
Abstract
Background
Assessment of spleen size is an important part of the clinical skills of medical students and physicians. Many diseases can affect the size of the aforementioned organ, ranging from infective processes to malignant disorders. However, to detect changes, prior knowledge of the actual normal size of these viscera is required in the population being studied. Establishing a customized chart and curve for a specific population of the same sociodemographic characteristics enables a better interpretation of sonographic assessments.
Methods
A hospital-based cross-sectional study design was conducted among 403 children in primary and referral hospitals of the east and west Gojjam zone. Data were collected using a structured questionnaire, physical examination, and ultrasound. The collected data were entered into Epi Data version 3.1 and exports to SPSS version 24 for analysis. Descriptive data were analyzed using descriptive statistics. A Pearson product-moment correlation was run to determine the relationship between age, anthropometric measurements of children, and ultrasound measurements of the spleen. Reference intervals were established using non-parametric reference limits (2.5th -97.5th ) and (5th – 97th ) percentiles by MedCalc software version 20.0.3.
Results
Four hundred three children aged from 7 to 15 years were included in this study. The mean sonographic longitudinal (length), anteroposterior(depth) and transverse (width) dimension of the spleen was, (8.24 ± 1.26 cm), (3.98 ± 0.57 cm), and (4.26 ± 0.59 cm) respectively. The mean volume of the spleen was 75.04 ± 23.92 cm3. The height and body surface area of children were best correlated with sonographic dimensions of the spleen. Reference intervals were established using height, age, and body surface area specific for clinically practical dimensions of the spleen.
Conclusions
According to this study, the children are considered as having enlarged longitudinal dimension of the spleen(splenomegaly) if he or she has a size above 97.5th percentile based on their respective height.
Similar content being viewed by others


Background
Assessment of spleen size is an important part of the clinical skills of medical students and physicians, and determination of spleen span is essential. Many diseases can affect the spleen size, ranging from infective processes to malignant disorders. However, to detect changes, prior knowledge of the actual normal size of these viscera is required in the population being studied [1]. We can evaluate the size of these visceral organs by clinical and medical imaging techniques.
The clinical assessment of spleen size remains an important part of a physical examination, and knowledge of its normal values at different ages is essential in children and adolescents. This procedure is usually the first step in detecting the abnormal size of the spleen [2]. The spleen is palpable only when it is two to three times its normal size, although it may be palpable in 10 % of healthy children and 15 % of neonates [3]. However, the clinical examination has been established to be often inaccurate in detecting especially small increases in size [4].
Medical imaging techniques permit the observation of anatomical structures in living people and the study of their movements in normal and abnormal activities. Being able to identify normal structures on radiographs makes it easier to recognize the changes caused by disease and injury [5].
However, routine computed tomography and magnetic resonance imaging for the diagnosis and serial follow-up of patients for suspected enlargement of the spleen is difficult to justify because of the radiation exposure, the cost, and limited availability in many areas of the world, particularly in developing countries. So, ultrasonography is an established, safe, fast, and reliable method for the measurement of spleen sizes [6, 7]. In adults, ultrasound indicators of moderate splenomegaly include an anteroposterior diameter greater than two-thirds of the distance between the anterior and posterior abdominal wall, with a craniocaudal length exceeding the upper limit of 11–14 cm [8]. An interpolar diameter greater than 20 cm was considered massive splenomegaly [9].
Unfortunately, there is still no consensus on how to define splenomegaly in pediatric patients. The evaluation is challenging because the normal size varies because of nutritional factors, body habitus, geographical location, physical activities, genetic differences, race, and ethnicity [10,11,12,13].
The normal limit of the size of visceral organs according to age, body parameters have not been specified in northwest Ethiopia for school-age children. Hence, our currently used nomograms in primary and referral hospitals are based on the western database, which might lead to under or overestimation of the size of the spleen.
This study aimed to assess and document the splenic sizes in apparently healthy school-age children in an Ethiopian population in the Amhara region and thereby serve as a baseline for comparison in cases of splenomegaly using transabdominal sonography. In addition to this, we evaluated the relationship between splenic measurements, chronological and auxological data, and body proportions.
Methods
Study design, setting, and period
The institutional-based cross-sectional study design was conducted among 403 school-age children, from December 2019-June 2020 in Debre Markos referral hospital, Finote Selam general hospital and Bichena primary hospitals of east and west Gojjam zone, northwest Amhara.
Study participants
All apparently healthy children of 7 to 15 years that came to the hospitals’ pediatrics departments during study periods for a follow-up examination for mildly treated conditions; or who were examined because of problems unrelated to the spleen or a routine check-up were included in the study. However, in children who did not have normal height and weight curves, a history and physical examination finding of oncologic and hematologic disorders or infectious causes of splenic enlargement or splenic trauma, and the accidental discovery of one or more accessory spleens were excluded.
Sample size and sampling procedures
We calculated the sample size using online sample size calculators for designing clinical research developed by the University of California San Francisco (UCSF) clinical research program; assuming a power of 80 %, correlation coefficient of 0.145 of age, and splenic length among female subjects [14], the significance level of 95 %, and none response rate of 10 %. The computed sample size was 403.
The standard normal deviate for \(\mathrm\alpha\;=\;{\mathrm Z}_{\mathrm\alpha}\;=\;1.96\)
The standard normal deviate for \(\mathrm\beta\;=\;{\mathrm Z}_{\mathrm\beta}\;=\;0.842\)
By considering none response rate of 10 % in 37 samples, the total sample size of the study is 403. Assuming the heterogeneity nature of the population, we conducted a purposive sampling technique.
Data collection procedure and quality control
Sociodemographic characteristics of the study participants were collected using a structured interviewer-administered questionnaire. Anthropometric measurements of the participants, including height (cm), weight (kg), waist circumference (cm), body mass index (BMI), xipho-pubic distance (cm), and abdominal volume, were rigorously evaluated. Height was measured by stadiometer and weight with a standard beam balance scale (digital). Waist circumference was got at the midpoint between the lowest rib and the iliac crest using a tape meter. Xiphopubic distance was measured from the inferior border surface landmark of the xiphoid bone to the superior border of the symphysis pubis. We calculated BMI as body weight (kilograms) divided by body height (meters) squared. Body surface area (BSA) was calculated according to the Mosteller formula: BSA (m2) = square root of ([Height (cm) x Weight (kg)]/ 3600) [15]. The abdominal volume was computed according to the standard formula: (waist Circumference/6.28)2 *xipho-pubic distance*3.14 [16]. All anthropometric measurements were taken by three trained medical interns who were in pediatrics attachment.
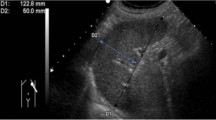
Sonographic evaluation: All children were asked to lie down in a supine position or a lateral position to get optimal images. We measured: longitudinal dimension: between the highest superior-medial and the lower inferior-lateral points of the spleen; anteroposterior dimension: between the anterior and posterior surfaces; transverse dimension: between the hilum and the superior-lateral edge of the spleen. Scanning was conducted three times, and the average dimension was taken. The volume of the spleen was calculated using the prolated ellipsoid formula (Length *Width*Thickness* 0.523) [17].
To maintain the quality of the research, the data collectors were trained. There was close monitoring and supervision during the data collection period.
Variables of the study
The dependent variables were sonographic dimensions (longitudinal, anteroposterior, and transverse dimensions and the volume) of the spleen. Whereas socio-demographic; height, weight, waist circumference, body mass index (BMI), body surface area, abdominal volume, and xipho-pubic distances of children were independent variables.
Definition of variables
Apparently healthy children: refers to the absence of disease of the spleen based on clinical signs and symptoms, normally assessed by history, physical evaluation, and routine laboratory methods available in the hospitals (like for malaria, typhus, and typhoid).
Data processing and analysis
We used EPI-Data Version 3.1 for data entry and SPSS Version 24 and mainly MedCalc version 20.0.3 for analysis. Descriptive statistics for continuous variables were described using the measure of central tendency (mean) dispersion (standard deviation). A one-way ANOVA was conducted to compare the means of anthropometric measurements among children of each age group. A Pearson product-moment correlation was run to determine the relationship between age, weight, height, waist circumference, xiphopubic distance, body surface area, abdominal volume, and sonographic measurements of the spleen. Pediatric non-parametric reference limits (2.5th —97.5th and 3rd – 97th percentiles) for spleen measures are reported. Model-based specific reference intervals were computed with age, height, and body surface area modeled as fractional polynomials. Transformation of variables was conducted before model fitting and then plotted against height body surface area and age.
Results
Anthropometric assessments of children
A total of four hundred three apparently healthy children were enrolled in this study. A one-way ANOVA was conducted to compare the means of anthropometric measurements among children of each age group. There was a statistically significant difference between groups ANOVA (F (8,394) = 191.66, p < 0.001) for height; F (8,394) = 73.06, p < 0.001) for weight; F (8,394) = 24.97, p < 0.001) for waist circumference; F (8,394) = 101.95, p < 0.001) for xiphopubic distance; F (8,394) = 103.61, p < 0.001) for body surface area, and F (8,394) = 44.53, p < 0.001) for abdominal volume (Table 1).
Sonographic evaluation of spleen and anthropometric measurements (body parameters)
The mean sonographic longitudinal (length), anteroposterior(depth) and transverse (width) dimension of the spleen was, (8.24 ± 1.26 cm), (3.98 ± 0.57 cm), and (4.26 ± 0.59 cm) respectively. The mean volume of the spleen was 75.04 ± 23.92cm3. The longitudinal dimension of the spleen was moderately correlated with height (r =. 384, n = 403, p < 0.001). The anteroposterior dimension (thickness) of the spleen was best correlated with the weight (r = 0.475, n = 403, p < 0.001) and body surface area (r = 0.493, n = 403, p < 0.001) of the children. Similarly, the volume of spleen showed moderate correlation with the weight (r = 0.464, n = 403, p < 0.001) and body surface area (r = 0.479, n = 403, p < 0.001) of the children but best predicted by their age. However transverse diameter of the spleen showed a weak correlation with body parameters (Table 2).
Reference intervals for dimensions of spleen and body parameters
Model-based body parameter-specific reference intervals were computed, using MedCalc version 20.0.3. We established smoothened height for the longitudinal dimension of the spleen (Table 3; Fig. 1); body surface area for the anteroposterior dimension (Table 4; Fig. 2), and age for the volume of the spleen (Table 5; Fig. 3) using non-parametric reference limits (2.5th -97.5th ) and 5th – 97th percentiles).

Percentile curves of the model-based reference limits (2.5th -97th and 5th -95th ) for the longitudinal dimension of the spleen

Percentile curves of the model-based reference limits (2.5th -97th and 5th -95th ) for the anteroposterior dimension of the spleen

Percentile curves of the model-based reference limits (2.5th -97th and 5th -95th ) for the volume of the spleen
When to say splenomegaly?
According to our study, the children are considered as having enlarged longitudinal dimension of the spleen (splenomegaly) if he or she has a size above 97.5th percentile based on the respective height.
Discussion
In the literature, there are few detailed studies to interpret the spleen dimensions in school-aged children in Africa and Ethiopia. Sonographic determination of pathologic changes in the size of the spleen necessitates knowing the normal ranges of its measurements especially concerning anthropometric assessments in school-age children. The morphology of the spleen varies from person to person. During the maturation process from infancy through adolescence, the growth of the spleen shows a high correlation with gains in height, weight, and body surface area [6, 18].
To the best of our knowledge, our study, which aimed to investigate the normal limits of the spleen of school-aged children, comprises one of the largest series in the literature from Ethiopia, including the age group of 7 to 15 years.
There is no agreement on which anthropometric measurements are generally acceptable for exploring the normal limit of organ measurements [6, 19,20,21] as these parameters might varies due to nutritional factors, body habitus, geographical location, physical activities, genetic differences, race, and ethnicity. Previous studies showed that the longitudinal dimensions of the spleen, were best correlated with body parameters [6, 21,22,23,24,25,26,27,28,29,30]. This is in accordance with the results of our study. The height, weight, and body surface area of the children were best correlated with the dimensions of the spleen.
Assessment of longitudinal dimensions (length) of the spleen is more practical either by palpation and percussion or using ultrasound. The estimation of spleen width and volume is less solid and questionable in diagnosing splenomegaly [31]. In this study, the height of children was best correlated with the longitudinal dimensions of the spleen hence reference intervals and curves were established using the height of the children. The transverse dimension of the spleen showed a weak correlation with the body parameters. This is supported by similar studies in different countries [6, 32]. However, others reported that weight was best correlated with longitudinal dimensions of the spleen [24, 33]. These differences might be because of variations in the race or different ethnic origins, nutritional factors, body habitus, and geographical location.
In most studies, sizes between the 5th and 95th percentiles were the accepted normal limits [33, 34]. This practice results in approximately 10 % of children with normal visceral organs falling outside these limits [21]. We preferred to define the lowermost and uppermost dimensions of the spleen to best correlated anthropometric measurements using the 2.5th and 97.5th percentile values in addition to the 5th and 95th percentile values respectively as a guide.
Conclusions
The normal limits of the spleen are important parameters during a sonographic examination. Reference intervals were established based on the best-correlated and predictor anthropometric measurements. Children with the longitudinal dimension of spleen above 97.5th percentile values with their specific height are considered as having splenomegaly. We hope this study contributes to daily practice in radiology clinics to interpret the normal sizes of the spleen of school-aged children in northwest Ethiopia.
Limitations
Calibration of measuring tools in the hospitals were not conducted frequently.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Khan, S.A., et al., Sonographic evaluation of normal liver, spleen, and renal parameters in the adult population: a multicenter study. 2018;28(11):834.
El-Shafie, A.M, et al, Correlation between clinical examination and ultrasound of liver and spleen span in normal children between 12 and 18 years of age. 2015;28(2):382.
RE B. Nelson Textbook of Pediatrics. 17th ed. Philadelphia: Elsevier Saunders; 2004.
Zhang, B., S.J.C. Lewis, and L. Haematology, a study of the reliability of clinical palpation of the spleen. 1989;11(1):7–10.
Keith, L.M., Clinically oriented anatomy 7th edition. 2014, Wolters Kluwer,Philadelphia, PA 19103
Konuş, O, et al, Normal liver, spleen, and kidney dimensions in neonates, infants, and children: evaluation with sonography. 1998;171(6):1693–1698.
Ehimwenma, O. and M.T.J.N.m.j.j.o.t. N.M.A. Tagbo, Determination of normal dimension of the spleen by ultrasound in an endemic tropical environment. 2011;52(3):198.
Robertson, F., P. Leander, and O.J.E.r. Ekberg, Radiology of the spleen. 2001;11(1):80–95.
Goerg, C., et al., Sonographic patterns of the affected spleen in malignant lymphoma. 1990;18(7):569–574.
Kliegman, R. and J.J.E. St Geme, Nelson textbook of pediatrics 21st edition. 2019.
Emamian, S.A., et al., Kidney dimensions at sonography: correlation with age, sex, and habitus in 665 adult volunteers. 1993;160(1):83–86.
Odita, J., C.J.T. Ugbodaga, and G. Medicine, roentgenologic estimation of kidney size in adult Nigerians. 1982;34(2):177–181.
Gul, S., M.S. Itoo, and G.J.I.J.o.R.i.M.S. Nisa, Normative data of liver size in Kashmiri adult population using ultra-sonography, India. 2019;7(6):2408.
Tekle, Y., et al., Determination of normal dimension of the spleen by ultrasound and its correlation with age. 2018;7(4):8.
Mosteller, R.J.T.N.E.j.o.m., Simplified calculation of body-surface area. 1987;317(17):1098–1098.
Pelizzo, G., et al., Spleen size evaluation in children: Time to define splenomegaly for pediatric surgeons and pediatricians. 2018;13(8):e0202741.
Sauerbrei, E.E., K.T. Nguyen, and R.L. Nolan, A practical guide to ultrasound in obstetrics and gynecology. 1986;18(14):224.
Megremis SD, Vlachonikolis IG, Tsilimigaki AM. Spleen length in childhood with US: normal values based on age, sex, and somatometric parameters. Radiology. 2004;231(1):129–34.
De Sanctis, J.T., S.A. Connolly, and R.T.J.A.A.j.o.r. Bramson, Effect of patient position on sonographically measured renal length in neonates, infants, and children. 1998;170(5):1381–1383.
Rosenbaum, D.M., E. Korngold, and R.L.J.A.j.o.r. Teele, Sonographic assessment of renal length in normal children. 1984;142(3):467–469.
Zerin, J. and C.J.P.r. Blane, Sonographic assessment of renal length in children: a reappraisal. 1994;24(2):101–106.
Rosenberg, H., et al., Normal splenic size in infants and children: sonographic measurements. 1991;157(1):119–121.
Carpentieri, U., et al., Liver size in normal infants and children. 1977;70(9):1096–1097.
Soyupak, S.K., et al., Sonographic measurements of the liver, spleen and kidney dimensions in the healthy term and preterm newborns. 2002;43(1):73–78.
Dinkel, E., et al., Kidney size in childhood sonographical growth charts for kidney length and volume. 1985;15(1):38–43.
Han, B.K. and D.S.J.A.j.o.R. Babcock, Sonographic measurements and appearance of normal kidneys in children. 1985;45(3):611–616.
Dremsek, P., et al., Kidney dimensions in ultrasound compared to somatometric parameters in normal children. 1987;17(4):285–290.
Carrico, C.W. and J.M.J.P.r. Zerin, Sonographic measurement of renal length in children: does the position of the patient matter? 1996;26(8):553–555.
Mathur, S., et al., Sonographic renal length in Indian children. 1996;63(4):553–557.
Christophe, C., et al., Ultrasound: a method for kidney size monitoring in children. 1986;145(6):532–538.
Hosey, R.G., et al., Ultrasound assessment of spleen size in collegiate athletes. 2006;40(3):251–254.
Eze, C.U., et al., Sonographic biometry of spleen among school-age children in Nsukka, Southeast, Nigeria. 2013;13(2):384–392.
Safak, A.A., E. Simsek, and T.J.J.o.u.i.m. Bahcebasi, Sonographic assessment of the normal limits and percentile curves of the liver, spleen, and kidney dimensions in healthy school-aged children. 2005;24(10):1359–1364.
Schlesinger, A., K. Edgar, and L.J.A.A.j.o.r. Boxer, Volume of the spleen in children as measured on CT scans normal standards as a function of body weight. 1993;160(5):1107–1109.
Acknowledgements
We would like to say thank you to the Debre Markos university research directorate that sponsored us while collecting data. Debre Markos comprehensive specialized hospital, Bichena primary hospital, and F/Selam general hospital staffs of pediatric and radiology departments thank you very much for your continuous support of the data collection procedure.
Funding
No funding.
Author information
Authors and Affiliations
Contributions
BT and DS, AA conceived and designed the study; had analyzed data. ME involved in the ultrasonographic measurement of spleen dimension. BT also wrote the initial draft of the manuscript, which was critically reviewed by DS, AA, and ME. All have read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Written informed consent was obtained from the participants and parents, the study was conducted per the Declaration of Helsinki. The ethical clearance was taken from Debre Markos University, school of medicine Ethical review committee. A permission letter was also accepted from primary and referral hospitals.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tsehay, B., Shitie, D., Afenigus, A. et al. Sonographic evaluation of spleen size in apparently healthy children in north-west Ethiopia, 2020: time to define splenomegaly. BMC Pediatr 21, 318 (2021). https://doi.org/10.1186/s12887-021-02792-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-021-02792-z