
Abstract
Background
This study was designed to evaluate the effect of progesterone receptor (PR) status on the prognosis of advanced estrogen receptor (ER)-high human epidermal growth factor receptor 2 (HER2)-negative breast cancer patients receiving CDK4/6 inhibitor combined with endocrine as first-line therapy.
Methods
Advanced ER-high HER2-negative breast cancer patients who were admitted to Harbin Medical University Cancer Hospital and received cyclin-dependent kinase (CDK)4/6 inhibitor combined with endocrine as first-line therapy were included for analysis. Patients were divided into PR-high group (11-100%), PR-low group (1-10%), and PR-negative group (< 1%) according to the expression of PR. Chi-square test was used to analyze the correlation of variables between groups. COX regression analysis were used to analyze the risk factors of survival. Kaplan-Meier survival curve was used to analyze the differences of progression-free survival (PFS) and overall survival (OS) between groups.
Results
Among the 152 patients, 72 were PR-high, 32 were PR-low, and 48 were PR-negative. Compared with PR-negative group, the proportions of disease-free survival (DFS) ≥ 5 years and Ki-67 index ≤ 30% in PR-low group and PR-high group were significant higher. PR-negative patients were more likely to occur first-line progression of disease within 24 months (POD24) than PR-high(P = 0.026). Univariate and multivariate analysis showed that PR-negative and first-line POD24 occurrence were risk factors for survival. Survival curve analysis showed that compared with PR-high group, the PFS and OS were significantly lower in PR-negative group (P = 0.001, P = 0.036, respectively). Patients with first-line POD24 had shorter OS in the overall population as well as in subgroups stratified by PR status.
Conclusions
PR-negative and first-line POD24 occurrence were risk factors of advanced ER-high HER2-negative breast cancer patients receiving CDK4/6 inhibitor combined with endocrine as first-line therapy. PR-negative patients had shortest PFS and OS. Regardless of PR status, first-line POD24 occurrence predicted shorter OS.
Similar content being viewed by others

Introduction
Breast cancer is currently the most common cancer in women worldwide [1, 2], and its incidence is also increasing year by year. Hormone receptor(HR)-positive HER2-negative is the most common molecular subtype, accounting for about 60–70% of female breast cancer [3]. At present, according to the National Comprehensive Cancer Network (NCCN) guideline, CDK4/6 inhibitors combined with endocrine are recommended as first-line therapy for patients with ER-positive and HER2-negative advanced or metastatic breast cancer(MBC) [3]. However, studies have shown that patients with low expression of ER have similar biological characteristics and clinical outcomes to ER-negative patients, and have limited benefits from endocrine therapy [4], therefore, the choice of endocrine therapy for ER-low patients should be cautious. Based on a large number of clinical trial data, patients with ER-high and HER2-negative advanced breast cancer have clearly benefited from CDK4/6 inhibitor combined with endocrine therapy [5,6,7,8,9], but there are still some patients with poor prognosis. There is limited understanding of predictive markers for prognosis in combination with CDK4/6 therapy other than ER expression levels. Finding simple and reliable markers to predict the prognosis of CDK4/6 inhibitor combined with endocrine therapy is a critical clinical issue that needs to be solved immediately.
PR belongs to the steroidal hormone receptor family, which is the target gene of ER up-regulation, and its expression is dependent on estrogen [10]. It can be divided into two subtypes: PR-A and PR-B. PR-B is a transcription activator of target genes, while PR-A is an inhibitory factor with transcriptional activity and has an inhibitory effect on PR-B [11]. As a basic predictive marker and important prognostic factor for endocrine therapy [12], PR has been well known in early breast cancer and previous first-line treatment of advanced breast cancer, but whether it can predict the survival benefit of patients with CDK4/6 inhibitors combined with endocrine therapy is still limited.
Therefore, we investigated whether PR status exerted effect on prognosis of advanced ER-high HER2-negative breast cancer patients receiving CDK4/6 inhibitor combined with endocrine as first-line therapy in order to find simple and effective markers to predict the efficacy of CDK4/6 inhibitor.
Methods
Patients selection
The complete clinicopathological data of 152 patients with advanced ER-high and HER2-negative breast cancer who received CDK4/6 inhibitors and endocrine as first-line therapy in Harbin Medical University Cancer Hospital from January 2017 to December 2019 were collected. Patients received at least two cycles of systemic therapy and could be evaluated for treatment effect. All patients had biopsy pathology of recurrent or metastatic lesions, with comprehensive follow-up data and no loss to follow-up. The study protocol was approved by the Institutional Ethics Committee of Harbin Medical University Cancer Hospital, and has been performed in accordance with the ethical standards laid down in the 1964 Helsinki Declaration and its later amendments. All patients provided written informed consent for data use.
Data collections
The clinicopathological data of patients were collected, including age, menopause, adjuvant therapy, DFS, initial diagnosis or recurrence of breast cancer, metastatic site, number of metastases, pathology of metastases, first-line endocrine drugs, first-line PFS and OS. Immunohistochemical staining was used to analyze ER, PR, HER2 and Ki-67 index in metastatic lesions by pathologists who were fully dedicated to breast cancer pathology. According to the American Society of Clinical Oncology (ASCO) /College of American Pathologists (CAP) guidelines, breast cancer samples with 11–100% of tumor cell nuclei positive should be interpreted as ER-high, ER-low was with 1-9% of cells staining. A sample would be considered ER-negative if < 1% or 0% of tumor cell nuclei were immunoreactive. Similar principles apply to PR testing. Patients were separated into three groups based on IHC result of PR staining: PR-high, PR-low and PR-negative. The efficacy of the treatment was evaluated by computerized tomography (CT). According to Response Evaluation Criteria In Solid Tumors (RECIST) 1.1, treatment-associated curative effects were classified into complete remission (CR), partial remission (PR), stable disease (SD), and progressive disease (PD) subtypes.
Follow-up
Through the medical record review system and telephone follow-up of Harbin Medical University Cancer Hospital, the disease recurrence, metastasis and survival status of patients up to October 2023 were collected. DFS was defined as the time from the diagnosis of breast cancer to disease recurrence or metastasis. PFS was defined as the time from the initiation of first-line therapy to disease progression or the last visit or death, whichever came first. OS was calculated from the initiation of first-line therapy to the date of death or last follow-up.
Statistical analysis
IBM SPSS program version 26.0 was used for data analysis. Normality test was performed on the measurement data, and the measurement data conforming to the normal distribution were described by x ± S. Chi-square test was used to analyze the correlation of variables between groups. Univariate and multivariate COX regression were used to analyze the risk factors for PFS and OS of advanced ER-high HER2-negative breast cancer. Kaplan-Meier method was used for survival analysis, and log-rank test was used to compare the disease-free survival rate between the two groups. Hazard ratios (HRs) together with 95% confidence intervals (CI) were provided. P < 0.05 was considered statistically significant.
Results
General data
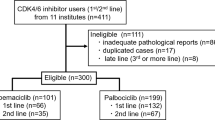
The complete clinicopathological features of 152 patients with advanced ER-high HER2-negative breast cancer receiving CDK4/6 inhibitor combined with endocrine as first-line therapy were collected in this study. The age of patients ranged from 27 to 72 years, with a median age of 50.0 years. 96 (63.2%) patients were non-menopausal. 26 (17.1%) were treatment-naive stage IV. All patients had advanced biopsy pathology. Among the patients in the study, 72 (47.4%) were PR-high, 32 (21.1%) were PR-low, and 48 (31.6%) were PR-negative. Besides, 66 (43.4%) patients were with first-line POD24. Clinicopathological characteristics of the study participants are summarized in Table 1. The results of immunohistochemical staining of different PR expression are shown in Fig. 1.

immunohistochemical staining of different PR expression. (A) Negative expression of PR (a:100×, b:200×).(B) 5%(low) expression of PR (a:100×, b:200×).(C) 90%(high) expression of PR (a:100×, b:200×)
Comparison of clinicopathological characteristics
The clinicopathological characteristics of the three groups were compared, and the results are shown in Table 2. Compared with PR-high and PR-low group, PR-negative group had a higher proportion of patients with DFS < 5 years (both P < 0.001), and no significant difference was observed between PR-high and PR-low patients (P = 0.597). Patients in PR-negative group had higher rate of Ki-67 index>30% (P = 0.018). 33.3% of PR-high patients, 43.8% of PR-low patients, and 58.3% of PR-negative patients were with first-line POD24 (PR-high versus PR-low P = 0.309, PR-high versus PR-negative P = 0.007, PR-low versus PR-negative P = 0.201). There were no significant differences in other clinicopathological features among the three groups.
Univariate and multivariate analyses
Univariate and multivariate analyses of clinicopathological characteristics affecting first-line PFS and OS of advanced ER-high HER2-negative breast cancer were performed by COX regression model. The variables included age, menstrual status, breast cancer status, DFS, adjuvant endocrine therapy, adjuvant chemotherapy, adjuvant radiotherapy, number of metastases, metastatic site, PR status, HER2 status, Ki-67 index, endocrine drugs, and first-line POD24 (only included in OS analysis).
Univariate analysis showed that DFS < 5 years, without adjuvant radiation therapy and PR-negative were risk factors of PFS in patients with advanced ER-high HER2-negative breast cancer (P = 0.027, P = 0.016, P<0.001, respectively. Table 3). Multivariate analysis showed that PR-negative was associated with shorter PFS (P = 0.013, Table 3). Univariate analysis showed that DFS < 5 years and PR-negative were associated with shorter OS in patients with advanced ER-high HER2-negative breast cancer (P = 0.039, P = 0.032, Table 4). Both univariate and multivariate analyses of risk factors for OS showed that first-line POD24 was associated with shorter OS (both P < 0.001, Table 4).
PFS and OS
Kaplan-Meier analysis was used to analyze the relationship between PR status and survival in 152 patients with advanced ER-high HER2-negative breast cancer. The results showed that PFS in the PR-negative group was significantly lower than that in the PR-high group (P = 0.001, Fig. 2). Compared with the PR-high group, the median OS in the PR-negative group was significantly lower (P = 0.036, Fig. 3). In all patients enrolled, patients with first-line POD24 had shorter OS regardless of PR status(Fig. 4).

Kaplan-Meier PFS curves of advanced ER-high HER2-negative breast cancer

Kaplan-Meier OS curves of advanced ER-high HER2-negative breast cancer

Kaplan-Meier OS curves of advanced ER-high HER2-negative breast cancer. (A). All patients. (B).PR-negative group. (C).PR-low group. (D). PR-high group
Discussion
CDK4/6 inhibitors are a class of small molecule targeted drugs. CDK4 or CDK6 binds to cyclin D1 to form a cyclin D1-CDK4/6 complex, phosphorylates retinoblastoma protein (pRb) to release transcription factor E2F and drive cell cycle progression from G1 to S phase [13]. Blocking cyclin D1-CDK4/6-pRb signaling pathway can inhibit the proliferation of tumor cells [14]. CDK4/6 inhibitor combined with endocrine therapy is the standard first-line therapy for patients with HR-positive advanced breast cancer [3], and a large number of clinical trials have proved that it can improve the durability of response [5], prevent and overcome endocrine resistance of HR-positive breast cancer [6], and bring a better prognosis to patients [7,8,9]. However, the markers that can predict the prognosis after treatment are not fully clear [15, 16]. Due to the continuous in-depth study of ER status, it is generally believed that the characteristics of patients with low expression of ER are closer to triple negative [17], and the low expression of ER will affect the prognosis of patients treated with CDK4/6 inhibitors combined with endocrine therapy. In order to reduce the effect of ER status on prognosis, patients with ER-low expression were excluded in our study, and patients with ER-high expression were selected as study subjects.
As a basic predictive marker in endocrine therapy, the effect of PR expression on the prognosis after endocrine therapy has been studied in many cases, such as ER-positive, PR-negative breast cancer has a poor prognosis and is associated with endocrine resistance. Kurozumi et al. [18] pointed out that PR expression level is an independent prognostic factor for HR-positive and HER2-negative breast cancer patients, especially when Ki-67 expression level is between 10% and 30%, patients with PR < 20% have a worse prognosis. Piasecka et al. [19] found that PR-negative is a marker of increased EGFR activity, and the activation of EGFR can increase resistance to endocrine drugs. A European retrospective analysis of GEICAM/9906 study found that ER-positive /PR-negative breast cancer had stronger tumor proliferation, higher risk of recurrence and death, and worse survival outcomes [20]. In the study by Rocca A et al., in patients receiving only first-line endocrine therapy with an aromatase inhibitor, high PR (> 20%) was found to be independently associated with long time to progression in those with ER-high [21]. The prognostic value of PR status in CDK4/6 inhibitor combined with endocrine therapy is different. A pooled analysis by the FDA showed that all clinicopathological subgroups of patients with HR-positive, HER2-negative advanced breast cancer benefited from CDK4/6 inhibitors when combined with CDK4/6 inhibitors as first-line therapy, regardless of PR expression. However, the authors noted heterogeneity in the patients included in the analysis which may differ from the general population, the prognostic value of PR status on endocrine combined with CDK4/6 inhibitors still needs to be further studied [22]. In PALOMA-3, patients with PR-high expression showed longer benefits in both groups who received palbociclib plus fulvestrant or placebo plus fulvestrant [23]. Shao X et al. also found that PR ≥ 20% was associated with longer PFS in patients receiving a combination therapy with CDK4/6 inhibitors (8.5 vs. 6.7 months), and PFS was significantly shorter in the PR-negative/low cohort (p = 0.008) [24].
In this study, the clinicopathological characteristics of PR-high, PR-low, and PR-negative groups were compared. The results showed that compared with PR-negative group, the proportion of DFS>5 years and Ki-67 index ≤ 30% in PR-low and PR-high groups were significant higher (P < 0.001, P = 0.018). Compared with the PR-high group, the proportion of first-line POD24 occurrence in the PR-negative group was higher (P = 0.007), suggesting that PR-negative breast cancer patients were more likely to have disease recurrence within 5 years and disease progression within 2 years. COX regression analysis showed that DFS ≤ 5 years, without adjuvant radiation therapy and PR-negative were risk factors for PFS. First-line POD24 occurrence and PR-negative were risk factors for OS, indicating that the expression level of PR may affect the prognosis of patients. Further survival curve analysis also showed that the PFS and OS of the PR-negative group were significantly lower than those of the PR-high group (P = 0.001, P = 0.036), indicating that the prognosis of the PR-negative group was poor, which was similar to previous reports [24]. This study also found that the first-line PFS and OS of patients with PR-low expression were not statistically different from those of patients with PR-high expression, which may be related to the small number of patients with PR-low in this study. As we were able to collect data from only a single center and the number of patients using CDK4/6 inhibitors during the collection period was still limited by the high cost of the drug, this trial was still insufficient. Further studies with larger sample sizes are needed to analyze the prognosis difference between patients with PR-low and PR-high.
In addition, it was exciting to find that first-line POD24 occurrence was an independent risk factor for survival in the study population, independent of PR status. This analysis was mainly inspired by the study of the effect of POD24 on the prognosis of follicular lymphoma. Follicular lymphoma is a kind of inertia lymphoma, compared to other aggressive lymphoma, it is not easy to happen disease progression but hard to cure [25]. A large number of studies have proved when follicular lymphoma patients occur POD24, their prognosis are poorer, POD24 can be used as an independent predictor of prognosis of follicular lymphoma [26,27,28]. Compared with HER2-positive and triple-negative breast cancer, ER-positive HER2-negative breast cancer has a relatively ‘indolence’ of slow progression and good prognosis. Some patients with early-stage breast cancer can be cured, while those with advanced breast cancer are difficult to cure. Therefore, we analyzed the significance of first-line POD24 in advanced ER-high HER2-negative breast cancer patients, and our conclusion also verified that the prognosis of ER-positive HER2-negative breast cancer patients with first-line POD24 was worse and PR-negative patients were more likely to occur first-line POD24. This is the first time that the POD24 concept has been introduced into breast cancer, and its impact on breast cancer prognosis needs to be further investigated with a larger sample size. Meaningful, the effect of first-line POD24 on prognosis provides us with a new idea. We will continue to explore the effect of the time of first-line PFS on OS, and strive to provide more valuable prognostic indicators for patients.
In conclusion, PR-negative and first-line POD24 occurrence were risk factors of advanced ER-high HER2-negative breast cancer patients receiving CDK4/6 inhibitor combined with endocrine as first-line therapy. PR-negative patients had shortest PFS and OS. PR status may become a simple and accurate marker for predicting the efficacy of CDK4/6 inhibitors. For the first time, we found that the occurrence of first-line POD24 predicted shorter OS regardless of PR status. This is very important for clinical guidelines that doctors should use effective treatment as early as possible to improve the patient’s PFS and OS. However, this study still has some shortcomings, such as recall bias during patient follow-up and small sample size. With the increasing use of CDK4/6 inhibitors, more prospective studies are needed to confirm the effect of PR status and first-line POD24 on the prognosis of advanced ER-high HER2-negative breast cancer patients receiving CDK4/6 inhibitors combined with endocrine as first-line therapy.
Data availability
Data is provided within the manuscript and supplementary information files.
Abbreviations
- ASCO:
-
American Society of Clinical Oncology
- CAP:
-
College of American Pathologists
- CDK:
-
Cyclin-dependent kinase
- DFS:
-
Disease-free survival
- ER:
-
Estrogen receptor
- HER2:
-
Human epidermal growth factor receptor 2
- HR:
-
Hormone receptor
- HRs:
-
Hazard ratios
- MBC:
-
Metastatic breast cancer
- OS:
-
Overall survival
- PFS:
-
Progression-free survival
- POD24:
-
Progression of disease within 24 months
- PR:
-
Progesterone receptor
- pRb:
-
Phosphorylates retinoblastoma protein
- RECIST:
-
Response Evaluation Criteria In Solid Tumors
References
Sung H, Ferlay J, Siegel RL, et al. Global Cancer statistics 2020: GLOBOCAN estimates of incidence and Mortality Worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–49. https://doi.org/10.3322/caac.21660.
Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022;72(1):7–33. https://doi.org/10.3322/caac.21708.
Gradishar WJ, Moran MS, Abraham J, et al. Breast Cancer, Version 3.2022, NCCN Clinical Practice guidelines in Oncology. J Natl Compr Canc Netw. 2022;20(6):691–722. https://doi.org/10.6004/jnccn.2022.0030.
Reinert T, Cascelli F, de Resende CAA, Gonçalves AC, Godo VSP, Barrios CH. Clinical implication of low estrogen receptor (ER-low) expression in breast cancer. Front Endocrinol (Lausanne). 2022;13:1015388. Published 2022 Nov 24. https://doi.org/10.3389/fendo.2022.1015388 Jiang Z, Li J, Chen J,. Chinese Society of Clinical Oncology (CSCO) Breast Cancer Guidelines 2022. Transl Breast Cancer Res. 2022;3:13.
Goldner M, Pandolfi N, Maciel D, Lima J, Sanches S, Pondé N. Combined endocrine and targeted therapy in luminal breast cancer. Expert Rev Anticancer Ther. 2021;21(11):1237–51. https://doi.org/10.1080/14737140.2021.1960160.
Knudsen ES, Hutcheson J, Vail P, Witkiewicz AK. Biological specificity of CDK4/6 inhibitors: dose response relationship, in vivo signaling, and composite response signature. Oncotarget. 2017;8(27):43678–91. https://doi.org/10.18632/oncotarget.18435.
Cristofanilli M, Turner NC, Bondarenko I et al. Fulvestrant plus palbociclib versus fulvestrant plus placebo for treatment of hormone-receptor-positive, HER2-negative metastatic breast cancer that progressed on previous endocrine therapy (PALOMA-3): final analysis of the multicentre, double-blind, phase 3 randomised controlled trial [published correction appears in Lancet Oncol. 2016;17 (4):e136] [published correction appears in Lancet Oncol. 2016;17 (7):e270]. Lancet Oncol. 2016;17(4):425–439. https://doi.org/10.1016/S1470-2045(15)00613-0.
Finn RS, Rugo HS, Gelmon KA, et al. Long-term pooled Safety Analysis of Palbociclib in Combination with endocrine therapy for hormone Receptor-Positive/Human epidermal growth factor receptor 2-Negative advanced breast Cancer: updated analysis with up to 5 years of Follow-Up. Oncologist. 2021;26(5):e749–55. https://doi.org/10.1002/onco.13684.
Slamon DJ, Neven P, Chia S, et al. Ribociclib plus fulvestrant for postmenopausal women with hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer in the phase III randomized MONALEESA-3 trial: updated overall survival [published correction appears in Ann Oncol. 2021;32(10):1307]. Ann Oncol. 2021;32(8):1015–24. https://doi.org/10.1016/j.annonc.2021.05.353.
Mohammed H, Russell IA, Stark R et al. Progesterone receptor modulates ERα action in breast cancer [published correction appears in Nature. 2015;526(7571):144. Serandour, Aurelien A A[Corrected to Serandour, Aurelien A]]. Nature. 2015;523(7560):313–317. https://doi.org/10.1038/nature14583.
Li Z, Wei H, Li S, Wu P, Mao X. The role of progesterone receptors in breast Cancer. Drug Des Devel Ther. 2022;16:305–14. https://doi.org/10.2147/DDDT.S336643. Published 2022 Jan 26.
Bartlett JM, Brookes CL, Robson T, et al. Estrogen receptor and progesterone receptor as predictive biomarkers of response to endocrine therapy: a prospectively powered pathology study in the tamoxifen and exemestane adjuvant multinational trial. J Clin Oncol. 2011;29(12):1531–8. https://doi.org/10.1200/JCO.2010.30.3677.
Rubin SM, Sage J, Skotheim JM. Integrating Old and New paradigms of G1/S control. Mol Cell. 2020;80(2):183–92. https://doi.org/10.1016/j.molcel.2020.08.020.
Du Q, Guo X, Wang M, Li Y, Sun X, Li Q. The application and prospect of CDK4/6 inhibitors in malignant solid tumors. J Hematol Oncol. 2020;13(1):41. Published 2020 May 1. https://doi.org/10.1186/s13045-020-00880-8.
Asghar US, Kanani R, Roylance R, Mittnacht S. Systematic Review of Molecular Biomarkers Predictive of Resistance to CDK4/6 inhibition in metastatic breast Cancer. JCO Precis Oncol. 2022;6:e2100002. https://doi.org/10.1200/PO.21.00002.
Anurag M, Haricharan S, Ellis MJ. CDK4/6 inhibitor Biomarker Research: are we barking up the wrong tree? Clin Cancer Res. 2020;26(1):3–5. https://doi.org/10.1158/1078-0432.CCR-19-3119.
Yu KD, Cai YW, Wu SY, Shui RH, Shao ZM. Estrogen receptor-low breast cancer: Biology chaos and treatment paradox. Cancer Commun (Lond). 2021;41(10):968–80. https://doi.org/10.1002/cac2.12191.
Kurozumi S, Matsumoto H, Hayashi Y, et al. Power of PgR expression as a prognostic factor for ER-positive/HER2-negative breast cancer patients at intermediate risk classified by the Ki67 labeling index. BMC Cancer. 2017;17(1):354. https://doi.org/10.1186/s12885-017-3331-4. Published 2017 May 22.
Piasecka D, Składanowski AC, Kordek R, Romańska HM, Sądej R. Aspekty regulacji aktywności receptora progesteronu (PR) - znaczenie w progresji raka gruczołu piersiowego [Aspects of progesterone receptor (PR) activity regulation - impact on breast cancer progression]. Postepy Biochem. 2015;61(2):198–206.
Ethier JL, Ocaña A, Rodríguez Lescure A, et al. Outcomes of single versus double hormone receptor-positive breast cancer. A GEICAM/9906 sub-study. Eur J Cancer. 2018;94:199–205. https://doi.org/10.1016/j.ejca.2018.02.018.
Rocca A, Farolfi A, Maltoni R, et al. Efficacy of endocrine therapy in relation to progesterone receptor and Ki67 expression in advanced breast cancer. Breast Cancer Res Treat. 2015;152(1):57–65. https://doi.org/10.1007/s10549-015-3423-2.
Gao JJ, Cheng J, Bloomquist E, et al. CDK4/6 inhibitor treatment for patients with hormone receptor-positive, HER2-negative, advanced or metastatic breast cancer: a US Food and Drug Administration pooled analysis. Lancet Oncol. 2020;21(2):250–60. https://doi.org/10.1016/S1470-2045(19)30804-6.
Cristofanilli M, DeMichele A, Giorgetti C, et al. Predictors of prolonged benefit from palbociclib plus fulvestrant in women with endocrine-resistant hormone receptor-positive/human epidermal growth factor receptor 2-negative metastatic breast cancer in PALOMA-3. Eur J Cancer. 2018;104:21–31. https://doi.org/10.1016/j.ejca.2018.08.011.
Shao X, Zheng Y, Cao W, et al. Ki67 and progesterone receptor status predicts sensitivity to palbociclib: a real-world study. Ann Transl Med. 2021;9(8):707. https://doi.org/10.21037/atm-21-1340.
Jacobsen E. Follicular lymphoma: 2023 update on diagnosis and management. Am J Hematol. 2022;97(12):1638–51. https://doi.org/10.1002/ajh.26737.
Gordon MJ, Smith MR, Nastoupil LJ. Follicular lymphoma: the long and winding road leading to your cure? Blood Rev. 2023;57:100992. https://doi.org/10.1016/j.blre.2022.100992.
Casulo C, Dixon JG, Le-Rademacher J, et al. Validation of POD24 as a robust early clinical end point of poor survival in FL from 5225 patients on 13 clinical trials. Blood. 2022;139(11):1684–93. https://doi.org/10.1182/blood.2020010263.
Sortais C, Lok A, Tessoulin B, et al. Progression of disease within 2 years (POD24) is a clinically relevant endpoint to identify high-risk follicular lymphoma patients in real life. Ann Hematol. 2020;99(7):1595–604. https://doi.org/10.1007/s00277-020-04025-2.
Acknowledgements
Not applicable.
Funding
This research was supported by the basic scientific research business fees for universities in Heilongjiang Province and Haiyan youth fund of Harbin medical university cancer hospital(NO.JJQN2019-14).
Author information
Authors and Affiliations
Contributions
Liru Li and Qingyuan Zhang conceived the study. Lin Jia and Junning Peng completed the study. Liru Li and Nan Sun analyzed the data. Lin Jia, Junning Peng, Hongying Chen, Zhenyu Liu and Wenhui Zhao interpreted the data and wrote the manuscript. All authors have reviewed and approved the final version of the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Harbin Medical University Cancer Hospital, China, and has been performed in accordance with the ethical standards laid down in the 1964 Helsinki Declaration and its later amendments. This article does not contain any studies with animals performed by any of the authors. Informed consent was obtained from all individual participants included in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Jia, L., Peng, J., Sun, N. et al. Effect of PR status on the prognosis of advanced ER-high HER2-negative breast cancer patients receiving CDK4/6 inhibitor combined with endocrine as first-line therapy. BMC Cancer 24, 850 (2024). https://doi.org/10.1186/s12885-024-12621-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-024-12621-y