
Abstract
Background
we conducted our meta-analysis of published studies to assess existing evidence about the efficacy and safety of vitrectomy with ILM peeling vs. that of vitrectomy with no ILM peeling for Macular hole-induced retinal detachment.
Methods
Databases, including Pubmed, Cochrane Library, Ovid, Web of Science, Wanfang and CNKI, were searched to identify studies comparing outcomes following vitrectomy with ILM peeling and that with no ILM peeling for macular hole-induced retinal detachment. The meta-analysis was performed by RevMan 5.1.
Results
Six comparative studies comprising 180 eyes were identified. It was indicated that the rate of retinal reattachment (Odds ratio (OR) = 3.03, 95 % Confidence interval (CI):1.35 to 6.78; P = 0.007) and macular hole closure (OR = 6.74, 95 % CI:3.26 to 13.93; P < 0.001) after initial surgery was higher and the rate of recurrent retinal detachment (OR = 0.08, 95 % CI:0.02 to 0.30; P = 0.0002) was lower in the group of vitrectomy with ILM peeling than that in the group of vitrectomy with no ILM peeling. However, the improved BCVA (Weighted mean difference (WMD) = 0.14, 95 % CI: −0.20 to 0.47; P = 0.42) and the rate of postoperative complications were similar between the two groups.
Conclusion
Vitrectomy with internal limiting membrane peeling is an efficient and safe procedure for macular hole-induced retinal detachment.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
Macular hole-induced retinal detachment (MHRD), also named retinal detachments resulting from macular hole is usually a vision-threatening complication to highly myopic eyes, which is more common in Asian adult population [1]. In the past years, MHRD was presumed as a rare disease according to the paucity of literatures. But with the OCT routinely used to evaluate RDs preoperatively, macular holes were found more frequently in RD [2]. The important causative factors of MHRD might be related to the tangential traction caused by a premacular membrane or fibrosis and the inverse traction caused by the posterior staphyloma [3–5]. More recent analysis by OCT showed that tangential traction of the vitreous cortex behind the vitreous pocket contributed to the development of MHRD [3–6]. In highly myopic eyes, the elongation of the axial length of the eye and the development of a posterior staphyloma result in thinning of the retina and choroid, which also leads to the development of MHRD [3, 7].
Since the early 1990s, pars plana vitrectomy, gas endotamponade, and epiretinal membrane removal had been used in retinal detachment related to a macular hole [8–13]. However, the primary success rate of retinal reattachment (43.9–75 %) was not as high as expected and the visual outcomes in some cases were poor [11–15]. To facilitate macular hole closure, removal of the internal limiting membrane (ILM) had been used a surgical adjunct primarily to counter surface traction and promote the closure of the macular hole in the past fifteen years [16–18]. It was proposed that removing the internal limiting membrane (ILM) ensures the complete removal of any overlying ERM adjacent to an indiopathic macular hole and the vitreous traction on the retina [19–24].
Although an increasing number of PPV with ILM peeling has been reported treating retinal detachments resulting from a macular hole with better retinal reattachment and visual acuity [25–29], ILM peeling has been shown to lead to small but noticeable anatomic and functional changes in the peeled area of the retina, which should also be considered in the risk–benefit analysis. There is still debate among vitreoretinal surgeons about whether and when to peel the ILM in MHRD cases. The removal of the ILM may increase the incidence of postoperative complications, including the development of a MH and a MHRD [21]. Moreover, some functional outcomes such as postoperative scotomas and dissociated optic nerve fibre layer (DONFL) should also be considered in the risk–benefit analysis [30, 31]. Most studies have been limited by small sample size and a single institution design, so consensus has not been reached as to the necessity of ILM peeling in MHRD. To overcome these limitations, we conducted this meta-analysis of published studies to assess existing evidence about the efficacy and safety of vitrectomy with ILM peeling vs that of vitrectomy with no ILM peeling for macular hole-induced retinal detachment.
Methods
Literature search
A literature search was performed to identify all relevant prospective or retrospective studies that compared outcomes following vitrectomy with ILM peeling and that with no ILM peeling for macular hole-induced retinal detachment. The Pubmed, Cochrane Library, Ovid, Web of Science, Wanfang and CNKI databases were searched systematically for all articles published before June 2014. The following terms were used for the search: “retinal detachment”, “macular hole”, “myopic”, “macular hole-induced retinal detachment”, “internal limiting membrane peeling” and “vitrectomy”. Only studies in the English or Chinese language were considered for inclusion. Reference lists of all retrieved articles were manually searched to broaden the search. All abstracts, studies and citations scanned were reviewed.
Data extraction and assessment of study quality
Two reviewers independently extracted the data from each study. The following information was extracted from each study: first author, year of publication, study design, inclusion and exclusion criteria, quality of study, study population characteristics, number of subjects in vitrectomy with ILM peeling group and vitrectomy with no ILM peeling group, baseline characteristics of the patients such as duration of symptoms, refractive error, axial length and preoperative BCVA in each group, postoperative data. Discrepancies between the two reviewers were resolved by discussion and consensus with the corresponding author.
Since most of our selected studies were non-randomized surgical research, the quality of each included trial was accessed using methodological index for non-randomized studies (MINORS) [32]. This validated index involves 12 items, the first eight items specifically designed for non-comparative studies and the remaining four items applied to comparative studies. Items are scored as 0 (not reported), 1 (reported but inadequate) and 2 (reported and adequate). The maximum ideal score for comparative studies is 24. It is important to appreciate that such scoring system was use in the quality comparison of nonrandomized research because other quality grading according to levels of evidence does not provide adequate stratification [32]. We evaluated each study with a quality score and the score of 12 or more indicated a higher quality study.
Criteria for inclusion and exclusion
To be included in this meta-analysis, studies had to fulfill the following criteria: (1) compare outcomes of patients receiving vitrectomy with ILM peeling with those of patients receiving vitrectomy with no ILM peeling for macular hole-induced retinal detachment; (2) report on at least one of the outcome measures mentioned below; and (3) if multiple studies were reported by the same institution and/or authors, either the best quality or the most recent publication was included in our analysis.
Noncomparative studies were excluded. Abstracts, letters, editorials and experts opinions and reviews without original data were excluded. The following studies or data were also excluded: (1) studies included cases with both MHs and peripheral breaks; (2) the outcomes and parameters of patients were not clearly reported; (3) significant differences existed in duration of symptoms, refractive error, axial length and preoperative BCVA between vitrectomy with ILM peeling group and vitrectomy with no ILM peeling group; (4) If end points were not comparable, (5) if it was impossible to extract or calculate appropriate data from the published results.
Outcomes of interest
The following outcomes were used to compare between the group of vitrectomy with ILM peeling and that of vitrectomy with no ILM peeling. (1) data of efficacy, including rate of retinal reattachment after initial surgery, rate of macular hole closure after initial surgery, improved BCVA and rate of recurrent retinal detachment; (2) data of safety, the rate of postoperative complication such as retinal breaks, ERM (epiretinal membrane), cataract and intraocular pressure rise.
Statistical analysis
We used the Cochrane Collaboration’s Review Manager Software (RevMan Version 5.1) for the data analysis. Dichotomous variables were analyzed by using estimation of odds ratios with a 95 % confidence interval (95 % CIs) and continuous variables using weighted mean difference (WMD) with 95 % CIs. For studies that presented continuous data such as median and range values, we converted these data to the mean and standard deviation by using the method of Hozo et al. [33]. Thus all continuous data were standardized for analysis.
The homogeneous test of effects was performed using χ2 test, with P < 0.05 and I2 > 50 % indicating significant heterogeneity. A fixed-effects model was used when no heterogeneity was detected, which meant that there was no variances among studies. If any heterogeneity existed, a random-effects model, which leads to wider CIs than the fixed-effects model, was used for the meta-analysis. Presence of publication bias was evaluated qualitatively by a funnel plot. We also systematically describe and assess the results that are not appropriate to be combined in the meta-analysis.
Results
Selection of studies
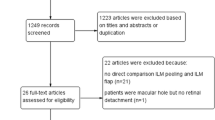
The initial search yielded 417 relevant studies. But most of these studies were not suitable for our analysis because they included duplicates, lab or animal studies, case reports, review and other study subjects irrelevant to our title. After screening all titles, abstracts and full-test, 411 publications were excluded according to the selection criteria and a total of 6 studies [28, 34–38] were retrieved for more detailed evaluation. The search process is illustrated in Fig. 1.

Flow diagram of the trial selection process
Characteristics and baseline of the included studies
In total 6 studies [28, 34–38], 180 eyes (92 eyes with ILM peeling, 88 eyes with no ILM peeling) were included with retinal detachment resulting from macular hole. The characteristics of these 6 studies are summarized in Table 1. None of the studies were randomized controlled trials. Five studies [28, 35–38] were conducted in China, one in Japan [34]. The sample size of each study varied from 11 to 52. All the studies included in the meta-analysis were considerably well conducted and had balanced populations.
The baseline characteristics of each included trial, such as duration of symptoms, refractive error, axial length and preoperative BCVA were found to be equivalent between the group of vitrectomy with ILM peeling and the group of vitrectomy with no ILM peeling. Meanwhile, analysis of the pooled data revealed that the two groups did not differ significantly and there was no statistical heterogeneity between the studies (Table 2).
Quality assessment
The methodologic quality of the included trials is explained comprehensively in Table 3. In general, the quality of the studies was moderate to good (all >12). All data were analyzed in accordance with intention-to-treat principle.
Meta-analysis of efficacy outcomes
The pooled data from 5 studies including 128 eyes in the meta-analysis indicated that the group of vitrectomy with ILM peeling had higher rate of retinal reattachment after initial surgery than the group of vitrectomy with no ILM peeling (OR = 3.03, 95 % CI: 1.35 to 6.78; P = 0.007) and there was no statistical heterogeneity between the two groups (heterogeneity P = 0.26, I2 = 25 %) (Fig. 2).

A forest plot showing the rate of retinal reattachment after initial surgery between the group of vitrectomy with ILM peeling and the group of vitrectomy with no ILM peeling for retinal detachments resulting from a macular hole. VT = vitrectomy, ILMP = internal limiting membrane peeling
The rate of macular hole closure after initial surgery was reported in 6 studies including 180 eyes. There was no statistical heterogeneity between the studies (heterogeneity P = 0.81, I2 = 0 %). By using a fixed effects model, it was indicated that the rate of macular hole closure after initial surgery was higher in the group of vitrectomy with ILM peeling than that in the group of vitrectomy with no ILM peeling (OR = 6.74, 95 % CI: 3.26 to 13.93; P < 0.001) (Fig. 3).

A forest plot showing the rate of macular hole closure after initial surgery between the group of vitrectomy with ILM peeling and the group of vitrectomy with no ILM peeling for retinal detachments resulting from a macular hole. VT = vitrectomy, ILMP = internal limiting membrane peeling
In 3 studies, it was indicated that there was no significant difference in the improvement of BCVA after surgery between the two groups. Analysis of the extracted data revealed that there was statistical heterogeneity between the studies (heterogeneity P = 0.03, I2 = 72 %), which may have resulted from variations in the method used to measure the visual acuity and the data conversion from other unit to logMAR. Patients undergoing vitrectomy with ILM peeling experience a similar improvement of BCVA of those undergoing vitrectomy with no ILM peeling. The two groups did not differ significantly in the regard (WMD = 0.14, 95 % CI: −0.20 to 0.47; P = 0.42) using the random effects model (Fig. 4).

A forest plot showing the improvement of BCVA after surgery between the group of vitrectomy with ILM peeling and the group of vitrectomy with no ILM peeling for retinal detachments resulting from a macular hole. VT = vitrectomy, ILMP = internal limiting membrane peeling
The pooled data from 3 studies including 102 eyes in the meta-analysis indicated that the group of vitrectomy with ILM peeling had lower rate of recurrent retinal detachment after initial surgery than the group of vitrectomy with no ILM peeling (OR = 0.08, 95 % CI: 0.02 to 0.30; P = 0.0002) and there was no statistical heterogeneity between the two groups (heterogeneity P = 0.87, I2 = 0 %) (Fig. 5).

A forest plot showing the rate of recurrent retinal detachment after initial surgery between the group of vitrectomy with ILM peeling and the group of vitrectomy with no ILM peeling for retinal detachments resulting from a macular hole. VT = vitrectomy, ILMP = internal limiting membrane peeling
Meta-analysis of safety outcomes
Five studies reported postoperative complications such as retinal breaks, ERM (epiretinal membrane), cataract and intraocular pressure rise. As is shown in Table 4, we analyzed the pooled data of complications respectively and revealed that the two groups did not differ significantly in the regard of using the fixed effects model. It is important to note that heterogeneity testing indicated no significant heterogeneity between the two groups.
Testing for publication bias
A funnel plot of the macular hole closure rate in including studies demonstrated symmetry, which indicated no serious publication bias (Fig. 6).

A funnel plot for the result from the studies comparing the rate of retinal reattachment showing no significant publication bias. SE = standard error, OR = odds ratio
Discussion
Gonvers and Machemer [39] first introduced the surgical procedures for treating retinal detachments (RDs) resulting from a macular hole. Since then, pars plana vitrectomy, gas endotamponade, and epiretinal membrane removal has been widely accepted as the treatment for retinal detachment related to a macular hole [8–13]. Despite the universality of pars planavitrectomy for MHRD, the primary success rate of retinal reattachment was not as high as expected. Previous studies on retinal detachment related to high myopia in patients with macular hole have demonstrated that vitreous surgery can lead to anatomic macular hole closure, with the primary anatomic closure rate ranging from 46–75 % [8–15]. Kadonosono et al. first reported ILM peeling with the assistance of indocyanine green and sulfur hexafluoride gas injection for retinal detachment related to high myopia in patients with macular hole with a high reattachment success rate of 91 % [25]. However most studies have been limited by small sample size and a single institution design, consensus has not been reached as to the necessity of ILM peeling in MHRD.
Since macular hole-induced retinal detachment is relatively uncommon, it is unlikely to perform large scale studies or randomized studies to study on the necessity of ILM peeling in it. So we design our meta-analysis to determine the efficacy and safety of ILM peeling in macular hole-induced retinal detachment. In this meta-analysis, we pooled data from 7 studies and examined eight factors associated efficacy and safety: rate of retinal reattachment after initial surgery, rate of macular hole closure after initial surgery, improved BCVA, rate of recurrent retinal detachment and rate of postoperative complication such as retinal breaks, ERM (epiretinal membrane), cataract and intraocular pressure rise.
We realized that the efficacy and safety outcomes were associated with the baseline characteristics of eyes including in studies such as duration of symptoms, refractive error, axial length and preoperative BCVA. So we excluded the studies which existed significant difference in duration of symptoms, refractive error, axial length and preoperative BCVA between the group of vitrectomy with ILM peeling and that of vitrectomy with no ILM peeling. Before we analyzed the outcomes of efficacy and safety, we compared the duration of symptoms, refractive error, axial length and preoperative BCVA between the two groups and found no significant difference. According to this result we consider that the groups have comparability and the conclusion below was reasonable.
Our meta-analysis summarized the efficacy and safety outcomes of ILM peeling in vitrectomy with a total of 113 case eyes and 102 control eyes. The result indicated that the rate of retinal reattachment and macular hole closure after initial surgery was higher and the rate of recurrent retinal detachment was lower in the group of vitrectomy with ILM peeling than that in the group of vitrectomy with no ILM peeling (Figs. 2–3, 5). However, the improved BCVA and the rate of postoperative complications were similar between the two groups (Fig. 4, Table 4).
Macular hole-induced retinal detachment (MHRD) is usually a vision-threatening complication to highly myopic eyes, which is more common in Asian adult population [1]. The important causative factors of MHRD might be related to anterior-posterior traction of the vitreous on the macular area of the retina or fibrosis and the inverse traction caused by the posterior staphyloma [3–5]. Histologic studies of excised posterior vitreous cortex in the eyes with MHRD have shown that the fibrous astrocytes made up the majority of cells, and the cortical vitreous contained abundant newly formed collagen including fibrous long-spacing collagen surrounded by sparsely distribute native vitreous collagen [40]. These findings indicated that the removal of the vitrous cortex should reduce the tangential traction and resolve the myopic traction maculopathy. In highly myopic eyes, the elongation of the axial length of the eye and the development of a posterior staphyloma result in thinning of the retina and choroid, which then leads to the development of MHRD [3, 7]. It was found that the posterior vitreous cortex or a thin ERM was adherent to the detached retina during surgery in all cases [34]. Thus, ILM peeling is considered to ensure the complete removal of the overlying residual vitreous cortex or ERMs and to relieve the tangential traction of residual prefoveal vitreous after posterior vitreous detachment of the contraction of epiretinal cellular constituents adjacent to the macular hole, resulting in closing the macular hole and aiding in the recovery of macular shape [41]. However, it is usually difficult to remove a thin and fragile ERM or posterior vitreous cortex completely from a detached retina. It was supposed that without ILM peeling, the remaining vitreous may act as a scaffold for the epiretinal membrane, thereby exerting traction on both the MH and retina in the posterior pole, thus limiting MH closure or even promoting reopening.
In our meta-analysis, the improved BCVA was not significantly difference between the group of vitrectomy with ILM peeling and the group of vitrectomy with no ILM peeling (Fig. 4). No visual acuity improvement difference are likely explained by the fact that patients whose macular hole had not closed or who developed recurrent retinal detachment after initial surgery in the group of no ILM peeling were ethically allowed to receive second surgery including ILM peeling in clinical study. Thus the outcome of improved BCVA was observed similar in the last data point of follow-up between the two groups [42]. The ILM is the basal lamina of the Müller cells, and the Müller cell cone, which is an inverted cone-shaped zone of specialized Müller cells that form the base of the fovea [43], serves as a plug that binds the photoreceptor cells together in the macula and supports the macula structurally [44]. ILM peeling may decrease the structural support of the macula [21], reduce the amplitude of the local electroretinogram (ERG) [45] and dissociate optic nerve fiber layer [30]. Despite the anatomic change, there are no functional consequences have been attributed to these findings. However, we supposed that these anatomic changes had potential negative effect on the improvement of BCVA in the group of vitrectomy with ILM peeling.
In our meta-analysis, the rate of postoperative complications was not significantly different between the group of vitrectomy with ILM peeling and the group of vitrectomy with no ILM peeling (Table 4). We supposed that the surgeons’ experience increasing and the dye application in ILM peeling made the adverse effect of ILM peeling be avoided. Retinal breaks, ERM (epiretinal membrane), cataract and intraocular pressure rise were the most common complications after the progresses. However, all the major surgical complications were few both in the two groups.
The results of the present meta-analysis should be interpreted with caution because of several limitations. First, all the studies available for this meta-analysis were retrospective studies, so there was a possibility of evident selection bias and observer bias with regard to the adoption of the operative approach. The surgeons might deal the eyes which had larger macular hole size, higher refractive errors and longer symptom duration with no ILM peeling to avoid postoperative application such as retinal breaks and cataract. Second, as is known, successful vitrectomy with or without ILM peeling depends on individual experiences. Surgeons with varying expertise from different clinical centers were included our study. Therefore, the efficacy outcomes such as rate of retinal reattachment after initial surgery, rate of macular hole closure after initial surgery, improved BCVA and rate of recurrent retinal detachment might be affected. The problem of intersurgeon variability, which most of the clinical trials might encounter was difficult to solve. Third, although our funnel plot showed that publication bias is unlikely, it is important to bear in mind that publication bias usually existed in meta-analysis based on published studies. Finally, converting non-normally distributed statistics (median and range) to normally distributed statistics (mean and SD) may be a cause of bias in our analysis.
Conclusions
In conclusion, the present meta-analysis of published studies has shown that vitrectomy with internal limiting membrane peeling is an efficient and safe procedure for the treatment of macular hole-induced retinal detachment with high rate of retinal reattachment and macular hole closure, lower rate of recurrent retinal detachment as compared to the procedure of vitrectomy with no internal limiting membrane peeling. Therefore, vitrectomy with ILM peeling may be a preferred treatment for macular hole-induced retinal detachment.
References
Zhang CF, Hu C. High incidence of retinal detachment secondary to macular hole in a Chinese population. Am J Ophthalmol. 1982;94:817–9.
Shukla D, Kalliath J, Srinivasan K, Neelakantan N, Rajendran A, Naresh KB, et al. Management of rhegmatogenous retinal detachment with coexisting macular hole: a comparison of vitrectomy with and without internal limiting membrane peeling. Retina. 2013;33:571–8.
Panozzo G, Mercanti A. Optical coherence tomography findings in myopic traction maculopathy. Arch Ophthalmol. 2004;122:1455–60.
Mitry D, Zambarakji H. Recent trends in the management of maculopathy secondary to pathological myopia. Graefes Arch Clin Exp Ophthalmol. 2012;250:3–13.
Ikuno Y, Sayanagi K, Oshima T, Gomi F, Kusaka S, Kamei M, et al. Optical coherence tomographic findings of macular holes and retinal detachment after vitrectomy in highly myopic eyes. Am J Ophthalmol. 2003;136:477–81.
Takano M, Kishi S. Foveal retinoschisis and retinal detachment in severely myopic eyes with posterior staphyloma. Am J Ophthalmol. 1999;128:472–6.
Tano Y. Pathologic myopia: where are we now? Am J Ophthalmol. 2002;134:645–60.
Kuriyama S, Matsumura M, Harada T, Ishigooka H, Ogino N. Surgical techniques and reattachment rates in retinal detachment due to macular hole. Arch Ophthalmol. 1990;108:1559–61.
Seike C, Kusaka S, Sakagami K, Ohashi Y. Reopening of macular holes in highly myopic eyes with retinal detachments. Retina. 1997;17:2–6.
Oshima Y, Ikuno Y, Motokura M, Nakae K, Tano Y. Complete epiretinal membrane separation in highly myopic eyes with retinal detachment resulting from a macular hole. Am J Ophthalmol. 1998;126:669–76.
Chen YP, Chen TL, Yang KR, Lee WH, Kuo YH, Chao AN, et al. Treatment of retinal detachment resulting from posterior staphyloma-associated macular hole in highly myopic eyes. Retina. 2006;26:25–31.
Rouhette H, Cauchi O, Zur C, Gastaud P. Retinal detachment due to macular holes in highly myopic eyes. Prognostic factors. J Fr Ophtalmol. 2001;24:49–53.
Patel SC, Loo RH, Thompson JT, Sjaarda RN. Macular hole surgery in high myopia. Ophthalmology. 2001;108(2):377–80.
Sulkes DJ, Smiddy WE, Flynn HW, Feuer W. Outcomes of macular hole surgery in severely myopic eyes: a case–control study. Am J Ophthalmol. 2000;130:335–9.
Kwok AK, Cheng LL, Tse MW, Cheung EY, Lam DS. Outcomes of primary rhegmatogenous retinal detachment in myopes of five or more diopters. Ophthalmic Surg Lasers. 2002;33:188–94.
Brooks Jr HL. Macular hole surgery with and without internal limiting membrane peeling. Ophthalmology. 2000;107:1939–49.
Smiddy WE, Feuer W, Cordahi G. Internal limiting membrane peeling in macular hole surgery. Ophthalmology. 2001;108:1471–6.
Kumar A, Prakash G, Singh RP. Indocyanine green enhanced maculorhexis in macular hole surgery. Indian J Ophthalmol. 2002;50:123–6.
Yooh HS, Brooks Jr HL, Capone Jr A, L’Hernault NL, Grossniklaus HE. Ultrastructural features of tissue removed during idiopathic macular hole surgery. Am J Ophthalmol. 1996;122:67–75.
Park DW, Sipperley JO, Sneed SR, Dugel PU, Jacobsen J. Macular hole surgery with internal-limiting membrane peeling and intravitreous air. Ophthalmology. 1999;106:1392–8.
Kobayashi H, Kishi S. Vitreous surgery for highly myopic eyes with foveal detachment and retinoschisis. Ophthalmology. 2003;110:1702–7.
Kanda S, Uemura A, Sakamoto Y, Kita H. Vitrectomy with internal limiting membrane peeling for macular retinoschisis and retinal detachment without macular hole in highly myopic eyes. Am J Ophthalmol. 2003;136:177–80.
Zheng B, Chen Y, Chen Y, Zhao Z, Zhang Z, Zheng J, et al. Vitrectomy and internal limiting membrane peeling with perfluoropropane tamponade or balanced saline solution for myopic foveoschisis. Retina. 2011;31(4):692–701.
Kim KS, Lee SB, Lee WK. Vitrectomy and internal limiting membrane peeling with and without gas tamponade for myopic foveoschisis. Treatment of retinal detachment resulting from myopic macular hole with internal limiting membrane removal. Am J Ophthalmol. 2012;153:320–326.e1.
Kadonosono K, Yazama F, Itoh N, Uchio E, Nakamura S, Akura J, et al. Treatment of retinal detachment resulting from myopic macular hole with internal limiting membrane removal. Am J Ophthalmol. 2001;131:203–7.
Oie Y, Emi K, Takaoka G, Ikeda T. Effect of indocyanine green staining in peeling of internal limiting membrane for retinal detachment resulting from macular hole in myopic eyes. Ophthalmology. 2007;114:303–6.
Cheung BT, Lai TY, Yuen CY, Lai WW, Tsang CW, Lam DS. Results of high-density silicone oil as a tamponade agent in macular hole retinal detachment in patients with high myopia. Br J Ophthalmol. 2007;91:719–21.
Li KK, Tang EW, Li PS, Wong D. Double peel using triamcinolone acetonide and trypan blue in the management of myopic macular hole with retinal detachment: a case–control study. Clin Experiment Ophthalmol. 2010;38:664–8.
Wilkinson CP, Rice TA. Complicated types of retinal detachment. In: Wilkinson CP, Rice TA, editors. Michels’ Retinal Detachment. 2nd ed. St. Louis, MO: Mosby; 1997. p. 641–771.
Tadayoni R, Paques M, Massin P, Mouki-Benani S, Mikol J, Gaudric A. Dissociated optic nerve fiber layer appearance of the fundus after idiopathic epiretinal membrane removal. Ophthalmology. 2001;108:2279–83.
Ito Y, Terasaki H, Takahashi A, Yamakoshi T, Kondo M, Nakamura M. Dissociated optic nerve fiber layer appearance after internal limiting membrane peeling for idiopathic macular holes. Ophthalmology. 2005;112:1415–20.
Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index for non-randomized studies (MINORS): development and validation of a new instrument. ANZ J Surg. 2003;73:712–6.
Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol. 2005;5:13.
Uemoto R, Yamamoto S, Tsukahara I, Takeuchi S. Efficacy of internal limiting membrane removal for retinal detachments resulting from a myopic macular hole. Retina. 2004;24:560–6.
Liu ZL, Sun P, Zhang H. Therapeutic effects of internal limiting membrane peeling on retinal detachment with macular hole in eyes with high myopia. Chin J Ocul Fundus Dis. 2009;25:337–40.
Yu J, Wang F, Cao H, Fan Y, Zhang X. Combination of internal limiting membrane peeling and endophotocoagulation for retinal detachment related to high myopia in patients with macular hole. Ophthalmic Surg Lasers Imaging. 2010;41:215–21.
Fan DJ. 11 cases of retinal detachment due to macular hole in high myopia: A clinical analysis. Chin J Rural Med Phar. 2013;20:26–7.
Wei Y, Wang N, Zu Z, Bi C, Wang H, Chen F, et al. Efficacy of vitrectomy with triamcinolone assistance versus internal limiting membrane peeling for highly myopic macular hole retinal detachment. Retina. 2013;33:1151–7.
Gonvers M, Machemer R. A new approach to treating retinal detachment with macular hole. Am J Ophthalmol. 1982;94:468–72.
Ishida S, Yamazaki K, Shinoda K, Kawashima S, Oguchi Y. Macular hole retinal detachment in highly myopic eyes: ultrastructure of surgically removed epiretinal membrane and clinicopathologic correlation. Retina. 2000;20:176–83.
Uemoto R, Yamamoto S, Aoki T, Tsukahara I, Yamamoto T, Takeuchi S. Macular configuration determined by optical coherence tomography after idiopathic macular hole surgery with or without internal limiting membrane peeling. Br J Ophthalmol. 2002;86:1240–2.
Spiteri Cornish K, Lois N, Scott NW, Burr J, Cook J, Boachie C, et al. Vitrectomy with internal limiting membrane peeling versus no peeling for idiopathic full-thickness macular hole. Ophthalmology. 2014;121:649–55.
Yamada E. Some structural features of the fovea centralis in the human retina. Arch Ophthalmol. 1969;82:151–9.
Gass JD. Müller cell cone, an overlooked part of the anatomy of the fovea centralis: hypotheses concerning its role in the pathogenesis of macular hole and foveomacualr retinoschisis. Arch Ophthalmol. 1999;117:821–3.
Terasaki H, Miyake Y, Nomura R, Piao CH, Hori K, Niwa T, et al. Focal macular ERGs in eyes after removal of macular ILM during macular hole surgery. Invest Ophthalmol Vis Sci. 2001;42:229–34.
Acknowledgments
This study is completed by our research team independently and we do not have someone or group to acknowledge to.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interest
All authors have no conflict of interest to declare. There are no sources of financial support to declare in this paper.
Authors’ contributions
HC conceived and carried out the design of the study, revised the manuscript and decided the final version of manuscript. JS and XL collected the data, analyzed and drafting the manuscript. JS and XL are co-first authors, contributing equally to the study of this paper. LZ provided assistance in the literature search and data analysis. All authors have read and approved the content of the final manuscript.
Jing Su and Xinquan Liu contributed equally to this work.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Su, J., Liu, X., Zheng, L. et al. Vitrectomy with internal limiting membrane peeling vs no peeling for Macular Hole-induced Retinal Detachment (MHRD): a meta-analysis. BMC Ophthalmol 15, 62 (2015). https://doi.org/10.1186/s12886-015-0048-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12886-015-0048-5