
Abstract
Background
This study aimed to compare surgically induced astigmatism (SIA) on the anterior and total cornea during cataract surgery through a 2.2 mm steep meridian incision.
Methods
The study included 69 left eyes of 69 patients who had undergone cataract surgery. The 69 eyes were classified into three subgroups according to the preoperative steep meridian. Following phacoemulsification, an intraocular lens was inserted into the bag. The keratometric measurements were taken 12 months postoperatively, on the anterior cornea (automated keratometer and anterior keratometry [K] from a rotating Scheimpflug camera) and total cornea (equivalent K reading [EKR] 3.0 mm, EKR 4.5 mm, total corneal refractive power (TCRP) 2.0 mm ring, TCRP 3.0 mm zone, TCRP 4.0 mm zone). The SIA was analyzed for each parameter.
Results
On the double-angle polar plot, the summated vector mean values of SIA determined by the automated keratometer and Scheimpflug anterior K were 0.28 diopter (axis: 177°) and 0.37 diopter (axis: 175°) in with-the-rule (WTR) astigmatism; 0.03 diopter (axis: 156°) and 0.18 diopter (axis: 177°) in oblique astigmatism; 0.15 diopter (axis: 96°) and 0.17 diopter (axis: 73°) in against-the-rule (ATR) astigmatism. The mean SIAs on the total cornea ranged from 0.31 to 0.42 diopter in WTR astigmatism; from 0.16 to 0.27 diopter in oblique astigmatism; from 0.04 to 0.11 diopter in ATR astigmatism. Mean magnitude SIA ranged from 0.41 to 0.46 diopter on anterior corneal surface and 0.50 to 0.62 diopter on total cornea. J0 and J45 of the posterior cornea showed no significant changes after cataract surgery, and the changes in J0 and J45 did not show any statistical differences between the anterior and total cornea (all p > 0.05).
Conclusions
There were no differences in the summed vector mean values of SIA between the anterior cornea and the total cornea.
Similar content being viewed by others


Background
In modern cataract surgery, complications are uncommon, and the importance of refractive outcomes is increasing [1]. Consequently, minimizing residual astigmatism is one of the main goals of modern cataract surgery. It is important to calculate surgically induced astigmatism (SIA) accurately in the process of astigmatic correction.
The proper choice of incision location in cataract surgery helps reduce astigmatism. The clear corneal incision located on the preoperative steep meridian decreased keratometric astigmatism at the sup, superotemporal, and temporal locations [2,3,4]. The accurate assessment of SIA is also necessary for surgical procedures, such as toric IOL implantation and astigmatic keratotomy combined with cataract surgery. SIA is included as part of the toric IOL nomogram [5] or the arcuate keratotomy nomogram. Jin et al. [6] found that 0.5 diopter of SIA would be added by a 2.8-mm wide superior incision, whereas Goggin et al. [7, 8] found that 0.62 diopter of SIA would be added by a 2.2–2.3 mm wide superior incision. Alio et al. [9] applied 0.5 diopter of SIA after a 2.7-mm-wide steep meridian incision. Zhang et al. [10] recently compared residual astigmatism according to keratometric measurements and concluded that the 0.2 diopter of SIA is induced by a temporal incision.
Ofir et al. [11] found that there were differences in the calculated SIA depending on the type of keratometer used. SIA on the posterior corneal surface was also found to be an important factor that had a clinical impact on the assessment of astigmatism [12]. However, most previous studies investigating SIA only considered the anterior corneal surface [2, 5, 13,14,15,16,17,18]. It is also important for cataract surgeons to know whether the posterior cornea has an effect on enhancing or reducing the SIA of the anterior cornea. Additionally, no previous study has calculated SIA on the total cornea after 2.2-mm micro coaxial cataract surgery on the steep axis.
In this study, we aimed to evaluate the SIA using an automated keratometer and a Scheimpflug rotating camera. SIAs on the total cornea were also analyzed using a Scheimpflug camera. The SIAs calculated using various keratometric measurements were compared.
Methods
Participants
This retrospective study included 69 left eyes of 69 patients who underwent cataract surgery at our institution between September 2017 and August 2018. This study was approved by the Institutional Review Board Committee of Yeouido St. Mary Hospital, and informed consent was obtained from all patients before commencement. The study adhered to the tenets of the Declaration of Helsinki for the use of human participants in biomedical research. None of the patients had a history of ocular disease, previous ocular surgery, or general disorders that affected the cornea, and there were no intraoperative complications.
Cataract surgery
After preoperative measurements, all patients underwent cataract surgery through a 2.2 mm micro coaxial incision. All surgeries were performed using the OZil torsional handpiece with the Centurion System (Alcon, Fort Worth, TX, USA). All procedures were performed by a single surgeon (W. J. W.). Local anesthesia was administered using 0.5% proparacaine hydrochloride (Alcaine, Alcon). Surgery was performed through a self-sealing, clear corneal incision on the steep meridian provided by Scheimpflug anterior keratometry (K) to reduce keratometric astigmatism [3, 19, 20]. With the patient seated, the corneal limbus was marked at the 0°, 180°, and 270° axes using pre-op toric reference marker (ASICO, IL, USA). Next, with the patient lying on the surgical table, the steep meridian was identified and marked using a Mendez degree gauge (Katena Eye Inc., NJ, USA) with the aid of preplaced reference points. The Intrepid ClearCut 2.2 mm dual-bevel metal keratome (Alcon, Fort Worth, Texas) was used to make a two-step 2.2 mm incision. Using a Beaver blade, a 1.0 mm single-plane side-port clear corneal incision was made 90° to the left of the main corneal incision. The cataract was removed using a 0.9 mm mini flared 30-degree Kelman ABS tip with a 2.2 mm micro coaxial incision. Phacoemulsification was performed with 100% torsional ultrasound, a vacuum of 350 mmHg, and an aspiration rate of 35 cc/min. Following phacoemulsification, an intraocular lens (IOL; Johnson & Johnson ZCB00, Santa Ana, USA) was inserted into the bag. At the end of the surgery, the incision sites were hydrated with a balanced salt solution and no sutures were applied.
Keratometric measurements
The keratometric values were measured preoperatively and 12 months postoperatively using an RK-5 automated keratometer (Canon, Tochigiken, Japan) and Pentacam rotating Scheimpflug camera (Oculus, Wetzler, Germany). The Pentacam HR analyzed the cornea via 25 picture scans, and only scans that had an examination quality specification graded by the instrument as “OK” were included in this study.
The average K reading was the arithmetic mean of the pair of meridians, 90° apart, showing the greatest difference in axial power within the central 3.0 mm. This was equivalent to the simulated K of traditional corneal topography and was calculated by entering the corneal curvature radius into the thin-lens formula for paraxial imagery, which considers the cornea as a single refractive sphere.
The equivalent K reading (EKR) was calculated using the formula previously described by Holladay et al. [21], taking into account the effect of the posterior corneal curvature.
The total corneal refractive power (TCRP) was calculated using the ray tracing method. Corneal thickness and curvatures of both the anterior and posterior corneal surfaces were obtained using Scheimpflug imaging. Snell’s law and the specific refractive indices of air, cornea, and aqueous humor were used to calculate the corneal power.
Data analysis
A total of 69 eyes were classified into three subgroups based on the steep meridian measured by Scheimpflug anterior K. Thirty-two eyes were defined as with-the-rule (WTR) astigmatism with a steep meridian between 60° and 120°. Twenty-four eyes were classified as against-the-rule (ATR) astigmatism with a steep meridian between 150° and 30°. The remaining 13 eyes were classified into the oblique astigmatism group.
Two parameters were used to analyze the SIA: (1) the mean magnitude SIA [22] and (2) the summed mean values of SIA [2, 23, 24]. SIA was determined as the vectorial difference between the preoperative and postoperative astigmatism, and the mean magnitude SIA was defined as the mean absolute value of each vector. The preoperative and postoperative corneal astigmatism with their constituent magnitude and meridian were decomposed to J0 (vertical and horizontal components of corneal astigmatism transposed in the Jackson coefficient orthogonal system) and J45 (an oblique component of corneal astigmatism transposed in the Jackson coefficient orthogonal system). ∆ J0 was defined as the value obtained by subtracting the preoperative J0 from the postoperative J0, and ∆ J45 was defined as the value obtained by subtracting the preoperative J45 from the postoperative J45. The mean centroid SIA was calculated using Eye Pro 2013: Astig PLOT (for iPhone/iPad [Apple, Cupertino, CA, USA]), developed by Dr. Edmondo Borasio and was represented by double-angle polar plots [2]. The flattening effect providing the astigmatic change at the steep meridian and torque rotating preoperative astigmatism were also calculated [5, 25].
Statistical analysis
Statistical analysis was performed using SPSS statistical software (version 23.0, SPSS, Inc., Chicago, IL, USA). The normality of the distribution for each data point was checked using the Kolmogorov-Smirnov test. The paired t-test and the Wilcoxon ranked-sum test were used to compare preoperative corneal astigmatism with postoperative corneal astigmatism and to determine if there were significant differences between the SIA on the anterior cornea and the SIA on the total cornea. Statistical significance was set at p < 0.05.
Results
A total of 69 left eyes (69 patients) were evaluated in this study. The mean age was 63.39 ± 8.17 years (range: 46–83 years). There were 43 female patients (62.3%).
Table 1 presents the preoperative and postoperative data. The mean corneal astigmatism measured by automated keratometer, Scheimpflug anterior K, EKR 4.5 mm zone, and TCRP 4.0 mm zone showed significant changes at 3 months postoperatively (all p < 0.01). Table 2 shows the preoperative and postoperative data for the three subgroups. In the WTR astigmatism group, the mean corneal astigmatism by automated keratometer, Scheimpflug anterior K, EKR 4.5 mm zone, and TCRP 4.0 mm zone were significantly reduced (all p < 0.01). In contrast, in the oblique astigmatism and ATR astigmatism groups, only the mean corneal astigmatism measured with Scheimpflug anterior K was significantly decreased (p = 0.037, for the oblique astigmatism group and p = 0.021, for the ATR astigmatism group).
Table 3 shows the arithmetic mean SIA, change in J0 (∆ J0), and change in J45 (∆ J45) as determined by each type of keratometric measurement. The arithmetic mean SIAs determined by the automated keratometer and Pentacam anterior K were 0.41 and 0.46 diopter, respectively, whereas the SIA on the posterior cornea was 0.13 diopter. The SIA determined using the TCRP 2.0 mm ring was 0.68 diopter, which was the largest among the SIAs on the total cornea. This was followed by the SIA determined by the EKR 3.0 mm zone, TCRP 3.0 mm zone, EKR 4.5 mm zone, and TCRP 4.0 mm zone. In our comparison of arithmetic mean SIAs on the anterior cornea, the values determined by the automated keratometer and Scheimpflug anterior K were not significantly different (p = 0.09). The arithmetic mean SIAs of the anterior cornea were significantly higher than the mean arithmetic SIAs on the posterior cornea (all p < 0.001) but were less than the arithmetic mean SIAs on the total cornea except for the TCRP 4.0 mm zone (p = 0–0.021). However, the ∆ J0 and ∆ J45 values measured on the anterior corneal surface and the total cornea were not different (all p > 0.05). The arithmetic mean SIA, ∆ J0, and ∆ J45 classified according to the preoperative steep corneal meridian are listed in Table 4. The arithmetic mean SIA analyzed in the TCRP 4.0 mm zone showed no significant difference from the mean arithmetic SIAs calculated on the anterior corneal surface. In the case of ∆ J0 and ∆ J45, there was no statistically significant difference between the changes measured on the anterior surface of the cornea and those of the whole cornea, irrespective of the preoperative steep corneal meridian and the location of the corneal incision.
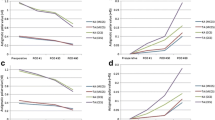
Figure 1 shows the mean SIAs on the double-angle polar plots calculated by the aggregate analysis. All mean SIAs were less than 0.25 diopter. Figure 2 shows the mean SIAs in the preoperative WTR group. The mean SIAs determined by the automated keratometer and Scheimpflug anterior K were 0.28 diopter (axis: 177°) and 0.37 diopter (axis: 175°). The mean SIAs on the total cornea ranged from 0.31 to 0.42 diopter in WTR astigmatism. The mean SIAs in the oblique astigmatism group are shown in Fig. 3. The mean SIAs of the anterior corneal surface were 0.03 diopter (axis: 156°, for the automated keratometer) and 0.18 diopter (axis: 177°, for Scheimpflug anterior K). The mean SIAs of the total cornea ranged from 0.16 to 0.27 diopter. Figure 4 shows the results of the preoperative ATR astigmatism. In the ATR group, in particular, the mean SIA of the total cornea did not exceed the mean SIA of the anterior corneal surface (0.05 diopter, axis: 79 ° ~ 0.11 diopter, axis: 89°, for total cornea vs. 0.15 diopter, axis: 96 ° ~ 0.17 diopter, axis: 73°, for total cornea). The mean magnitude of SIA on the posterior corneal surface ranged from 0.12 to 0.13 diopter, but the mean SIAs on the double-angle polar plot did not exceed 0.1 diopter in the three subgroups (Figs. 2, 3 and 4).

Surgically induced astigmatism (SIA) was calculated using each keratometric measurement. Each vector and the mean SIA are represented on a double-angle polar plot. A automated keratometer, B Scheimpflug anterior K, C Scheimpflug posterior K, D Scheimpflug EKR 3.0 mm, E Scheimpflug EKR 4.5 mm, F Scheimpflug TCRP 2.0 mm ring, G Scheimpflug TCRP 3.0 mm zone, and H Scheimpflug TCRP 4.0 mm zone

Mean surgically induced astigmatism (SIA) in superior incision (preoperative WTR astigmatism) group. A automated keratometer, B Scheimpflug anterior K, C Scheimpflug posterior K, D Scheimpflug EKR 3.0 mm, E Scheimpflug EKR 4.5 mm, F Scheimpflug TCRP 2.0 mm ring, G Scheimpflug TCRP 3.0 mm zone, and H Scheimpflug TCRP 4.0 mm zone

Mean surgically induced astigmatism (SIA) in superotemporal or superonasal incision (preoperative oblique astigmatism) group. A automated keratometer, B Scheimpflug anterior K, C Scheimpflug posterior K, D Scheimpflug EKR 3.0 mm, E Scheimpflug EKR 4.5 mm, F Scheimpflug TCRP 2.0 mm ring, G Scheimpflug TCRP 3.0 mm zone, and H Scheimpflug TCRP 4.0 mm zone

Mean surgically induced astigmatism (SIA) in temporal incision (ATR astigmatism) group. A automated keratometer, B Scheimpflug anterior K, C Scheimpflug posterior K, D Scheimpflug EKR 3.0 mm, E Scheimpflug EKR 4.5 mm, F Scheimpflug TCRP 2.0 mm ring, G Scheimpflug TCRP 3.0 mm zone, and (H) Scheimpflug TCRP 4.0 mm zone
Discussion
This study demonstrated that ∆ J0 and ∆ J45 did not show any significant differences between the anterior cornea and the total cornea. Regardless of the preoperative steep meridian or location of the incision, the summated vector for the mean SIA on double-angle polar plots also did not show any significant differences.
The mean arithmetic SIA of the posterior cornea was 0.13 ± 0.08 diopter, and these results are similar to those in the study by Cheng et al. [26] However, our values were lower than those of the study by Nemeth et al. [12] The differences may be due to differences in inclusion criteria, as they included only patients with preoperative WTR astigmatism. The posterior cornea has a relatively steeper radius than the anterior cornea. Furthermore, when a more central location is created on the posterior cornea, a greater change is observed compared to a cut located more peripherally on the anterior cornea [26]. However, the difference in refractive indices between the cornea and aqueous humor is small [26]; hence, the posterior cornea induces minimal refractive astigmatism and can be ignored in the calculations of astigmatism [27]. In this study, the effect of the posterior corneal change on astigmatism was limited. Unlike the mean magnitude SIA on the posterior surface of the cornea, the summated vector mean SIA in double-angle polar plots did not exceed 0.1 diopters. The direction of the astigmatic change on the posterior surface was also the opposite direction to the astigmatic change on the anterior surface of the cornea (76° vs. 175–177°, for the WTR astigmatism group; 176° vs. 73–96°, for the ATR astigmatism group). Klijn et al. [28] found that the incision effect on the posterior corneal surface was of the same order of magnitude as the test-retest effect and concluded that the contribution of the posterior cornea to astigmatic change is limited. Kohnen et al. [29] also concluded that the SIA on the posterior corneal surface of a 2.2 mm femtosecond laser-assisted clear corneal incision was clinically insignificant. These results are contrary to the results of a recent study showing that posterior corneal astigmatism increased after the creation of a 1.8 mm steep meridian clear corneal incision [30]. Kim et al. [31] concluded that the direction of the astigmatism change in the posterior corneal surface after 2.2 mm temporal limbo-corneal incision was not uniform.
The mean magnitude of SIA on the total cornea was greater than the mean arithmetic SIA on the anterior corneal surface. Among the arithmetic mean SIAs on the total cornea, SIA on the more central cornea had a greater magnitude, and the TCRP 2.0 mm ring produced the greatest magnitude value of SIA. However, these results do not indicate that the amount of astigmatism reduction in the total cornea is greater than that in the anterior cornea. As the astigmatic changes in the total cornea occur in inconsistent directions, the mean change in the double-angle polar plot is not different from that of the anterior cornea. In Figs. 2, 3 and 4, the standard deviation of mean centroid SIA values on the total cornea ranged from 0.56 to 0.70 diopter (0.55–0.78 diopter in WTR astigmatism; 0.49–0.74 diopter in oblique astigmatism; 0.52–0.80 diopter in ATR astigmatism) and they were relatively greater than the standard deviation of the mean centroid SIA from the anterior corneal surface. (0.48–0.53 diopter in total 69 eyes; 0.47–0.54 diopter in WTR astigmatism; 0.43–0.46 diopter in oblique astigmatism; 0.41–0.43 diopter in ATR astigmatism).
A limitation of this study is that there is no clear indicator to determine the location of the steep meridian clear corneal incision. A rotating Scheimpflug camera provides various parameters for evaluating the astigmatism of the total cornea. The total corneal power can be calculated using a ray tracing method (TCRP) at 2.0, 3.0, 4.0, 5.0, 6.0, 7.0, and 8.0 mm and EKR at 2.0, 3.0, 4.0, 4.5, 5.0, and 6.0 mm. Savini et al. [32] concluded that a 3.0 mm zone TCRP and 2.0 mm ring TCRP accurately reflect surgically induced refractive changes in photorefractive keratectomy (PRK) and laser-assisted in situ keratomileusis (LASIK). They also found that 3.0 mm EKR and 2.0 mm TCRP induced the lowest median absolute errors when corneal measurements obtained by Pentacam HR were applied in cataract surgery [33]. Holladay et al. [21] demonstrated that EKR in the 4.5 mm zone yielded the highest correlation with subjective refraction compared to the historical method of K reading after LASIK and PRK. However, we performed a steep meridian incision, as determined by a Scheimpflug anterior K.
Conclusion
In conclusion, our study demonstrated that, when considering the cornea as a whole, the SIA was not different from the SIAs with consideration of the anterior corneal surface only. A comparison between the steep meridian incision planned based on anterior corneal power measurements (automated keratometer or Scheimpflug anterior K) and the steep meridian incision based on total corneal power measurements (Scheimpflug EKR or TCRP) should be performed in future studies.
Availability of data and materials
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Abbreviations
- SIA:
-
Surgically induced astigmatism
- EKR:
-
Equivalent keratometry reading
- TCRP:
-
Total corneal refractive power
- WTR:
-
With-the-rule
- ATR:
-
Against-the-rule
- IOL:
-
Intraocular lens
References
Kohnen T, Koch MJ. Refractive aspects of cataract surgery. Curr Opin Ophthalmol. 1998;9(1):55–9.
Borasio E, Mehta JS, Maurino V. Surgically induced astigmatism after phacoemulsification in eyes with mild to moderate corneal astigmatism: temporal versus on-axis clear corneal incisions. J Cataract Refract Surg. 2006;32(4):565–72.
Rho CR, Joo CK. Effects of steep meridian incision on corneal astigmatism in phacoemulsification cataract surgery. J Cataract Refract Surg. 2012;38(4):666–71.
Ozyol E, Ozyol P. The relation between superior phacoemulsification incision and steep axis on astigmatic outcomes. Int Ophthalmol. 2012;32(6):565–70.
Borasio E, Mehta JS, Maurino V. Torque and flattening effects of clear corneal temporal and on-axis incisions for phacoemulsification. J Cataract Refract Surg. 2006;32(12):2030–8.
Jin H, Limberger IJ, Ehmer A, Guo H, Auffarth GU. Impact of axis misalignment of toric intraocular lenses on refractive outcomes after cataract surgery. J Cataract Refract Surg. 2010;36(12):2061–72.
Goggin M, Moore S, Esterman A. Toric intraocular lens outcome using the manufacturer's prediction of corneal plane equivalent intraocular lens cylinder power. Arch Ophthalmol. 2011;129(8):1004–8.
Goggin M, Moore S, Esterman A. Outcome of toric intraocular lens implantation after adjusting for anterior chamber depth and intraocular lens sphere equivalent power effects. Arch Ophthalmol. 2011;129(8):998–1003.
Alio JL, Pinero DP, Tomas J, Aleson A. Vector analysis of astigmatic changes after cataract surgery with toric intraocular lens implantation. J Cataract Refract Surg. 2011;37(6):1038–49.
Zhang L, Sy ME, Mai H, Yu F, Hamilton DR. Effect of posterior corneal astigmatism on refractive outcomes after toric intraocular lens implantation. J Cataract Refract Surg. 2015;41(1):84–9.
Ofir S, Abulafia A, Kleinmann G, Reitblat O, Assia EI. Surgically induced astigmatism assessment: comparison between three corneal measuring devices. J Refract Surg. 2015;31(4):244–7.
Nemeth G, Berta A, Szalai E, Hassan Z, Modis L Jr. Analysis of surgically induced astigmatism on the posterior surface of the cornea. J Refract Surg. 2014;30(9):604–8.
Altan-Yaycioglu R, Akova YA, Akca S, Gur S, Oktem C. Effect on astigmatism of the location of clear corneal incision in phacoemulsification of cataract. J Refract Surg. 2007;23(5):515–8.
Kohnen S, Neuber R, Kohnen T. Effect of temporal and nasal unsutured limbal tunnel incisions on induced astigmatism after phacoemulsification. J Cataract Refract Surg. 2002;28(5):821–5.
Morlet N, Minassian D, Dart J. Astigmatism and the analysis of its surgical correction. Br J Ophthalmol. 2001;85(9):1127–38.
Kershner RM. Clear corneal cataract surgery and the correction of myopia, hyperopia, and astigmatism. Ophthalmology. 1997;104(3):381–9.
Pfleger T, Skorpik C, Menapace R, Scholz U, Weghaupt H, Zehetmayer M. Long-term course of induced astigmatism after clear corneal incision cataract surgery. J Cataract Refract Surg. 1996;22(1):72–7.
Rauz S, Reynolds A, Henderson HW, Joshi N. Variation in astigmatism following the single-step, self-sealing clear corneal section for phacoemulsification. Eye. 1997;11(Pt 5):656–60.
Amesbury EC, Miller KM. Correction of astigmatism at the time of cataract surgery. Curr Opin Ophthalmol. 2009;20(1):19–24.
Nielsen PJ. Prospective evaluation of surgically induced astigmatism and astigmatic keratotomy effects of various self-sealing small incisions. J Cataract Refract Surg. 1995;21(1):43–8.
Holladay JT, Hill WE, Steinmueller A. Corneal power measurements using scheimpflug imaging in eyes with prior corneal refractive surgery. J Refract Surg. 2009;25(10):862–8.
Thibos LN, Wheeler W, Horner D. Power vectors: an application of Fourier analysis to the description and statistical analysis of refractive error. Optometry Vision Sci. 1997;74(6):367–75.
Holladay JT, Dudeja DR, Koch DD. Evaluating and reporting astigmatism for individual and aggregate data. J Cataract Refract Surg. 1998;24(1):57–65.
Holladay JT, Moran JR, Kezirian GM. Analysis of aggregate surgically induced refractive change, prediction error, and intraocular astigmatism. J Cataract Refract Surg. 2001;27(1):61–79.
Reinstein DZ, Archer TJ, Srinivasan S, Mamalis N, Kohnen T, Dupps WJ, et al. Standard for reprting refractive outcomes of intraocular lens-based refractive surgery. J Cataract Refract Surg. 2017;43(4):435–9.
Cheng LS, Tsai CY, Tsai RJ, Liou SW, Ho JD. Estimation accuracy of surgically induced astigmatism on the cornea when neglecting the posterior corneal surface measurement. Acta Ophthalmol. 2011;89(5):417–22.
Koch DD, Jenkins RB, Weikert MP, Yeu E, Wang L. Correcting astigmatism with toric intraocular lenses: effect of posterior corneal astigmatism. J Cataract Refract Surg. 2013;39(12):1803–9.
Klijn S, van der Sommen CM, Sicam VA, Reus NJ. Value of posterior keratometry in the assessment of surgically induced astigmatic change in cataract surgery. Acta Ophthalmol. 2016;94(5):494–8.
Kohnen T, Löffler F, Herzog M, Petermann K, Böhm M. Tomographic analysis of anterior and posterior surgically induced astigmatism after 2.2 mm temporal clear corneal incisions in femtosecond laser-assisted cataract surgery. J Cataract Refract Surg. 2019;45(11):1602–11.
Li X, Chen X, He S, Xu W. Effect of 1.8-mm steep-axis clear corneal incision on the posterior corneal astigmatism in candidates for toric IOL implantation. BMC Ophthalmol. 2020;20(1):187.
Kim YJ, Knorz MC, Auffarth GU, Choi CY. Change in anterior and posterior curvature after cataract surgery. J Refract Surg. 2016;32(11):754–9.
Savini G, Hoffer KJ, Carbonelli M, Barboni P. Scheimpflug analysis of corneal power changes after myopic excimer laser surgery. J Cataract Refract Surg. 2013;39(4):605–10.
Savini G, Barboni P, Carbonelli M, Hoffer KJ. Comparison of methods to measure corneal power for intraocular lens power calculation using a rotating Scheimpflug camera. J Cataract Refract Surg. 2013;39(4):598–604.
Acknowledgements
Not applicable for this study.
Funding
There is no funding to declare in this study.
Author information
Authors and Affiliations
Contributions
MH and YCY contributed to the design of the manuscript. MH and YCY collected the data. MH, YCY and WJW performed the clinical examination and investigation. WJW and MH shared in data analysis and interpretation and revised the intellectual content of the manuscript. WJW critically revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the institutional research board (IRB) of the St.Mary’s Hospital and was performed in accordance with the ethical standards of the Declaration of Helsinki. All patients included in the study provided verbal informed consent. As this study conducted retrospectively and all data was anonymized, the written informed consent procedures have been exempted under the provisions of IRB of St.Mary’s Hospital.
Consent for publication
Not applicable for this study.
Competing interests
The authors declare that they have no competing interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yoon, Yc., Ha, M. & Whang, WJ. Comparison of surgically induced astigmatism between anterior and total cornea in 2.2 mm steep meridian incision cataract surgery. BMC Ophthalmol 21, 373 (2021). https://doi.org/10.1186/s12886-021-02131-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12886-021-02131-x