
Abstract
Aim
To evaluate association between pretreatment serum metrics and best corrected visual acuity ( BCVA) of patients with macular edema secondary to retinal vein occlusion and its subtypes after intravitreal ranibizumab or conbercept implant.
Methods
This prospective research included 201 patients(201 eyes) who were diagnosed with macular edema secondary to retinal vein occlusion at Heibei Eye Hospital between January 2020 and January 2021, who all received intravitreal anti- vascular endothelial growth factor treatment. Serum metrics were measured before the first treatment, and correlations between BCVA and each of four parameters— platelets, neutrophil- to- lymphocyte ratio(NLR), platelet- to- lymphocyte ratio(PLR) and monocyte- to- lymphocyte ratio(MLR)— were analyzed to identify predictors of effective intravitreal injection treatment outcomes.
Results
The mean platelets was significantly different in the effective and ineffective group for RVO-ME (273.02 ± 41.49 × 109/L,214.54 ± 44.08 × 109/L P < 0.01),BRVO-ME (269.43 ± 49.52 × 109/L,214.72 ± 40.42 × 109/L P < 0.01), and CRVO-ME (262.32 ± 32.41 × 109/L,209.27 ± 42 0.91 × 109/L P < 0.01). The cutoff value of the platelets was 266.500, the area under the curve was 0.857,and the sensitivity and specificity were 59.8% and 93.6%, respectively. The mean PLR was significantly different in the effective and ineffective group for RVO-ME (154.66 ± 49.60, 122.77± 44.63 P < 0.01),BRVO-ME (152.24 ± 54.99, 124.72 ± 41.46 P = 0.003), and CRVO-ME (152.06±44.23, 118.67 ± 41.80 P = 0.001). The cutoff value of the platelets was 126.734, the area under the curve was 0.699, and the sensitivity and specificity were 70.7% and 63.3%, respectively. There were no statistical differencies between the effective and ineffective group(RVO- ME and its subtypes) in NLR and MLR.
Conclusion
Higher pretreatment platelets and PLR were associated with BCVA in patients with RVO- ME and its subtypes who were treated with anti- VEGF drugs. The platelets and PLR may be used as predictive and prognostic tools for effective intravitreal injection treatment outcomes.
Similar content being viewed by others


Introduction
Retinal vein occlusion (RVO) is the second most common retinal vascular disorder after diabetic retinopathy. Retinal ischemia and hypoxia may be present due to RVO, and the increase of vascular permeability leads to sub-or intra-retinal exudation, which results in the appearance of macular edema (ME). ME is a severe complication that can cause dramatic vision loss [1]. The exact pathological mechanism of thrombosis remains unclear. Hypertension, diabetes, cardiovascular and cerebrovascular diseases, hyperlipidemia, pregnancy, oral contraceptives, hypercoagulable state, and hyperhomocysteinemia have been found to be high-risk factors for RVO [2]. Furthermore, local and systemic inflammation can induce vascular sclerosis and hypercoagulable state, which accelerate the formation of venous thrombosis.
Vascular endothelial growth factor (VEGF) is a cytokine that regulates vascular permeability and endothelial cell mitosis; the tight junctions between retinal vascular endothelial cells will be phosphorylated, and their content can be changed [3]. Anti-VEGF therapy can reduce the leakage and prevent the remodeling of blood vessels, thereby reducing ME. Compared to grid laser photocoagulation, anti-VEGF therapy is considered the first-line treatment for RVO-ME.
Rezar-Dreindl et al. proved that VEGF, IL-6, and IL-1 β are correlated with RVO-ME [4]. Moreover, several studies have shown that inflammatory factors play an important role in RVO-ME. The prognoses of malignant tumors and cardiovascular abnormal infectious diseases have been confirmed to be correlated with NLR, MLR, and PLR [5]; however, the correlations between NLR, MLR, and PLR and the efficiency of anti-VEGF for RVO-ME have rarely been reported. This study will focus on these correlations and whether they can be indicators for the prognosis of RVO-ME.
Subjects and methods
Participants
From January 2020 to January 2021, 201 patients (201 eyes) were diagnosed with RVO-ME using fundus fluorescein angiography (FFA) and optical coherence tomography (OCT). The inclusion criteria were as follows: the patients (1) underwent a complete examination, including best-corrected visual acuity (BCVA), intraocular pressure (IOP), slit-lamp biomicroscopy, and fundus pre-set lens; (2) had RVO diagnosed with FFA and ME diagnosed with OCT; (3) voluntarily participated in the trial, signed the informed consent form, and completed the treatment and follow-up; and (4) had IOP in the normal range (10–21 mmHg). The exclusion criteria comprised the following: (1) other treatments for RVO-ME during the follow-up period, such as retinal laser photocoagulation, intravitreal corticosteroids injection, and corticosteroids retrobulbar or peribulbar injection; (2) patients with other concomitant ocular diseases, such as uveitis, age-related macular degeneration, glaucoma, and diabetes retinopathy, and other severe refracting opacity–affected examinees; (3) the presence of diabetes mellitus, systemic inflammatory diseases, cardiovascular diseases, sepsis, and malignant tumors; (4) a history of routine anti-inflammatory and anticoagulant drugs or oral contraceptives; (5) a history of alcoholism and heavy smoking; (6) a history of intraocular surgery, vitreous hemorrhage, endophthalmitis, ocular trauma, or other laser treatments.
Methods
Two anti-VEGF drugs were used in this experiment: ranibizumab and conbercept. Everyone chose either of the anti-VEGF drugs on their own will randomly at the first treament for comparison, receiving intravitreal injections of 0.5 mg or 0.05 ml under aseptic conditions. The patients were divided into the efficient group and the inefficient group based on the BCVA results after treatment; those with better results were placed in the efficient group, and the others were placed in the inefficient group. The criteria for the efficient group was one line of improvement as minimal after treatment at least. If multiple injections of anti-VEGF drugs had been needed,the initial species was used for the following injections, only the results of the first treatment were analyzed. The patients returned for follow-ups 1 week postoperatively; they were then evaluated on a monthly basis and received injections as needed or pro re nata.
Blood samples were obtained from the antecubital vein before treatment at 6: 00 am. Leukocyte subtypes (neutrophils, lymphocytes, and monocytes) and platelets were measured using an Automated Blood Coagulation Analyzer (Sysmex XN-550, Japan). Afterward, the neutrophil-to-lymphocyte ratio (NLR), monocyte-to-lymphocyte ratio (MLR), and platelet-to-lymphocyte ratio (PLR) were calculated and recorded for all blood samples. The patients and their families signed informed consent forms, and this study was approved by the Medical Ethics Committee of Hebei Eye Hospital.
Statistical analysis
All statistical analyses were conducted using SPSS 23.0 (SPSS, Inc., Chicago, IL, USA). Quantitative data were presented as mean ± standard deviation (SD). The independent samples t-test was used to compare the two sets of parametric data of each group. The categorical variables were expressed as percentages, which were compared using chi-square tests. Spearman’ s correlation analysis was used to analyze the correlation between the parameters. The optimal cutoffpoints of NLR, PLR, and MLR were determined using receiver operator characteristic (ROC) curve analysis. The areas under the curve (AUC) were calculated to determine the accuracy of the tests. A p-value less than 0.05 was considered significant in all of the analyses.
Results
Total results
There were no differences in the gender, age, RVO subtypes, anti-VEGF drugs, baseline BCVA, IOP before and after treatment, or neutrophil, lymphocyte, and monocyte counts of the patients in the efficient and inefficient groups. The differences in the changes in BCVA between the efficient and inefficient groups were remarkable (0.26 ± 0.22 vs. 0.09 ± 0.09, P < 0.01), but no significant differences in IOP were observed between the efficient and inefficient groups (3.67 ± 0.63 vs. 3.10 ± 0.58, P > 0.05). The platelet levels in the efficient group were higher than those in the inefficient group (273.02 ± 41.49 vs. 214.54 ± 44.08, P < 0.01). The PLR values in the efficient group were significantly higher than those in the inefficient group (154.66 ± 49.60 vs.
122.77 ± 44.63, P < 0.05). There were no differences in the NLR and MLR between the efficient and inefficient groups (2.01 ± 0.87 vs. 2.08 ± 1.08, P > 0.05 and 0.21 ± 0.07 vs. 0.23 ± 0.09, P > 0.05, respectively). The total results are shown in Table 1.
The results of the BRVO and CRVO groups
There were no differences in the gender, age, anti-VEGF drugs, baseline BCVA, IOP before and after treatment, or neutrophil, lymphocyte, and monocyte counts of the patients in the BRVO and CRVO groups. For BRVO, the platelet levels and PLR values in the efficient group were higher than those in the inefficient group (269.43 ± 49.52 vs. 214.72 ± 40.42, P < 0.01 and 152.24 ± 54.99 vs. 124.72 ± 41.46, P = 0.003, respectively). However, there were no statical differences in NLR or MLR between the efficient and inefficient groups (2.00 ± 0.78 vs. 1.98 ± 0.90, P > 0.05 and 0.21 ± 0.07 vs. 0.23 ± 0.07, P > 0.05). For CRVO, the platelet levels and PLR values in the efficient group were higher than those in the inefficient group (262.32 ± 32.41 vs. 209.27 ± 42.91, P < 0 0.01 and 152.06 ± 44.23 vs. 118.67 ± 41.80, P = 0.001, respectively); however, there were no statical differences in NLR or MLR between the efficient and inefficient groups (2.00 ± 0.98 vs. 2.18 ± 1.17, P > 0.05 and 0.21 ± 0.08 vs. 0.24 ± 0.11, P > 0.05, respectively). The results of the BRVO and CRVO groups are shown in Tables 2 and 3 respectively.
Ranibizumab and conbercept in the efficient groups of RVO and its subtypes
There were no differences in the NLR, MLR, PLR, or platelet levels of the two drugs in the efficient groups of RVO and its subtypes. The results are shown in Table 4.
ROC curve
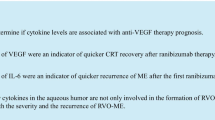
Platelets, PLR, and NLR were analyzed using the ROC curve. The optimal cutoff value of platelets was 266.500, with 59.8% sensitivity and 93.6% specificity (AUC: 0.857; 95% confidence interval [CI]: 0.807–0.908). The optimal cutoff value of PLR was 126.734, with 70.7% sensitivity and 63.3% specificity (AUC: 0.699; 95% CI: 0.627–0.772). The optimal cutoff value of NLR was 1.651, with 56.5% sensitivity and 36.7% specificity (AUC: 0.497; 95% CI: 0.417–0.577). The results are shown in Table 5; Fig. 1.

The ROC curve of platelets, NLR, and PLR
Discussion
The correlations between the BCVA of RVO-ME after anti-VEGF therapies and platelets, PLR, NLR, and MLR have been presented in this study. The differences in the platelets and PLR of RVO and its subtypes between the efficient and inefficient groups were prominent after treatment; however, the outcomes of MLR and NLR were converse. Compared to NLR and MLR, platelets and PLR exhibited higher sensitivity and specificity. Hence, platelets and PLR can be used as an index to evaluate the prognosis of RVO-ME. However, this is not completely consistent with Rao’s conclusion [6].
Ray et al. showed that the inflammatory action mediated by leukocytes and its subtypes is closely related to the occurrence and development of tumors, as well as cardiovascular and cerebrovascular diseases [7, 8]; furthermore, the incidence rate and mortality of coronary heart disease are directly proportional to the level of neutrophils, and low-level lymphocytes are high-risk factors for coronary vascular disease [9]. NLR has been widely used to evaluate the incidence rate and prognosis of systemic inflammatory diseases [10]. It was confirmed that NLR in patients with RVO-ME was significantly higher compared to the control group byAhin [11], Ayhan [12] and Emrullah [13]. It was speculated that NLR could be used as a predictor of the occurrence and development of RVO-ME. However, in the studies of Antonio [14] and Esra [15], there was no significant difference in NLR between the RVO-ME group and the control group.
Platelets can regulate inflammatory reaction and the release of VEGF by interacting with neutrophils and vascular endothelial cells [16]. Activated neutrophils can release a variety of cytokines, including VEGF, which may damage the blood retinal barrier, increase the permeability of the vascular wall, and aggravate ME [6]. Therefore, platelets can indirectly lead to the occurrence of ME. Meanwhile, the increase of platelets is an important factor in the formation and development of retinal vein thrombosis [14]. Bian [17] confirmed that the platelet levels in the RVO group was significantly higher than those in the control group.
There was a positive correlation between platelet level, PLR, and VEGF level in the RVO-ME group at baseline [18]. From our research, it can be concluded that the BCVA outcome of the patients who underwent anti-VEGF treatment was significantly correlated with the platelet level and PLR at baseline. Thus, platelets and PLR can be used as independent predictors of the prognosis. However, there was no significant difference in MLR between the effective and ineffective groups. The number of lymphocytes and monocytes will decrease under the condition of increased systemic pressure and sub-health, which can be seen as a response to stress, but neither of these can regulate the release of VEGF [9]. Thus, MLR cannot be used as an independent predictor of the prognosis. However, Li [19] had arrived at a different conclusion, finding that MLR was significantly higher in the efficient group than in the inefficient group. This will be demonstrated in subsequent research.
Two anti-VEGF drugs were used in this study. Ranibizumab is a human anti-VEGF monoclonal antibody that can be used in combination with all VEGF-A active isomers. Conbercept is a humanized, soluble VEGF receptor (VEGFR) protein comprising extra-cellular domain-2 of VEGFR-1 and extra-cellular domain-3 and − 4 of VEGFR-2; all these domains are connected via the Fc region of human immunoglobulin G [20, 21]. These two anti-VEGF drugs can reduce the permeability of the vascular wall, promote the absorption of intraretinal and subretinal fluids, and improve the density of superficial and deep capillaries of the retina of posterior especially in macular.Furthermore, the function of the photoreceptor cells and ganglion cells of the macular will be further improved.
There were no significant differences regarding platelets, PLR, NLR, and MLR in the RVO group and its subtypes, and no significant differences were observed in the outcomes of the conbercept and ranibizumab groups.
This study has some limitations. First, recent occurrences of acute coronary artery disease and stroke, which will affect neutrophils, lymphocytes, and platelets, were not taken into account. Second, BCVA was the only index used as a predictor of the effectiveness of the treatment, and the changes in central macular thickness were not considered. Third, the interactions of other serum inflammatory factors, such as C-reactive protein, interleukin, and the tumor necrosis factor family, with platelets, neutrophils, and lymphocytes were not studied.
Conclusion
In general, compared with other indexes (such as MPV, PCT, and PDW), PLR and platelets are cheap and convenient indexes for predicting the prognosis of the anti-VEGF treatment of RVO-ME. The role of NLR should be further demonstrated in the follow-up study.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BRVO:
-
Branch retinal vein occlusion
- CRVO:
-
Central retinal vein occlusion
- BCVA:
-
Best-corrected visual acuity
- IOP:
-
Intraocular pressure
- NLR:
-
Neutrophil-to-lymphocyte ratio
- MLR:
-
Monocyte-to-lymphocyte ratio
- PLR:
-
Platelet-to-lymphocyte ratio
- ROC:
-
Receiver operating characteristic AUC:Area under curve
- AUC:
-
Area under curve
- CI:
-
Confidence level
References
Rogers S, McIntosh RL, Cheung N et al. The Prevalence of Retinal Vein Occlusion: Pooled Data from Population Studies from the United States, Europe, Asia, and Australia.Ophthalmology,2010, 117(2):313–319.
Zhao F, Du F, Shi D et al. Mapping research trends of retinal vein occlusion from 2009 to 2018: a bibliometric analysis.PeerJ,2019,7(3).
Vinores SA, Derevjanik NL, Ozaki H et al. Cellular mechanisms of blood-retinal barrier dysfunction in macular edema.Doc Ophthalmol, 1999,7(3–4):217–228.
Rezar-Dreindl S, Eibenberger K, Pollreisz A et al. Effect of intravitreal dexamethasone implant on intraocular cytokines and chemokines in eyes with branch and central retinal vein occlusion.Acta Ophthalmol,2017,95(2):e119-e127.
Bakirci EM, Topcu S, Kalkan K, et al. The role of the nonspecific inflammatory markers in determining the anatomic extent of venous thromboembolism. Clin Appl Thromb Hemost. 2013;21(2):181–5.
Rao J, Wu N, Qu X et al. The role of serum inammation-based factors in Anti-VEGF treatment for macular edema secondary to retinal vein occlusion and its subtypes.Ophthalmic Research,2020,64(2).
Ray-Coquard I, Cropet C, Glabbeke MV, et al. Lymphopenia as a prognostic factor for overall survival in Advanced Carcinomas, Sarcomas, and Lymphomas. Cancer Res. 2009;69(13):5383–91.
Unal S, Yayla, et al. White blood cell subtypes and ratios in cardiovascular disease. Volume 68. Angiology; 2017. p. 651. 7.
Seropian IM, Romeo FJ, Pizarro R et al. Neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio as predictors of survival after heart transplantation. ESC Heart Fail. 2018;5(1):149–156.
Gonzalez-Fajardo JA, Brizuela-Sanz JA, Aguirre-Gervas B, Prognostic significance of an elevated neutrophil-lymphocyte ratio in the amputation-free survival of patients with chronic critical limb ischemia. Annals of vascular surgery,2014, 28(4):999–1004.
.Ahin M, Elbey B, Ahin A et al. Neutrophil -to ‐ lymphocyte ratio and platelet ‐ to ‐ lymphocyte ratio in retinal vein occlusion.Clinical& experimental optometry,2020, 103(4):490–494.
Ayhan D, Sultan O, Hasan Y, et al. Association of neutrophil/lymphocyte ratio and retinal vein occlusion. Eur J Ophthalmol. 2015;25(4):343–6.
Emrullah B, Mehmet I, Mert Ş et al. Branch retinal vein occlusion associated with platelet activation.Turkish journal of medical sciences,2019,49(1):283–287.
Antonio P, Tiziana P, Jacopo M, et al. Mean Platelet Volume, Red Cell Distribution Width, and Complete Blood Cell Count Indices in Retinal Vein Occlusions. Ophthalmic Epidemiol, 2021, 28(1):39–47.
Esra TK, Nursal MY, Nimet YE, et al. Neutrophil/lymphocyte ratio and mean platelet volume in branch retinal vein occlusion.Saudi Journal of Ophthalmology, 2016, 30(2):105–108.
Fu H, Qin B, Hu Z et al. Neutrophil-and platelet-to-lymphocyte ratios are correlated with disease activity in rheumatoid arthritis.Clinical Laboratory,2015, 61(3–4):269–273.
Bian C, Wu Y, Shi Y, et al. Predictive value of the relative lymphocyte count in coronary heart disease. Heart Vessels. 2010;25(6):469–73.
Kurtul A, Yarlioglues M, Murat SN, et al. Usefulness of the platelet-to-lymphocyte ratio in predicting angiographic reflow after primary percutaneous coronary intervention in patients with acute ST-segment elevation myocardial infarction. Am J Cardiol. 2014;114(3):342–7.
Li F, Sun M, Guo J et al. Comparison of Conbercept with Ranibizumab for the Treatment of Macular Edema Secondary to Branch Retinal Vein Occlusion. Curr Eye Res. 2017; 42(8):1174–1178.
Avery RL, Castellarin AA, Steinle NC, et al. Systemic pharmacokinetics and pharmacodynamics of intravitreal aflibercept, bevacizumab, and ranibizumab. Retina. 2017;37(10):1847–1858.
Zhang M, Zhang J, Yan M, et al. A phase 1 study of KH902, a vascular endothelial growth factor receptor decoy, for exudative age-related Macular Degeneration. Ophthalmology. 2011;118(4):672.
Acknowledgements
Not applicable.
Funding
This study was supported by Grants from National Natural Science Foundation of China (MW:81700873,FZ:81570877) and Hebei Province Science and Technology Support Program (MW:18277754D).
Author information
Authors and Affiliations
Contributions
Yun-Chang Wang conceived and designed the experiments, Rong-Rong Li wrote the manuscript, Meng-Meng Wang and Yi Cai perform the data analyses, Chuan-Qi Zhoucollect data and information, Li-Fei Yuan and Yi-Qing He helped perform the analysis and follow up patients. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Heibei Eye Hospital and was performed in adherence to the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants.
Consent for publication
Written informed consent was obtained from the patients for publication of the clinical details and clinical images used in this work.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, YC., Zhou, CQ., Li, RR. et al. The role of serum metrics in anti- VEGF treatment for macular edema induced by retinal vein occlusion. BMC Ophthalmol 23, 173 (2023). https://doi.org/10.1186/s12886-023-02921-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12886-023-02921-5