
Abstract
Background
Fluid therapy is a cornerstone of pediatric intensive care medicine. We aimed at quantifying the load of water, sodium and chloride due to different fluid indications in our pediatric intensive care unit (PICU). We were particularly interested in the role of fluid creep, i.e. fluid administered mainly as the vehicle for drugs, and the association between sodium load and water balance.
Methods
Critically ill children aged ≤3 years and invasively ventilated for ≥48 h between 2016 and 2019 in a single tertiary center PICU were retrospectively enrolled. Need for renal replacement therapy, plasmapheresis or parenteral nutrition constituted exclusion criteria. Quantity, quality and indication of fluids administered intravenously or enterally, urinary output and fluid balance were recorded for the first 48 h following intubation. Concentrations of sodium and chloride provided by the manufacturers were used to compute the electrolyte load.
Results
Forty-three patients (median 7 months (IQR 3–15)) were enrolled. Patients received 1004 ± 284 ml of water daily (153 ± 36 ml/kg/day), mainly due to enteral (39%), creep (34%) and maintenance (24%) fluids. Patients received 14.4 ± 4.8 mEq/kg/day of sodium and 13.6 ± 4.7 mEq/kg/day of chloride, respectively. The majority of sodium and chloride derived from fluid creep (56 and 58%). Daily fluid balance was 417 ± 221 ml (64 ± 30 ml/kg/day) and was associated with total sodium intake (r2 = 0.49, p < 0.001).
Conclusions
Critically ill children are exposed, especially in the acute phase, to extremely high loads of water, sodium and chloride, possibly contributing to edema development. Fluid creep is quantitatively the most relevant fluid in the PICU and future research efforts should address this topic in order to reduce the inadvertent water and electrolyte burden and improve the quality of care of critically ill children.
Similar content being viewed by others
Background
Water is the main constituent of the human body. Indeed, 60–70% of the body weight of an adult is made of water and the percentage rises up to 75–80% when dealing with infants and young children [1,2,3]. Due to several reasons, including this very high total body water content, greater insensible losses caused by a higher surface area to body mass ratio [4], a higher metabolic rate [5] and the possible presence of immature regulatory mechanisms [6, 7], children (especially newborns and children up to three years) develop frequent water and electrolyte imbalances.
Intravenous fluid therapy is therefore a cornerstone of pediatric critical care medicine and the prescription of intravenous fluids needs to be approached as any other pharmacological treatment, i.e., intravenous fluids have clear indications, contraindications and possible side effects [8]. Classically, only three clinical indications for intravenous fluid prescription exist:
1) Fluid resuscitation, i.e. rapid infusion of parenteral fluids in order to correct an acute intravascular fluid deficit [9]; 2) fluid replacement, i.e. parenteral fluids administered in stable patients in order to replace past or ongoing extracellular fluid losses, when oral fluid intake is inadequate, and 3) fluid maintenance, i.e. to provide water and electrolytes in hemodynamically stable children that are not able/allowed to drink water [10].
In addition, a substantial and frequently neglected water and electrolyte amount is administered to patients as a vehicle for intravenous drugs (sedatives, antibiotics, etc.), to provide patency of indwelling vascular catheters and to flush venous lines after blood withdrawal or drug administration [11,12,13]. This frequently neglected category of fluids has been recently termed as fluid creep [14], in analogy to the excess water administered inadvertently during burn care resuscitation [15].
Isotonic saline, i.e. NaCl 0.9%, which is constituted of 154 mEq of sodium and 154 mEq of chloride per Liter, is the classical fluid creep [13]. Besides the well-known side-effects of NaCl 0.9%, including hyperchloremic metabolic acidosis and hypernatremia [16,17,18,19,20], NaCl 0.9% contributes significantly to the total daily intake of sodium and chloride. It is important to underline the fact that recommended sodium intakes for both adults and children range between 1 and 2 mEq/kg/day [21]. Furthermore, it is well known that during an abrupt increase in sodium intake, in healthy subjects, only a fraction of the excessive sodium is excreted on the first day, leading to a positive sodium balance, thus increasing the body’s sodium stores and favoring a consensual water retention and weight gain [22]. It is conceivable that these mechanisms are even more pronounced in critically ill patients who frequently have altered homeostatic mechanisms. This, of course, might foster the formation of edema and favor the worsening of the clinical condition.
The aim of the present retrospective study is to describe the current clinical practice regarding fluid therapy in the pediatric intensive care unit (PICU) of a tertiary Italian referral hospital, quantify the load of water, sodium and chloride due to different fluid indications and assess the association between sodium intake and water balance.
Methods
This retrospective, single center study was approved by the institutional review board of our hospital (decision number 502/2019). The need for informed consent was waived owing to the retrospective nature of the study.
All patients admitted to the 5-bed tertiary PICU of the Fondazione IRCCS Ca′ Granda – Ospedale Maggiore Policlinico, Milan between January 2016 and the end of May 2019 were screened for eligibility. The inclusion criteria were age ≤ 3 years and ≥ 48 h of continuative invasive mechanical ventilation. Exclusion criteria included patients < 28 days, patients who received renal replacement therapy, plasmapheresis and parental nutrition. Patients were studied for 48 h starting from the time of intubation or PICU admission if the endotracheal tube was already in place.
Clinical data were extracted from the patient data management system of our PICU (Digistat ICU- Ascom software, Scandicci, Italy). Demographic data included age, gender, body weight, height, presence and type of comorbidities. The cause of PICU admission was categorized in 4 classes: respiratory failure, sepsis/septic shock, neurological disease and post-operative. Several variables were extracted from the digital records in order to describe the severity of patients’ clinical condition. These included the use of vasopressors and/or inotropes (epinephrine, norepinephrine, dopamine or dobutamine), rescue respiratory strategies (high frequency oscillatory ventilation (HFOV), prone position) and worst values of the 48-h study period for positive end-expiratory pressure (or mean airway pressure in case of HFOV), fraction of inspired oxygen (FiO2), and ratio of arterial partial pressure of oxygen to FiO2 (P/F ratio).
In addition, data regarding administered intravenous fluids were collected. Of note, our patient data management system records semi-automatically, on an hourly basis, the type and amount of parenteral fluids administered through infusion/peristaltic pumps, while the nurses input in the system the amount and type of any other fluid administered manually. Furthermore, the patient data management system records the type and amount of enteral nutrition and/or enteral water administered to the patients.
The amount of sodium and chloride administered with each fluid was calculated multiplying the amount of intravenous fluid by the electrolyte concentration declared by the manufacturer or as assessed in previous studies [17]. In addition, the amount of sodium administered with enteral nutrition was calculated considering the electrolyte composition of the enteral preparations, as declared by the manufacturer and as summarized in Table 1.
According to the medical records, each fluid administered was assigned to a fluid indication [14]: fluid resuscitation, maintenance/replacement, enteral nutrition, blood products, and fluid creep. Fluid creep was defined as the amount of fluid administered to patients as a vehicle for intravenous drugs (sedatives, antibiotics, etc.), to provide patency of indwelling vascular catheters and to flush venous lines after blood withdrawal or drug administration.
Daily forms included also urinary output and a simplified daily fluid balance, calculated by subtracting total urinary output from the total input of parenteral and enteral water. Finally, the percentage of water, sodium and chloride administered with each indication were computed.
Statistical analysis
All data were tested for homogeneity of variance and normality of distribution using the Shapiro-Wilk test. Normally distributed data were expressed as mean ± standard deviation, while non-normally distributed data were reported as median and interquartile range. Pearson’s correlation was used to assess the association between sodium intake and cumulative water balance. Analysis was performed with SAS 9.4 (SAS Institute Inc., Cary, NC, USA) and Sigma Plot 12.0 (Systat Software Inc., San Jose, CA). A P-value lower than 0.05 was considered as statistically significant.
Results
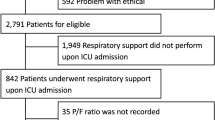
Fifty-four patients fulfilled the inclusion criteria, 11 presented exclusion criteria, leaving 43 patients for the analysis (Fig. 1). Demographic and clinical characteristics of the study population are summarized in Table 2. Patients had a median age and weight of 7 [3–15] months and 6.6 [4.7–9.0] kg, respectively. Acute respiratory failure was the cause of PICU admission in 77% percent of included patients. Comorbidities were present in 51% of patients, including children with a history of premature birth (< 37 weeks of gestational age).

Study flow chart
Acetated Ringer’s was the preferred choice for both fluid resuscitation (88 ± 33%) and fluid maintenance (88 ± 26%). The other employed intravenous fluid for these purposes was NaCl 0.9%, which was also the only type of fluid used for fluid creep. Table 3 summarizes total daily amount of water, sodium and chloride administered during the study period. On average, a daily dose of 1004 ± 284 ml (153 ± 36 ml/kg/day) of water was administered. The major source of water input was enteral nutrition (60 ± 23 ml/kg/day, 39% of total water input), followed by fluid creep (51 ± 23 ml/kg/day, 34.2%) and fluid maintenance (34 [21–50] ml/kg/day, 23.4%). The quantitative role of fluid boluses/fluid resuscitation was minor (1.7%) and quantitatively similar to blood components (1.5%).
Fluids administered as a vehicle for intravenous drugs constituted 76 ± 12% of fluid creep, while fluids administered to provide patency of catheters and for flushes constituted the remaining 24 ± 12% of fluid creep. Among intravenously administered drugs, sedatives and antibiotics where the two major sources of fluid creep (44 ± 22% and 18 ± 18%, respectively).
The daily dose of sodium was 97 ± 42 mEq (14.4 ± 4.8 mEq/kg/day). Fluid creep represented the major source of sodium (7.9 ± 3.6 mEq/kg/day, 55.7% of total sodium input), followed by maintenance fluids (32.8%), enteral feed (6.9%), fluid resuscitation (2.3%) and blood components (2.2%) (Table 3).
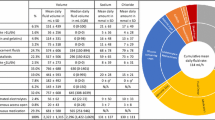
The daily dose of chloride was 92 ± 40 mEq (13.6 ± 4.7 mEq/kg/day), slightly lower than sodium. Fluid creep represented the major source of chloride (7.9 ± 3.6, 58.2% of total chloride input), followed by maintenance fluids (29.9%), enteral feed (8%), fluid resuscitation (2.1%) and blood components (1.7%). Figure 2 represents the pie charts summarizing the percentage contribution of different fluid categories to water, sodium and chloride load.

The three pie charts represent the percentage contribution of each fluid category to water, sodium and chloride input. Percentages are reported numerically within the slice for Fluid Creep, Enteral Fluid and Maintenance fluids. Both fluid resuscitation and blood components contributed approximately 2% to water, sodium and chloride input. The “exploded” pie slice refers to Fluid Creep
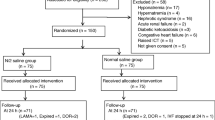
Patients had an average daily urinary output of 602 ± 242 ml, i.e. 92 ± 32 ml/kg per day. Given the total fluid input (Table 3), the result was an average daily positive fluid balance of 417 ± 221 ml, i.e. 64 ± 30 ml/kg per day. Figure 3 represents the association between the total 48-h sodium intake and total fluid balance. As can be noted, the total amount of sodium administered was strongly associated (r2 = 0.49, p < 0.0001) with cumulative fluid balance.

Correlation between total sodium intake and cumulative 48-h fluid balance. Fluid balance was calculated as total fluid intake (parenteral and enteral) – urinary output. The regression line (y = 168 + 3.3 x; r2 = 0.49, p < 0.0001) and 95% confidence band are reported
Discussion
We studied a population of young (≤3 years), severely ill, mechanically ventilated children during the first 48 h of the acute phase. The main findings of our study are (i) the overall extremely high water, sodium and chloride load, (ii) the predominant role of fluid creep, especially regarding electrolytes’ input, and (iii) the strong association between total sodium input and positive fluid balance.
In our population, the major source of water input was enteral nutrition, which already provided approximately 65% of expected water needs for healthy children, according to Holliday and Segar [23]. The second water source was fluid creep, accounting for 34% of water input, followed by fluid maintenance. As already pointed out by other authors [14, 24], also in our patients the quantitative role of fluid boluses/fluid resuscitation and blood components was minor. Given the quantitative amount and the composition of employed fluid creep, it is not surprising that this category of fluids represented the major source of sodium (56% of total sodium input, Fig. 2). Overall, the sodium load exceeded approximately 10 times the recommended sodium input [21]. Of course, it is likely that the recommended sodium inputs might not be sufficient for critically ill patients with altered vascular permeability, i.e. in patients with relative hypovolemia. Nevertheless, the administration of 56% of this load was inadvertent, i.e., from fluids administered as vehicle for intravenous drugs and to guarantee patency of indwelling intravascular catheters, namely fluid creep. It is therefore conceivable that this sodium load was not a therapeutic choice, but rather a side effect of other therapies. It might be interesting underling the fact that the sodium load deriving from enteral preparations was, on average, 1.0 ± 0.4 mEq/kg/day, i.e. very close to the recommended sodium input. This is reasonable, as enteral feeds have been prepared in order to cover all the nutritional needs, including electrolytes.
The total chloride load was slightly lower than sodium (13.6 ± 4.7 mEq/kg/day). The prevalent use of acetated Ringer’s as maintenance fluid explains this finding. Indeed, acetated Ringer’s has a sodium and chloride concentration of 132 and 110 mEq/L, respectively. Consequently, the chloride load deriving from this source is slightly lower than the corresponding sodium load. On the contrary, sodium and chloride load deriving from fluid creep are equal (7.9 ± 3.6 mEq/kg/day) as NaCl 0.9% was used for this purpose.
The high chloride burden due to fluid therapy in general, and fluid creep in particular, might contribute to the development of hyperchloremia, with the related side effects [25]. Hyperchloremia might cause metabolic acidosis [16, 20], alter the contractility of arteriolar smooth muscles [26, 27], potentially altering renal perfusion and contributing to renal dysfunction [28]. Furthermore, high chloride concentrations might favor lower urinary sodium excretion thus contributing to edema formation [29, 30]. Indeed, despite a preserved renal function, the fluid balance was extremely positive (64 ± 30 ml/kg/day), significantly higher than the one reported in previous studies [11]. This is likely due to the fact that we selected a population of young, particularly sick and mechanically ventilated children. These three factors taken together certainly amplified the clinical significance. Nevertheless, fluid overload, a major issue in the ICU, is associated with worse clinical outcomes [31]. Interestingly, a good linear correlation was found between total sodium intake and fluid balance (Fig. 3). Again, it is worth repeating that 56% of the sodium load was inadvertent, i.e. it derived from fluid creep. When analyzing the two major components of fluid creep, we found that the majority (76%) was due to the dilution of intravenous drugs, while the remaining part (24%) was due to the use of fluids to guarantee catheters’ patency.
The cultural awareness regarding intravenous fluids is certainly increasing [32,33,34,35] and careful determination is occurring with regards to the indication, the preferred composition and the possible side effects to intravenous fluids. However, most of the scientific attention has been directed towards resuscitation, replacement and maintenance fluids.
Indeed, there is strong consensus regarding the tonicity of fluids for resuscitation and replacement, i.e., in this context isotonic, possibly balanced fluids should be preferred. On the contrary, there is a great debate regarding the appropriate tonicity of maintenance fluids [36,37,38,39]. Many clinicians suggest to use isotonic maintenance fluids in order to avoid the risk of hyponatremia and cerebral edema [40]. On the contrary, other authors promote the use of hypotonic fluids in order to avoid “water and salt intoxication” [41, 42].
Finally, it is not surprising that, at the time of writing, no indication exists regarding fluid creep. Indeed, these fluids have been neglected for a very long time and only recently, the research interest in the topic is increasing [11, 12, 14, 24, 43, 44]. However, given the fact that fluid creep can account up to 50% of daily parenteral fluid administration and a similar percentage of total daily sodium load in critically ill children admitted to the PICU, we can firmly state that they are conceptually as important as, and quantitatively even more important than resuscitation, replacement and maintenance fluids. Indeed, in a recent before-and-after study performed in a single center adult ICU, Bihari and colleagues demonstrated that the sodium burden and positive fluid balance deriving from fluid creep can be safely reduced by switching from an isotonic solution, such as NaCl 0.9%, to a hypotonic solution, such as 5% glucose [45]. This important research topic needs to be addressed further, possibly with randomized control trials, also in the pediatric population.
Other possible strategies to reduce the water, sodium and chloride burden of intravenous fluids would be to favor, whenever possible, the enteral route for drug administration; to concentrate as much as possible parenteral drugs; to review, on a daily basis, the indications of intravenous fluids, i.e. to adopt strategies of fluid stewardship [46] and to avoid displaying tracings of central venous pressure or arterial pressure, unless strictly necessary. Indeed, pressure transducers used in our PICU require a continuous drip of 3 ml/h of fluid. If both an arterial and central line are in place, this already results in a daily load of 144 ml of water and 22 mEq of sodium and chloride.
There were several limitations to our study. First, the study was retrospective in nature and data derived from only 43 patients of the same PICU. Consequently, the small number of patients hampers the generalizability of our findings. The extensive use of non-invasive ventilation in our PICU and the established tendency to intubate and ventilate invasively patients only as last resort, might in part explain the limited number of included patients. Second, we had no data on urinary sodium and chloride excretion. It was thus impossible to assess sodium and chloride balance. Third, we did not consider the sodium content of antibiotics, which can be significant [12]. Finally, it is possible that some flushes or extemporary therapies were not inserted manually in the patient management system. Taking together these last two aspects, it is conceivable that the effective water, sodium and chloride load might have been slightly underestimated.
Conclusions
In conclusion, our study described the clinical practice regarding fluid administration in critically ill, mechanically ventilated patients under 3 years of age, treated at our PICU. We had established protocols in our unit for drug dilution, not necessarily employing the maximal possible concentration. Furthermore, we did not have local protocols to reduce the inadvertent amount of fluids deriving from crystalloids used to guarantee the patency of catheters. As a result, our current clinical approaches and habits unequivocally lead to an inadvertent and excessive water, sodium and chloride load, which might contribute to the development of edema and significantly impact on patients’ outcomes. Fluid creep is quantitatively the most relevant fluid in the PICU and future research and clinical efforts should address this topic in order to improve the quality of care of critically ill children.
Availability of data and materials
All data generated or analysed during this study are made available from the authors.
Abbreviations
- Cl:
-
Chloride
- FiO2 :
-
Fraction of inspired oxygen
- HFOV:
-
High frequency oscillatory ventilation
- IQR:
-
Interquartile range
- IRCCS:
-
Istituto di Ricerca e Cura a Carattere Scientifico
- Na:
-
Sodium
- P/F ratio:
-
Ratio of arterial pressure of oxygen to FiO2
- PEEP:
-
Positive end-expiratory pressure
- PICU:
-
Pediatric Intensive Care Unit
- PICU LOS:
-
PICU length of stay
References
Friis-Hansen B. Body water compartments in children: changes during growth and related changes in body composition. Pediatrics. 1961;28:169–81.
Friis-Hansen BJ, Holiday M, Stapleton T, Wallace WM. Total body water in children. Pediatrics. 1951;7(3):321–7.
Langer T, Limuti R, Tommasino C, van Regenmortel N, Duval E, Caironi P, et al. Intravenous fluid therapy for hospitalized and critically ill children: rationale, available drugs and possible side effects. Anaesthesiol Intensive Ther. 2018;50(1):49–58.
Heeley AM, Talbot NB. Insensible water losses per day by hospitalized infants and children. AMA Am J Dis Child. 1955;90(3):251–5.
Darrow DC, Pratt EL. Fluid therapy; relation to tissue composition and the expenditure of water and electrolyte. J Am Med Assoc. 1950;143(5):432–9.
Mårild S, Jodal U, Jonasson G, Mangelus L, Odén A, Persson NG. Reference values for renal concentrating capacity in children by the desmopressin test. Pediatr Nephrol. 1992;6(3):254–7.
O'Brien F, Walker IA. Fluid homeostasis in the neonate. Paediatr Anaesth. 2014;24(1):49–59.
Malbrain ML, Van Regenmortel N, Owczuk R. It is time to consider the four D's of fluid management. Anaesthesiol Intensive Ther. 2015;47(Spec):s1–5.
Myburgh JA, Mythen MG. Resuscitation fluids. N Engl J Med. 2013;369(25):2462–3.
Moritz ML, Ayus JC. Maintenance intravenous fluids in acutely ill patients. N Engl J Med. 2016;374(3):290–1.
Bihari S, Festa M, Peake SL, Seppelt IM, Williams P, Wilkins B, et al. Sodium administration in critically ill paediatric patients in Australia and New Zealand: a multicentre point prevalence study. Crti Care Resusc. 2014;16(2):112–8.
Bihari S, Ou J, Holt AW, Bersten AD. Inadvertent sodium loading in critically ill patients. Crti Care Resusc. 2012;14(1):33–7.
Choo WP, Groeneveld AB, Driessen RH, Swart EL. Normal saline to dilute parenteral drugs and to keep catheters open is a major and preventable source of hypernatremia acquired in the intensive care unit. J Crit Care. 2014;29(3):390–4.
Van Regenmortel N, Verbrugghe W, Roelant E, Van den Wyngaert T, Jorens PG. Maintenance fluid therapy and fluid creep impose more significant fluid, sodium, and chloride burdens than resuscitation fluids in critically ill patients: a retrospective study in a tertiary mixed ICU population. Intensive Care Med. 2018;44(4):409–17.
Saffle JI. The phenomenon of “fluid creep” in acute burn resuscitation. J Burn Care Res. 2007;28(3):382–95.
Langer T, Carlesso E, Protti A, Monti M, Comini B, Zani L, et al. In vivo conditioning of acid-base equilibrium by crystalloid solutions: an experimental study on pigs. Intensive Care Med. 2012;38(4):686–93.
Langer T, Ferrari M, Zazzeron L, Gattinoni L, Caironi P. Effects of intravenous solutions on acid-base equilibrium: from crystalloids to colloids and blood components. Anaesthesiol Intensive Ther. 2014;46(5):350–60.
Langer T, Santini A, Scotti E, Van Regenmortel N, Malbrain ML, Caironi P. Intravenous balanced solutions: from physiology to clinical evidence. Anaesthesiol Intensive Ther. 2015;47(Spec):s78–88.
Morgan TJ, Venkatesh B, Hall J. Crystalloid strong ion difference determines metabolic acid-base change during in vitro hemodilution. Critical Care Med. 2002;30(1):157–60.
Scheingraber S, Rehm M, Sehmisch C, Finsterer U. Rapid saline infusion produces hyperchloremic acidosis in patients undergoing gynecologic surgery. Anesthesiology. 1999;90(5):1265–70.
Jochum F, Moltu SJ, Senterre T, Nomayo A, Goulet O, Iacobelli S. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Fluid and electrolytes. Clin Nutr. 2018;37(6 Pt B):2344–53.
Drummer C, Gerzer R, Heer M, Molz B, Bie P, Schlossberger M, et al. Effects of an acute saline infusion on fluid and electrolyte metabolism in humans. Am J Phys. 1992;262(5 Pt 2):F744–54.
Holliday MA, Segar WE. The maintenance need for water in parenteral fluid therapy. Pediatrics. 1957;19(5):823–32.
Bihari S, Peake SL, Seppelt I, Williams P, Bersten A. Sodium administration in critically ill patients in Australia and New Zealand: a multicentre point prevalence study. Crit Care Resusc. 2013;15(4):294–300.
Handy JM, Soni N. Physiological effects of hyperchloraemia and acidosis. Br J Aneasth. 2008;101(2):141–50.
Hansen PB, Jensen BL, Skott O. Chloride regulates afferent arteriolar contraction in response to depolarization. Hypertension. 1998;32(6):1066–70.
Wilcox CS. Regulation of renal blood flow by plasma chloride. J Clin Invest. 1983;71(3):726–35.
Semler MW, Self WH, Rice TW. Balanced crystalloids versus saline in critically ill adults. N Engl J Med. 2018;378(20):1951.
Lobo DN, Stanga Z, Aloysius MM, Wicks C, Nunes QM, Ingram KL, et al. Effect of volume loading with 1 liter intravenous infusions of 0.9% saline, 4% succinylated gelatine (Gelofusine) and 6% hydroxyethyl starch (Voluven) on blood volume and endocrine responses: a randomized, three-way crossover study in healthy volunteers. Crti Care Med. 2010;38(2):464–70.
Reid F, Lobo DN, Williams RN, Rowlands BJ, Allison SP. (ab) normal saline and physiological Hartmann's solution: a randomized double-blind crossover study. Clin Sci (London). 2003;104(1):17–24.
Flores-González JC, Valladares CM, Yun Castilla C, Mayordomo-Colunga J, Quesada SP, Martín Delgado CM, et al. Association of Fluid Overload with Clinical Outcomes in critically ill children with bronchiolitis: Bronquiolitis en la Unidad de Cuidados Intensivos Pediátricos (BRUCIP) study. Pediatr Crit Care Med. 2019;20(3):e130–e6.
Caironi P, Langer T, Gattinoni L. Albumin in critically ill patients: the ideal colloid? Curr Opin Crit Care. 2015;21(4):302–8.
Finfer S, Myburgh J, Bellomo R. Intravenous fluid therapy in critically ill adults. Nat Rev Nephrol. 2018;14(9):541–57.
Malbrain M, Langer T, Annane D, Gattinoni L, Elbers P, Hahn RG, et al. Intravenous fluid therapy in the perioperative and critical care setting: executive summary of the international fluid academy (IFA). Ann Intensive Care. 2020;10(1):64.
Van Regenmortel N, Jorens PG, Malbrain ML. Fluid management before, during and after elective surgery. Curr Opin Crit Care. 2014;20(4):390–5.
Choong K, Arora S, Cheng J, Farrokhyar F, Reddy D, Thabane L, et al. Hypotonic versus isotonic maintenance fluids after surgery for children: a randomized controlled trial. Pediatrics. 2011;128(5):857–66.
Friedman JN, Beck CE, DeGroot J, Geary DF, Sklansky DJ, Freedman SB. Comparison of isotonic and hypotonic intravenous maintenance fluids: a randomized clinical trial. JAMA Pediatr. 2015;169(5):445–51.
McNab S. Isotonic vs hypotonic intravenous fluids for hospitalized children. JAMA. 2015;314(7):720–1.
McNab S, Ware RS, Neville KA, et al. Isotonic versus hypotonic solutions for maintenance intravenous fluid administration in children. Cochrane Database Syst Rev. 2014;(12):CD009457. Published 2014 Dec 18. https://doi.org/10.1002/14651858.CD009457.pub2.
Arieff AI, Ayus JC, Fraser CL. Hyponatraemia and death or permanent brain damage in healthy children. BMJ. 1992;304(6836):1218–22.
Van Regenmortel N, De Weerdt T, Van Craenenbroeck AH, Roelant E, Verbrugghe W, Dams K, et al. Effect of isotonic versus hypotonic maintenance fluid therapy on urine output, fluid balance, and electrolyte homeostasis: a crossover study in fasting adult volunteers. Br J Anaesth. 2017;118(6):892–900.
Van Regenmortel N, Hendrickx S, Roelant E, Baar I, Dams K, Van Vlimmeren K, et al. 154 compared to 54 mmol per liter of sodium in intravenous maintenance fluid therapy for adult patients undergoing major thoracic surgery (TOPMAST): a single-center randomized controlled double-blind trial. Intensive Care Med. 2019;45(10):1422–32.
Bihari S, Gelbart B, Seppelt I, Thompson K, Watts N, Prakash S, et al. Maintenance fluid practices in paediatric intensive care units in Australia and New Zealand. Crit Care Resusc. 2017;19(4):310–7.
Fuhrman D, Crowley K, Vetterly C, Hoshitsuki K, Koval A, Carcillo J. Medication use as a contributor to fluid overload in the PICU: a prospective observational study. J Pediatr Intensive Care. 2018;7(2):69–74.
Bihari S, Prakash S, Potts S, Matheson E, Bersten AD. Addressing the inadvertent sodium and chloride burden in critically ill patients: a prospective before-and-after study in a tertiary mixed intensive care unit population. Crit Care Resusc. 2018;20(4):285–93.
Malbrain M, Van Regenmortel N, Saugel B, De Tavernier B, Van Gaal PJ, Joannes-Boyau O, et al. Principles of fluid management and stewardship in septic shock: it is time to consider the four D's and the four phases of fluid therapy. Ann Intenisve Care. 2018;8(1):66.
Acknowledgements
The authors are thankful to the patients, to their parents, to the nurses and doctors of the pediatric ICU “De Marchi” and to the Associazione Bambino Nefropatico.
Funding
The publication fees of the present study were covered by institutional funds of the Fondazione IRCCS Ca′ Granda Ospedale Maggiore Policlinico, Milan, Italy. Ricerca Corrente 2019: “Water and sodium administration in the paediatric intensive care unit”.
Author information
Authors and Affiliations
Contributions
TL designed the study, contributed to the literature research, analyzed data, prepared the manuscript and approved the final version of the manuscript. VDO and GCS collected data and contributed to study design, literature research, data analysis and manuscript preparation. GC, SSC, TM contributed to the study design and manuscript preparation. MG and AC contributed to data collection, literature research and data analysis. CA, AP and EC contributed to the study design, revised critically the manuscript for important intellectual content. All authors gave final approval of the version to be submitted.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the ethics committee (N°502/2019) of the Policlinico Ca′ Granda Hospital in Milan (Comitato Etico Milano Area 2).
Consent for publication
Given the retrospective nature of the study, the ethics committee waived the need for informed consent.
Competing interests
The authors declare that they have no competing interests related to the present study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Langer, T., D’Oria, V., Spolidoro, G.C.I. et al. Fluid therapy in mechanically ventilated critically ill children: the sodium, chloride and water burden of fluid creep. BMC Pediatr 20, 424 (2020). https://doi.org/10.1186/s12887-020-02322-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-020-02322-3