
Abstract
Background
Previous research has shown that female adolescents and adults report lower health status than their male peers. Possibly, this discrepancy already develops during childhood. We collected sex-specific data with the Pediatric Quality of Life Inventory (PedsQL) in a large school-based sample.
Methods
The online version of the PedsQL was administered to healthy Dutch children aged 5–7 years (parent proxy-report), 8–12 years (parent proxy-report and child self-report), and 13–17 years (parent proxy-report and child self-report), recruited through regular primary and secondary schools. Sex differences were assessed using t-tests or Mann–Whitney U-tests. Wilcoxon signed-rank tests and intraclass correlation coefficients served to compare parent proxy-reports with child self-reports. Multivariable linear regression analyses were used to assess the associations of sex of the child, age, and parental educational level with PedsQL scores.
Results
Eight hundred eighty-two parents and five hundred eighty one children were recruited from 15 different schools in the Netherlands. Parents of 8-to-12-year-olds reported higher scores on School Functioning for girls than for boys (mean difference [MD]: 6.56, p < 0.001). Parents of 13-to-17-year-olds reported lower scores on Physical and Emotional Functioning for girls than for boys (MDs: 2.14 and 5.79, p = 0.014 and p < 0.001, respectively). Girls aged 8–12 years reported lower scores than boys in this age group on Physical Functioning (MD: 3.09, p = 0.005). Girls aged 13–17 years reported lower scores than boys in this age group on Physical Functioning (MD: 3.67, p < 0.001), Emotional Functioning (MD: 8.11, p < 0.001), and the Total Score (MD 3.26, p = 0.004). No sex differences were found in children aged 5–7 years. Agreement between child self-reports and parent proxy-reports was poor to moderate.
Conclusions
Girls generally had lower PedsQL scores than boys, both in parent proxy-reports and in child self-reports. We recommend to apply sex-specific data when assessing health status using the PedsQL.
Similar content being viewed by others


Background
The quality of pediatric healthcare has improved and mortality rates have declined over the last decades [1, 2]. An increasing number of children are living with a chronic health condition and the focus of healthcare and research is shifting towards outcomes on the long-term [2,3,4]. Next to monitoring the health status of chronically ill children, the impact of events such as the COVID-19 pandemic on the physical and mental health of these children should be carefully monitored.
Input from parents and their children has become an essential part of modern pediatric healthcare and parent- or patient-reported outcome measures (PROMs) are increasingly being implemented [5]. The information collected from PROMs can help clinicians to monitor a child’s progress, to guide and adjust treatment, and to improve the quality of value-based healthcare [5, 6]. One of the most frequently used instruments to measure children’s health status (HS) is the Pediatric Quality of Life Inventory (PedsQL™)[7]. The PedsQL has been translated into multiple languages and data have been validated for over 35 translations worldwide [8].
Previous research has shown that adolescent and adult females report a lower HS than their male age peers [9, 10]; it is not inconceivable that this phenomenon goes back to childhood. Previous PedsQL validation studies reported a lower HS in girls in the United Kingdom [11] but no sex differences in the United States [7]. Establishing sex-specific normative values can help improve our understanding of sex differences and, consequently, enable the provision of sex-sensitive healthcare [12, 13].
In the Netherlands, the most recent data from a large sample for the online version of the PedsQL have been collected more than ten years ago [14]. Despite the finding that girls aged 8–12 years reported lower Emotional Functioning than boys [14], sex-specific data were not presented. Next to this, parent proxy-report data in children aged 8–17 years are still lacking in the Netherlands [14]. It is necessary to also obtain proxy data from a large sample as child self-reports regularly need to be substituted by parent proxy-reports for a variety of reasons. For instance, a child may be too young or too ill to complete the questionnaire. Next to this, inclusion of a proxy-report provides a broader view of the child’s health status.
For this study, we collected sex-specific data for both the parent proxy-report and the child self-report online version of the PedsQL. The primary aim of our study was to determine whether the discrepancy in health status among males and females already develops during childhood and adolescence. Secondarily, we assessed agreement between child self-reports and parent proxy-reports and evaluated sociodemographic influences on PedsQL scores.
Methods
Participants and procedure
The PedsQL was administered online to healthy Dutch children aged 5–17 years and their parents, between April 2015 and June 2017, using our institutional program for online surveys (LimeSurvey GmbH version 2.06lts, Hamburg, Germany). Participants were recruited through regular primary and secondary schools in different regions of the Netherlands. Children with a parent-reported chronic disease (e.g. asthma, cerebral palsy; according to the 10th revision of the International Statistical Classification of Diseases and Related Health Problems [15]) and/or a mental disorder (e.g. autism spectrum disorder, attention deficit/hyperactivity disorder, anxiety disorder; according to the 5th edition of the Diagnostic and Statistical Manual of Mental Disorders [16]) were excluded from analysis of both proxy-reported and self-reported data. Parents of participating schools had been sent a letter in which the purpose and procedure of the study were explained. All parents, as well as children aged 12 years and older, had been asked to provide informed consent for use of data for study purposes before filling out the online questionnaire. Parent and child responses were anonymously linked by means of personal tokens. The local Medical Ethics Review Board waived approval (‘Medical Research in Human Subjects Act does not apply to this research proposal’; Medical Ethics Committee Erasmus MC; MEC 2015–244).
Measures
PedsQL
The PedsQL assesses HS on four subscales: Physical (8 items), Emotional (5 items), Social (5 items), and School Functioning (5 items). Psychosocial Health is calculated as the mean score of Emotional, Social, and School Functioning. The Total Score is calculated as the mean score of all four subscales. Each item reflects a problem, for example 'problems with running', during the past month. Answers vary from never (= 0) to almost always (= 4) on a 5-point Likert scale. The scoring of each answer is reversed, and rescaled to a 0–100 scale (0 = 100, 4 = 0). Total Scores range from 0–100; higher scores reflect better health status [7]. We administered three age-appropriate versions of the PedsQL in this study: 5–7 years (parent proxy-report), 8–12 years (child self-report and parent proxy-report), and 13–17 years (child self-report and parent proxy-report). The layout of our web-based version of the PedsQL resembled the paper version as much as possible, except that questions were presented per subscale instead of all at once and missing values were not accepted.
Sociodemographic questionnaire
Parents were asked to fill out a sociodemographic questionnaire, consisting of three items on own sex, country of birth of both parents (i.e. the Netherlands or another country), and highest completed education: low, middle, or high based on the International Standard Classification of Education (ISCED) 2011 [17]), and four items concerning their child (sex, month and year of birth, presence of a chronic disease, and need for psychological help during the past year).
Statistical analysis
Continuous sociodemographic variables are presented as median (range) and categorical variables as number (%). Associations between sociodemographic characteristics (i.e. parental sex, level of education, and country of birth) and PedsQL scores were assessed using Mann–Whitney U-tests. To facilitate comparisons with reference data obtained in other populations, PedsQL scores are shown as mean ± standard deviation (SD). Differences in PedsQL scores between boys and girls were compared using t-tests or Mann–Whitney U tests, depending on the distribution of the data (i.e. normally or not normally distributed according to Shapiro–Wilk test). Wilcoxon signed-rank tests and intraclass correlation coefficients (ICCs; two-way mixed model, absolute agreement, single measures) served to compare parent proxy-reports with child self-reports. ICCs were interpreted as poor agreement (< 0.50), moderate agreement (0.50–0.75), good agreement (0.75–0.90), or excellent agreement (> 0.90) [18]. Effect sizes were calculated using Cohen’s d. Effect sizes were considered small (0.20), medium (0.50), or large (0.80) [19]. Additionally, we performed linear multivariable regression analyses to assess the relationship between sex of the child, age, and parental educational level (dichotomized into ISCED class Low or Middle/High – based on a one-way ANOVA test) selected as independent variables, and PedsQL scores (each subscale selected as dependent variable). We applied a Bonferroni correction to account for multiple comparisons; as we assessed sociodemographic influences and sex differences for two (child self-reports) or three (parent proxy-reports) different age categories: alpha was set at 0.05/2 = 0.025 or 0.05/3 = 0.017, respectively. Statistical analyses were performed using SPSS V.24.0.
Results
We recruited 882 parents and 581 children from 15 different schools in the Netherlands, who completed the PedsQL (Fig. 1). Sociodemographic characteristics of participants are shown in Table 1.

Inclusion flow chart. Regions: West (n = 8), South (n = 6), East (n = 1)
Sociodemographic influences
Parental sex
We found no effect of parental sex in any age group; PedsQL scores reported by fathers did not differ significantly from those reported by mothers.
Level of education
In multivariable linear regression analyses, parental level of education was found only to be predictive of proxy-rated School Functioning in 8–12 year-olds (unstandardized regression coefficient = 8.03, p = 0.006; Additional file 4A), which means that parents with a higher educational level rated the School Functioning of their child in this age group higher than parents with a lower educational level did.
Country of birth
In proxy ratings, School Functioning of children with two Dutch parents was rated higher than that of age peers with one Dutch parent and a parent born in a different country in the age categories of 5–7 years (mean difference: 11.53, effect size: 0.65, p = 0.012) and 13–17 years (mean difference: 4.94, effect size: 0.32, p = 0.016). Apart from this, no significant differences in any age category were found with regard to country of birth – neither for parent proxy-reports nor for child self-reports.
Age
In multivariable linear regression analyses, an additional effect of age was found in 8–12 year-olds for self-rated School Functioning (unstandardized regression coefficient = 1.38, p = 0.010; Additional file 4B), which means that older children report better School Functioning than younger children in this age group did.
Sex differences
Parents of 5-to-7-year-olds reported similar scores for boys and girls. In the group of 8-to-12-year-olds, parents reported higher scores on School Functioning for girls than for boys (mean difference: 6.56, p < 0.001). Parents of 13-to-17-year-olds reported lower scores on Physical Functioning and Emotional Functioning for girls than for boys (mean differences: 2.14 and 5.79; p = 0.014 and p < 0.001, respectively) (Table 2, Fig. 2, and Additional file 1). Effect sizes ranged from 0.01 to 0.46.

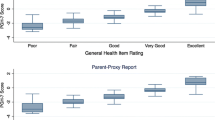
Bar chart showing sex differences per PedsQL subscale. Panel a: parent proxy-report; panel b: child self-report. PF = Physical Functioning; EF = Emotional Functioning; SF = Social Functioning; ScF = School Functioning. Asterisk indicates significance, on a Bonferroni-adjusted significance level of 0.017 (parent proxy-report) or 0.025 (child self-report)
Girls aged 8–12 years reported lower scores than boys on Physical Functioning (mean difference: 3.09, p = 0.005). Girls aged 13–17 years reported lower scores than boys on Physical Functioning (mean difference: 3.67, p < 0.001), Emotional Functioning (mean difference: 8.11, p < 0.001), and on the Total Score (mean difference 3.26, p = 0.004) (Table 3, Fig. 2, and Additional file 2). Effect sizes ranged from 0.00 to 0.50.
In multivariable regression analyses, sex of the child was found to be predictive of both proxy- and self-reported School Functioning in 8–12 year-olds (coefficient = -7.18 and -3.92, p < 0.001 and p = 0.022, respectively), indicating higher scores for boys on School Functioning in this age group. In the group of 13-to-17-year olds, sex of the child was significantly predictive of self-reported Physical Functioning (coefficient = 3.59, p < 0.001), proxy- and self-reported Emotional Functioning (coefficient = 5.75 and 8.13, respectively, both p < 0.001), self-reported Psychosocial Health (coefficient = 3.09, p = 0.011), and of the self-reported Total Score (coefficient = 3.27, p = 0.001; Additional file 4A and B). This means that in 13–17-year olds, scores of girls and parents of girls were lower than scores of boys and parents of boys on these scales.
Differences between child self-report and parent proxy-report
In the age category of 8–12 years, parent proxy-reports were comparable to child self-reports (Table 4). Children aged 13–17 years reported higher scores than their parents on Physical Functioning (mean difference: 4.03, p < 0.001), and on the Total Score (mean difference: 1.57, p = 0.017). Effect sizes ranged from 0.00 to 0.34. Agreement between child self-reports and parent proxy-reports was poor to moderate; ICCs ranged from 0.34 (Physical Functioning in 13-to-17-year-olds) to 0.58 (Emotional Functioning in 8-to-12-year-olds). A visual representation of agreement on PedsQL Total Scores between parents and children is given in Additional file 3.
Discussion
We collected online data for the PedsQL in a school-based sample of 882 parents and 581 healthy children. Statistically significant sex differences were found from the age of 8 years onwards; girls generally had lower scores than boys, except for parent-reported School Functioning at age 8–12 years, which was higher in girls. Sex differences remained present after correcting for age and parental educational level, suggesting that boys and girls have different HS patterns that need to be assessed separately. Parents of children aged 13–17 years rated their child’s Physical Functioning lower than did the children themselves.
Sex differences in HS have been well reported among adults. Women reporting lower scores than men has been demonstrated not only for the PedsQL [9, 10], but also for other HS instruments across the world [20,21,22]. Our finding that sex differences in HS already emerge during childhood is supported by previous studies in clinical groups [14, 23,24,25,26,27,28]. Although these studies unanimously concluded that girls report lower scores than boys, their results varied with regard to the specific subscales. Some studies reported sex differences in Emotional Functioning only [14, 25], whereas others showed differences on a larger variety of subscales and on the Total Score [23, 24, 26,27,28].
The agreement between child self-reported and parent proxy-reported HS differs between studies. While some studies found that parents reported their child’s HS higher than did the child itself [29], other studies reported opposite findings [30, 31], or found differences in both directions – depending on the subscale [25, 32]. To make things even more complicated, previous research in children with chronic conditions has shown that sex – either that of the parent or the child – may affect parent–child agreement. Ooi et al., for instance, reported that parent–child agreement in children with obesity was higher with mothers than with fathers as proxies [31]. Blake et al. studied adolescents with sickle cell disease and found that parents of girls reported a higher HS than did the girls themselves, whereas parents of boys reported a lower HS than did the boys themselves [32]. One should keep in mind that a study’s conclusion might also depend on the way the data are assessed and interpreted: although we barely found any statistically significant differences between parent proxy-reports and child self-reports, ICCs showed poor to moderate agreement between parents and their children. Cross-informant discrepancies are a common finding; not only for the PedsQL, but also for other instruments such as the Child Behavior Checklist and the Youth Self Report [33]. These differences may indicate that both informants make unique contributions to a view of children’s HS.
Discrepancies between studies on HS with regard to sex differences or parent–child agreement can have various causes. HS may be affected by country of residence [27, 28], differences over time [34], socioeconomic status [28], physical and mental conditions [14, 35], a child’s age [28], and presumably many other factors. These factors need to be taken into account as much as possible when interpreting a study’s results. For this reason, up-to-date, country-specific data are essential to make valid inferences about a child’s HS. We chose not to present any cut-off points, but rather would recommend longitudinal follow-up of children’s PedsQL scores, which would alert to possible differences between time points and/or between child self-report and parent proxy-reports.
One of the strengths of our study is its large sample size, allowing us to present valid sex-specific data for both parent proxy-reported and child self-reported HS. Second, we included most regions of our country to improve the study’s representativeness of the general Dutch population. Several limitations need to be taken into account. First, as we did not collect data of non-participants, we compared our sociodemographic data to those of the general Dutch population. The proportion of participants with a Dutch background in our study was slightly higher than that of the total population in 2015 (85% versus 78% [36]). This finding is in line with the previous Dutch normative study [14], and may be explained by the fact that parents with insufficient understanding of the Dutch language could not participate. Furthermore, a relatively high proportion of participants had a high educational level (68% versus 43% in the general Dutch population aged 25–45 years [37]). This finding is not uncommon in similar studies [14, 38], but needs to be taken into account when interpreting these data. Second, we did not evaluate child self-reports in 5–7 year-olds. Based on our own experience within the infrastructure of a longitudinal follow-up program for children with congenital anatomical anomalies we decided to refrain from using the self-reports for 5–7 years. Our decision is justified by the recent publication of Conijn and coworkers [39]. Third, fathers were underrepresented, as more than 80% of proxy-reports were filled out by mothers. This is a common finding as well [7, 14]. Nevertheless, as we found no effect of parental sex in any age group, we presume that this underrepresentation has had little effect on our results.
Conclusions
Our study is the first to report sex-specific PedsQL data for a large school-based sample of the Dutch population. Girls generally had lower PedsQL scores than boys, both in parent proxy-reports and in child self-reports. We recommend to apply sex-specific data when assessing a child’s HS using the PedsQL. Taking into account sex, a fairer distinction can be made between normal and impaired HS. Sex-specific data would be more appropriate to study differences between boys and girls when it comes to the consequences of a disease on HS.
Agreement between parent proxy-reports and child self-reports was poor to moderate; children reported slightly higher scores than their parents, except for School Functioning. We therefore recommend to use both parent and child perspectives to get a complete picture and to address potential differences.
Availability of data and materials
Anonymized data are available upon reasonable request by contacting the corresponding author.
Abbreviations
- HS:
-
Health status
- ICCs:
-
Intraclass correlation coefficients
- ISCED:
-
International Standard Classification of Education
- PedsQL:
-
Pediatric Quality of Life Inventory
- PROMs:
-
Patient-reported outcome measures
- SD:
-
Standard deviation
References
Zeitlin J, Mohangoo AD, Delnord M, Cuttini M. Committee E-PS: The second European Perinatal Health Report: documenting changes over 6 years in the health of mothers and babies in Europe. J Epidemiol Community Health. 2013;67(12):983–5.
Murray CJ, Atkinson C, Bhalla K, Birbeck G, Burstein R, Chou D, Dellavalle R, Danaei G, Ezzati M, Fahimi A, et al. The state of US health, 1990–2010: burden of diseases, injuries, and risk factors. JAMA. 2013;310(6):591–608.
Wise PH. The future pediatrician: the challenge of chronic illness. J Pediatr. 2007;151(5 Suppl):S6-10.
Perrin JM, Bloom SR, Gortmaker SL. The increase of childhood chronic conditions in the United States. JAMA. 2007;297(24):2755–9.
Black N. Patient reported outcome measures could help transform healthcare. The BMJ. 2013;346:f167.
Kampstra NA, Zipfel N, van der Nat PB, Westert GP, van der Wees PJ, Groenewoud AS. Health outcomes measurement and organizational readiness support quality improvement: a systematic review. BMC Health Serv Res. 2018;18(1):1005.
Varni JW, Seid M, Kurtin PS. PedsQL 4.0: reliability and validity of the Pediatric Quality of Life Inventory version 4.0 generic core scales in healthy and patient populations. Med Care. 2001;39(8):800–12.
PedsQL Translations [https://www.pedsql.org/translations.html]
Limperg PF, Haverman L, van Oers HA, van Rossum MA, Maurice-Stam H, Grootenhuis MA. Health related quality of life in Dutch young adults: psychometric properties of the PedsQL generic core scales young adult version. Health Qual Life Outcomes. 2014;12:9.
Varni JW, Limbers CA. The PedsQL 4.0 Generic Core Scales Young Adult Version: feasibility, reliability and validity in a university student population. J Health Psychol. 2009;14(4):611–22.
Upton P, Eiser C, Cheung I, Hutchings HA, Jenney M, Maddocks A, Russell IT, Williams JG. Measurement properties of the UK-English version of the Pediatric Quality of Life Inventory 4.0 (PedsQL) generic core scales. Health Qual Life Outcomes. 2005;3:22.
Oertelt-Prigione S. Putting gender into sex- and gender-sensitive medicine. EClinicalMedicine. 2020;20:100305.
Celik H, Lagro-Janssen TA, Widdershoven GG, Abma TA. Bringing gender sensitivity into healthcare practice: a systematic review. Patient Educ Couns. 2011;84(2):143–9.
Engelen V, Haentjens MM, Detmar SB, Koopman HM, Grootenhuis MA. Health related quality of life of Dutch children: psychometric properties of the PedsQL in the Netherlands. BMC Pediatr. 2009;9:68.
World Health Organization. International Statistical Classification of Diseases and Related Health Problems. 10th ed. Geneva: WHO; 1992.
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. 2013.
International Standard Classification of Education ISCED 2011. Montreal, Canada: UNESCO Institute for Statistics; 2012.
Koo TK, Li MY. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J Chiropr Med. 2016;15(2):155–63.
Cohen J. Statistical power analysis for the behavioral sciences. New York: Academic Press; 1988.
Nolte S, Liegl G, Petersen MA, Aaronson NK, Costantini A, Fayers PM, Groenvold M, Holzner B, Johnson CD, Kemmler G, et al. General population normative data for the EORTC QLQ-C30 health-related quality of life questionnaire based on 15,386 persons across 13 European countries, Canada and the Unites States. Eur J Cancer. 2019;107:153–63.
McCaffrey N, Kaambwa B, Currow DC, Ratcliffe J. Health-related quality of life measured using the EQ-5D-5L: South Australian population norms. Health Qual Life Outcomes. 2016;14(1):133.
Zhang J, Xu L, Li J, Sun L, Qin W, Ding G, Wang Q, Zhu J, Yu Z, Xie S, et al. Gender differences in the association between body mass index and health-related quality of life among adults:a cross-sectional study in Shandong, China. BMC Public Health. 2019;19(1):1021.
Lukács A, Sasvári P, Török A, Barkai L. Generic and disease-specific quality of life in adolescents with type 1 diabetes: comparison to age-matched healthy peers. J Pediatr Endocrinol Metab. 2016;29(7):769–75.
Limperg PF, Joosten MMH, Fijnvandraat K, Peters M, Grootenhuis MA, Haverman L. Male gender, school attendance and sports participation are positively associated with health-related quality of life in children and adolescents with congenital bleeding disorders. Haemophilia. 2018;24(3):395–404.
Reinfjell T, Diseth TH, Veenstra M, Vikan A. Measuring health-related quality of life in young adolescents: reliability and validity in the Norwegian version of the Pediatric Quality of Life Inventory 4.0 (PedsQL) generic core scales. Health Qual Life Outcomes. 2006;4:61.
Dalton AG, Smith C, Dalton WT III, Slawson DL. Examining General Versus Condition-Specific Health-Related Quality of Life Across Weight Categories in an Adolescent Sample. J Pediatr Health Care. 2015;29(5):453–62.
Michel G, Bisegger C, Fuhr DC, Abel T. group K: Age and gender differences in health-related quality of life of children and adolescents in Europe: a multilevel analysis. Qual Life Res. 2009;18(9):1147–57.
Ow N, Mayo NE. Health-related quality of life scores of typically developing children and adolescents around the world: a meta-analysis with meta-regression. Qual Life Res. 2020;29(9):2311–32.
Cremeens J, Eiser C, Blades M. Factors influencing agreement between child self-report and parent proxy-reports on the Pediatric Quality of Life Inventory 4.0 (PedsQL) generic core scales. Health Qual Life Outcomes. 2006;4:58.
Lee YC, Yang HJ, Lee WT, Teng MJ. Do parents and children agree on rating a child’s HRQOL? A systematic review and Meta-analysis of comparisons between children with attention deficit hyperactivity disorder and children with typical development using the PedsQL(TM). Disabil Rehabil. 2019;41(3):265–75.
Ooi DSQ, Loke KY, Ho CWL, Lim YY, Tay V, Karuppiah V, Sng AA, Lai LY, Lee YS, Griva K. Self and parent-proxy rated health-related quality of life (HRQoL) in youth with obesity: are parents good surrogates? Qual Life Res. 2020;29(8):2171–81.
Blake A, Guthrie-Dixon N, Grindley M, Barton-Gooden A, Knight-Madden J, Asnani M. Level of agreement between adolescents’ self-assessment and parent proxy report of health-related quality of life in adolescents with sickle cell disease. Pediatr Blood Cancer. 2020;67(4):e28198.
Parent-Youth and Parent-Teacher Agreement on Children’s Mental Health Problems in Many Societies [https://aseba.org/research/parent-youth-and-parent-teacher-agreement-on-childrens-mental-health-problems-in-many-societies/]
Zahran HS, Kobau R, Moriarty DG, Zack MM, Holt J, Donehoo R. Centers for Disease C, Prevention: Health-related quality of life surveillance–United States, 1993–2002. Morb Mortal Wkly Rep Recomm Rep. 2005;54(4):1–35.
Varni JW, Limbers CA, Burwinkle TM. Impaired health-related quality of life in children and adolescents with chronic conditions: a comparative analysis of 10 disease clusters and 33 disease categories/severities utilizing the PedsQL 4.0 Generic Core Scales. Health Qual Life Outcomes. 2007;5:43.
Population; sex, age, migration background and generation, 1 January [https://www.cbs.nl/en-gb/figures/detail/37325eng]
Bevolking; hoogstbehaald onderwijsniveau en onderwijsrichting [https://opendata.cbs.nl/statline/#/CBS/nl/dataset/82816ned/table?dl=8083&ts=1592387332066]
Cella D, Hahn EA, Jensen SE, Butt Z, Nowinski CJ, Rothrock N, Lohr KN. Patient-Reported Outcomes in Performance Measurement. North Carolina United States: Research Triangle Institute; 2015.
Conijn JM, Smits N, Hartman EE. Determining at What Age Children Provide Sound Self-Reports: An Illustration of the Validity-Index Approach. Assessment. 2020;27(7):1604–18.
Acknowledgements
Ko Hagoort provided editorial advice. Mapi Research Trust provided permission to use the PedsQL™ (not-funded academic research project, February 26, 2015). We gratefully thank the schools that recruited participants and the parents and children who took part in our study.
Funding
No funding was received for this study.
Author information
Authors and Affiliations
Contributions
AH: Made substantial contributions to acquisition, analysis and interpretation of data. Drafted the manuscript and revised it critically for important intellectual content. Gave final approval of the version to be published. CtK: Made substantial contributions to analysis and interpretation of the data. Revised the manuscript critically for important intellectual content. Gave final approval of the version to be published. MM: Made substantial contributions to study conception and design, and acquisition of the data. Revised the manuscript critically for important intellectual content. Gave final approval of the version to be published. HIJ: Made substantial contributions to study conception and design, and interpretation of the data. Revised the manuscript critically for important intellectual content. Gave final approval of the version to be published. JR: Made substantial contributions to study conception and design, and acquisition of the data. Gave final approval of the version to be published. HK: Made substantial contributions to study conception and design, and interpretation of the data. Revised the manuscript critically for important intellectual content. Gave final approval of the version to be published. JvR: Made substantial contributions to analysis and interpretation of the data. Revised the manuscript critically for important intellectual content. Gave final approval of the version to be published. AR: Made substantial contributions to study conception and design, and analysis and interpretation of the data. Revised the manuscript critically for important intellectual content. Gave final approval of the version to be published.
Corresponding author
Ethics declarations
Ethics approval
All methods were carried out in accordance with relevant guidelines and regulations/Declaration of Helsinki.
The local Medical Ethics Review Board waived approval (‘Medical Research in Human Subjects Act does not apply to this research proposal’; Medical Ethics Committee Erasmus MC; MEC 2015–244).Consent to participate: All parents, as well as children aged 12 years and older gave informed consent for use of data for study purposes before completing the online questionnaire.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Parent proxy-reports: Normative data, including medians and interquartile ranges.
Additional file 2.
Child self-reports: Normative data, including medians and interquartile ranges.
Additional file 3.
Scatter plot showing agreement on PedsQL Total Scores between parent proxy-report and child self-report.
Additional file 4: Table S1.
Multivariable linear regression analyses showing significant predictors of the PedsQL scales; parent proxy-reports per age category Table S2. Multivariable linear regression analyses showing significant predictors of the PedsQL scales; child self-reports per age category.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hijkoop, A., ten Kate, C.A., Madderom, M.J. et al. Sex differences in children's health status as measured by the Pediatric Quality of Life Inventory (PedsQL)™: cross-sectional findings from a large school-based sample in the Netherlands. BMC Pediatr 21, 580 (2021). https://doi.org/10.1186/s12887-021-03059-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-021-03059-3