
Abstract
Background
To determine the association between malnutrition and early childhood caries (ECC) in children resident in sub-urban, Nigeria.
Methods
This study was a subset of a larger cross-sectional study the data of which was generated through a household survey conducted in Ile-Ife, Nigeria. The study’s explanatory variable was malnutrition (underweight, overweight, wasting and stunting) and the outcome variable was ECC. Poisson regression analysis was used to determine the association between ECC and malnutrition. Variables (sex, frequency of sugar consumption, maternal knowledge of oral hygiene, oral hygiene status) associated with ECC in the primary study were adjusted for to obtain the adjusted prevalence ratio (APR).
Results
Of the 370 children, 20 (5.41%) were underweight, 20 (5.41%) were overweight, 67 (18.11%) were wasting, 120 (32.43%) were stunted and 18 (4.86%) had ECC. Factors associated with ECC were being stunted, underweight, overweight and fair oral hygiene. The prevalence of ECC was lower in children who were stunted (APR: 0.14; 95% CI: 0.03–0.69; p = 0.02), almost seven times higher in children who were overweight (APR: 6.88; 95% CI: 1.83–25.85; p < 0.001), and predictively absent in children who were underweight (APR: 0; 95% CI: 0–0; p < 0.001) when compared with children who had normal weight. Non-significant risk indicators for ECC included consuming sugar between meals three times a day or more, having low socioeconomic status and being female.
Conclusions
For this study population, the indicators of malnutrition – being stunted, underweight, overweight - and fair oral hygiene were risk indicators for ECC. The frequency of sugar consumption was not a significant risk indicator when malnutrition was included as an explanatory variable for ECC in the study population.
Similar content being viewed by others


Background
Early childhood caries (ECC) – defined as caries in children under 6 years of age who had one or more decayed, missing or filled tooth surfaces in any primary tooth [1] - raises concern because of the possible link with malnutrition (little or too much of some nutrients). ECC leads to pain when not managed, and the pain contributes to poor feeding, nutrient deficiency [2,3,4] and growth failure (underweight, stunted and wasted) [5, 6]. Also, children with ECC have high levels of pro-inflammatory cytokines [7], which trigger a cascade of inflammatory processes [8] associated with impaired growth and obesity inducing mechanisms [9]. Obesity and stunting also cause changes in the salivary glands and the composition of saliva, which increases the risk for ECC by lowering salivary pH [10].
The association between ECC and malnutrition is however, not clear. Although a few studies have found an association between ECC, body mass index (BMI) [11,12,13] and growth failure [14,15,16,17,18], others have found no associations [6, 19,20,21]. Also, while large population-based studies found no association between BMI and ECC [19, 22,23,24], a longitudinal study indicated that malnutrition causes ECC [25], ECC causes stunting, and underweights have more ECC [26], ECC and obesity are both risk factors for type 2 diabetes [27].
Recent emerging evidence suggest that children with ECC have higher levels of pro-inflammatory cytokines [8]. Cytokines act as mediators of inflammation, infection and immunological processes [28] and they increase with increased severity of ECC [8]. The pro-inflammatory cytokines produces free radicals that generate peroxides, Prostaglandin E2, interleukin 6, tumour necrotizing factor -alpha and cysteinyl leukotrienes – powerful agents in the inflammatory response [29] – which are significantly associated with increased nutritional risk [30]. These inflammatory activities seen in ECC are a component of the pathogenesis of illness-related malnutrition [31, 32] and can impair growth [33]. Severe ECC is associated with iron deficiency anemia [34] which reduces salivary flow [3]; and vitamin D [2, 4], vitamin A, calcium and albumin deficiencies which causes enamel hypoplasia/hypomineralization [35], and lose of the protective effect of iron, vitamins and zinc for the teeth [36].
Malnutrition accounted for 21 to 50% of under-5 deaths and a large proportion of morbidity in low and middle-income countries in 2017 [37]. Malnutrition also contributes to under-5 mortality in Nigeria [38]. The prevalence of malnutrition in Nigeria is higher in rural than in urban areas [39]. For a developing country like Nigeria, identifying factors that contribute to malnutrition may help enhance the design of comprehensive programs to tackle the problem.
The studies on the association between malnutrition and caries in Nigeria were conducted in children older than 5 years [11, 40]. These studies were school-based and found no association between BMI and caries. School-based studies in Nigeria have a problem of representativeness because only 35.6% of children aged 36–59 months receive early childhood education [41], making the samples non-representative of the general population. Consequently, we have conducted a secondary data analysis of a population-based survey of a semi-urban population in Nigeria, to determine if there was any association between ECC and malnutrition in children younger than 6 years. We hypothesized that there is no association between ECC and the nutritional status of children younger than 6 years in Ile-Ife, Nigeria.
Methods
This study was a sub-study of a primary study that determined the association between digit sucking, caries and periodontitis in 6-months-olds to 12-year-olds resident in Ile-Ife [42]. The primary data were collected through a household survey using a three-level cluster sampling procedure. This involved an initial random selection of enumeration areas within the Ife Central local government area, then the selection of every third household on each street in the randomly selected enumeration areas in the local government area, and finally the selection of an eligible individual from each household. Children who fell within the target age group, were living with their biological parents or legal guardians, and who consented to participate in the study were recruited for the study. Details on the sampling process had been discussed in the primary study [43].
Ethics consideration
Ethical approval for the study was obtained from the Health Research Ethics Committee of the Obafemi Awolowo University Teaching Hospitals’ Complex Ile-Ife (ERC/2013/07/14). The primary study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects/patients were approved by the Institute of Public Health-Health Research Ethics Committee. Written informed consent was obtained from the parents or legal guardian of the study participants.
Sample size and data collection procedures
The estimated sample size for this secondary data analysis was based on the ECC prevalence of 6.6% generated from the primary study [43]. With a 3% margin of error and a confidence level of 95% precision, a sample size of 263 study participants will be adequate to determine the association between ECC and malnutrition for this secondary data analysis. There were 370 data points extracted from the primary study database for this analysis. This exceeded the needed minimum sample required for this study. We therefore had adequate sample size to determine an association between ECC and malnutrition. The data collection instrument for the main study is included in this manuscript as Additional file 1.
Socioeconomic status
Socioeconomic status was assessed because of its role as a determinant of malnutrition. It was measured according to a classification validated for use in Nigeria. The index combines the mother’s education and the father’s occupation to obtain five socio-economic classes for children [44]. Class 1 indicates upper class, class II upper middle class, class III middle class, class IV lower middle class, and class V lower class. For the present analysis, these classes were regrouped into three: high (upper and upper middle classes), middle (middle class) and low (lower middle and lower classes).
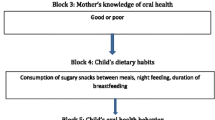
Mothers’ knowledge of oral health
Folayan et al. [43] described how data on mothers’ knowledge of oral health were collected and handled. The same data were used for this study. Briefly, data were collected using a tool with a possible score ranging from 8 to 40. Scores of 21 and above were categorized as good oral health knowledge, and scores of 20 and below were categorized as poor oral health knowledge.
Cariogenic diet
The frequency of consumption of sugary snacks between main meals was collected with a tool described in detail by Folayan et al. [45]. Consumption of sugary snacks between main meals three times a day or more is a significant risk factor for ECC [43].
Nutritional status
Nutritional status was assessed based on weight and height of each child according to the International Society for the Advancement of Kinanthropometry standard protocol [46]. Weight was measured in kilograms with an electronic weighing scale and recorded to the nearest tenth of a kilogram. The weighing scale was zero-balanced before the child stepped on it. Each child removed heavy items of clothing and mounted the scale bare footed, standing still and looking straight. Measurements were recorded after fluctuations on the digital screen had stopped
Children’s height was measured in meters with an anthropometer-calibrated customized stadiometer. Each child was asked to step on the standiometer bare footed. Height was the maximum vertical distance from the feet to the vertex of the head, with the head held parallel to the Frankfort plane [47]. In this position, the child looked straight, with arms hanging naturally by the sides and both heels together touching the base of the stadiometer. The heels, buttocks and upper part of the back and back of the head were in contact with the stadiometer. The headpiece was brought down to contact the vertex of the head. The measurement was read to the nearest tenth of a centimeter and converted to a fraction of meter.
Nutritional status was determined according to criteria used by the WHO: height (H), age (A) and weight (W) [47]. Children whose H/A Z-score was below minus two standard deviations from the median of the WHO reference population were considered stunted. Children whose W/H Z-score was below minus two standard deviations from the reference population median were considered wasted. Children whose W/A was below minus two standard deviations from the reference population median were classified as underweight. Children whose W/Z-score was plus one standard deviations from the reference median were considered overweight, and those who were two standard deviations from the reference median were considered obese.
Oral examination for each child was conducted in the homes of the study participants. The participants were examined sitting, under natural light, using sterile dental mirrors and probes by trained dentists who were calibrated on the use of the WHO criteria for caries diagnosis, and the OHI-S index for assessment of the oral hygiene status. Radiographs were not used in this study. The intra-examiner correlation scores ranged between 0.89–0.94, while inter-examiner kappa Cohen scores ranged between 0.82–0.90 for caries detection and OHI-S [42, 43].
ECC status
The dmft was identified according to the World Health Organization (WHO) criteria [48]. The dmft score was obtained by adding the d, m and f scores for each child less than 6 years of age. The dmft score was dichotomized into 0 = ECC absent and > 0 = ECC present.
Oral hygiene status
Oral hygiene status was assessed with the index of Greene and Vermillion [49]. Good oral hygiene was graded from 0.0 to 1.2; fair oral hygiene from 1.3 to 3.0; and poor oral hygiene from 3.1 and above.
Data analysis
The mean(SD) age, dmft, oral hygiene score, and proportion of those with ECC, and malnutrition were calculated. Socio-demographic profile of participants in the present study and the original study were compared using chi-square test to establish comparability and ensuring that the present sample is representative of the target population like the original sample.
The association between nutritional status and ECC presence (yes/ no) and confounding variables (age, sex, socio-economic status, frequency of sugar consumption between meals, oral hygiene status and maternal knowledge of oral health) was determined with the chi-square test or Fisher’s exact test where appropriate.
Multivariable Poisson regression models were used to assess the relationship between exposure (nutritional status) and confounders on the outcome variable (presence of ECC measured by prevalence ratio: ECC PR). A modified theoretical model outlined by Folayan et al. [43], was used to assess how various indicators explained ECC PR when they were grouped into blocks. Factors were grouped under three blocks and were successively introduced, one block at a time. Each model included the block of nutritional status (WAZ, HAZ and WHZ) as this was the variable assessed for being a risk indicator for ECC. Other blocks moved into the next model if the p value was < 0.2. Model 1 included only the block of nutritional status, while Model 2 included the block of nutritional status and the block of socio-economic and demographic factors (age was excluded because of possible collinearity since it was used to compute nutritional status) since these factors could influence caries and nutritional status. Model 3 included variables that met the inclusion criteria for the next model and they were known moderator variables of the association between ECC and malnutrition namely mother’s knowledge of oral health, frequency of daily consumption of sugar and oral hygiene index. At the introduction of a new block with its factor(s), the variables of all blocks were adjusted simultaneously for each other to produce adjusted prevalence ratios (APRs). To avoid sparse data bias [50] introduced by the low prevalence of ECC, underweight, overweight or their combination, we used robust variance estimation [51].
The cross tabulations were generated with IBM SPSS version 23. The test of association was and the Poisson regression analysis was conducted using Stata 15. The test of significance was set at P < 0.05.
Results
Although 497 children younger than 6 years were recruited into the primary study, only 370 (74.45%) with data on nutritional status were included in this analysis. The mean(SD) age of the 370 children was 44.35 (16.03) months. Also, 20 (5.41%) were underweight, 20 (5.41%) were overweight, 67 (18.11%) were wasting, 120 (32.43%) were stunted and 18 (4.86%) had ECC. The mean (SD) dmft score was 0.14(0.80) and the mean(SD) oral hygiene score was 1.12(1.21).
Table 1 shows the socio-demographic profile of the study participants in the primary study and this study. There was no significant difference in the age (p = 0.89), sex (p = 0.69), socioeconomic status (p = 0.19) and the prevalence of ECC (p = 0.19) of the children in the primary study and the current study.
Factors associated with ECC: Table 2 shows the factors associated with ECC. ECC was significantly associated with only age (p = 0.02): ECC prevalence was highest in the age group 48–59 months.
Risk indicators for ECC: Table 3 shows the results of the Poisson regression models with robust variance estimation because of sparse data. The significant risk indicators for ECC were stunted, underweight, overweight and fair oral hygiene. None of the study participants had poor oral hygiene. In Model 3 where all confounders were controlled for, the prevalence of ECC was 66% lower in children who were stunted (APR: 0.14; 95% CI: 0.03–0.69; p = 0.02) and almost seven times higher in children who were overweight (APR: 6.88; 95% CI: 1.83–25.85; p < 0.001) than in children who had normal weight. The APR of ECC in children with underweight was nil (APR: 0; 95% CI: 0–0; p < 0.001) when compared with children who had normal weight. Among the studied children with ECC, none had poor oral hygiene (APR: 0; 95% CI: 0–0; p < 0.001, Tables 2 and 3). Non-significant risk indicators for ECC included consuming sugar between meals three times a day or more (APR: 2.18), having low socioeconomic status (APR: 2.40) and being female (APR: 2.90). This model explained 18% of the differences in the prevalence of ECC observed. The pseudo R2 of the model for ECC increased with the addition of each block, indicating validity of the choice of confounders for caries in the study population.
Discussion
For this study population, our hypothesis was sustained - there was an association between ECC and nutritional status of pre-school children: children who were stunted or underweight had a lower prevalence of ECC and children who were overweight had higher prevalence of ECC. ECC was also associated with oral hygiene status ECC in the study population: children with fair oral hygiene had higher prevalence of ECC than those with good oral hygiene. There were no child with ECC who had poor oral hygiene and so the full extent of the oral hygiene/ECC relationship cannot be assessed. Prior significant factors associated with ECC in the study population – consumption of sugar between meals three times a day or more, being female and having mothers with poor knowledge of oral health – lost their significance in this study, as explanatory factors for ECC.
One of the strengths of the study was that its theoretical model for the study was built on evidence generated from the latest study conducted to identify risk indicators for ECC in Ile-Ife. Also, the study sample is representative of the study population and therefore, the results can be generalized to the study population and to Southwestern Nigeria, a region where the culture and diet – social factors associated with ECC - are similar to that of Ile-Ife [52]. The z score used to determine the nutritional status of the study population is more appropriate for children 2-year-old and younger [53], thereby increasing the validity of the study results [54]. Also, the robust estimation of variance analysis enhanced the validity of the inferential analysis conducted for the subgroups with small sample size.
This study contributes to the sparse literature on the relationship between malnutrition and ECC in sub-Saharan Africa. Although the continent has a high prevalence of malnutrition [55] and a rising caries prevalence [56], the publications on ECC and nutrition are only from Kenya [57, 58], South Africa [59] and Egypt [60]. These previous studies found no significant relationship between ECC and nutritional status. Unlike those studies, we found that being stunted, underweight and overweight were associated with ECC.
The association between ECC and malnutrition had been highlighted in prior studies. Malnutrition results in salivary gland hypofunction, changes in the saliva composition and reduction in its buffering capacity thereby enhancing caries formation [61]. A prior study conducted in Nigeria, had also identified that fair oral hygiene was associated with higher prevalence of ECC [62], while another study highlighted an increase in ECC prevalence as oral hygiene worsened [63]. The calculated estimate for the association between oral hygiene and ECC in this study should be interpreted with caution bearing in mind that there were no children with poor oral hygiene among those with ECC though the overall prevalence of poor oral hygiene was 2.2%. It is important to explore this finding.
We found no significant association between ECC and high sugar consumption in the study population when the analytical model included nutrition status. This may be an indication that the oral hygiene status may be the pathway for caries formation in this population rather than the high frequency of sugar consumption. Malnutrition results in enamel hypoplasia, which creates a nitche environment for plaque retention [61]. Our study finding that malnutrition is associated with fair oral hygiene in the study population further strengthen our hypothesis. The Arantes et al. [64] suggested a more comprehensive assessment of dietary risks related to caries beyond that addressing sugar intake alone. We feel that our study finding – the absence of a relationship between ECC and frequency of sugar consumption in an analysis model that included nutritional status – supports the suggestion of Arantes et al. [64]. We therefore postulate that our observed association between ECC and malnutrition may reflect a complex impact of the household dietary choices – consumption of oil, salt, fat, vegetable, carbohydrate, sugar and micronutrients – on nutritional status and ECC since malnutrition is not limited exclusively to a sugar-caries pathway. Future studies are needed to explore this.
This is a cross-sectional study and therefore liable to the limitations associated with that design such as our inability to establish that malnutrition is a cause of ECC or otherwise. Although we controlled for some confounders by using multivariable analysis techniques [65], we were unable to control for all possible confounders in the absence of suggestive data. An example is that seasonality reportedly affects access to food, with an impact on the prevalence of malnutrition [66]. Also possible confounding variables for ECC such as access to fluoride application, history of breast feeding and feeding at night were not collected in the primary study. The study data may also be limited in its generalizability to the Nigeria as the study was conducted in only one of the 774 local government areas in the country. The proportion of study participants with ECC was low leading to estimates with wide confidence intervals of some associations. Similarly, the low prevalence of poor oral hygiene may be the reason for the observed lower prevalence of ECC association with it. We addressed the issues of low ECC and poor oral hygiene prevalence using robust estimation of variance so that the observed associations are based on sound statistical techniques. Thus, our study findings provide new information on the relationship between ECC and malnutrition in a country where malnutrition is endemic [55]. These findings are important because they produce evidence that is difficult to obtain in other countries where malnutrition prevalence may be lower. The study findings raise a few questions that require further exploration to help improve our understanding of the relationship between ECC and malnutrition.
Conclusion
We found a significant association between the presence of ECC in children younger than 6 years and being stunted, underweight and overweight in a suburban population with low prevalence of ECC. We also found that there was no association between ECC and the frequency of sugar consumption when the nutritional status of children moderated the relationship. Further studies that examine diet and ECC comprehensively are required. Also, for this study population, further studies are required to help build a stronger predictive model for ECC.
Availability of data and materials
All study related data and materials are included in this publication. This study is a sub-study of a larger study the raw data of which is accessible on request.
Abbreviations
- APR:
-
Adjusted Prevalence Ratio
- BMI:
-
Body Mass Index
- dmft:
-
Decay, missing, filled teeth
- ECC:
-
Early Childhood Caries
- HAZ:
-
Height for Age Z score
- OHI-S:
-
Simplified Oral Hygiene Index
- PR:
-
Prevalence Ratio
- SD:
-
Standard Deviation
- WAZ:
-
Weight for Age Z score
- WHO:
-
World Health Organization
- WHZ:
-
Weight for Height Z score
References
AAPD. Policy on early childhood caries (ECC): classifications, consequences, and preventive strategies. Pediatr Dent. 2008; 30(7 Suppl): 40.
Schroth R, Jeal N, Kliewer E, et al. The relationship between vitamin D and severe early childhood caries: a pilot study. Int J Vitam Nutr Res. 2012;82:53–62.
Schroth RJ, Levi J, Kliewer E, et al. Association between iron status, iron deficiency anaemia, and severe early childhood caries: a case--control study. BMC Pediatr. 2013;13:22.
Schroth RJ, Levi JA, Sellers EA, et al. Vitamin D status of children with severe early childhood caries: a case-control study. BMC Pediatr. 2013;13:174.
Clarke M, Locker D, Berall G, et al. Malnourishment in a population of young children with severe early childhood caries. Pediatr Dent. 2006;28:254–9.
Sheller B, Churchill SS, Williams BJ, et al. Body mass index of children with severe early childhood caries. Pediatr Dent. 2009;31:216–21.
Lima GQT, Brondani MA, da Silva AAM, et al. Serum levels of proinflammatory cytokines are high in early childhood caries. Cytokine. 2018;111:490–5.
Ribeiro CCC, Pachêco CDJB, Costa EL, et al. Proinflammatory cytokines in early childhood caries: salivary analysis in the mother/children pair. Cytokine. 2018;107:113–7.
Cregger RA, Langworthy KL, Salako NO, et al. Relationship between salivary cytokines, and caries experience in children with different body mass indices. Journal of Dental and Oral Health. 2017;3(5):075.
Matczuk J, Zalewska A, Łukaszuk B, et al. Insulin resistance and obesity affect lipid profile in the salivary glands. J Diabetes Res. 2016;8163474.
Chukwumah N, Azodo C, Adeghe H, et al. Relating dental caries experience with body mass index among Nigerian primary school children: a cross-sectional survey. Journal of Education and Ethics in Dentistry. 2012;2(1):28–32.
Bhoomika W, Ramakrishna Y, Munshi AK. Relationship between severe early childhood caries and body mass index. J Clin Pediatr Dent. 2013;37(3):235–42.
Davidson K, Schroth RJ, Levi JA, et al. Higher body mass index associated with severe early childhood caries. BMC Pediatr. 2016;16(1):137.
Janakiram C, Antony B, Joseph J. Association of undernutrition and early childhood dental caries. Indian Pediatr. 2018;55(8):683–5.
Zaror SC, Sapunar ZJ, Muñoz NS, et al. Association between overweight and early childhood caries. Rev Chil Pediatr. 2014;85(4):455–61.
Ribeiro CCC, Silva MCBD, Nunes AMM, et al. Overweight, obese, underweight, and frequency of sugar consumption as risk indicators for early childhood caries in Brazilian preschool children. Int J Paediatr Dent. 2017;27(6):532–9.
Ahmed TES, Abuaffan A. Correlation between body mass index and dental caries among a sample of Sudanese children. Braz Dent Sci. 2015;18(3):42–51.
Hooley M, Skouteris H, Boganin C, et al. Body mass index and dental caries in children and adolescents: a systematic review of literature published 2004 to 2011. Syst Rev. 2012;1:57.
Xavier A, Bastos RDS, Arakawa AM, et al. Correlation between dental caries and nutritional status: preschool children in a Brazilian municipality. Revista de Odontologia. 2013;42(5):378–83.
Chen W, Chen P, Chen SC, et al. Lack of association between obesity and dental caries in three-year-old children. Zhonghua Min Guo Xiao Er Ke Yi Xue Hui Za Zhi. 1998;39(2):109–11.
Krishna HVNS, Manaswini E, Kumar VY, et al. Association between Nutritional Status and Early Childhood Caries in Indian Children. J Int Soc Prev Community Dent. 2017;7(3):131–5.
Dye BA, Shenkin JD, Ogden CL, et al. The relationship between healthful eating practices and dental caries in children aged 2-5 years in the United States, 1988-1994. J Am Dent Assoc. 2004;135:55–66.
Macek MD, Mitola DJ. Exploring the association between overweight and dental caries among US children. Pediatr Dent. 2006;28:375–80.
Hong L, Ahmed A, McCunniff M, et al. Obesity and dental caries in children aged 2-6 years in the United States: National Health and nutrition examination survey 1999-2002. J Public Health Dent. 2008;68L:227–33.
Alvarez JO, Caceda J, Woolley TW, et al. A longitudinal study of dental caries in the primary teeth of children who suffered from infant malnutrition. J Dent Res. 1993;72(12):1573–6.
Shen A, Bernabe E, Sabbah W. The bidirectional relationship between weight, height and dental caries among preschool children in China. PLoS One. 2019;14(4):e0216227.
Lifshitz F, Casavalle PL, Bordoni N, et al. Oral health in children with obesity or diabetes mellitus. Pediatr Endocrinol Rev. 2016;14(2):159–67.
Werner H, Katz J. The emerging role of the insulin-like growth factors in oral biology. J Dent Res. 2004;83(11):832–6.
Dülger H, Arik M, Sekeroğlu MR, Tarakçioğlu M, Noyan T, Cesur Y, Balahoroğlu R. Pro-inflammatory cytokines in Turkish children with protein-energy malnutrition. Mediat Inflamm. 2002;11(6):363–5.
Zehnder M, Delaleu N, Du Y, Bickel M. Cytokine gene expression--part of host defence in pulpitis. Cytokine. 2003;22(3–4):84–8.
Santetti D, de Albuquerque Wilasco MI, Dornelles CT, Werlang IC, Fontella FU, Kieling CO, et al. Serum proinflammatory cytokines and nutritional status in pediatric chronic liver disease. World J Gastroenterol. 2015;21(29):8927–34.
Mehta NM, Corkins MR, Lyman B, Malone A, Goday PS, Carney LN, et al. Defining pediatric malnutrition: a paradigm shift toward etiology-related definitions. American Society for Parenteral and Enteral Nutrition Board of directors. JPEN J Parenter Enteral Nutr. 2013;37(4):460–81.
Zoico E, Roubenoff R. The role of cytokines in regulating protein metabolism and muscle function. Nutr Rev. 2002;60(2):39–51.
Hashemi A, Bahrololoomi Z, Salarian S. Relationship between early childhood caries and anemia: a systematic review. Iran J Ped Hematol Oncol. 2018;8(2):126–38.
Sheetal A, Hiremath VK, Patil AG, et al. Malnutrition and its oral outcome - a review. J Clin Diagn Res. 2013;7(1):178–80.
Moynihan P, Petersen PE. Diet, nutrition and the prevention of dental diseases. Public Health Nutr. 2004;7(1A):201–26.
Chao F, You D, Pedersen J. National and regional under-5 mortality rate by economic status for low-income and middle-income countries: a systematic assessment. Lancet Glob Health. 2018;6(5):e535–47.
Adewemimo A, Kalter HD, Perin J, et al. Direct estimates of cause-specific mortality fractions and rates of under-five deaths in the northern and southern regions of Nigeria by verbal autopsy interview. PLoS One. 2017;12(5):e0178129.
Akanbiemu FA, Fatiregun AA, Adejugbagbe AM. Nutritional status of under-fives in rural and urban communities in southwest, Nigeria. World Academic Journal of Community Health and Epidemiology. 2016;2(4):64–73.
Denloye O, Popoola B, Ifesanya J. Association between dental caries and body mass index in 12–15 year old private school children in Ibadan. Nigeria Pediatr Dent J. 2016;26(1):28–33.
UNICEF Nigerian-The Children-Education. Available at: https://www.unicef.org/nigeria/education. Accessed: 22 February 2019.
Kolawole KA, Folayan MO, Agbaje HO, et al. Digit sucking habit and association with dental caries and oral hygiene status of children aged 6 months to 12 years resident in semi-urban Nigeria. PLoS One. 2016;11(2):e0148322.
Folayan MO, Kolawole KA, Oziegbe EO, et al. Prevalence, and early childhood caries risk indicators in preschool children in suburban Nigeria. BMC Oral Health. 2015;15:72.
Olusanya O. The importance of social class in voluntary fertility control in a developing country. West Afr J Med. 1985;4:205–12.
Folayan MO, Kolawole KA, Chukwumah NM, et al. Use of caries prevention tools and associated caries risk in a suburban population of children in Nigeria. European Archives of Pediatric Dentistry. 2016;17(3):187–93.
De Onis M, Onyango AW, Borghi E, et al. Comparison of the World Health Organization (WHO) child growth standards and the National Center for Health Statistics/WHO international growth reference: implications for child health programmes. Public Health Nutr. 2006;9(7):942–7.
World Health Organisation. Measuring a child’s growth. 2008. Available at: www.who.int/childgrowth/training/measuring_growth.pdf. Accessed: 14 June, 2015.
WHO. World Health Organisation Oral Health surveys: Basic Methods. Geneva. 1997.
Greene JC, Vermillion JR. The simplified Oral hygiene index. J Am Dent Assoc. 1964;68:7–13.
Greenland S, Mansournia MA, Altman DG. Sparse data bias: a problem hiding in plain sight. BMJ. 2016;352:i1981.
Lo W-H, Chen S-H. Robust estimation for sparse data. 2009. IEEE Xplore. Accessible at: https://ieeexplore.ieee.org/document/4761668/authors. Accessed: 11th May, 2019.
Onyejaka NK, Popoola BA, Folayan MO. Nigeria. In: Folayan MO (Ed). A compendium on oral health of children around the world: early childhood caries. Nova Science Publishers Inc. 400 Ser Avenue, Suite 1600, Hauppauge, NY, 11788. 2018; 291–302.
Munthali T, Jacobs C, Sitali L, et al. Mortality and morbidity patterns in under-five children with severe acute malnutrition (SAM) in Zambia: a five-year retrospective review of hospital-based records (2009-2013). Archives of Public Health. 2015;73(1):23.
Chung S. Body mass index and body composition scaling to height in children and adolescent. Ann Pediatr Endocrinol Metab. 2015;20(3):125–9.
Akombi BJ, Agho KE, Merom D, et al. Child malnutrition in sub-Saharan Africa: a meta-analysis of demographic and health surveys (2006-2016). PLoS One. 2017;12(5):e0177338.
Manji F, Fejerskov O. Dental caries in developing countries in relation to the appropriate use of fluoride. J Dent Res 1990; 69 (Spec No): 733–471.
Wassuna D, Opinya G, Masiga M, et al. The nutritional status of the children with severe- ECC comparison with the nutritional status of children without caries aged 3-5-years-old and with the caregiver’s demographics in a Kenyan hospital. Modern Approaches in Dentistry and Oral Health Care. 2018;2(1):123–30.
Kagasi EO. Nutritional status and prevalence of dental caries among children aged 3–5 years attending outpatients health Care at Gertrude’s Children’s Hospital in Nairobi, Kenya (2011–2012). Doctoral dissertation, Public Health, Jomo Kenyatta University of Agriculture Technology. 2015. Available at: http://hdl.handle.net/123456789/1923.
Cleaton JP. Nutritional status and dental caries in a large sample of 4-and 5-year-old south African children. South African Journal of Clinical Nutrition. 2000;90(6):631–5.
Ahmed HA, Taha SE, El-Dokky NA. General health status of Egyptian children with early childhood caries. Egyptian Dental Journal. 2016;60(2):1–5.
Psoter WJ, Reid BC, Katz RV. Malnutrition and dental caries: a review of the literature. Caries Res. 2005;39(6):441–7.
Onyejaka NK, Amobi EO. Risk factors of early childhood caries among children in Enugu, Nigeria. Brazilian Research in Pediatric Dentistry and Integrated Clinic. 2016;16(1):381–91.
Abiola AA, Eyitope OO, Sonny OJ, et al. Dental caries occurrence and associated oral hygiene practices among rural and urban Nigerian pre-school children. Journal of Dentistry and Oral Hygiene. 2009;1(5):64–70.
Arantes R, Welch JR, Tavares FG, et al. Human ecological and social determinants of dental caries among the Xavante indigenous people in Central Brazil. PLoS One. 2018;13(12):0208312.
West BT, Sakshaug JW, Aurelien GAS. How big of a problem is analytic error in secondary analysis of survey data? PLoS One. 2016;11(6):e0158120.
Osgood-Zimmerman A, Millear AI, Stubbs RW, et al. Mapping child growth failure in Africa between 2000 and 2015. Nature. 2018;555:41–7.
Acknowledgements
We acknowledge the study participants who gave their time for this study.
Funding
No funding was obtained for this study.
Author information
Authors and Affiliations
Contributions
The idea of the manuscript was conceived by EOO. The study was designed and data collection process managed by EOO, MOF, KAK. The data analysis was conducted by OA1 and MET. The first draft of the manuscript was developed by MOF, MO and OA2. All the authors made intellectual inputs to the development of and finalization of the manuscript. All authors agreed to the final version of the manuscript to its submission. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval for the study was obtained from the Health Research Ethics Committee of the Obafemi Awolowo University Teaching Hospitals’ Complex Ile-Ife (ERC/2013/07/14). Written informed consent was obtained from the parents or legal guardian of the study participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that Morenike Oluwatoyin Ukpong and Maha El Tantawi are Sectional and Associate editors with the BMC Oral Health respectively.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1.
Questionnaire for data collection for the primary study. This is the comprehensive study data collection instrument used to generate the data for this study. This study is a subset of a larger primary study that determined the association between caries and oral habits in children 12 years and below.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Folayan, M.O., Arije, O., El Tantawi, M. et al. Association between early childhood caries and malnutrition in a sub-urban population in Nigeria. BMC Pediatr 19, 433 (2019). https://doi.org/10.1186/s12887-019-1810-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-019-1810-2