Before collecting the data, informed consent was obtained from all participants/parents/legal guardians. Each study participants were informed about the purpose of the study and participation was voluntary without payment for their participation. Each study participants also were informed that the right to withdraw at any time during the interview. All gathered information were protected from its confidentiality, anonymity was explaining clearly to participant. Except for the principal investigator, information is not exposed to a third person.
Results
Socio demographic and economic characteristics of study participants
The study included 648 mothers and their children aged 6–59 months (with a 95.0 percent response rate). The mean (+ SD) age of the mothers and children in households (HHs) with home gardening was 28.7(5.5) years and 30.8(12.6) months, respectively, and 29.7(5.8) years and 29.1 (10.3) months in households without home gardening. Almost sixty-eight percent (67.9%) of mothers from HHs with home gardening and eighty percent (79.9%) of mothers from HHs without home gardening had no formal education. Nearly, all mothers in both HHs (with home gardening = 99.4% and without home gardening = 98.4%) were married. The mean (± SD) family size in this study was 4.2(± 1.1) from HHs with home gardening and 4.3(± 0.9) from HHs without home gardening. Sixty nine percent (69.2%) from HHs with home garden and fifty four percent (54.5%) from HHs without home gardening were food secure (Table 1).
Health, Nutrition and WASH related characteristics
The majority of mothers from HHs who did not practice home gardening (96.1 percent) and those who did practice home gardening (88.0 percent) had an ANC visit. More than three-quarters (96.4%) of children in HHs without a home garden were fully immunized. Eighty-six percent (86.4%) of children from HHs with a home garden were breastfed exclusively. At 6 months, more than half of the children in both households (67.2 percent in HHs with a home garden and 66.2 percent in HHs without a home garden) had begun complementary feeding. The dietary diversity score among children was higher in HHs with a home garden (67.5%) than in HHs without a home garden (34.4 percent). The majority of (85.4%) HHs without home gardening and (66.6%) HHs with home gardening mothers practiced good hand wa(Table 2)
Nutritional status of children from households with and without home gardening
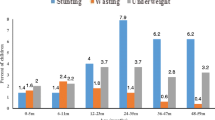
About forty-six percent (46.1%) of children from HHs with home gardening and 50.30% from HHs without home gardening were stunted. Eighteen percent (18.2%) of children from home gardening and almost thirty percent (29.9%) from non-home gardening were underweight. Whereas nine percent (9.1%) of children from home gardening households and ten percent (10.1%) of children from non-home gardening households were wasted. (Fig. 1).

Prevalence of stunting and wasting from HHs with and without home gardening in Zege Northwest Ethiopia, 2020
Factors associated with stunting among children aged 6–59 months in Zege, Northwest Ethiopia
In the bivariate logistic regression model, age of mother, resident of respondent, age of child, sex of child, educational status of mother, drinking water source, presence of latrine, take vitamin A, immunization, Prelactal feeding, DDS and food security status of the household were associated with stunting at P-value < 0.2. After controlling for potential confounders, the final multivariable logistic regression analysis revealed that sex of child, feeding frequency, DDS and presence of diarrhea were factors significantly associated with child stunting.
The odds of male children to become stunted was 2.0 times higher than female children (AOR = 2. 0, 95% CI: 1.4–3.0). It was also observed that the odds of children who had less than 3 feeding frequency to become stunted was 1.6 times higher than children who had > = 3 feeding frequency (AOR = 1.67, 95% CI: 1.1–2.4). Children who had diarrhea in the past two weeks prior to the study were 2.6 times more likely to be stunted than those children without diarrheal disease (AOR = 2.6, 95% CI: 1.4–4.6) and the odds of children who had low DDS to become stunted was 2.7 times higher than children who had high DDS (AOR = 2.7, 95% CI: 1.9–3.9) (Table 3).
Factors associated with wasting among children aged 6–59 months in Zege, Northwest Ethiopia
Among the variables entered into bivariate logistic regression analysis, drinking water source, hand washing practice of mother, immunization status of child, sex of child, presence of latrine, time to start complimentary feeding, take vitamin A and exclusive breast feeding were associated with child wasting at p-value < 0.2. However, after controlling for potential confounders, the final multivariable logistic regression analysis revealed that sex of child, drinking water source, and immunization status were factors significantly associated with child wasting.
Therefore the odds of female children to become wasted was 2.4 times higher than male children (AOR=2.4, 95% CI: 1.3-4.6) and the odds of children who didn’t fully immunized to become wasted was 2.6 times higher than children who were fully immunized (AOR=2.6, 95% CI: 1.3-5.1). Moreover the odds of children from unprotected water source households to become wasted was 2 times higher than their counterparts (AOR=2.09, 95% CI 1.03-4.2) (table 4).
Discussion
Agriculture, food security, and nutrition security are all intertwined issues in the human development [32]. Children's nutritional status is the result of complex interactions between food consumption, agricultural products, and the overall health status and health care practices [33]. Given this, increased agricultural productivity can contribute to improved livelihoods, including increased food consumption. The purpose of this study was to compare the nutritional status of children aged 6–59 months in Zege, North West Ethiopia, between households that practiced home gardening and those that did not.
In this study, The overall prevalence of stunting is 48% (95%, CI: 44.3–52.2). The finding are consistent with those of numerous studies conducted in various parts of the country [8, 9, 22, 23, 27]. However, The prevalence is higher than in the Amhara region and the country value [11] and study done on Nepal and Nigeria [33, 34]. Stunting indicated a lack of adequate food over a long period of time, which was exacerbated by infections. Despite minor improvements in the 2019 EDHS report, the current prevalence of stunting is remains a public health issues in the study area. This disparity in prevalence difference could be explained by difference in the socioeconomic status, agricultural productivity, food insecurity at household level, and intra household resource allocation. The diversity in agricultural production and livestock ownership enhance individual dietary diversity outcomes in young children aged 6–23 months [35, 36]. Another reason for this could be a difference in cultural and child feeding habits, study setting, and study periods [37, 38].
The prevalence of wasting in this study was comparable to the regional and the national values [11] and other parts of the country such as, rural Ethiopia,South Ethiopia, North west Ethiopia,East Gojam zone and Northeast Thailand [8, 22, 27, 39, 40] but the result was lower than other studies like Pastoral communities of Afar, Meta-Analysis conducted in Ethiopia,Nepal, Nigeria and Maharashtra [9, 23, 33, 34, 41]. Wasting is an indicator of acute malnutrition which can occur as result recent infection or as result weight loss due to seasonal variation of food supply. This difference could be explained by difference in the sample- size, socioeconomic, socio –cultural, feeding habits, study area and period of the study population.
According to the current study, there is no significance difference in child nutritional status between households with and without home gardening practice [15, 42]. However, Studies conducted in Southern Ethiopia and Zimbabwe revealed a signifcant relationship between home gardening and child nutrition [27, 43]. This could be due to participants' consumption of monotonous type habit. Production alone does not guarantee for good nutritional status unless it is supplemented with dieversified poducion and consumption of these products [36].
In the current study, male children were more likely to be stunted than female children. Male children had a 3.1 times greater chance of becoming stunted than female children but female children had a 2.4 times greater chance of being wasted. This could be explained partially by the fact that boys are more vulnerable to health inequalities than their female counterparts in the same age groups and there may be biological differences that boys are more susceptible to infectious diseases and show higher biological fragility in the first year of life [44, 45]. It could also be explained by unmeasured factors such as parental gender preference or sex difference in feeding practice[9]. Many studies in Ethiopia, Afar regional state [9], Meta-analysis in Ethiopia [23], South Ethiopia [27] East Hararghe Zone and South Wollo Zone [46] and EDHS 20,119 report [11] revealed the same finding.
In the current study, children’s immunization status was found to have a significant association with increased risk of high prevalence of stunting and wasting from gardening households. Non-immunized children were 1.9 and 6.2 times more likely to become stunted and wasted than immunized children respectively. This could be explained by the fact that non immunized children are at risk of many vaccine preventable diseases such as diarrhea and respiratory infections, which lead to nutrients depletion in the body. This finding was consistent with other studies conducted in pastoral communities of Afar [9], EDHS 2016 report [47] and Nepal [33].
Prelactal feeding was found to be another factor associated with stunting in the current study. The risk of stunting was 1.9 times higher in children who received prelactal feeding at birth than in children who did not receive prelactal feeding at birth. This could be because it has a negative impact on breastfeeding, and when children are not breastfed properly, they are at higher risk of developing malnutrition [9].
In this study, dietary diversity was found to be associated with child stunting in both households with and without home gardening practice. Children with low DDS were more likely to be stunted than children with high DDS. This could be explained by saying that children who ate monotonous or limited variety of foods were at risk of micro nutrient deficiency which could lead to chronic malnutrition. This finding was supported with study done in Meta-Analysis conducted in Ethiopia [23],Study conducted at south Ethiopia [27], Study conducted on rural Myanmar [48] and South Africa [15].
The presence of diarrheal disease was found to be significantly associated with an increase prevalence of stunting in the current study. Children who had diarrheal disease in the past two weeks prior to the study were 3.2 times more likely to be stunted than those children without diarrheal disease. According to UNICEF, this could be because diarrhea causes a decrease in appetite, poor digestion, and malabsorption, all of which lead to malnutrition [49].This result was consistent with other findings conducted in south Ethiopia [27], Meta-Analysis conducted in Ethiopia [23], EDHS 2016 report [47] and South Africa [15].
In the current study, a child's feeding frequency was also significantly associated with an increase in the prevalence of stunting in non-gardening households. Children who had fewer than three feedings per day were 1.7 times more likely to be stunted than children who had more than three feedings per day. This could be because low feeding frequency leads to insufficient nutrient intake, which leads to malnutrition. This result was consistent with the findings of a study conducted in Northwest Ethiopia [50].
Drinking water source was found to be a significant association with increased risk of wasting in this study. Children in households with unprotected water source were 2.5 times more likely to be wasting than children in households with protected water source. This could be due to the fact that water from a contaminated source may serves as a source for different parasitic and gastrointestinal infection, which causes children to be malnourished (wasting) [49]. This finding was supported by research conducted in the East Go jam zone [8], the EDHS 2016 report [47] and rural Ethiopia [22].
Conclusions and recommendations
This study found that there was no statistically significance difference in nutritional status of under-five children from households with and without home gardening. The significant predictors of nutritional status (stunting and wasting) were sex of child dietary diversity score, immunization status, drinking water source and, feeding frequency, and presence of diarrhea.
Prevention and control of childhood illness such as diarrheal through improving environmental health conditions such as provision of safe and adequate water, prevention of contamination of food and water and health care services. Incite heath extension workers to address vaccine preventable disease integrated with the access of nutrition education programs to improve feeding frequency and dietary diversity of children are recommended activities to reduce malnutrition among under five children.
To researchers: Farther nutritional status studies for under –five children on different seasons and repeated recall days for identify dietary diversity of children, in addition to that studies on maternal awareness and attitude on proper use of home gardening products to child nutrition.
Limitations of the study
This study should be interpreted in the context of the following limitations. There may be a recall bias during data collection time that might be over and under estimate the finding and the Dietary intake was assessed using a single day recall which may not show permanent habit of the households. The study may not free from social desirability bias in responding to questions on house hold food security.
Availability of data and materials
All the required data has been included in the manuscript.
Abbreviations
- AOR:
-
Adjusted Odds Ratio
- CI:
-
Confidence Interval
- COR:
-
Crude Odds Ratio
- DDS:
-
Dietary Diversity Score
- EDHS:
-
Ethiopia Demographic Health Survey
- FANTA:
-
Food and Nutrition Technical Assistance
- FAO:
-
Food Agricultural Organization
- FNP:
-
Food and Nutrition Policy
- G.C:
-
Gregorian Calendar
- GDP:
-
Gross Domestic Product
- HEW:
-
Health Extension worker
- HHS:
-
Households
- HAZ:
-
Height for Age Z score
- NNP:
-
National Nutrition Program
- OR:
-
Odds Ratio
- SD:
-
Standard Deviation
- SDG:
-
Sustainable Development Goal
- SPSS:
-
Statistical Package for Social Sciences
- UNICEF:
-
United Nations International Children’s Emergency Fund
- WAZ:
-
Weight for Age Z score
- WHO:
-
World Health Organization
- WHZ:
-
Weight for Height Z score
References
Blossner M, De Onis M, Prüss-Üstün A. Malnutrition: quantifying the health impact at national and local levels. 2005.
Mengistu K, Alemu K, Destaw B. Prevalence of malnutrition and associated factors among children aged 6–59 months at Hidabu Abote District, North Shewa, Oromia Regional State. J nutr disorders ther. 2013;1:1–15.
Darsene H, Geleto A, Gebeyehu A, Meseret S. Magnitude and predictors of undernutrition among children aged six to fifty nine months in Ethiopia: a cross sectional study. Arch Public Health. 2017;75(1):29.
Young M, Wolfheim C, Marsh DR, Hammamy D. World Health Organization/United Nations Children’s fund joint statement on integrated community case management: an equity-focused strategy to improve access to essential treatment services for children. Am J Trop Med Hyg. 2012;87(5):6–10.
Fanzo J, Hawkes C, Udomkesmalee E, Afshin A, Allemandi L, Assery O, et al. 2018 Global nutrition report: shining a light to spur action on nutrition. 2018.
World Health Organization. Nutrition in universal health coverage. World Health Organization; 2019.
Mya KS, Kyaw AT, Tun T. Feeding practices and nutritional status of children age 6–23 months in Myanmar: a secondary analysis of the 2015–16 demographic and health survey. PloS One. 2019;14(1):e0209044.
Zeray A, Kibret GD, Leshargie CT. Prevalence and associated factors of undernutrition among under-five children from model and non-model households in east Gojjam zone, Northwest Ethiopia: a comparative cross-sectional study. BMC Nutrition. 2019;5(1):27.
Gebre A, Reddy PS, Mulugeta A, Sedik Y, Kahssay M. Prevalence of malnutrition and associated factors among under-five children in pastoral communities of Afar Regional State, Northeast Ethiopia: a community-based cross-sectional study. J Nutr Metab. 2019;2019:9187609.
Ethiopian Public Health Institute (EPHI)[Ethiopia] and ICF. Ethiopia mini demographic and health survey 2019: key indicators.
Institute EPH, ICF. Ethiopia mini demographic and health survey 2019: key indicators. EPHI and ICF Rockville, Maryland, USA; 2019.
Achadi E, Ahuja A, Bendech MA, Bhutta ZA, De-Regil LM, Fanzo J, et al. Global Nutrition Report: From promise to impact: Ending malnutrition by 2030: International Food Policy Research Institute; 2016.
Nutrition G. Global nutrition report 2018: The burden of malnutrition. Retrieved; 2019.
Johnson-Welch C, Alemu B, Msaki TP, Sengendo M, Kigutha H, Wolff A. Improving household food security: institutions, gender, and integrated approaches. 2000.
Selepe BM. The impact of home gardens on dietary diversity, nutrient intake and nutritional status of pre-school children in a home garden project in Eatonside, the Vaal triangle, Johannesburg, South Africa 2010.
Galhena DH. Home gardens for improved food security and enhanced livelihoods in northern Sri Lanka: Michigan State University. Crop and Soil Sciences; 2012.
Talukder A, Haselow NJ, Osei AK, Villate E, Reario D, Kroeun H, SokHoing L, Uddin A, Dhunge S, Quinn V. Homestead food production model contributes to improved household food security and nutrition status of young children and women in poor populations. Lessons learned from scaling-up programs in Asia (Bangladesh, Cambodia, Nepal and Philippines). Field Actions Science Reports. The journal of field actions. 2010;(Special Issue 1).
Odebode S. Assessment of home gardening as a potential source of household income in Adinyele local government are of Oyo state. Niger J Hortic Sci. 2006;11(1):47–55.
Ethiopia FDRo. National Nutrition Programme II: 2016–2020. 2016.
Ethiopia FDRo. seqota-declaration-implementation-plan-(20162030). March 2016.
Ethiopia FDRo. Food and Nutriiton Policy November 2018.
Endris N, Asefa H, Dube L. Prevalence of malnutrition and associated factors among children in rural Ethiopia. BioMed Res Int. 2017;2017:6587853.
Abdulahi A, Shab-Bidar S, Rezaei S, Djafarian K. Nutritional status of under five children in Ethiopia: a systematic review and meta-analysis. Ethiop J Health Sci. 2017;27(2):175–88.
Yalew B, Amsalu F, Bikes D. Prevalence and factors associated with stunting, underweight and wasting: A community based cross sectional study among children age 6–59 months at Lalibela Town, Northern Ethiopia. J Nutr Disorders Ther. 2014;4(147):2161-0509.1000147.
Zur Heide F. Feasibility study for a Lake Tana biosphere reserve. Ethiopia: Bundesamt für Naturschutz, BfN; 2012.
Bahir Dar city administration. Population projection, 2019. https://www.statsethiopia.gov.et/population-projection/.
Petros L, Mulugeta A, Kabeta A, Fekadu T. Comparison of nutritional status of pre-school children from households with home garden and without home garden in Wondogenet Woreda, South Ethiopia. Clinics Mother Child Health. 2018;15(292):2.
Cogill B. Anthropometric indicators measurement guide. 2003.
Organization WH. Indicators for assessing infant and young child feeding practices: part 1: definitions: conclusions of a consensus meeting held 6–8 November 2007 in Washington DC, USA. 2008.
Coates J, Swindale A, Bilinsky P. Household Food Insecurity Access Scale (HFIAS) for measurement of household food access: indicator guide (v. 3). Washington, DC: Food and Nutrition Technical Assistance Project, Academy for Educational Development; 2007. DC: Food and Nutrition Technical Assistance Project, Academy for Educational Development.
Abebe Z, Gebeye E, Tariku A. Poor dietary diversity, wealth status and use of un-iodized salt are associated with goiter among school children: a cross-sectional study in Ethiopia. BMC Public Health. 2017;17(1):1–1.
Niñez VK. Household gardens: theoretical considerations on an old survival strategy. Lima: International Potato Center; 1984.
Bhandari TR, Chhetri M. Nutritional status of under five year children and factors associated in Kapilvastu District. Nepal J Nutr Health Food Sci. 2013;1(1):1–6.
Olodu MD, Adeyemi AG, Olowookere SA, Esimai OA. Nutritional status of under-five children born to teenage mothers in an urban setting, south-western Nigeria. BMC Res Notes. 2019;12(1):116.
Kumar N, Harris J, Rawat R. If they grow it, will they eat and grow? Evidence from Zambia on agricultural diversity and child undernutrition. J Dev Stud. 2015;51(8):1060–77.
Slavchevska V. Agricultural production and the nutritional status of family members in Tanzania. J Dev Stud. 2015;51(8):1016–33.
Alkerwi Aa, Vernier C, Sauvageot N, Crichton GE, Elias MF. Demographic and socioeconomic disparity in nutrition: application of a novel correlated component regression approach. BMJ open. 2015;5(5):e006814.
Mengesha AD, Ayele TT. The impact of culture on the nutritional status of children and mothers durrinng recurring food insecurity: the case of boreicha woreda (SNNPRS). Am J Educ Res. 2015;3(7):849–67.
Schipani S, van der Haar F, Sinawat S, Maleevong K. Dietary intake and nutritional status of young children in families practicing mixed home gardening in northeast Thailand. Food Nutr Bull. 2002;23(2):175–80.
Bhattacharjee L, Phithayaphone S, Nandi BK. Home gardens key to improved nutritional well-being. RAP Publication (FAO). 2006.
Purohit L, Sahu P, Godale LB. Nutritional status of under-five children in a city of Maharashtra: a community based study. Int J Community Med Public Health. 2017;4(4):1171–8.
Mulugeta A, Hagos F, Kruseman G, Linderhof V, Stoecker B, Abraha Z, et al. Child malnutrition in Tigray, northern Ethiopia. East Afr Med J. 2010;87(6):248–54.
Mutambara J, Satambara T, Masvongo J. Impacts of nutritional gardens on health of communal households: a case study of Nyanga North District. Greener J Agricul Sci. 2013;3:579–84.
Kirsten BA, Diallo A. Boys are more stunted than girls from early infancy to 3 years of age in Rural Senegal. J Nutr. 2017;147(5):940–7. https://doi.org/10.3945/jn.116.243246.
Wamani H, Åstrøm AN, Peterson S, et al. Boys are more stunted than girls in Sub-Saharan Africa: a meta-analysis of 16 demographic and health surveys. BMC Pediatr. 2007;7:17. https://doi.org/10.1186/1471-2431-7-17.
Beyene S, Willis MS, Mamo M, Legesse B, Regassa T, Tadesse T, Wolde-Hawariat Y, Roslan NF. Nutritional status of children aged 0–60 months in two drought-prone areas of Ethiopia. South African Journal of Clinical Nutrition. 2020;33(4):152-7.
EDHS E. demographic and health survey 2016: key indicators report. The DHS Program ICF. 2016.
Rammohan A, Pritchard B, Dibley M. Home gardens as a predictor of enhanced dietary diversity and food security in rural Myanmar. BMC Public Health. 2019;19(1):1145.
UNICEF, Unicef. ’s approach to scaling up nutrition for mothers and their children. United Nations Children’s Fund. 2015.
Girma A, Woldie H, Mekonnen FA, Gonete KA, Sisay M. Undernutrition and associated factors among urban children aged 24–59 months in Northwest Ethiopia: a community based cross sectional study. BMC Pediatr. 2019;19(1):214.
Acknowledgements
We would like to offer our in-depth gratitude to the data collectors, participants for their support to
Funding
No funding received for this specific study.
Author information
Authors and Affiliations
Contributions
All authors were equally contributed in the production of this manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical clearance was obtained from ethical Review Board of Bahir Dar University College of Medicine and Health Sciences and zonal health department and selected kebele through formal letter. All methods were performed in accordance with the relevant guidelines and regulations of ethical Review Board. Before collecting the data, written consent was obtained from each study participants. Each study participants were informed about the purpose of the study and participation was voluntary without payment for their participation. Each study participants also were informed that the right to withdraw at any time during the interview. All gathered information were protected from its confidentiality, anonymity was explaining clearly to participant. Except the principal investigator information is not exposed third person.
Consent for publication
Not applicable.
Competing interest
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visithttp://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Bayih, M.T., Arega, Z. & Motbainor, A. Nutritional status of 6–59 months of age children is not significantly varied between households with and without home gardening practices in Zege, North West Ethiopia, 2020: community based comparative study. BMC Pediatr 22, 221 (2022). https://doi.org/10.1186/s12887-022-03283-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-022-03283-5