
Abstract
Background
Brain metastasis (BrM) is prevalent among patients with NSCLC, and surgical resection of BrM constitutes a promising treatment strategy for local management and histopathological diagnosis, although it is offered for a select group of patients. Limited information exists concerning the improvement in performance status (PS) following BrM resection or the outcomes stratified by subsequent systemic therapy.
Methods
We conducted a retrospective single-center cohort study including NSCLC patients with surgically resected BrM and focused on the improvement in PS and subsequent therapy after BrM resection.
Results
71 patients were included, and the median overall survival was 18.3 months (95% confidence interval [95% CI]: 8.7, not reached). Patients with NSCLC who underwent surgical resection of BrM showed significant improvement in PS (18% and 39% showed ECOG PS of 0–1, before and after BrM resection, respectively [p = 0.006]), and patients with PS improvement were younger than those with PS unimprovement (median, 62 years versus 66 years; p = 0.041). Regarding subsequent systemic therapy after BrM resection, 21 patients (30%) received cytotoxic chemotherapy, 14 patients (20%) received tyrosine kinase inhibitors (TKIs), 3 patients (4%) received immune checkpoint inhibitors (ICIs), and 21 patients (30%) received no subsequent therapy. The survival outcomes of patients stratified by subsequent systemic treatments suggested the tendency that those who received TKI or ICI showed better survival outcomes, although a small number of patients hindered statistical comparisons.
Conclusions
We describe the outcomes of patients with NSCLC who underwent surgical resection of BrM, revealing that younger patients were more likely to anticipate improvement in PS, and patients who received TKI or ICI after BrM resection tended to exhibit a more preferable prognosis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Lung cancer is the leading cause of cancer-related death worldwide [1]. Non-small cell lung cancer (NSCLC) accounts for approximately 80% of all lung cancer cases, most of which are diagnosed at an advanced stage [2]. Many patients with NSCLC develop brain metastases (BrMs) during their disease course, which is reported in 40% of cases [3,4,5]. NSCLC patients with BrMs have a very poor prognosis and deteriorated quality of life [6, 7]; thus, the brain is an important metastatic site and has attracted particular attention.
Surgical resection serves as a localized therapeutic intervention for BrMs with distinct status and has been performed for selected patients [8, 9]. Common alternative localized treatment modalities encompass whole-brain radiotherapy (WBRT) and stereotactic radiosurgery (SRS). WBRT has been used for over 70 years and is currently prescribed for patients with multiple metastases or a relatively short life expectancy due to WBRT-induced delayed neurological injury. SRS has more recently emerged and is used for patients presenting with a limited number or volume of BrMs. Both methods rely on radiation, thereby enabling the targeting of multiple metastases, surgically unattainable deep lesions, or metastases in patients exhibiting relatively aggressive systemic conditions. As for surgical resection, it is predominantly recommended for patients with a solitary BrM in an accessible region and with controlled systemic disease [10]. Surgical resection offers a notable advantage in the histological diagnosis of targeted lesions; it has been reported that a diagnosis other than malignancy (such as radiation necrosis or abscess) is made in a certain proportion of cases [11]. Furthermore, it confers another important advantage of immediate improvement of the intracranial mass effect, with subsequent improvement of symptoms. Consequently, surgical resection has also been conducted for patients with severe progressive symptoms from BrMs and who require rapid improvement of symptoms. Some studies have shown that patients who undergo surgical resection of BrMs tend to show improvement in performance status (PS) [12,13,14]. However, little is known about the characteristics of patients whose PS could be expected to improve.
The efficacy of systemic therapy for NSCLC BrMs has been demonstrated in several studies [15]. Systemic treatments for NSCLC can be categorized as cytotoxic chemotherapy, tyrosine kinase inhibitors (TKIs) as targeted therapy for driver oncogene-addicted tumors, and immune-checkpoint inhibitors (ICIs). The treatment paradigm has undergone a transformation in recent decades, which has resulted from the clinical implementation of TKIs and ICIs. Each of these therapeutic modalities has shown clinical benefit for patients with BrMs to varying degrees [16, 17], but the optimal subsequent treatment for patients who have undergone surgical resection of BrMs remains uncertain, and the outcomes of each treatment have been poorly reported [18, 19].
This study focused on patients with NSCLC who had undergone surgical resection of BrMs. The aim was to clarify treatment characteristics and outcomes, with particular emphasis on PS changes caused by surgery, and subsequent systemic treatments.
Methods
Study population
This was a retrospective, cohort study including advanced NSCLC patients with BrMs who underwent surgical resection of BrMs of NSCLC between February 1, 2008, and December 31, 2021. Patients who (1) underwent surgical resection of BrMs only for diagnosis (not for treatment or palliation of symptoms) or (2) had missing clinical information before or after BrM resection were excluded. This study protocol was approved by the ethics committee of Kyoto University Hospital.
Clinical variables and outcomes
The investigation focused on the first surgical resection of BrMs in patients who underwent repeated resections. In all patients, Eastern Cooperative Oncology Group (ECOG) performance status (PS) was evaluated immediately before BrM resection. In addition, the ECOG PS after resection was evaluated as the best ECOG PS observed within 90 days after resection. The numbers of BrMs and complete resections were evaluated radiologically and clinically. The TNM classification was determined at the time of BrM resection, based on the 8th edition of the TNM staging system. For patients whose primary tumor had been previously surgically resected, the T and N categories were reported as X due to the unavailability of accurate staging information. Information on driver oncogenes was obtained through a review of electronic medical records; patients who underwent BrM resection in the early chronological period could not have been adequately profiled. Subsequent systemic therapy after BrM resection was defined as the systemic chemotherapy that the patients received after BrM resection and before disease progression or death, regardless of the site of progression. Subsequent systemic therapy was categorized as follows: (1) none; (2) cytotoxic agents; (3) TKIs; and (4) ICIs. Patients who received (2) cytotoxic chemotherapy plus (3) TKIs or (4) ICIs were categorized as (3) TKIs or (4) ICIs, respectively, considering the relatively stronger effect expected. Patients who received subsequent resection of BrM were defined as those who received any prior therapy for NSCLC, including surgical resection of the primary lesion, radiation therapy for the primary lesion or intracranial lesion, systemic chemotherapy, etc. Conversely, patients who received upfront resection of BrM included those who underwent BrM resection as the first treatment for NSCLC. The time between the date of BrM resection and that of death was calculated for each patient to evaluate overall survival (OS). The data cut-off was June 30, 2022.
Statistical analyses
Continuous variables are reported as means and ranges, and categorical variables as numbers and percentages. OS was calculated using Kaplan–Meier estimates and compared using the log-rank test. To investigate the potential factors associated with OS, univariate Cox proportional hazard models were constructed for all clinically relevant factors (age, sex, smoking status, ECOG PS before resection, previous anticancer therapy, complete resection, BrM histology, ECOG PS after resection, and subsequent therapy). The multivariate Cox proportional hazards model included factors that were clinically predicted to be associated with prognosis and factors we focused on (age, timing of resection, ECOG PS after resection, and subsequent therapy). In the comparison of characteristics, ECOG PS change was compared with the Wilcoxon signed-rank test, and the correlation between age and ECOG PS change was analyzed using the Mann–Whitney U test. Dichotomous variables were analyzed using Fisher’s exact test.
For the analyses, a two-tailed p-value of < 0.05 was considered significant. Statistical analyses were conducted using R (version 4.2.2) [20], data processing was conducted using the package dplyr (version 1.1.2) [21], description and analysis of characteristics were conducted using the package gtsummary (version 1.7.2) [22], survival analyses were conducted using the packages survival (version 3.5-7) [23] and survminer (version 0.4.9) [24], and figures were produced using the package ggplot2 (version 3.4.2) [25].
Results
Patients’ characteristics and overall survival
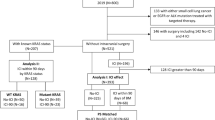
In total, 80 patients with NSCLC underwent surgical resection of BrMs between January 2008 and December 2021. Of them, 9 patients were excluded for the following reasons: 6 for BrM histology showing high-grade neuroendocrine carcinoma; 1 for BrM resection only for diagnosis; 1 for preceding BrM resection in another hospital; and 1 for missing information after BrM resection. Finally, 71 patients who were clinically indicated for BrM resection to alleviate or prevent symptoms were included. The patients’ characteristics are summarized in Table 1.
For all patients, the median OS was 18.3 (95% confidence interval [95% CI]: 8.7 - not reached) months, and the Kaplan-Meier curve is shown in Fig. 1.

Kaplan-Meier curve of overall survival
Improvement of ECOG PS
The change in ECOG PS before and after BrM resection is shown in Fig. 2. In summary, 13 (18.3%) and 58 (81.7%) of 71 patients showed an ECOG PS of 0–1 and 2–4 before BrM resection, whereas 28 (39.4%) and 43 (60.6%) patients showed 0–1 and 2–4 after BrM resection, respectively, demonstrating significant improvement (p = 0.006). To further examine the characteristics of patients with improved ECOG PS after resection, patients with an ECOG PS of 2–4 before BrM resection were examined, and the baseline characteristics of patients whose ECOG PS improved to 0–1 after resection were compared to those whose ECOG PS did not improve (summarized in Table 2). The patients who had improved ECOG PS after resection were younger than those with no improvement in PS (median, 62 years versus 66 years; p = 0.041), and other clinically relevant factors showed no significant correlations.

Changes in ECOG performance status (PS) after resection of brain metastases
Subsequent therapy after BrM resection
As subsequent systemic therapy after BrM resection before progression, 21 patients (29.6%) received cytotoxic chemotherapy, 14 patients (19.7%) received TKIs, 3 patients (4.2%) received ICIs, and 34 patients (47.9%) received no subsequent systemic therapy. Kaplan-Meier curves are summarized in Fig. 3A; there was a trend for longer OS for patients receiving subsequent TKI or ICI therapies (p = 0.12).

Kaplan-Meier curves of overall survival stratified by subsequent therapy after brain metastasis (BrM) resection and before progression for all patients (A) and for patients with no previous anti-cancer therapy before brain metastasis resection (B)
To clearly investigate the associations between subsequent systemic therapy and OS, patients who had received no anticancer treatment before BrM resection or who had received BrM resection as the first therapy for NSCLC after clinical diagnosis were selected. Kaplan-Meier curves are summarized in Fig. 3B; there was a trend for longer OS for patients receiving subsequent TKI or ICI therapies (p = 0.057).
As subsequent consolidative radiotherapy, 20 patients (28.2%) received whole brain radiotherapy and 8 patients (11.2%) received stereotactic radiosurgery therapy.
Univariate and multivariate analysis of OS
Univariate analysis for OS, including known clinical prognostic factors and the factors investigated above, was performed. The results are summarized in Table 3, and the ECOG PS after BrM resection, but not for ECOG PS before resection, was correlated with significantly longer OS (p = 0.007). Other clinically known prognostic factors showed no significant correlations with OS. The Kaplan-Meier curves of OS stratified by ECOG-PS after BrM resection are summarized in Fig. 4.

Kaplan-Meier curves of overall survival stratified by ECOG performance status (PS) after brain metastasis (BrM) resection
Furthermore, we conducted multivariate analysis; however, due to only 40 events occurred, the number of explanatory variables that could be considered was limited. We incorporated variables that were considered major prognostic factors (age, timing of resection [upfront or subsequent]) and factors of interest (ECOG PS after resection, subsequent therapy) into the model as explanatory variables. In this analysis, better ECOG PS after resection and subsequent TKI therapy were shown to be significantly associated with longer OS (Table 3).
Discussion
This investigation focused on NSCLC patients with surgically resected BrMs who showed an improvement in PS after BrM resection, which is more frequently observed in younger patients, and the associations between subsequent systemic therapy and prognosis.
In this study, the median OS of NSCLC patients with a surgically resected BrM was 18.3 months. This result aligns with historical controls [13, 26,27,28,29,30,31] from retrospective cohorts of NSCLC patients with resected BrM, which reported median OS ranging from 12 to 20 months. During earlier periods when the only possible intervention for BrM consisted of best supportive care, the prognosis of patients with BrM was 1–2 months [32]. With the introduction of WBRT in the 1950s, it improved to 4–6 months [10]. In recent years, the prognosis for NSCLC patients with BrMs has much improved, to 5–8 months [33]. Considering the inevitable bias of the present study in which patients in good general condition who could be considered for an invasive procedure, surgical resection of BrM, were selected, it is not surprising that patients who underwent surgical resection of BrMs showed a better prognosis.
NSCLC patients who underwent surgical resection of BrMs demonstrated improvements in PS, which is comparable to previous studies [12,13,14]. From the further analysis of patients who had poor ECOG PS prior to BrM resection, those who experienced PS improvement postoperatively had a younger age than those who showed no PS improvement. To the best of our knowledge, no previous study investigated the baseline characteristics of patients who tend to show PS improvement after BrM resection. It is plausible, given that a younger age has been identified as a factor associated with a good prognosis for patients who underwent surgical resection of BrMs [30, 34]. The cause is unknown, but it could result from superior baseline status or preserved functional capacity prior to the appearance of symptoms, encompassing comorbidities unrelated to NSCLC. On univariate analyses for OS, ECOG PS after BrM resection, rather than preoperative values, was associated with a better prognosis. Previous studies focused mainly on ECOG PS before BrM resection and posited it as a potential factor associated with a good prognosis [28, 30, 35, 36]. The reason for this discrepancy is unknown, but it could be influenced by the diverse characteristics of the participating patients. Specifically, the selection criteria for surgical resection could largely rely on medical accessibility or the collective agreement of medical practitioners within various countries and regions. In summary, younger patients with symptomatic and operable BrMs could be deemed suitable candidates for surgical resection to alleviate symptoms and improve their prognoses, although further investigations are needed.
Advances in systemic therapy could affect the outcomes of NSCLC patients with resected BrMs. In previous studies, TKIs or ICIs were reported to be associated with superior outcomes in selected NSCLC patients with BrMs which were not surgically resected [18, 19]. The results of the present study aligned with these studies, and the present one specifically focused on the prognosis of NSCLC patients with surgically resected BrMs for the first time. However, the present cohort had an inevitable bias, as those who underwent BrM resection with or without preceding systemic treatment were included. To circumvent this bias, patients who received BrM resection as the initial therapy for NSCLC were examined, and more pronounced associations between subsequent systemic treatments and survival outcomes were found. Of course, the results could not be interpreted simply as causal connections between subsequent systemic treatment and survival outcomes because of the inevitable selection bias; patients who could receive only cytotoxic chemotherapy or no systemic therapy must have some background characteristics precluding access to other treatments. Moreover, patients who had undergone BrM resection in previous decades lacked comprehensive genetic profiling of their tumors and no chance to receive TKI or ICI treatment. The effects of TKIs or ICIs for BrMs have been widely studied in preclinical and clinical retrospective studies, but they are seldom investigated in prospective clinical trials, since patients with BrMs are excluded from the majority of trials. Consequently, real-world studies are still needed to investigate and optimize therapy for NSCLC patients with BrMs.
The present study had several limitations. First, it was a retrospective study and included only patients who underwent surgical resection of BrMs. The background characteristics of patients undergoing BrM resection were heterogeneous, which could affect the results and their interpretations. Furthermore, we acknowledge that patients selected for surgical resection of brain metastases likely had better overall health and prognosis compared to the general population of NSCLC patients with BrMs. This introduces a potential selection bias, which may limit the generalizability of our findings to all NSCLC patients with BrMs. Second, given that patients who underwent BrM resection over an extended period (2009–2022) were included, genomic profiling of tumors was not conducted uniformly. Additionally, during this extended study period, treatment protocols and diagnostic methods underwent significant advancements, which could have potentially affected the observed outcomes. Third, the present study included a limited number of participants. Consequently, the statistical power could be limited. Fourth, our study design did not include a non-surgical control group, which limits our ability to directly compare the effectiveness of surgical resection against other treatment modalities for NSCLC brain metastases. This was intentional, as our primary aim was to describe outcomes in surgically treated patients, with a focus on post-operative performance status changes and subsequent treatments. Fifth, due to the small number of patients in each subgroup receiving subsequent systemic therapies, we were unable to provide detailed statistical comparisons for the survival outcomes across these therapies. This limitation in sample size for subgroup analysis restricts our ability to draw definitive conclusions about the relative efficacy of various systemic treatments following BrM resection. Future studies with larger cohorts would be valuable to further elucidate the impact of specific systemic therapies on survival outcomes in this patient population.
Conclusions
In this study, the prognosis and characteristics of NSCLC patients with BrMs who underwent surgical resection of BrMs were investigated. The results suggested that PS improvement after BrM resection could be expected, particularly in younger patients. Recent advances in systemic treatment such as TKIs and ICIs could potentially correlate with survival outcomes.
Data availability
No datasets were generated or analysed during the current study.
Abbreviations
- BrM:
-
Brain metastasis
- CI:
-
Confidence interval
- ECOG:
-
Eastern Cooperative Oncology Group
- ICI:
-
Immune-checkpoint inhibitor
- NSCLC:
-
Non-small cell lung cancer
- OS:
-
Overall survival
- PS:
-
Performance status
- SRS:
-
Stereotactic radiosurgery
- TKI:
-
Tyrosine kinase inhibitor
- WBRT:
-
Whole-brain radiation therapy
References
Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022;72(1):7–33. https://doi.org/10.3322/caac.21708.
Ganti AK, Klein AB, Cotarla I, Seal B, Chou E. Update of incidence, prevalence, survival, and initial treatment in patients with Non-small Cell Lung Cancer in the US. JAMA Oncol. 2021;7(12):1824–32. https://doi.org/10.1001/jamaoncol.2021.4932.
Barnholtz-Sloan JS, Sloan AE, Davis FG, Vigneau FD, Lai P, Sawaya RE. Incidence proportions of brain metastases in patients diagnosed (1973 to 2001) in the Metropolitan Detroit Cancer Surveillance System. J Clin Oncol off J Am Soc Clin Oncol. 2004;22(14):2865–72. https://doi.org/10.1200/JCO.2004.12.149.
Nayak L, Lee EQ, Wen PY. Epidemiology of brain metastases. Curr Oncol Rep. 2012;14(1):48–54. https://doi.org/10.1007/s11912-011-0203-y.
Kim M, Suh CH, Lee SM, et al. Development of Brain metastases in patients with Non-small Cell Lung Cancer and No Brain metastases at initial staging evaluation: cumulative incidence and risk factor analysis. AJR Am J Roentgenol. 2021;217(5):1184–93. https://doi.org/10.2214/AJR.21.25787.
Arrieta O, Villarreal-Garza C, Zamora J, et al. Long-term survival in patients with non-small cell lung cancer and synchronous brain metastasis treated with whole-brain radiotherapy and thoracic chemoradiation. Radiat Oncol Lond Engl. 2011;6:166. https://doi.org/10.1186/1748-717X-6-166.
Sperduto PW, Kased N, Roberge D, et al. Summary report on the graded prognostic assessment: an accurate and facile diagnosis-specific tool to estimate survival for patients with brain metastases. J Clin Oncol off J Am Soc Clin Oncol. 2012;30(4):419–25. https://doi.org/10.1200/JCO.2011.38.0527.
Vogelbaum MA, Brown PD, Messersmith H, et al. Treatment for Brain metastases: ASCO-SNO-ASTRO Guideline. J Clin Oncol. 2022;40(5):492–516. https://doi.org/10.1200/jco.21.02314.
Brenner AW, Patel AJ. Review of current principles of the diagnosis and management of Brain metastases. Front Oncol. 2022;12:857622. https://doi.org/10.3389/fonc.2022.857622.
Hatiboglu MA, Akdur K, Sawaya R. Neurosurgical management of patients with brain metastasis. Neurosurg Rev. 2020;43(2):483–95. https://doi.org/10.1007/s10143-018-1013-6.
Patchell RA, Tibbs PA, Walsh JW, et al. A randomized trial of surgery in the treatment of single metastases to the brain. N Engl J Med. 1990;322(8):494–500. https://doi.org/10.1056/NEJM199002223220802.
Schödel P, Schebesch KM, Brawanski A, Proescholdt MA. Surgical Resection of Brain metastases—impact on neurological outcome. Int J Mol Sci. 2013;14(5):8708–18. https://doi.org/10.3390/ijms14058708.
Kim SY, Hong CK, Kim TH, et al. Efficacy of Surgical Treatment for Brain Metastasis in patients with Non-small Cell Lung Cancer. Yonsei Med J. 2015;56(1):103–11. https://doi.org/10.3349/ymj.2015.56.1.103.
Heßler N, Jünger ST, Meissner AK, Kocher M, Goldbrunner R, Grau S. Recurrent brain metastases: the role of resection of in a comprehensive multidisciplinary treatment setting. BMC Cancer. 2022;22:275. https://doi.org/10.1186/s12885-022-09317-6.
Page S, Milner-Watts C, Perna M, et al. Systemic treatment of brain metastases in non-small cell lung cancer. Eur J Cancer Oxf Engl. 2020;132:187–98. https://doi.org/10.1016/j.ejca.2020.03.006.
Angeli E, Bousquet G. Brain metastasis treatment: the place of tyrosine kinase inhibitors and how to facilitate their diffusion across the blood–brain barrier. Pharmaceutics. 2021;13(9):1446. https://doi.org/10.3390/pharmaceutics13091446.
Pathak R, Amini A, Hill A, Massarelli E, Salgia R. Immunotherapy in Non-small Cell Lung Cancer patients with Brain metastases: Clinical challenges and future directions. Cancers. 2021;13(14):3407. https://doi.org/10.3390/cancers13143407.
Shah PP, Franke JL, Medikonda R, et al. Mutation status and postresection survival of patients with non-small cell lung cancer brain metastasis: implications of biomarker-driven therapy. J Neurosurg. 2022;136(1):56–66. https://doi.org/10.3171/2020.10.JNS201787.
Wasilewski D, Radke J, Xu R, et al. Effectiveness of Immune Checkpoint Inhibition vs Chemotherapy in Combination with Radiation Therapy among patients with non–small cell Lung Cancer and Brain Metastasis Undergoing Neurosurgical Resection. JAMA Netw Open. 2022;5(4):e229553. https://doi.org/10.1001/jamanetworkopen.2022.9553.
Ihaka R, Gentleman R. R: a language for data analysis and graphics. J Comput Graph Stat. 1996;5(3):299–314.
Wickham H, François R, Henry L, Müller K, Vaughan D. Dplyr: A Grammar of Data Manipulation.; 2023. https://CRAN.R-project.org/package=dplyr
Sjoberg DD, Whiting K, Curry M, Lavery JA, Larmarange J. Reproducible summary tables with the gtsummary package. R J. 2021;13(1):570–80. https://doi.org/10.32614/RJ-2021-053.
Terry M, Therneau PM, Grambsch. Modeling Survival Data: extending the Cox Model. Springer; 2000.
Kassambara A, Kosinski M, Biecek P. Survminer: Drawing Survival Curves Using Ggplot2; 2021. https://CRAN.R-project.org/package=survminer
Wickham H. Ggplot2: elegant graphics for data analysis. New York: Springer-; 2016. http://ggplot2.org.
Ilic I, Faron A, Heimann M, et al. Combined Assessment of Preoperative Frailty and Sarcopenia allows the prediction of overall survival in patients with Lung Cancer (NSCLC) and surgically treated Brain Metastasis. Cancers. 2021;13(13):3353. https://doi.org/10.3390/cancers13133353.
Bougie E, Masson-Côté L, Mathieu D. Comparison between Surgical Resection and Stereotactic Radiosurgery in patients with a single brain metastasis from Non-small Cell Lung Cancer. World Neurosurg. 2015;83(6):900–6. https://doi.org/10.1016/j.wneu.2015.01.029.
Perng PS, Hsu HP, Lee PH, Huang CC, Lin CC, Lee JS. Correlation of EGFR mutation subtypes and survival in surgically treated brain metastasis from non-small-cell lung cancer. Asian J Surg. 2023;46(1):269–76. https://doi.org/10.1016/j.asjsur.2022.03.076.
Fuchs J, Früh M, Papachristofilou A, et al. Resection of isolated brain metastases in non-small cell lung cancer (NSCLC) patients - evaluation of outcome and prognostic factors: a retrospective multicenter study. PLoS ONE. 2021;16(6):e0253601. https://doi.org/10.1371/journal.pone.0253601.
Antuña AR, Vega MA, Sanchez CR, Fernandez VM. Brain metastases of Non-small Cell Lung Cancer: prognostic factors in patients with Surgical Resection. J Neurol Surg Part Cent Eur Neurosurg. 2018;79(2):101–7. https://doi.org/10.1055/s-0037-1601874.
Hanagiri T, Takenaka M, Oka S, et al. Results of a surgical resection for patients with stage IV non–small-cell lung cancer. Clin Lung Cancer. 2012;13(3):220–4. https://doi.org/10.1016/j.cllc.2011.05.006.
Soffietti R, Rudà R, Trevisan E. Brain metastases: current management and new developments. Curr Opin Oncol. 2008;20(6):676–84. https://doi.org/10.1097/CCO.0b013e32831186fe.
Owen S, Souhami L. The management of brain metastases in non-small cell lung cancer. Front Oncol. 2014;4:248. https://doi.org/10.3389/fonc.2014.00248.
Stark AM, Tscheslog H, Buhl R, Held-Feindt J, Mehdorn HM. Surgical treatment for brain metastases: prognostic factors and survival in 177 patients. Neurosurg Rev. 2005;28(2):115–9. https://doi.org/10.1007/s10143-004-0364-3.
Korinth MC, Delonge C, Hütter BO, Gilsbach JM. Prognostic factors for patients with microsurgically resected brain metastases. Onkologie. 2002;25(5):420–5. https://doi.org/10.1159/000067435.
Kim YZ, Kim KH, Kim JS, Song YJ, Kim KU, Kim HD. Clinical analysis of patients who survived for less than 3 months after brain metastatectomy. J Korean Med Sci. 2009;24(4):641–8. https://doi.org/10.3346/jkms.2009.24.4.641.
Acknowledgements
The authors are grateful to all patients who participated in this study.
Funding
This work was supported by Grants-in-Aid from the Ministry of Education, Culture, Sports, Science and Technology of Japan (22H03186).
Author information
Authors and Affiliations
Contributions
KH: Conceptualization, Investigation, Methodology, Data curation, Writing – original draft. HO: Conceptualization, Supervision, Writing – review & editing. MT: Writing – review & editing. HY1: Writing – review & editing. HA: Writing – review & editing. TT: Writing – review & editing. HY2: Writing – review & editing. YT: Writing – review & editing. NS: Writing – review & editing. YM: Writing – review & editing. SM: Writing – review & editing. TH: Writing – review & editing. YA: Conceptualization, Supervision, Data curation, Writing – review & editing.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was was approved by the Institutional Review Board of Kyoto University Hospital (R2088). The requirement for individual consent was waived for this retrospective analysis.
Consent for publication
Not applicable.
Competing interests
YA reports grants from Philips, Otsuka, Chugai, Nihon Medi-Physics, Daiichi Sankyo, Stryker, Eisai, Japan Blood Products Organization, Ono Pharmaceutical, Taiho Pharma, Sumitomo Dainippon Pharma, Astellas Pharma, Incyte Biosciences, and Servier and personal fees from Nippon Kayaku, Novocure, UCB Japan, Ono Pharmaceutical, Brainlab, Merck, Chugai, Eisai, Daiichi Sankyo, Carl Zeiss, and Nihon Medi-Physics. The other authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Hosoya, K., Ozasa, H., Tanji, M. et al. Performance status improvement and advances in systemic treatment after brain metastases resection: a retrospective single-center cohort study of non-small cell lung cancer patients. BMC Cancer 24, 1030 (2024). https://doi.org/10.1186/s12885-024-12798-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-024-12798-2