
Abstract
Background
The paediatric Human Immunodeficiency Virus (HIV) epidemic still progresses because of operational challenges in implementing prevention of mother-to-child HIV transmission (PMCT) programs. We assessed the knowledge, attitudes and practices (KAP) of children’s caregivers regarding mother-to-child transmission (MTCT) of HIV, paediatric HIV infection, early infant diagnosis (EID), and paediatric antiretroviral treatment in Ouagadougou, Burkina Faso.
Methods
We undertook a qualitative survey in the four public hospitals managing HIV exposed or infected children, in Ouagadougou in 2011. A sociologist used a semi-structured questionnaire to interview caregivers of children less than 5 years old attending the paediatrics wards on their KAP. Study participants were divided into four groups as follows:
those who did not yet know their children’s HIV infection status, those who were waiting for their children’s HIV test results, those who were waiting for antiretroviral treatment, and those who were already on antiretroviral treatment.
Results
A total of 37 caregivers were interviewed. The mean age was 32.5 years, and 29 (78 %) were mothers. Twenty seven (73 %) caregivers had primary or higher level of education, and 15 (40 %) described their occupation as “housewife”. Overall, 36 (97 %) of caregivers knew that the main route of HIV transmission for infants was through MTCT and 14 (38 %) specified that it occurred during pregnancy or delivery. Five percent thought that MTCT of HIV occurred during conception. PMTCT interventions could help prevent infant HIV infection according to 32 (87 %) caregivers. Thirty five percent of caregivers stated EID as a prevention strategy. Fifty-four percent of the participants believed that replacement feeding option would prevent MTCT of HIV; 24 (65 %) stated that they would prefer medical practitioners seek caregivers’ consent before carrying out any HIV-test for their child, and that caregivers’ consent was not compulsory before antiretroviral treatment. All caregivers thought that it was necessary to treat HIV-infected children, although they did not know what interventions could be done.
Conclusions
This study highlighted the low level of caregivers’ knowledge on paediatric HIV prevention and care in Ouagadougou. Awareness programs targeting caregivers need to be strengthened in order to improve the uptake of HIV early infant diagnosis and care.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
An estimated 3.3 million of children under 15 years of age are currently living with Human Immunodeficiency Virus (HIV) worldwide, with the majority in sub-Saharan Africa [1]. The infant mortality among perinatally HIV-infected children is high and can reach 52 % at 2 years of age in the absence of antiretroviral treatment [2, 3]. In 2008, the World Health Organization (WHO) recommended the universal early antiretroviral treatment (ART) for all HIV-infected children less than 12 months of age, irrespective of clinical status or symptomatology, because early infant antiretroviral treatment has proved to be efficient in improving their survival [4]. This recommendation was extended to all children less than 24 months of age in 2010 [5]. However, only 34 % of eligible children for treatment were actually on ART at the end of 2012, compared with a 63 % adult coverage, and only 35 % of infants born to HIV-positive mothers had an early infant HIV diagnosis (EID) in their first 2 months of life [1]. This inequity in access to EID and ART in children is worst in West Africa, compared to East and Southern Africa [6].
To improve early access to paediatric antiretroviral therapy in resource-limited settings, it is crucial to implement public health strategies to promote the acceptability of HIV EID at the community level, targeting both health care professionals and children’s caregivers [7]. This is even truer in West Africa [8, 9].
Thus, it is crucial to understand caregivers’ knowledge and perception in order to understand the barriers to paediatric HIV prevention and treatment strategies. Caregivers’ knowledge regarding paediatric HIV care is important for children’s antiretroviral treatment adherence as reported elsewhere [10–14].
Burkina Faso is a West African developing country with a gross national income per capita of $1,500 in 2013 [15]. The overall schooling rate at primary school in 2009/2010 was estimated at 74.8 % [16]. The public health system was divided into three levels: the health districts, the regional hospitals, and the university hospitals. In addition, there were 398 private health care facilities operating in the country in 2012 [17]. The 2010 health and demographic survey reported a national HIV prevalence of 1.0 %, reaching 2.1 % (sample size 2018) in Ouagadougou [18].
The 2010 health demographic survey also revealed that 98.3 % of women (sample size 17, 087) and 98.1 % of men, aged from 15 to 49 years (sample size 6,500) were aware of Acquired Immunodeficiency Syndrome (AIDS) in the whole country. In Ouagadougou, the capital of the country, 99.4 % (sample size 2,240) of women and 99.8 % (sample size 977) men were aware of AIDS. The use of condom as a mean of HIV prevention was known in 78.0 % (sample size 17,087) of women and 90.1 % (sample size 6,500) of men, aged from 15 to 49 years in the country. Knowledge related to the limited sexual intercourses to a single HIV-uninfected partner as a mean of prevention of sexual transmission, was mentioned by 86.1 % of women and 91.6 % of men aged from 15 to 49 years [18]. According to a study conducted in 2009 in Bobo Dioulasso, only 27.3 % (82/300) of women were aware of HIV MTCT through breastfeeding [19].
In Ouagadougou, Burkina Faso, it has been reported that 71 % of HIV exposed children did not have access to EID in 2011 [20]. Several factors are associated with this big gap: poor health facilities, health workers’ and caregivers’ low level of knowledge, negative attitudes and bad practices. In 2014, few data were available on caregivers’ knowledge about EID and paediatric HIV care in Burkina Faso’s field conditions. Thus, the objective of our study was to assess the knowledge, attitudes, and practices of the parents/caregivers regarding mother-to-child-transmission (MTCT) of HIV infection, EID, paediatric HIV infection, and antiretroviral treatment for HIV-infected children in Ouagadougou in 2011.
Methods
Study setting
The present study was carried out in the only four public hospitals providing antiretroviral treatment to HIV-infected children in Ouagadougou. Two of them were university hospitals: Yalgado Ouédraogo (YO) university hospital and Charles De Gaulle (CDG) paediatric university hospital. YO was the country’s largest referral hospital and CDG the national referral paediatric hospital.
The two other study sites were district hospitals (Boulmiougou and Nongr-Massom) which also served as reference hospitals for their respective health districts. Some of the study sites characteristics are described in the Table 1.
Our study was part of a larger multidisciplinary (sociology, immunology, virology, pharmacokinetics, nutrition) research project aimed to improve EID and ART initiation with lopinavir/ritonavir before the age of 2 years among HIV-infected children, and to assess strategies for the simplification of ARV among children who had achieved virological suppression after 1 year of ART (the MONOD ANRS 12206 project).
Study design
We conducted a 2-week qualitative cross-sectional survey in January 2011 in Ouagadougou. Based on the 2010’s Ministry of health records, we selected the four public hospitals which provided paediatric HIV care in Ouagadougou in 2010 [20]. In order to represent all the stages of paediatric HIV cascade of care, we chose to have four groups of caregivers in our sample: caregivers’ children HIV status unknown, caregivers’ children HIV test result pending, caregivers’ children HIV infection confirmed but untreated with antiretroviral drugs, and caregivers’ HIV-infected children treated with ART. In the first place, caregivers were identified in the paediatric wards of the study sites, especially in the units where the HIV-infected children were treated. Then, the sociologist visited the symptomatic children (severe malnutrition for instance) seeking the children already screened for HIV but who were not yet on antiretroviral treatment. Lastly, she looked among the outpatient caregivers consulting in paediatric wards, for those whose children’s HIV infection status was unknown. This group of “unknown HIV infection status” represented the general population of children’s caregivers. In each unit visited, all caregivers with children less than 5 years old were contacted for enrolment in the study. Those who consented were face-to-face interviewed using a semi-structured questionnaire. To maintain confidentiality, each caregiver was interviewed in a room. The sociologist who carried out the interview had been trained and had experience in HIV/AIDS care. The interviews were done in French and in Mooré (a national language), languages in which the sociologist was fluent.
The answers were tape-recorded, further transcribed, and analysed both manually by the sociologist, and with Stata software for the quantitative data. The comparison between groups was carried out using Pearson chi2 or Fisher’s exact test if at least one expected frequency was < 5. The confidence interval was set at 95 % and the significance P-value < 0.05.
The questionnaire was designed to collect the caregivers’ knowledge, attitudes and practices about prevention of HIV infection, MTCT, EID, paediatric HIV infection, and antiretroviral treatment for HIV-infected children in Ouagadougou.
The study was implemented as a situational analysis of the ANRS 12206 MONOD trial (ClinicalTrial.gov registry n°NCT01127204) and approved by the Ethics committee for health research and the Health Ministry of Burkina Faso. All the interviewees gave their verbal clear consent.
Results
Overall, 47 caregivers of eligible children were enrolled in the study, of whom 37 (79 %) consented to be interviewed. The refusal proportion was 21 % (10/47). Among the caregivers who accepted the interview, the mean age was 32.5 years ± 7 years, 29 (78 %) were women, and 31 (84 %) lived with their partner. Among these 29 women, 28 were the mothers and the remaining one was an aunt. Fathers were 8 (22 %). Twenty-seven (73 %) had primary or higher education, and 15 (40 %) described their occupation as “housewife” (Table 2). Each caregiver interviewed belonged to one of the four groups of HIV paediatric care: caregivers whose HIV-infected child was on ART (n = 11), caregivers whose child was known to be HIV-infected but not yet on ART (n = 4), caregivers waiting for their child’s HIV test results (n = 5), and those just attending outpatient paediatric ward with an unknown HIV status child (n = 17), as described in Table 2.
Knowledge on prevention of mother to-child-transmission (PMTCT), EID, and treatment of HIV
Overall, 97 % of caregivers knew that the main transmission route for HIV-infected infants was through their mothers. Fourteen (38 %) specified that mother-to-child transmission occurred during pregnancy or delivery. For instance a mother stated: “if the mother ignores her own HIV infection status, or if she is aware of it and does not benefit from mother-to-child HIV prevention treatment, she can infect her foetus during pregnancy”. Another caregiver said: “during delivery if the delivery table and the materials used on an HIV-infected woman is not well cleaned”. Some of them declared: “during delivery if there are wounds” or “a child can be infected when the umbilical cord is cut”. Five percent of caregivers thought that infant HIV transmission can occur during sexual intercourses, at the time of conception. For instance, a caregiver said that “an infant can get the disease through sexual intercourse (at conception) if the parents are HIV-infected”.
To the question about how can we prevent children’s HIV infection, 87 % of the caregivers responded that testing mothers and providing antiretroviral drugs to the HIV-infected ones (PMTCT interventions) can help prevent children’s HIV infection. A caregiver mentioned: “to protect infants from the disease, when a woman is pregnant, she must attend a health centre for HIV testing, and if she is infected, she should be given some drugs to prevent her infant from being infected”. Twenty (54 %) were aware that breast milk substitutes could prevent HIV transmission.
For EID, 32 (86 %) had a general knowledge on diagnostic method using blood sample, among them those attending paediatric ward with an unknown HIV status child were the most represented (Table 2). However, 6 (16 %) of caregivers felt that the EID was not necessary if the child was not symptomatic; 24 (65 %) stated that health workers should obtain caregivers’ consent before carrying out any HIV-test. “Concerning infant HIV diagnostic, health worker should not seek caregivers’ consent, but they can inform them” said another caregiver. Infant HIV diagnosis should be motivated by the child’s recurrent illnesses, for 10 (27 %) caregivers, of whom 4 were fathers and 6 mothers. “I have not performed HIV test for my child yet, because he is healthy, he is not frequently sick”, said one parent.
As for antiretroviral treatment, 24 (65 %) thought that caregivers’ consent is not compulsory before treating an HIV-infected child with antiretroviral drugs. “A caregiver stated that “doctors must not seek caregivers’ consent, because they are the ones who know what is good for the child”. The caregivers’ knowledge perception of consent is summarised in Table 3.
Finally, for HIV infection management, all caregivers thought that it was necessary to treat HIV-infected children, although they did not know what type of interventions should be done. A caregiver said: “it is important to treat HIV-infected children because it makes them healthier. See, my daughter has regained health and she is playing”.
PMTCT interventions included EID for only 13 (35 %) caregivers.
There was no statistical significant difference between groups of caregiver’s whose children were already HIV tested (groups 1 + 2 + 3) and those coming for outpatient consultation (group 4) regarding knowledge and attitudes (Table 3).
Practice of children’s HIV testing
Among the twenty participants (51.1 %) who carried out the HIV test of their children, 17 (45.9 %) revealed that the major reason underlying their decision was the frequent illnesses of their children. For those who tested their children because of illness symptoms, two mentioned additional reasons for testing: PMTCT intervention and the death of the child’s mother. Furthermore two (5.4 %) caregivers admitted that they tested their children because of the positive HIV status of the parents. One (2.7 %) caregiver did not specify his motivation for carrying out the HIV test.
One mother revealed that her child was tested without her consent.
Among the 17 (48.9 %) caregivers who had not tested their children, six (16.6 %) justified their attitude by the mother’s negative test result after the prenatal HIV testing. The other reasons for not testing the children were: healthy appearance (2.7 %) of the child and unawareness of the possibility of carrying out the test of the child without a medical prescription (2.7 %). In addition, one (2.7 %) caregiver said: “my child is three years old, he is still young and he can do his HIV test later”. The eight (21.6 %) remaining caregivers who had not tested their children provided no explanation.
Discussion
This survey gave an insight of caregivers’ knowledge and attitude about PMTCT, paediatric HIV infection diagnostic, existing prevention and HIV treatment strategies for children in Ouagadougou in 2011. Firstly, this study showed that despite an overall knowledge of MTCT modes, a few misconceptions still existed. Secondly, we highlighted the low level of knowledge among caregivers about the importance of performing EID even in asymptomatic HIV-exposed children allowing an earlier access to ART. Our results are useful to understand the barriers of EID uptake and paediatric HIV care in West-African children.
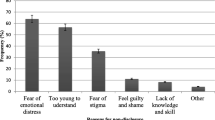
A total of 21 % of caregivers refused to participate in this survey, highlighting the possible lack of confidentiality and fear of stigma already mentioned in a similar context [21]. This lack of confidentiality may have also influenced the information collected among the responders, mainly in minimizing their difficulties facing the health care system or the health care workers.
Nevertheless, we were able to understand to some extent, caregivers’ knowledge, attitudes and practices at the different stages of paediatric HIV care cascade.
Our results showed that caregivers were globally aware of the HIV infection disease. We assume that this is the result of HIV prevention campaigns at community level in Burkina Faso since the early years when first cases of HIV infection were reported [22, 23].
Similarly, knowledge about PMTCT and EID using blood samples method was appreciable among caregivers, and there was no statistically significant difference between the groups when it comes to the method used to test their children. This result could be related either to a lack of statistical power, or to an absence of difference in terms of knowledge attitude and practices. However, as we expected a difference in knowledge about PMTCT and EID method in favour of those who were already in contact with HIV health care providers (groups 1 + 2 + 3), because of their frequent interactions with health staff, we could raise the hypothesis that health visits were not efficiently utilized to raise their awareness. So, health care providers should take advantage of the medical visits to cope with these issues.
But, the lack of difference in terms of knowledge of the group 4 versus the groups 1 + 2 + 3 can also be related to the level of education: the level of education amongst group 4 is greatly elevated and could account for any of the differences seen between the two groups.
In addition, caregivers misunderstanding and low level of knowledge about EID in asymptomatic children still remained. This could impede the routine EID coverage, and ultimately delay the ART treatment. This could partially explain the EID bottleneck in the 2011 cascade of care in Ouagadougou, with only 29 % of HIV-exposed children testing within their fist year of life [21]. Improving the coverage of the paediatric HIV care cascade at each stage requires addressing these misunderstandings through awareness campaigns. For instance in South Africa, a study showed that EID rate can be improved by using some strategies including awareness campaigns [24].
Some caregivers were reluctant to the practice of an EID without their consent, highlighting the fear of a possible stigmatization or mistrust of health workers’ practices. Conversely, they did not perceive the importance of consent prior to the infant antiretroviral treatment, whereas this formal consent would increase caregivers’ adherence to their infant ARV treatment [11, 14].
It is interesting to notice that all of the caregivers thought that early antiretroviral treatment was necessary for all HIV-infected infants, and this would decrease the mortality and morbidity rate if the service was accessible to the population. This could explain why we recorded a small proportion of refusal among caregivers referred for their infant HIV treatment initiation in the recruitment phase of the MONOD trial, implemented in Ouagadougou. The results of this trial will be presented elsewhere.
Some issues related to staff practices, such as carrying out the HIV test without caregivers’ prior consent, may be addressed by improving training in paediatric wards, as it has already been reported in Côte d’Ivoire [9] and South Africa [25]. However, changing caregivers’ attitudes may require interventions to raise their awareness at both individual and community level.
As for healthcare providers, they should actively promote HIV testing and care-seeking for children, by seizing all opportunities with caregivers.
Before concluding, we could discuss a few study limits. Although, our sample size was limited, the sampling method was adapted to qualitatively understand some perceptions, at the different steps of the cascade of paediatric HIV care from access to PMTCT services, EID services, and child care in Ouagadougou.
In addition, considering a group of “caregivers of HIV exposed but confirmed uninfected children” could have enriched the understanding of KAP in Ouagadougou, but it was not feasible in the cross-sectional design at the time of attendance in paediatric care.
Conclusions
In conclusion, although awareness of paediatric HIV infection among caregivers is significant in Ouagadougou, some misconceptions related to the moment of transmission and the importance of performing routine EID in all HIV-exposed children, still persist. These issues must be addressed by strengthening awareness campaigns and promoting best practices among medical staff. Therefore, changing caregivers’ attitudes may require interventions at both individual and community level. Healthcare providers should actively promote HIV testing and care-seeking for children in order to improve the uptake of EID among HIV-exposed children in Burkina Faso.
Abbreviations
- AIDS:
-
acquired immunodeficiency syndrome
- ANRS:
-
Agence Nationale de Recherche pour le SIDA et les hépatites virales (French National Agency for AIDS and viral hepatitis)
- ART:
-
antiretroviral treatment
- CRP-Santé:
-
centre de recherche publique pour la Santé (Public Research Centre for Health)
- EDCTP:
-
European and developing countries clinical trial partnership
- EID:
-
early infant diagnosis
- HIV:
-
human immunodeficiency virus
- KAP:
-
knowledge, attitudes and practices
- MTCT:
-
mother-to-child transmission
- PMTCT:
-
prevention of mother-to-child transmission
- Vs:
-
versus
- WHO:
-
world health organisation
References
UNAIDS: 2013 Global fact sheet. http://www.unaids.org/en/media/unaids/contentassets/documents/epidemiology/2013/gr2013/20130923_FactSheet_Global_en.pdf (2013). Accessed 14 Jan 2015.
Newell ML, Coovadia H, Cortina-Borja M, Rollins N, Gaillard P, Dabis F. Mortality of infected and uninfected infants born to HIV-infected mothers in Africa: a pooled analysis. Lancet. 2004;364:1236–43.
Newell ML, Brahmbhatt H, Ghys PD. Child mortality and HIV infection in Africa: a review. AIDS. 2004;18 Suppl 2:S27–34.
Violari A, Cotton MF, Gibb DM, Babiker AG, Steyn J, Madhi SA, Jean-Philippe P, 357 McIntyre JA. Early antiretroviral therapy and mortality among HIV-infected infants. N Engl J Med. 2008;359:2233–44.
WHO: Antiretroviral therapy for HIV infection in infants and children: Towards universal access. Recommendations for a public health approach - 2010 revision. http://www.who.int/hiv/pub/paediatric/infants2010/en/ (2010). Accessed 22 Apr 2014.
UNAIDS: Global report: UNAIDS report on the global AIDS epidemic 2013. “UNAIDS / JC2502/1/E”-. http://www.unaids.org/en/media/unaids/contentassets/documents/epidemiology/2013/gr2013/UNAIDS_Global_Report_2013_en.pdf (2013). Accessed 30 May 2014.
Ciaranello AL, Park JE, Ramirez-Avila L, Freedberg KA, Walensky RP, Leroy V. Early infant HIV-1 diagnosis programs in resource-limited settings: opportunities for improved outcomes and more cost-effective interventions. BMC Med. 2011;9:59.
Ndondoki C, Brou H, Timite-Konan M, Oga M, Amani-Bosse C, Menan H, Ekouevi D, 372 Leroy V. Universal HIV screening at postnatal points of care: which public health approach for early infant diagnosis in Cote d’Ivoire? PLoS One. 2013;8:e67996.
Oga MA, Ndondoki C, Brou H, Salmon A, Bosse-Amani C, Timite-Konan M, Leroy V. Attitudes and practices of health care workers toward routine HIV testing of infants in Cote d’Ivoire: the PEDI-TEST ANRS 12165 Project. J Acquir Immune Defic Syndr. 2011;57 Suppl 1:S16–21.
Mellins CA, Brackis-Cott E, Dolezal C, Abrams EJ. The role of psychosocial and family factors in adherence to antiretroviral treatment in human immunodeficiency virus-infected children. Pediatr Infect Dis J. 2004;23:1035–41.
Arrivé E, Anaki MF, Wemin ML, Diabate B, Rouet F, Salamon R, Msellati P. Assessment of adherence to highly active antiretroviral therapy in a cohort of African HIV-infected children in Abidjan, Cote d’Ivoire. J Acquir Immune Defic Syndr. 2005;40:498–500.
Muller AD, Bode S, Myer L, Stahl J, von Steinbuchel N. Predictors of adherence to antiretroviral treatment and therapeutic success among children in South Africa. AIDS Care. 2011;23:129–38.
Haberer J, Mellins C. Pediatric adherence to HIV antiretroviral therapy. Curr HIV/AIDS Rep. 2009;6:194–200.
Wrubel J, Moskowitz JT, Richards TA, Prakke H, Acree M, Folkman S. Pediatric adherence: perspectives of mothers of children with HIV. Soc Sci Med. 2005;61:2423–33.
WHO: Countries - Burkina Faso - Statistics. http://www.who.int/countries/bfa/en/ (2015). Accessed 03 Mar 2015.
Institut National de la Statistique et de la Démographie Burkina Faso: Tableau 05.34 : Evolution du taux brut de scolarisation de l’ensemble du secondaire (en %). Ouagadougou, Burkina Faso. http://www.insd.bf/n/contenu/tableaux/T0534.htm (2013). Access 27 May 2013.
Ministère de la Santé Burkina Faso: Annuaire statistique 2012. Ouagadougou, Burkina Faso. http://www.cns.bf/IMG/pdf/annuaire_ms_2012.pdf (2013). Accessed 30 Dec 2013.
Ministère de l’économie et des finances Burkina Faso: Enquête Démographique et de Santé et à indicateurs multiples (EDSBF-MICS IV) 2010 Ouagadougou, Burkina Faso. www.measuredhs.com/pubs/pdf/PR9/PR9.pdf (2011). Access 22 Apr 2013
Nacro B, Barro M, Gaudreault S, Dao B. Prevention of mother to child transmission of HIV in Burkina Faso: breastfeeding and wet nursing. J Trop Pediatr. 2010;56:183–6.
Ministère de la Santé du Burkina Faso. Annuaire statistique 2010. Ouagadougou, Burkina Faso; 2011. http://www.sante.gov.bf/phocadownload/Publications_statistiques/Annuaire/annuaire_statistique_sante_2010.pdf. Accessed 23 Apr 2013.
Coulibaly M, Meda N, Yonaba C, Ouedraogo S, Congo M, Barry M, Thio E, Siribie I, 415 Koueta F, Ye D, et al. Missed opportunities for early access to care of HIV-infected infants in Burkina Faso. PLoS One. 2014;9:e111240.
Bertrand JT, O’Reilly K, Denison J, Anhang R, Sweat M. Systematic review of the effectiveness of mass communication programs to change HIV/AIDS-related behaviors in developing countries. Health Educ Res. 2006;21:567–97.
Pulerwitz J, Michaelis A, Weiss E, Brown L, Mahendra V. Reducing HIV-related stigma: lessons learned from Horizons research and programs. Public Health Rep. 2010;125:272–81.
Bland RM, Ndirangu J, Newell ML. Maximising opportunities for increased antiretroviral treatment in children in an existing HIV programme in rural South Africa. BMJ. 2013;346:f550.
Yeap AD, Hamilton R, Charalambous S, Dwadwa T, Churchyard GJ, Geissler PW, Grant AD. Factors influencing uptake of HIV care and treatment among children in South Africa - a qualitative study of caregivers and clinic staff. AIDS Care. 2010;22:1101–7.
Ministère de la Santé Burkina Faso. Annuaire statistique 2011. Ouagadougou, Burkina Faso; 2012. http://www.insd.bf/n/contenu/pub_periodiques/annuaires_stat/Annuaires_stat_nationaux_BF/Annuaire_stat_2011.pdf. Accessed 27 May 2013.
Acknowledgements
The authors wish to acknowledge the families, the centre region director of health, the Ministry of Health division for HIV/AIDS, the heads of health districts in the centre region, and Kigocha Okengo for proof-reading the manuscript. We also thank the MONOD trial funders: the French National Agency for AIDS and viral hepatitis (ANRS), the European and Developing Countries Clinical Trials Partnership (EDCTP), the Luxembourg Public Research Centre for Health (CRP-Santé). Malik Coulibaly is a fellow PhD candidate funded by the MONOD consortium co-funders (see Additional file 1).
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
VL and NM conducted the overall study coordination. ET and MC conducted the study on the field. MC, DLD and ET performed the analysis and drafted the manuscript. LK, FK and DY supervised the study. SO, MG, AK and CY corrected the study protocol and the manuscript. All the authors reviewed, edited and approved the manuscript.
Additional file
Additional file 1:
Definition of the ANRS 12206 MONOD Collaboration Study Group. (DOC 31 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Coulibaly, M., Thio, E., Yonaba, C. et al. Prevention and care of paediatric HIV infection in Ouagadougou, Burkina Faso: knowledge, attitudes and practices of the caregivers. BMC Pediatr 16, 33 (2016). https://doi.org/10.1186/s12887-016-0569-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-016-0569-y