
Abstract
Purpose
We investigated the association between albuminuria and hypertensive retinopathy (HR) in hypertensive adults.
Methods
This was a cross-sectional subgroup analysis of data from the China Stroke Primary Prevention Trial. We enrolled 2,964 hypertensive adults in this study. Keith-Wagener-Barker stages was used to assess HR. The urinary albumin to creatinine ratio (UACR) was calculated to evaluate albuminuria.
Results
HR was found in 76.6% (n = 2, 271) of the participants, albuminuria was found in 11.1% (n = 330). The UACR levels were significantly higher in subjects with HR than in those without HR (grade 1, β = 1.42, 95% confidence intervals [CI]: -0.12, 2.95, p = 0.070; grade 2, β = 2.62, 95% CI: 0.56, 4.67, p = 0.013; grade 3, β = 5.17, 95% CI: 1.13, 9.20, p = 0.012). In the subgroup analyses, the association between HR and UACR was stronger in current smokers (p for interaction = 0.014). The correlation between HR grades 1 and 2 and UACR was stronger in subjects with higher triglyceride levels (≥ 1.7 mmol/L), but for grade 3 HR, this correlation was stronger in subjects with lower triglycerides levels (< 1.7 mmol/L, p for interaction = 0.023). The odds of albuminuria were significantly higher in subjects with HR than in those without HR (grade 1, odds ratio [OR] = 1.57, 95% CI: 1.08, 2.29, p = 0.019; grade 2, OR = 2.02, 95% CI: 1.28, 3.18, p = 0.002; grade 3, OR = 2.12, 95% CI: 0.99, 4.55, p = 0.053). In the subgroup analyses, the association between HR grades 1 and 2 and albuminuria was stronger in subjects with higher triglycerides levels (≥ 1.7 mmol/L), but for grade 3 HR, this correlation was stronger in subjects with lower triglyceride levels (< 1.7 mmol/L, p for interaction = 0.014).
Conclusion
HR was positively correlated with albuminuria in hypertensive Chinese adults. This correlation was more remarkable when the population was stratified by triglycerides levels and smoking status. HR can be used as an indicator of early renal injury.
Similar content being viewed by others


Introduction
Approximately one-third of people in China suffer from hypertension [1]. Chronic kidney disease (CKD), which is both a cause and complication of hypertension, affects approximately 119.5 million people in China and has become a serious public health concern [2].
Dipstick proteinuria tests are a common and inexpensive method for screening renal diseases, but they are not sufficiently precise [3]. A total of 10.5% of dipstick proteinuria‑negative subjects still have renal injury [4]. Albuminuria is a biomarker of early kidney injury. It is not only a risk factor for end-stage renal disease, progressive CKD and acute kidney injury [5] but also an independent predictive factor for cardiovascular and all-cause mortality [3]. According to an epidemiological study, more people in rural China than urban China have albuminuria [2]. However, laboratory tests for albuminuria are not widely used in rural China and some developing countries due to their high cost.
Retinal blood vessels are similar in anatomy and physiology to vessels in other end organs. Retinal microvascular abnormalities (RMAs), especially vasoconstriction, stenosis and enhanced arterial reflex, are considered the main pathological features of hypertension and are closely related to the left ventricular failure, stroke, nephropathy, and cardiovascular disease observed in hypertensive patients [6]. Retinal blood vessels can be observed directly through a fundus examination, which represents a noninvasive and convenient method for assessing end-organ damage.
The relationship between RMA and albuminuria has been reported in previous studies, but their results are controversial. For example, Bao et al. found that a lower retinal arteriovenous ratio was associated with higher albuminuria [7], but no positive association was found between these parameters in Masaidi’s study [8]. Previous studies were mainly carried out in Europe and America. However, in the Chinese population, especially in rural areas, the correlation between RMA and albuminuria has not been fully clarified, and this group is very different from European and American people in terms of diet structure, lifestyle and economic conditions. In addition, previous studies have not evaluated in detail the possible effect modifiers.
The purpose of this study was to assess the correlation between albuminuria and hypertensive retinopathy (HR) in hypertensive adults in rural China. These data may provide a theoretical basis for the use of fundus examination to screen for early renal injury in hypertensive subjects.
Material and methods
Study design and population
This is a cross-sectional study. Data used in this analysis were obtained from the China Stroke Primary Prevention Trial, a multicenter, double-blind and randomized clinical study performed in rural China. The purpose of the China Stroke Primary Prevention Trial was to compare the efficacy of folic acid combined with enalapril and enalapril alone in preventing stroke in Chinese hypertensive adults [9]. The study was carried out in 32 communities in Anhui and Jiangsu Provinces beginning in May 2008, and subjects were followed up for 5 years. We conducted a cross-sectional analysis of data obtained from the last follow-up in 2013. A total of 3,860 adults with primary hypertension aged between 45 and 75 years old who had laboratory tests for albuminuria were included in the study. Among these individuals, 3,121 underwent fundus photography. The procedures of the study were in accordance with the Helsinki Declaration. The Ethics Committee of the Institute of Biomedicine at Anhui Medical University approved all procedures used in the study. All participants provided informed consent before the study began. The study was registered at http://clinicaltrials.gov/, NCT number: NCT00794885.
Data collection
Demographic data
The general information related to the participants was collected through a questionnaire. Past history of illness, current medication use, smoking and drinking habits were recorded in detail. Smoking and drinking habits were each categorized into 3 levels: current smoking or drinking, former smoking or drinking and never smoking or drinking. Smoking at least 1 cigarette per day for 6 months was defined as current smoking. Drinking at least once a week for 6 months was defined as current drinking. The blood pressure of all participants was measured in the sitting position after at least 10 min of rest. The measurements were made 3 times at two-minute intervals, and the results were averaged. Hypertension was defined as systolic blood pressure (SBP) ≥ 140 mmHg, diastolic blood pressure (DBP) ≥ 90 mmHg, or the use of antihypertensive drugs [9], and diabetes mellitus was defined as having a history of diabetes, using antidiabetic medications, or fasting blood glucose (FBG) ≥ 7.0 mmol/L in laboratory tests. Body height and body weight were measured, and body mass index (BMI) was calculated by dividing weight (kg) by height2 (m2).
Laboratory tests
All participants provided spot urine samples, and fasting venous blood was drawn. The samples were tested in the laboratory of the National Clinical Research Center for Kidney Disease, Nanfang Hospital, Guangzhou, China. The test methods were as follows. Triglyceride (TG), total cholesterol (TCHO), serum creatine (Scr), FBG, homocysteine (HCY) and uric acid (UA) levels were tested using automatic clinical analyzers (Beckman Coulter); Hyperuricemia was defined as UA ≥ 360 μmol/L in females and 420 μmol/L in males [10]; the estimated glomerular filtration rate (eGFR) was calculated according to the Chronic Kidney Disease Epidemiology Collaboration creatinine equation [11]; serum folate levels were measured using chemiluminescent immunoassays (New Industrial); methylenetetrahydrofolate reductase (MTHFR) C677T gene polymorphisms (CC, CT and TT) were detected using an ABI Prism 7900HT sequence detection system (Life Technologies); urinary albumin levels were measured using an automatic protein analyzer (BN II; Dade Behring); urinary creatinine levels were tested using an automatic biochemical analyzer (Dimension RxL Max; Dade Behring); the urinary albumin to creatinine ratio (UACR) was calculated as the urinary albumin level divided by the urinary creatinine level (mg/g), and a UACR ≥ 30 mg/g was defined as albuminuria [2].
Evaluation of retinopathy
Macula-centered and nonmydriatic fundus pictures were taken by fundus cameras (Canon CR-2 AF, Japan, Kowa nonmyd 7, Japan and Topcon TRC-NW8, Japan) and randomly assessed by 4 eye doctors in a double-masked manner. The assessment of the effect of hypertension on retinal vessels was based on the Keith-Wagener-Barker stages of HR [12, 13] (Supplemental Table 1). Consistency checks were conducted, and the results were found to be reliable (kappa values ranged from 0.71 to 0.95) [14].
Statistical analysis
All statistical analyses were conducted using EmpowerStats (X&Y Solutions, Inc. Boston, MA) software and R (version 3.4.3). Among 3121 participants, only one female was diagnosed with grade 4 HR. Due to an insufficient sample size, subjects with grade 4 were not grouped for analysis. Then, according to the continuous distribution data of albuminuria, we selected the middle 95% of the population, and a total of 2964 subjects were included in the study (Fig. 1). The mean ± the standard deviation and median (interquartile range) are used to express continuous variables, while frequencies are used to express categorical variables. Differences in population characteristics by HR grades were compared using ANOVA tests, Kruskal–Wallis test, or chi-square tests, accordingly. The correlation between albuminuria (as a continuous variable or a categorical variable) and HR was evaluated using multiple linear regression analyses, with adjustment for age, sex, and BMI in model I and age, sex, BMI, SBP, DBP, MTHFR C677T polymorphisms, TCHO, TG, FBG, eGFR, folate, HCY, smoking status, alcohol consumption, and the use of antihypertensive medicine in model II. Stratified analyses were performed to evaluate the relationship between albuminuria (as a continuous variable or a categorical variable) and HR in the following different subgroups: age (< 65 or ≥ 65 years old), sex, BMI (< 24 or ≥ 24 and < 28 or ≥ 28 kg/m2), treatment group (enalapril or enalapril + folic acid), SBP (< 140 or ≥ 140 mmHg), TCHO (< 5.2 or ≥ 5.2 mmol/L), TG (< 1.7 or ≥ 1.7 mmol/L), FBG (< 7.0 or ≥ 7.0 mmol/L), HCY (< 10 or ≥ 10 and < 15 or ≥ 15 μmol/L), hyperuricemia (yes or no), and alcohol consumption and smoking status (never, former, or current). Tests of interactions were performed to assess whether a variable influenced the effect of HR on UACR and albuminuria. The outcomes were expressed as the β or odds ratio (OR) with 95% confidence intervals (CIs). HR was transformed into continuous variables for the trend test. P < 0.05 was considered statistically significant.

Flow chart of the participants
Results
HR was found in 76.6% (n = 2, 271) of the 2964 participants, including 58.9% (n = 1, 747) who were categorized as grade 1, 15.0% (n = 446) who were categorized as grade 2, and 2.6% (n = 78) who were categorized as grade 3.
The baseline characteristics of the subjects are shown in Table 1. There were 1070 males and 1894 females, and the mean age of the participants was 63.5 ± 7.3 years old. The median (interquartile range) UACR level was 10.5 (7.2, 17.1) mg/g, and albuminuria was found in 11.1% (n = 330). Compared with the normal subjects, the subjects with HR had a higher BMI (p = 0.035), SBP (p = 0.006), DBP (p = 0.002), UA (p = 0.005), Scr (p = < 0.001) and UACR (p = 0.003), a lower eGFR (p = 0.007), and a higher proportion of individuals with diabetes (p = 0.045) and albuminuria (p = 0.004).
The results of multivariable regression analyses between HR and UACR are shown in Table 2. In the unadjusted model, HR was associated with higher UACR levels than were found in those with a normal fundus test (grade 1, β = 1.53, 95% CI: 0.06, 3.01, p = 0.042; grade 2, β = 2.69, 95% CI: 0.69, 4.68, p = 0.008; grade 3, β = 5.61, 95% CI: 1.69, 9.54, p = 0.005). After adjusting for age, sex and BMI, this trend was sustained (grade 1, β = 1.72, 95% CI: 0.26, 3.17, p = 0.021; grade 2, β = 3.15, 95% CI: 1.18, 5.12, p = 0.002; grade 3, β = 5.88, 95% CI: 2.01, 9.76, p = 0.003). After adjusting for age, sex, MTHFR C677T genotypes, BMI, SBP, DBP, FBG, TG, TCHO, eGFR, folate, HCY, smoking status, alcohol consumption, and the use of antihypertensive medicine, the trend was also sustained (grade 1, β = 1.42, 95% CI: -0.12, 2.95, p = 0.070; grade 2, β = 2.62, 95% CI: 0.56, 4.67, p = 0.013; grade 3, β = 5.17, 95% CI: 1.13, 9.20, p = 0.012).
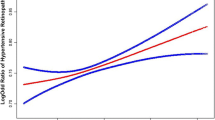
The results of multivariable regression analyses between HR and albuminuria are shown in Table 3. In the unadjusted model, HR was associated with higher odds of albuminuria than was found in subjects with a normal fundus test (grade 1, OR = 1.50, 95% CI: 1.10, 2.05, p = 0.011; grade 2, OR = 1.87, 95% CI: 1.28, 2.75, p = 0.001; grade 3, OR = 2.32, 95% CI: 1.20, 4.47, p = 0.012). This trend was sustained after adjusting for variables in model I (grade 1, OR = 1.51, 95% CI: 1.10, 2.07, p = 0.011; grade 2, OR = 1.99, 95% CI: 1.35, 2.95, p < 0.001; grade 3, OR = 2.37, 95% CI: 1.22, 4.61, p = 0.011) and after adjusting for variables in model II (grade 1, OR = 1.57, 95% CI: 1.08, 2.29, p = 0.019; grade 2, OR = 2.02, 95% CI: 1.28, 3.18, p = 0.002; grade 3, OR = 2.12, 95% CI: 0.99, 4.55, p = 0.053).
The results of stratified analyses between HR and the UACR are shown in Table 4. There were significant interactions when data were stratified by TG (p for interaction = 0.023) and smoking status (p for interaction = 0.014). The correlation between UACR and HR was stronger in current smokers (grade 1, β = 2.5, 95% CI: -1.22, 6.23; grade 2, β = 4.64, 95% CI: -0.13, 9.42; grade 3, β = 18.73, 95% CI: 8.47, 29.00). There were strong correlations between UACR and HR grades 1 and 2 in subjects with TGs ≥ 1.7 mmol/L (grade 1, β = 3.17, 95% CI: 0.53, 5.81; grade 2, β = 4.7, 95% CI: 1.25, 8.15). However, in regard to grade 3, a strong correlation between UACR and HR was found in subjects with TG < 1.7 mmol/L (β = 7.59, 95% CI: 2.8, 12.37).
The results of stratified analyses between HR and albuminuria are shown in Table 5. There was a significant interaction when data were stratified by TG (p for interaction = 0.014). There was a strong correlation between albuminuria and HR grades 1 and 2 in subjects with TGs ≥ 1.7 mmol/L (grade 1, OR = 2.58, 95% CI: 1.36, 4.9; grade 2, OR = 3.62, 95% CI: 1.75, 7.48). However, in regard to grade 3, a strong correlation between albuminuria and HR was found in subjects with TG < 1.7 mmol/L (OR = 2.7, 95% CI: 1.09, 6.73).
Discussion
The prevalence of albuminuria and CKD was 9.4% and 10.8%, respectively in the general Chinese population [2]. Since hypertension is a risk factor for albuminuria and CKD [2], this figure could be higher among hypertension patients. Our results show that among subjects with hypertension, the prevalence of albuminuria was 11.1%, which is slightly higher than that in the general population. Such a high proportion makes CKD a serious public health problem in China, and early detection is becoming particularly important.
Retinopathy and nephropathy are both microvascular diseases and target organ damage observed in hypertension, and there is a definite correlation between them. CKD has been associated with various ocular diseases, such as cataracts, glaucoma, diabetic retinopathy, age-related macular degeneration and vision loss due to various causes [15]. In Bao’s study, a lower arteriovenous ratio was associated with a higher risk of albuminuria and CKD [7]. Huang et al. found that the central retinal artery equivalent was negatively correlated with the UACR in a Chinese population with hypertension [16]. Shantha et al. indicated that HR of any grade had moderate accuracy in predicting microalbuminuria [17, 18]. Vadala et al. concluded that albuminuria was negatively correlated with the index of superficial foveal and parafoveal vessel density in hypertensive patients [19].
In this study, there was a significant correlation between HR grade and albuminuria in hypertensive subjects. In subjects with grade 1 HR, compared with the normal subjects, the UACR increased by 1.42 mg/g, and the odds of albuminuria increased by 57%; in subjects with grade 2 HR, the UACR increased by 2.62 mg/g, and the odds of albuminuria increased by 102%; and in subjects with grade 3 HR, the UACR increased by 5.17 mg/g, and the odds of albuminuria increased by 112%. This suggests that with the aggravation of HR, albuminuria is more obvious, and renal damage is more serious. As a systemic disease, the effects of hypertension on the retinal microvascular and renal microvascular are often parallel [19]. When the glomerular capillary endothelium is damaged, albumin leaks from the blood into the urine. As the structural characteristics of glomerular capillaries are similar to those of systemic vessels, the appearance of albuminuria reflects not only kidney injury but also systemic vascular endothelium abnormalities and atherosclerosis [20, 21]. RMAs are also closely related to endothelial dysfunction, inflammation and arteriosclerosis [14, 22]. This can explain the internal relationship between retinopathy and kidney injury. Therefore, HR can be used as a screening tool for albuminuria and early renal injury.
However, contradictory findings have also been reported. For example, in Bao’s study, the central retinal artery equivalent, central retinal vein equivalent and arteriovenous ratio were not associated with albuminuria and reduced renal function in hypertensive patients [7], and Masaidi et al. reported that there were no significant correlations between the arteriovenous ratio and either eGFR or microalbuminuria in hypertensive patients [8]. These differences may be due to the use of different study populations, the inclusion criteria or adjustment variables applied or the methods used to evaluate the fundus.
In the stratified analyses, a stronger correlation between the UACR and HR was found in current smokers and subjects with higher TG levels, except for in those with grade 3 HR, and the correlations between UACR and grade 3 HR were stronger in subjects with lower TG levels.
Smoking can induce inflammation, oxidative stress and renal fibrosis, leading to kidney injury [23]. Similarly, damage can also occur in the retina. For example, smoking is associated with thinning of the retinal nerve fiber layer [24], choroidal neovascularization and retinal pigment epithelium damage [25]. Recent studies have shown that smoking can reduce vascular density and expand the foveal avascular zone of the retina, indicating that smoking can lead to RMA [26]. Therefore, it is well understood that the correlation between HR and albuminuria is stronger in current smokers. The TG level is a risk factor for endothelial dysfunction [27], arteriosclerosis and cardiovascular disease [28], and TG-lowering therapy is an effective method to reduce cardiovascular and cerebrovascular events [28]. High TG levels are positively associated with nephropathy [29] and retinopathy [30, 31]. This finding can explain the results that the correlation between HR grades 1 and 2 and albuminuria is stronger in subjects with higher TG levels. Interestingly, however, in regard to grade 3, the correlation between HR and albuminuria was stronger in subjects with TG < 1.7 mmol/L. Some studies have also shown that TG is protective against retinopathy [32]. However, due to the small sample size of patients with grade 3 HR in the current study, the reliability of the results may also be affected, and the specific mechanism needs to be further studied.
The strength of this study is that we found a positive correlation between HR and albuminuria in hypertensive adults in rural China. We evaluated the possible effect modifiers in detail and found that this correlation was stronger when the population was stratified by TG levels and smoking status. This finding provides evidence for exploring the relationship between smoking, TG and RMA in the future. It also provides a theoretical basis for focusing on screening and follow-up in people with a possibility of kidney damage, such as smokers with HR. Retinal blood vessels, the only blood vessels that can be directly observed in vivo, are an important marker of systemic vascular disease. If ophthalmologists better understand the relationship between fundus diseases and systemic diseases, they will be able to detect many potential systemic diseases earlier. In the CSPPT cohort, we have been continuously following up the patients for many years to collect more endpoint data for exploration and analysis. We hope to obtain more meaningful information about the correlation between HR and other microvascular diseases by studying this cohort.
There are several limitations to this study. First, because of the limitations of cross-sectional studies, causality could not be obtained. Second, since the fundus pictures were obtained by a nonmydriatic fundus camera, peripheral lesions may have been missed. HR often occurs around the optic disc and macula, and nonmydriatic fundus examination can obtain most of the information. Third, we evaluated RMA based on the Keith-Wagener-Barker stage instead of quantitative parameters. This evaluation of clinical signs may lack objectivity, especially in evaluating “generalized retinal arteriolar narrowing” in grade 1 HR and “definite focal narrowing” in grade 2 HR. To improve the consistency, we trained the evaluators in detail before the study and conducted a consistency test [14]. In addition, although measurements of the arteriovenous ratio can be used to quantify arteriolar narrowing [7, 8, 16], this method lacks indicators, such as focal narrowing, arteriovenous nipping, hemorrhage and exudate, that can better reflect the severity of retinal atherosclerosis and destruction of the blood–retina barrier. Fourth, the sample size of patients with grade 3 HR was small, which may affect the reliability of the results of this group. Because most of the patients in this study were treated with antihypertensive therapy, malignant hypertension was rare. Fifth, our study did not exclude other preexisting kidney diseases, which may affect the accuracy of the UACR results. This should be taken into account when interpreting the results of the study. To reduce the possible impact of renal function on the outcome, we included eGFR in the adjusted variables for multiple regression analysis.
In conclusion, we found that HR was positively correlated with albuminuria in hypertensive adults. This correlation was stronger in current smokers. The correlation between HR grades 1 and 2 and albuminuria was stronger in subjects with higher TG levels, but in regard to grade 3 HR, this correlation was stronger in subjects with lower TG levels. RMA associated with hypertension can be used as an indicator of early renal injury. These results highlight the need for albuminuria screening in hypertensive patients complicated with HR to ensure early detection of CKD.
Availability of data and materials
The data that support the findings of this study are not publicly available because sharing these data might compromise the privacy of the research participants, but the data are available from the corresponding author upon reasonable request.
Abbreviations
- BMI:
-
Body mass index
- CI:
-
Confidence intervals
- CKD:
-
Chronic kidney disease
- DBP:
-
Diastolic blood pressure
- eGFR:
-
Estimated glomerular filtration rate
- FBG:
-
Fasting blood glucose
- HCY:
-
Homocysteine
- HR:
-
Hypertensive retinopathy
- MTHFR:
-
Methylenetetrahydrofolate reductase
- OR:
-
Odds ratio
- RMA:
-
Retinal microvascular abnormalities
- SBP:
-
Systolic blood pressure
- Scr:
-
Serum creatine
- TG:
-
Triglyceride
- TCHO:
-
Total cholesterol
- UA:
-
Uric acid
- UACR:
-
Urinary albumin to creatinine ratio
References
Lewington S, Lacey B, Clarke R, Guo Y, Kong XL, Yang L, et al. The burden of hypertension and associated risk for cardiovascular mortality in China. JAMA Intern Med. 2016;176(4):524–32.
Zhang L, Wang F, Wang L, Wang W, Liu B, Liu J, et al. Prevalence of chronic kidney disease in China: a cross-sectional survey. Lancet. 2012;379(9818):815–22.
Chronic Kidney Disease Prognosis C, Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, et al. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet. 2010;375(9731):2073–81.
Konta T, Hao Z, Takasaki S, Abiko H, Ishikawa M, Takahashi T, et al. Clinical utility of trace proteinuria for microalbuminuria screening in the general population. Clin Exp Nephrol. 2007;11(1):51–5.
Gansevoort RT, Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, et al. Lower estimated GFR and higher albuminuria are associated with adverse kidney outcomes. a collaborative meta-analysis of general and high-risk population cohorts. Kidney Int. 2011;80(1):93–104.
Cheung CY, Ikram MK, Sabanayagam C, Wong TY. Retinal microvasculature as a model to study the manifestations of hypertension. Hypertension. 2012;60(5):1094–103.
Bao S, Huang W, Liang Y, Jiang L, Wang F, Peng Y, et al. Retinal vessel diameter and chronic kidney disease in rural China: a cross-sectional study. Medicine (Baltimore). 2015;94(49): e2076.
Masaidi M, Cuspidi C, Giudici V, Negri F, Sala C, Zanchetti A, et al. Is retinal arteriolar-venular ratio associated with cardiac and extracardiac organ damage in essential hypertension? J Hypertens. 2009;27(6):1277–83.
Huo Y, Li J, Qin X, Huang Y, Wang X, Gottesman RF, et al. Efficacy of folic acid therapy in primary prevention of stroke among adults with hypertension in China: the CSPPT randomized clinical trial. JAMA. 2015;313(13):1325–35.
Qin X, Li Y, He M, Tang G, Yin D, Liang M, et al. Folic acid therapy reduces serum uric acid in hypertensive patients: a substudy of the China Stroke Primary Prevention Trial (CSPPT). Am J Clin Nutr. 2017;105(4):882–9.
Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–12.
Keith NM, Wagener HP, Barker NW. Some different types of essential hypertension: their course and prognosis. Am J Med Sci. 1974;268(6):336–45.
Downie LE, Hodgson LA, Dsylva C, McIntosh RL, Rogers SL, Connell P, Wong TY. Hypertensive retinopathy: comparing the Keith-Wagener-Barker to a simplified classification. J Hypertens. 2013;31(5):960–5.
Zhang W, Li J, Zhao L, Zhang J, She H, Meng Y, et al. Positive relationship of hypertensive retinopathy with carotid intima–media thickness in hypertensive patients. J Hypertens. 2020;38(10):2028–35.
Wong CW, Lamoureux EL, Cheng CY, Cheung GC, Tai ES, Wong TY, et al. Increased burden of vision impairment and eye diseases in persons with chronic kidney disease - a population-based study. EBioMedicine. 2016;5:193–7.
Huang QX, Zhu PL, Huang F, Lin F, Gao ZH, Chen FL, et al. The relationship between association of microalbuminuria and retinal vessel diameter in population with essential hypertension. Zhonghua Nei Ke Za Zhi. 2013;52(4):309–12.
Shantha GP, Kumar AA, Bhaskar E, Sivagnanam K, Srinivasan D, Sundaresan M, et al. Hypertensive retinal changes, a screening tool to predict microalbuminuria in hypertensive patients: a cross-sectional study. Nephrol Dial Transplant. 2010;25(6):1839–45.
Shantha GP, Bhaskar E, Kumar AA, Sundaram V, Senghor A, Swaminathan P, et al. Accuracy of retinal changes in predicting microalbuminuria among elderly hypertensive patients: a cross-sectional study from a teaching hospital in South India. Int Urol Nephrol. 2009;41(1):137–43.
Vadala M, Castellucci M, Guarrasi G, Terrasi M, La Blasca T, Mule G. Retinal and choroidal vasculature changes associated with chronic kidney disease. Graefes Arch Clin Exp Ophthalmol. 2019;257(8):1687–98.
Yun L, Xu R, Zhang L, Li G, Huang S, Yao Y, et al. The role of microalbuminuria in arterial endothelial dysfunction in hypertensive patients with carotid plaques. Int Heart J. 2014;55(2):153–9.
Tomiyama H, Ishizu T, Kohro T, Matsumoto C, Higashi Y, Takase B, et al. Longitudinal association among endothelial function, arterial stiffness and subclinical organ damage in hypertension. Int J Cardiol. 2018;253:161–6.
Klein R, Sharrett AR, Klein BE, Chambless LE, Cooper LS, Hubbard LD, et al. Are retinal arteriolar abnormalities related to atherosclerosis?: the atherosclerosis risk in communities study. Arterioscler Thromb Vasc Biol. 2000;20(6):1644–50.
Mayyas F, Alzoubi KH. Impact of cigarette smoking on kidney inflammation and fibrosis in diabetic rats. Inhal Toxicol. 2019;31(2):45–51.
Demirci S, Gunes A, Demirci S, Kutluhan S, Tok L, Tok O. The effect of cigarette smoking on retinal nerve fiber layer thickness in patients with migraine. Cutan Ocul Toxicol. 2016;35(1):21–5.
Nakayama M, Iejima D, Akahori M, Kamei J, Goto A, Iwata T. Overexpression of HtrA1 and exposure to mainstream cigarette smoke leads to choroidal neovascularization and subretinal deposits in aged mice. Invest Ophthalmol Vis Sci. 2014;55(10):6514–23.
Kalayci M, Cetinkaya E, Suren E, Yigit K, Duman F, Erol MK. The effect of electronic cigarette smoking on retinal microcirculation: enlargement of the foveal avascular zone. Photodiagnosis Photodyn Ther. 2020;32: 102068.
Kajikawa M, Maruhashi T, Matsumoto T, Iwamoto Y, Iwamoto A, Oda N, et al. Relationship between serum triglyceride levels and endothelial function in a large community-based study. Atherosclerosis. 2016;249:70–5.
Generoso G, Janovsky C, Bittencourt MS. Triglycerides and triglyceride-rich lipoproteins in the development and progression of atherosclerosis. Curr Opin Endocrinol Diabetes Obes. 2019;26(2):109–16.
Sacks FM, Hermans MP, Fioretto P, Valensi P, Davis T, Horton E, et al. Association between plasma triglycerides and high-density lipoprotein cholesterol and microvascular kidney disease and retinopathy in type 2 diabetes mellitus: a global case-control study in 13 countries. Circulation. 2014;129(9):999–1008.
Chung YR, Park SW, Choi SY, Kim SW, Moon KY, Kim JH, et al. Association of statin use and hypertriglyceridemia with diabetic macular edema in patients with type 2 diabetes and diabetic retinopathy. Cardiovasc Diabetol. 2017;16(1):4.
Zoppini G, Negri C, Stoico V, Casati S, Pichiri I, Bonora E. Triglyceride-high-density lipoprotein cholesterol is associated with microvascular complications in type 2 diabetes mellitus. Metabolism. 2012;61(1):22–9.
Zhang G, Chen H, Chen W, Zhang M. Prevalence and risk factors for diabetic retinopathy in China: a multi-hospital-based cross-sectional study. Br J Ophthalmol. 2017;101(12):1591–5.
Acknowledgements
Not applicable.
Funding
This work was supported by the National Key Research and Development Program [2016YFC0903103, 2016YFE0205400, 2018ZX09739, 2018ZX09301034003]; the Science and Technology Planning Project of Guangzhou, China [201707020010]; the Science, Technology and Innovation Committee of Shenzhen [JSGG20170412155639040, GJHS20170314114526143, JSGG20180703155802047]; the National Natural Science Foundation of China [81730019, 81973133]; the Outstanding Youths Development Scheme of Nanfang Hospital, Southern Medical University [2017J009].
Author information
Authors and Affiliations
Contributions
Jun Li and Wenbo Zhang are co-first authors and contributed equally. Study concept and design: Wenbo Zhang, Xiping Xu, Liu Yang and Yong Huo. Collection of epidemiological data: Ying Meng, Yadi Zhang, Xiaopeng Gu, Yan Zhang, Jianping Li, Xianhui Qin, Binyan Wang, Fanfan Hou, Genfu Tang, Rongfeng Liao, Lishun Liu and Meiqing Huang. Evaluated the grading of fundus lesions: Jun Li, Liang Zhao, Jing Zhang and Haicheng She. Data management and statistical analysis: Wenbo Zhang, Xinlei Bai, Lishun Liu and Meiqing Huang. Drafting of the manuscript: Wenbo Zhang. Critical review and revision of the manuscript: Jun Li and Liu Yang. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study complied with the Helsinki Declaration and was approved by the Ethics Committee of the Institute of Biomedicine, Anhui Medical University, Hefei, China (FWA assurance number FWA00001263). Written informed consent was obtained from all participants.
Consent for publication
Not applicable.
Competing interests
Dr. Yong Huo received a grant from the National Key Research and Development Program [2016YFC0903103]. Dr. Xiping Xu received grants from the National Key Research and Development Program [2016YFE0205400, 2018ZX09739, 2018ZX09301034003], the Science and Technology Planning Project of Guangzhou, China [201707020010], and the Science, Technology and Innovation Committee of Shenzhen [JSGG20170412155639040, GJHS20170314114526143, JSGG20180703155802047]. Dr. Xianhui Qin received grants from the National Natural Science Foundation of China [81730019, 81973133] and the Outstanding Youths Development Scheme of Nanfang Hospital, Southern Medical University [2017J009]. For the remaining authors, there are no conflicts of interest to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Supplementary Table 1. The Keith-Wagener-Barker classification for hypertensive retinopathy.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, J., Zhang, W., Zhao, L. et al. Positive correlation between hypertensive retinopathy and albuminuria in hypertensive adults. BMC Ophthalmol 23, 66 (2023). https://doi.org/10.1186/s12886-023-02807-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12886-023-02807-6