
Abstract
Background
To demonstrate that the Corvis ST could be used to quantify the biomechanical parameters of the orbital soft tissues by measuring and comparing whole eye movement (WEM) using the Corvis in normal eyes and in eyes of patients with Graves ophthalmopathy.
Methods
Forty four eyes of 44 ophthalmologically normal subjects and 28 eyes of 28 patients with Graves ophthalmopathy were included in the study. After Corvis test, the examiners recorded WEM by air puff. In the patients with Graves ophthalmopathy, the partial correlation coefficient adjusted for age and gender was calculated to analyze the correlation between exopthalmometry and WEM. Same analysis was repeated for the correlation between and the cross sectional area (%) of the extraocular muscles in the orbit CT and WEM.
Results
WEM was 0.314 ± 0.083 mm in the normal subjects and 0.227 ± 0.079 mm in the Graves ophthalmopathy group (p = 0.000). The exophthalmometry was not significantly correlated with WEM after adjusting for age and gender (R = 0.083, p = 0.688). In the 21 Graves ophthalmopathy patients examined by orbit CT, after adjusting for age and gender, WEM significantly decreased as the cross sectional area (%) of the extraocular muscles in the orbit increased (R = − 0.461, p = 0.047).
Conclusions
WEM by Corvis could be used to quantify the biomechanical parameters of the orbital soft tissue. However, it is unclear whether WEM effectively represents the orbital biomechanical parameters, because WEM is only 0.6% of the orbital depth.
Similar content being viewed by others


Background
The recently developed corneal dynamic scheimpflug analyser (Corvis ST; Oculus, Wetzler, Germany) is a diagnostic instrument comprising a noncontact tonometer, a Scheimpflug geometry, and an ultra-high speed camera that can measure intraocular pressure and corneal biomechanical parameters. The Corvis ST releases a puff of air onto the patient’s cornea just like a noncontact tonometer. The Scheimpflug geometry and ultra high-speed camera record a movie of the change in the corneal sagittal section in response to the air puff. When the air puff is released, the cornea first flattens, then becomes somewhat concave, flattens again, and then returns to its original contour. The Corvis ST measures not only intraocular pressure, but several other parameters as well, such as the deformation amplitude and first applanation time, which represent corneal biomechanical parameters. This device is therefore used in clinics and for studies of corneal biomechanics [1,2,3,4,5,6], keratoconus [7,8,9,10], changes after refractive surgery [11,12,13,14,15], and glaucoma [16,17,18,19,20].
During the measurement, there is a slight but significant movement of the whole eye globe [21]. As the cornea deforms and approaches maximum displacement, the whole eye displays a slow linear motion in the anterior-posterior direction. When the cornea reaches maximum displacement, the whole eye motion becomes more pronounced and nonlinear in nature, as the air puff pressure continues to increase to a consistent maximum.
The authors hypothesized that we could use the Corvis ST to quantify the biomechanical parameters of the orbital soft tissue behind the eyeball based on the eyeball displacement during the air puff. If the orbital soft tissues, such as the fat and extraocular muscles, change, we would expect that eyeball displacement would also change.
In the present study, the authors measured and compared whole eye movement (WEM) using the Corvis ST in normal eyes and in eyes of patients with Graves ophthalmopathy whose orbital soft tissue might be altered. The authors demonstrated that the Corvis ST could be used to quantify the biomechanical parameters of the orbital soft tissues.
Methods
Corvis ST data collected during intraocular pressure measurement of patients who visited oculoplastics clinic of Seoul St. Mary’s Hospital were used in this study. A total of 44 right eyes of 44 ophthalmologically normal subjects and 28 right eyes of 28 patients with Graves ophthalmopathy were included in the study. This retrospective study adhered to the tenets of the Declaration of Helsinki and received institutional review board approval from Seoul St. Mary’s Hospital for the analysis of their medical records. This study was conducted from January 2016 to December 2016. The authors collected age, gender and Corvis ST data of normal subjects and patients with Graves ophthalmopathy and exophthalmometry, severity and activity of Graves ophthalmopathy and orbit computed tomography (CT) scans of patients with Graves ophthalmopathy. One author had access to information that could identify individual participants during or after data collection. Inclusion criteria for the normal group included the absence of the following: thyroid disease, orbital inflammation, blow out fracture, severe lid inflammation, corneal ulcer, and risk of eyeball rupture (severe thinning of cornea or sclera). The inclusion criterion for the Graves ophthalmopathy group was mild severity or higher according to European Group on Graves’ orbitopathy (EUGOGO) [22]. Patients who had received radiation therapy or systemic steroid treatment were included. Patients with a risk of eyeball rupture or who had undergone decompression surgery for Graves ophthalmopathy were excluded.
The examiners performed the Corvis ST test for intraocular pressure measurement. The examiners examined the eyes with a biomicroscope before the Corvis ST test, and confirmed the absence of exclusion criteria, such as the risk of eyeball rupture. The examiners performed the Corvis ST test as follows: the eye was positioned in front of the system at a distance of 11 mm between the corneal apex and the air tube. When the eye was aligned and the Scheimpflug image was in focus, the air puff was automatically released and the cornea was imaged during the deformation event.
The authors recorded the central corneal thickness measured by the Corvis ST. The authors found that upon release of the air puff, the eyeball itself moves backward a little, and after the cornea returns to its original contour, the eyeball moves forward again (Fig. 1, Additional file 1: Video S1). The new analysis software (version 1.5r1902) was used to measure whole eye movement [21, 23].

Whole eye movement during Corvis test. The movies showed that when the air puff was released (a), the cornea became concave (b) and the eyeball moved backward a little. After maximal deformation of the cornea (c), the corneal deformation decreased (D), and when the cornea returned to its original contour (e), the eyeball moved forward again (f)
Additional file 1: Movie S1. Eyeball displacement during an air puff. This movie showed that when the air puff was released, the cornea became concave and the eyeball moved backward a little. After maximal deformation of the cornea, the corneal deformation decreased, and when the cornea returned to its original contour, the eyeball moved forward again. (WMV 799 kb)
In the patients with Graves ophthalmopathy, the examiners performed exophthalmometry using a Hertel Exophthalmometer (K-0161, Inami, Fukuoka, Japan) and an author classified Graves’s ophthalmopathy severity according to EUGOGO [22] and assessed activity according to Clinical Activity Score (CAS) [24] for each severity subgroup. One experienced oculoplastics specialist (YSW) classified the patients. The cross-sectional area of extraocular muscle in the orbit by CT was calculated. Among the 28 patients with Graves’s ophthalmopathy, 21 underwent orbit CT scans. A coronal slice 6 mm behind the posterior pole was selected and the cross-sectional area of the orbit and four rectus muscles were measured. Next, the cross sectional area (%) of the four rectus muscles in the orbit was calculated according to the study by Kim et al. [25].
Statistical analyses
The mean and standard deviation of WEM in the normal group were calculated. In the normal group, a Kolmogorov-Smirnov one-sample test was applied to evaluate the normality of the distribution of WEM measurements. A non-parametric Spearman correlation test was used to examine the relation between age and WEM in the normal group. A t-test was used to compare WEM between male and female in the normal group. Age (Mann-Whitney U-test), gender (Fisher’s exact test), central corneal thickness (Mann-Whitney U-test), and WEM (Mann-Whitney U-test) between the normal group and patients with Graves ophthalmopathy were compared. In the patients with Graves ophthalmopathy, the partial correlation coefficient adjusted for age and gender was calculated to analyze the correlation between exopthalmometry and WEM. Same analysis was repeated for the correlation between and the cross sectional area (%) of the extraocular muscles in the orbit CT and WEM. The mean WEM values were compared among mild, moderate to severe and sight-threatening groups by analysis of variance (ANOVA). The authors used SPSS 18.0 for statistical analysis and considered p < 0.05 to indicate statistical significance.
Results
Patient characteristics
Table 1 shows the demographics and characteristics of the 44 eyes from the 44 normal subjects and the 28 eyes of the 28 patients with Graves ophthalmopathy.
Whole eye movement
Figure 2 shows the distribution of WEM in the normal subjects and Graves ophthalmopathy group. The mean WEM was 0.314 ± 0.083 mm (range, 0.174–0.492 mm) in the normal subjects and the values were fairly normally distributed (P = 0.200; Fig. 2) based on the Kolmogorov-Smirnov one-sample test. In the Graves ophthalmopathy group, the mean WEM was 0.227 ± 0.079 mm (range, 0.110–0.429 mm). WEM was significantly smaller in the Graves ophthalmopathy group compared with the normal group (Mann Whitney U-test, p = 0.000).

The distribution of whole eye movement (WEM) in the normal subjects and Graves ophthalmopathy group. The mean WEM was 0.314 ± 0.083 mm (range, 0.174–0.492 mm) in the normal subjects and the values were fairly normally distributed (P = 0.200) based on the Kolmogorov-Smirnov one-sample test. In the Graves ophthalmopathy group, the mean WEM was 0.227 ± 0.079 mm (range, 0.110–0.429 mm). WEM was significantly smaller in the Graves ophthalmopathy group compared with the normal group (Mann Whitney U-test, p = 0.000)
Relationship with age and gender
In the normal group, WEM was significantly positively correlated with age (Spearman correlation coefficient r = 0.531, p = 0.000, Fig. 3). Mean age of the 14 normal male subjects was 49.2 ± 20.0 years and mean age of 30 normal female subjects was 57.3 ± 16.5 years, with no significant difference between them (u-test p = 0.262). WEM in the male was 0.277 ± 0.076 mm and that in the female was 0.331 ± 0.081 mm (u-test, p = 0.045) (Fig. 4). In the Graves ophthalmopathy group, WEM was 0.198 ± 0.081 mm in the male and 0.237 ± 0.077 mm in the female (u-test, p = 0.288).

The correlation between eyeball displacement and age in the normal group and Graves ophthalmopathy group. In the normal group, whole eye movement was significantly positively correlated with age (Spearman correlation coefficient r = 0.531, p = 0.000)

Comparison of mean eyeball displacement between male and female in healthy subjects and Graves ophthalmopathy group. Whole eye movement (WEM) in the male was 0.277 ± 0.076 mm and that in the female was 0.331 ± 0.081 mm (u-test, p = 0.045). In the Graves ophthalmopathy group, WEM was 0.198 ± 0.081 mm in the male and 0.237 ± 0.077 mm in the female (u-test, p = 0.288)
Graves ophthalmopathy
Figure 5 shows the correlation between WEM and exopthalmometry in the 28 eyes of the 28 Graves ophthalmopathy patients. WEM tended to decrease as exophthalmometry increased, but the correlation was not statistically significant after adjusting for age and gender (R = 0.083, p = 0.688); Fig. 5). The mean WEM was 0.233 ± 0.077 mm in mild severity group, 0.235 ± 0.080 mm in moderate to severe group and 0.227 ± 0.079 mm in sight –threatening group. There was no significant differences among the groups (ANOVA, p = 0.244). Figure 6 shows mean WEM versus CAS in each severity subgroups.

The correlation between whole eye movement (WEM) and exopthalmometry in the 28 eyes of the 28 Graves ophthalmopathy patients. WEM tended to decrease as exophthalmometry increased, but the correlation was not statistically significant after adjusting for age and gender (R = 0.083, p = 0.688)

Whole eye movement (WEM) versus clinical activity score (CAS) in each severity subgroups. The mean WEM was 0.233 ± 0.077 mm in mild severity group, 0.235 ± 0.080 mm in moderate to severe group and 0.227 ± 0.079 mm in sight –threatening group. There was no significant differences between the groups (ANOVA, p = 0.244)
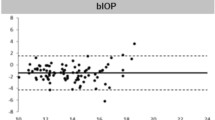
In the 21 Graves ophthalmopathy patients examined by orbit CT, after adjusting for age and gender, WEM significantly decreased as the cross sectional area (%) of the extraocular muscles in the orbit increased (R = − 0.464, p = 0.045; Fig. 7).

The correlation between whole eye movement (WEM) and the cross sectional area (%) of the extraocular muscles in the 21 Graves ophthalmopathy patients examined by orbit computed tomography (CT). After adjusting for age and gender, WEM significantly decreased as the cross sectional area (%) of the extraocular muscles in the orbit increased (R = − 0.464, p = 0.045)
Discussions
The Corvis ST is a diagnostic instrument originally developed to measure biomechanical response to an air puff by analyzing the shape of the deformation in the images, as well as the timing of specific events. By viewing the ultra-high speed video by the Corvis ST, the authors observed WEM induced by the air puff release and therefore evaluated whether the Corvis ST could be also used to assess the biomechanical parameters of the orbital soft tissue. WEM induced by the air puff increased with increasing age and was greater in female than in male. WEM was smaller in patients with Graves ophthalmopathy than in normal subjects.
Recently clinical research papers on WEM have been published. Vinciguerra et al. measured WEM in healthy subjects and obtained normative data. They found that WEM increases with age [21]. This is consistent with the results of the present study. WEM was used to develop a new index for keratoconus detection [23, 26, 27]. WEM was also used in glaucoma research. Jung et al. found that unadjusted WEM was smaller in glaucoma group compared to normal group [28]. Aoki et al. measured WEM in open angle glaucoma and obtained the relationship between WEM and axial length of eyeball [29].
In the present study, WEM in patients with Graves ophthalmopathy was smaller than that in normal subjects. In other words, orbital soft tissue is stiffer and less compliant in Graves ophthalmopathy patients than in normal subjects. It means a retrobulbar resistance as a clinical sign in Graves ophthalmopathy. A previous study reported that orbital compliance is decreased in Graves ophthalmopathy patients [30]. In that research, greater force was required to push the eyeball the same distance in Graves ophthalmopathy patients as in normal controls. The mean forward force for 3 mm retropulsion of the eye was 70.1 g in normal subjects, 102.5 g in compressive optic neuropathy, and 56.7 g in stable Graves ophthalmopathy. In Graves ophthalmopathy patients, the orbital fat becomes fibrotic [31] and the extraocular muscle accumulates mucopolysaccharides and become larger. These factors are thought to increase the stiffness of orbital soft tissue.
Recently, Vellara et al. [32] used the Corvis ST to assess the orbital compliance in patients with thyroid eye disease (TED) and compared the results with a cohort of healthy subjects. They investigated the feasibility of using measurements derived from the Corvis ST as a diagnostic tool for TED. They used Matlab (Natick, VA, V.8.4.0.150421 (R2014b)) for measurement of maximum orbital deformation (MOD). They measured MOD of 20 eyes of 20 patients with TED and 152 eyes of 152 healthy subjects using Corvis ST. The mean MOD was 0.16 ± 0.04 mm and 0.25 ± 0.05 mm for TED and healthy eyes, respectively (p < 0.001). The MOD values are smaller than WEM in the present study. The authors think that the difference of ethnicity between two studies might cause the different results. Eyes included in the study (20 eyes with TED and 152 healthy eyes) were incorporated into a receiver operating characteristic (ROC) analysis. A cut-off value of 0.18 mm yielded 92% sensitivity and 84% specificity.
Their research and ours have something in common. Eyeball displacement using Corvis ST was compared between patients with Graves ophthalmopathy and healthy subjects. These eyeball displacement was interpreted as an orbital compliance. The authors have some advances over their research. First, the authors analyzed correlation between WEM and clinical parameters such as exophalmometry, disease severity and activity, and the cross sectional area (%) of the extraocular muscles in the orbit. Second, the authors measured WEM using Corvis software instead of Matlab, so clinical ophthalmologists can easily use this method; Third, there is no significant difference of age and ethnicity between two groups unlike their research. Fourth, the authors obtained distribution of WEM (histrogram) in healthy subjects.
Leszczynska et al. investigated orbital biomechanical properties in patients with thyroid orbitopathy and in age and gender-matched healthy subjects using the Corvis-ST. [33] Whole eye movement length (WEMl) were measured in 39 patients with thyroid orbitopathy (= group I) and in 33 age- and gender-matched healthy subjects (= group II) using the CST. There was a statistically significant difference between both groups in mean WEMl (207 ± 57 vs. 322 ± 50 μm) (p = 0.01). WEMl values of each group were similar to our results and the mean WEMI of thyroid orbitopathy group was smaller than that of healthy group like the present study.
Eyeball displacement measured using the Corvis ST is true eyeball movement and not just axial shortening and elongation of eyeball induced by the air puff based on the fact that the eyeballs moved forward again after returning to their original corneal contour (S1Video). This finding is consistent with the findings of previous studies [21, 23, 26,27,28,29, 33, 34].
In the normal subject group, mean WEM was 0.314 ± 0.083 mm, which was 57.5% of mean central corneal thickness (546 μm). Mean orbital depth is 45–55 mm [35], so mean eyeball displacement was just 0.6% of the orbital depth. In normal adults, the mean volume of the orbit is 29.7 ml and the volume of the eyeball is 6.5 ml. Therefore, the volume of the orbit that does not include the eyeball is 23.2 ml [35]. Fat is the most predominant tissue in the orbit. Most of the rest of the orbit comprises extraocular muscle. Therefore, WEM measured by the Corvis ST represents the biomechanical parameters of 23.2 ml of fat and extraocular muscle in the orbit.
Eyeball displacement appears to decrease as exophthalmos increases, but after adjusting for age and gender, the authors found no significant correlation (R = 0.083, p = 0.688). WEM showed no significant differences among mild, moderate to severe and sight-threatening groups (ANOVA, p = 0.244). In 21 patients with Graves ophthalmopathy examined by orbital CT, WEM decreased as the cross sectional area (%) of the extraocular muscles in the orbit increased, after adjusting for age and gender (R = − 0.461, p = 0.047). That is, as the cross sectional area (%) of the extraocular muscles in the orbit increases, the orbit becomes stiffer and eyeball displacement decreases.
How can the biomechanical parameters of orbital soft tissue measured using the Corvis ST be applied clinically? The factors that contribute to WEM may be the state of the orbital fat and extraocular muscles, and the presence or absence of blow out fracture. In the present study, WEM decreased as the cross sectional area (%) of the extraocular muscles increased in patients with Graves ophthalmopathy. These findings indicate that WEM can be used as a measure to monitor orbital soft tissue stiffness resulting from Graves ophthalmopathy. Changes in the extraocular muscle can be examined by CT. CT scanning cannot be performed frequently, however, due to both the risk of radiation and the high cost. The Corvis ST is a simple and easy-to-perform method for evaluating orbital soft tissue and the progression of Graves ophthalmopathy during follow-up.
Advantages of using the Corvis ST to quantify the biomechanical parameters of the orbital soft tissue include its easy application and lack of discomfort for the subjects. And a recent study demonstrated good repeatability [36]. But, it is unclear whether eyeball displacement effectively represents the orbital biomechanical parameters because WEM is only 0.6% of the orbital depth.
Conclusions
In conclusion, the authors used the Corvis ST, which was developed to measure the biomechanical parameters of the cornea, to quantify the biomechanical parameters of the orbital soft tissue.
Abbreviations
- ANOVA:
-
Analysis of variance
- CAS:
-
Clinical Activity Score
- CT:
-
Computer tomography
- EUGOGO:
-
European Group on Graves’ orbitopathy
- MOD:
-
Maximum orbital deformation
- ROC:
-
Receiver operating characteristic
- TED:
-
Thyroid eye disease
- WEM:
-
Whole eye movement
- WEMl:
-
Whole eye movement length
References
Asaoka R, Nakakura S, Tabuchi H, Murata H, Nakao Y, Ihara N, Rimayanti U, Aihara M, Kiuchi Y: The relationship between Corvis ST tonometry measured corneal parameters and intraocular pressure Corneal Thickness and Corneal Curvature, PLoS One 2015, 10(10):e0140385. doi: 10.0141371/journal.pone.0140385. eCollection 0142015.
Hon Y, Lam AK. Corneal deformation measurement using Scheimpflug noncontact tonometry. Optom Vis Sci. 2013;90(1):e1–8. https://doi.org/10.1097/OPX.1090b1013e318279eb318287.
Hong J, Xu J, Wei A, Deng SX, Cui X, Yu X, Sun X. A new tonometer--the Corvis ST tonometer: clinical comparison with noncontact and Goldmann applanation tonometers. Invest Ophthalmol Vis Sci. 2013;54(1):659–65. https://doi.org/10.1167/iovs.1112-10984.
Huseynova T, GOt W, Roberts C, Krueger RR, Tomita M. Corneal biomechanics as a function of intraocular pressure and pachymetry by dynamic infrared signal and Scheimpflug imaging analysis in normal eyes. Am J Ophthalmol. 2014;157(4):885–93.
Nemeth G, Hassan Z, Csutak A, Szalai E, Berta A, Modis L Jr. Repeatability of ocular biomechanical data measurements with a Scheimpflug-based noncontact device on normal corneas. J Refract Surg. 2013;29(8):558–63. https://doi.org/10.3928/1081597X-20130719-20130706.
Pinero DP, Alcon N. In vivo characterization of corneal biomechanics. J Cataract Refract Surg. 2014;40(6):870–87. https://doi.org/10.1016/j.jcrs.2014.1003.1021.
Ali NQ, Patel DV, McGhee CN. Biomechanical responses of healthy and keratoconic corneas measured using a noncontact scheimpflug-based tonometer. Invest Ophthalmol Vis Sci. 2014;55(6):3651–9. https://doi.org/10.1167/iovs.3613-13715.
Bak-Nielsen S, Pedersen IB, Ivarsen A, Hjortdal J. Dynamic Scheimpflug-based assessment of keratoconus and the effects of corneal cross-linking. J Refract Surg. 2014;30(6):408–14. https://doi.org/10.3928/1081597X-20140513-20140502.
Steinberg J, Katz T, Lucke K, Frings A, Druchkiv V, Linke SJ. Screening for keratoconus with new dynamic biomechanical in vivo Scheimpflug analyses. Cornea. 2015;34(11):1404–12. https://doi.org/10.1097/ICO.0000000000000598.
Tian L, Ko MW, Wang LK, Zhang JY, Li TJ, Huang YF, Zheng YP: Assessment of ocular biomechanics using dynamic ultra high-speed Scheimpflug imaging in keratoconic and normal eyes. J Refract Surg 2014, 30(11):785–791. doi: https://doi.org/10.3928/1081597X-20140930-20140901. Epub 20142014 Oct 20140937.
Chen X, Stojanovic A, Hua Y, Eidet JR, Hu D, Wang J, Utheim TP: Reliability of corneal dynamic scheimpflug analyser measurements in virgin and post-PRK eyes. PLoS One 2014, 9(10):e109577. doi: 10.101371/journal.pone.0109577. eCollection 0102014.
Pedersen IB, Bak-Nielsen S, Vestergaard AH, Ivarsen A, Hjortdal J: Corneal biomechanical properties after LASIK, ReLEx flex, and ReLEx smile by Scheimpflug-based dynamic tonometry. Graefes Arch Clin Exp Ophthalmol 2014, 252(8):1329–1335. doi: 13https://doi.org/10.1007/s00417-00014-02667-00416. Epub 02014 May 00427.
Sefat SM, Wiltfang R, Bechmann M, Mayer WJ, Kampik A, Kook D. Evaluation of changes in human corneas after femtosecond laser-assisted LASIK and small-incision Lenticule extraction (SMILE) using non-contact tonometry and ultra-high-speed camera (Corvis ST). Curr Eye Res. 2015;10:1–6.
Shen Y, Chen Z, Knorz MC, Li M, Zhao J, Zhou X. Comparison of corneal deformation parameters after SMILE, LASEK, and femtosecond laser-assisted LASIK. J Refract Surg. 2014;30(5):310–8.
Shen Y, Zhao J, Yao P, Miao H, Niu L, Wang X, Zhou X: Changes in corneal deformation parameters after lenticule creation and extraction during small incision lenticule extraction (SMILE) procedure. PLoS One 2014, 9(8):e103893. doi: 10.101371/journal.pone.0103893. eCollection 0102014.
Lee R, Chang RT, Wong IY, Lai JS, Lee JW, Singh K. Novel parameter of corneal biomechanics that differentiate Normals from Glaucoma. J Glaucoma. 2015;16:16.
Reznicek L, Muth D, Kampik A, Neubauer AS, Hirneiss C: Evaluation of a novel Scheimpflug-based non-contact tonometer in healthy subjects and patients with ocular hypertension and glaucoma. Br J Ophthalmol 2013, 97(11):1410–1414. doi: https://doi.org/10.1136/bjophthalmol-2013-303400. Epub 302013 Aug 303422.
Salvetat ML, Zeppieri M, Tosoni C, Felletti M, Grasso L, Brusini P. Corneal deformation parameters provided by the Corvis-ST Pachy-tonometer in healthy subjects and Glaucoma patients. J Glaucoma. 2015;24(8):568–74. https://doi.org/10.1097/IJG.0000000000000133.
Tian L, Wang D, Wu Y, Meng X, Chen B, Ge M, Huang Y. Corneal biomechanical characteristics measured by the CorVis Scheimpflug technology in eyes with primary open-angle glaucoma and normal eyes. Acta Ophthalmol. 2015;1(10):12672.
Wang W, Du S, Zhang X. Corneal deformation response in patients with primary open-angle Glaucoma and in healthy subjects analyzed by Corvis ST. Invest Ophthalmol Vis Sci. 2015;56(9):5557–65. https://doi.org/10.1167/iovs.5515-16926.
Vinciguerra R, Elsheikh A, Roberts CJ, Ambrosio R, Jr., Kang DS, Lopes BT, Morenghi E, Azzolini C, Vinciguerra P: Influence of Pachymetry and intraocular pressure on dynamic corneal response parameters in healthy patients, J Refract Surg 2016, 32(8):550–561.
Bartalena L, Baldeschi L, Dickinson A, Eckstein A, Kendall-Taylor P, Marcocci C, Mourits M, Perros P, Boboridis K, Boschi A, et al. Consensus statement of the European group on Graves' orbitopathy (EUGOGO) on management of GO. Eur J Endocrinol. 2008;158(3):273–85.
Roberts CJ, Mahmoud AM, Bons JP, Hossain A, Elsheikh A, Vinciguerra R, Vinciguerra P, Ambrosio R Jr. Introduction of two novel stiffness parameters and interpretation of air puff-induced biomechanical deformation parameters with a dynamic Scheimpflug analyzer. J Refract Surg. 2017;33(4):266–73.
Mourits MP, Koornneef L, Wiersinga WM, Prummel MF, Berghout A, van der Gaag R. Clinical criteria for the assessment of disease activity in Graves' ophthalmopathy: a novel approach. Br J Ophthalmol. 1989;73(8):639–44.
Kim HC, Yoon SW, Lew H. Usefulness of the ratio of orbital fat to total orbit area in mild-to-moderate thyroid-associated ophthalmopathy. Br J Radiol. 2015;88(1053):20150164.
Vinciguerra R, Ambrosio R Jr, Elsheikh A, Roberts CJ, Lopes B, Morenghi E, Azzolini C, Vinciguerra P. Detection of keratoconus with a new biomechanical index. J Refract Surg. 2016;32(12):803–10.
Francis M, Pahuja N, Shroff R, Gowda R, Matalia H, Shetty R, Remington Nelson EJ, Sinha Roy A. Waveform analysis of deformation amplitude and deflection amplitude in normal, suspect, and keratoconic eyes. J Cataract Refract Surg. 2017;43(10):1271–80.
Jung Y, Park HL, Yang HJ, Park CK. Characteristics of corneal biomechanical responses detected by a non-contact scheimpflug-based tonometer in eyes with glaucoma. Acta Ophthalmol. 2017;95(7):e556–63.
Aoki S, Murata H, Matsuura M, Fujino Y, Nakakura S, Nakao Y, Kiuchi Y, Asaoka R. The effect of air pulse-driven whole eye motion on the association between corneal hysteresis and glaucomatous visual field progression. Sci Rep. 2018;8(1):2969.
Frueh BR. Graves’ eye disease: orbital compliance and other physical measurements. Trans Am Ophthalmol Soc. 1984;82:492–598.
Dik WA, Virakul S, van Steensel L. Current perspectives on the role of orbital fibroblasts in the pathogenesis of Graves’ ophthalmopathy. Exp Eye Res. 2016;142:83–91.
Vellara HR, Hart R, Gokul A, McGhee CNJ, Patel DV. In vivo ocular biomechanical compliance in thyroid eye disease. Br J Ophthalmol. 2017;101(8):1076–9.
Leszczynska A, Moehler K, Spoerl E, Ramm L, Herber R, Pillunat LE, Terai N. Measurement of orbital biomechanical properties in patients with thyroid Orbitopathy using the dynamic Scheimpflug analyzer (Corvis ST). Curr Eye Res. 2018;43(3):289–92.
Vellara HR, Ali NQ, Gokul A, Turuwhenua J, Patel DV, McGhee CN. Quantitative analysis of corneal energy dissipation and corneal and orbital deformation in response to an air-pulse in healthy eyes. Invest Ophthalmol Vis Sci. 2015;56(11):6941–7.
Deborah D, Sherman CNB, Bradley N, Lemke. In: TDJ D, Edward A, editors. Duane’s Clinical Ophthalmology, vol. 2. Philadelphia: Lippincott Williams & Wilkins; 2012.
Vellara HR, Ali NQ, Gokul A, Turuwhenua J, Patel DV, McGhee CN. Quantitative analysis of corneal energy dissipation and corneal and orbital deformation in response to an air-pulse in healthy eyes. Invest Ophthalmol Vis Sci. 2015;56(11):6941–7. https://doi.org/10.1167/iovs.6915-17396.
Acknowledgements
Not applicable.
Funding
This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HI17C0659) and Basic Science Research Program through the National Research Foundation of Korea(NRF) funded by the Ministry of Education(No. 2017R1A1A2A10000681). The funds were used in the design of the study, the collection, analysis, and interpretation of data and in writing the manuscript.
Availability of data and materials
For more information of the study, please contact the corresponding author.
Author information
Authors and Affiliations
Contributions
HHS, KEC, KMS and YSW participated in the design of this study, HHS, YSW carried out the study. HHS, KEC, KMS and YSW performed the statistical analysis. HHS, KEC, KMS and YSW drafted the manuscript. HHS, KEC, KMS and YSW performed manuscript review. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This retrospective study adhered to the tenets of the Declaration of Helsinki and received institutional review board (IRB) approval from Seoul St. Mary’s Hospital for the analysis of their medical records. The need for consent was waived by IRB (name of IRB: CMC IRB).
Consent for publication
Not applicable.
Competing interests
HHS is a member of the editorial board (Associate Editor) of BMC ophthalmology. The other authors declare that they have no competing interests. The authors declare that they have no financial competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Hwang, H., Kim, E., Kim, M. et al. A novel method for quantifying the biomechanical parameters of orbital soft tissue using a corneal dynamic scheimpflug analyser: a retrospective study. BMC Ophthalmol 19, 53 (2019). https://doi.org/10.1186/s12886-019-1064-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12886-019-1064-7