
Abstract
Background
Patients with hepatocellular carcinoma (HCC) who undergo transarterial chemoembolization (TACE) may have varied outcomes based on their liver function and tumor burden diversity. This study aims to assess the prognostic significance of the tumor burden score (TBS) in these patients and develop a prognostic model for their overall survival.
Methods
The study involved a retrospective analysis of 644 newly diagnosed HCC patients undergoing TACE treatment. The individuals were assigned randomly to a training cohort (n = 452) and a validation cohort (n = 192). We utilized a multivariate Cox proportional risk model to identify independent preoperative predictive factors. We then evaluated model performance using the area under the curve (AUC), consistency index (c-index), calibration curve, and decision curve analysis (DCA) methods.
Results
The multivariate analysis revealed four prognostic factors associated with overall survival: Tumor Burden Score, Tumor Extent, Types of portal vein invasion (PVI), and Child-Pugh score. The total score was calculated based on these factors. The model demonstrated strong discriminative ability with high AUC values and c-index, providing high net clinical benefits for patients. Based on the model’s scoring results, patients were categorized into high, medium, and low-risk groups. These results were validated in the validation cohort.
Conclusions
The tumor burden score shows promise as a viable alternative prognostic indicator for assessing tumor burden in cases of HCC. The new prognostic model can place patients in one of three groups, which will estimate their individual outcomes. For high-risk patients, it is suggested to consider alternative treatment options or provide the best supportive care, as they may not benefit significantly from TACE treatment.
Similar content being viewed by others

Background
Hepatocellular carcinoma (HCC) is the sixth most common cancer, and the second most lethal [1]. HCC ranks fourth in morbidity and second in mortality in China. It poses a serious threat to people’s health, with its high malignancy, rapid progression, poor prognosis, and a 5-year survival rate of only 12.1% [2]. Despite the improvements in screening and treatment over the years, a considerable proportion of patients are ineligible for surgical treatment at the time of diagnosis. According to many current HCC practice guidelines, transarterial chemoembolization (TACE) is considered one of the most commonly used local treatment modalities for intermediate-stage HCC [3, 4]. However, TACE is used in clinical practice beyond the guideline recommendations, not only for patients suffering from unresectable early HCC but also for those with liver-confined advanced disease [5,6,7]. Due to differences in tumor burden and liver reserve function among cancer patients, there may be heterogeneity in patients receiving TACE, which may result in variable outcomes [5, 8,9,10].
Researchers have explored the influencing factors of overall survival (OS) in HCC patients receiving TACE treatment, mainly including tumor characteristics and liver function [11]. Based on factors such as tumor size, number, liver function, and alpha-fetoprotein (AFP) level, researchers have developed several prognostic models, including the 6&12 score [5], HAP score [12], mHAP score [13], mHAPII score [14], mHAPIII score [15], and the pre-TACE prediction model [16]. However, these previous prognostic models have been questioned due to complex formulas, poor external validation results, and non-TACE populations [17,18,19], limiting their clinical application.
Recently, a new indicator called the “Tumor Burden Score (TBS)” has been proposed to stratify the risk of multifocal tumors [20]. The indicator considers tumor size and the number of tumors and has shown potential in predicting the prognosis of patients with colorectal liver metastasis, HCC, and intrahepatic cholangiocarcinoma who undergo surgical resection [20,21,22,23]. In this study, we created and validated a new model using preoperative TACE data in HCC patients. The model uses independent risk factors obtained from multivariate Cox analysis to determine the appropriateness of TACE as initial treatment.
Methods
Study population
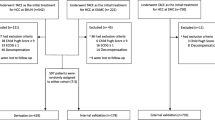
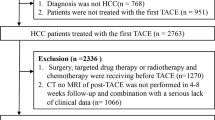
A total of 1276 patients with HCC who received the TACE procedure were enrolled from January 2017 to December 2021 at the First Affiliated Hospital of Wenzhou Medical University. Eventually, 644 HCC patients were included according to the inclusion and exclusion criteria (Fig. 1). Based on a training cohort verification cohort ratio of approximately 7: 3, 452 patients were included in the training cohort and 192 patients in the validation cohort. The study protocol was approved by the Institutional Ethics Committee of the First Affiliated Hospital of Wenzhou Medical University. This study adhered to the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the Ethics Committee of the First Affiliated Hospital of Wenzhou Medical University.

Diagram for inclusion of patients into the study. Abbreviations: TACE, transarterial chemoembolization; HAIC, hepatic artery infusion chemotherapy
Data collection
Clinical and sociodemographic data were collected from patients’ electronic medical records. Data captured included gender, age, etiology of hepatopathy (hepatitis B virus (HBV) infection or other causes), Barcelona Clinic Liver Cancer (BCLC) stage, China liver cancer staging (CNLC) stage, Child-Pugh score, presence of liver cirrhosis, presence of ascites, presence of extrahepatic metastasis (especially recorded lung metastasis and bone metastasis), level of AFP, and tumor characteristics such as maximum tumor size, number of liver lesions, lesion extent (unilobar or mutilobar), completeness of tumor capsule and types of portal vein invasion. The diagnosis of cirrhosis and PVI was based on clinical, radiological [computed tomography (CT) or magnetic resonance imaging (MRI)], and histological criteria.
TBS was calculated using a combination of tumor size and the total number of tumors for each patient [20]. TBS was defined as the distance from the origin to a point on a plane, incorporating the maximum tumor diameter and the number of intrahepatic tumors. The formula used to calculate TBS was: (maximum tumor diameter)2 + (number of liver lesions)2=TBS2 (Fig. 2). Cut-off values for TBS were determined using X-tile, a retrospective bioinformatics tool developed by Camp and colleagues [24]. Patients were divided into three groups according to the TBS: high (over 10.00; 185, 28.6%), medium (5.20–10.00; 227, 35.4%), and low (less than 5.20; 269, 36.0%). Increasing TBS was associated with a progressively higher risk of death (referent low TBS, medium TBS, HR 3.20, 95% CI 2.39–4.28, P < 0.001; high TBS, HR 6.62, 95% CI 4.72–9.27, P < 0.001).
The primary outcome measure was OS, defined as the time from the date of TACE to the date of death or last follow-up. Patients who were alive at last follow-up or lost to follow-up were censored. Several scoring systems, namely 6&12 score [5], HAP score [12], mHAP score [13], mHAPII score [14], mHAPIII score [15], and the pre-TACE-Predict Model [16], were calculated based on their criteria.

Scatter plot about maximum tumor diameter (x-axis) and number of intrahepatic tumors (y-axis), \( {\left(\text{m}\text{a}\text{x}\text{i}\text{m}\text{u}\text{m} \text{t}\text{u}\text{m}\text{o}\text{r} \text{d}\text{i}\text{a}\text{m}\text{e}\text{t}\text{e}\text{r}\right)}^{2}+{\left(\text{n}\text{u}\text{m}\text{b}\text{e}\text{r} \text{o}\text{f} \text{l}\text{i}\text{v}\text{e}\text{r} \text{l}\text{e}\text{s}\text{i}\text{o}\text{n}\text{s}\right) }^{2}={\text{T}\text{B}\text{S}}^{2}\). Abbreviations: TBS, Tumor Burden Score
Treatment procedure
The experienced interventional radiologists performed the conventional TACE (cTACE) procedure. Firstly, they used the modified Seldinger technique to insert an angiographic catheter through the right femoral artery and access the hepatic artery. They then performed angiography of the common hepatic artery and superior mesenteric artery to visualize hepatic artery anatomy and portal vein patency. Next, a microcatheter was super-selected to the tumor-feeding artery, and then a mixture of chemotherapeutics and lipiodol was injected, the dosage of which was adjusted according to the number, maximum diameter, and embolization extent of the tumor lesions. Gelatin sponge or embolic microsphere was used for embolization until the tumor arterial flow was reduced on angiography. The chemotherapy drugs mainly include pirarubicin (10-50 mg), epirubicin (10-50 mg), mitomycin (10 mg), oxaliplatin (50-150 mg), raltitrexed (1-4 mg) and 5-fluorouracil (250-1000 mg). The range of lipiodol is 1 to 30 ml.
During the drug-eluting beads-TACE (DEB-TACE) procedure, the recommended injection rate for drug-loaded microspheres is 1 ml/min. The microspheres should be well distributed and evenly suspended during the injection process. When the flow rate of microspheres loaded with drug and contrast agent suspension in the artery has not emptied within 3–4 cardiac cycles, the injection should be stopped as it marked the endpoint of embolization. After a pause of 5 to 15 min, angiography was repeated. If tumor staining was still present, continue embolization until the endpoint of embolization was reached (tumor staining disappeared). Lesions that had not yet reached the endpoint of embolization could be further embolized with drug-loaded microspheres or blank microspheres, with a single embolization dose not exceeding 4 ml. Other particle embolic agents could be injected or re-embolized if economic conditions were limited.
TACE procedures would be repeated if viable tumor lesions or new emerging lesions were found by imaging examination in patients with tolerable physical conditions.
Statistical analysis and model development
The presentation of quantitative variables following a normal distribution was expressed as mean ± standard deviation. Otherwise, they were described as the median and interquartile range (IQR). These data were compared using either Student’s t-test or non-parametric Mann-Whitney U test. Categorical variables were presented as their n (%) and compared using the Chi-squared test or Fisher’s exact test. In the training cohort, univariate Cox proportional hazards regression analysis was performed to determine the association of each parameter with all-cause mortality. A correlation heat map was performed to check the variables’ collinearity included in the previous step. A correlation coefficient greater than 0.7 indicated multicollinearity. Next, the variables with a P value less than 0.10 in the univariate regression analysis were included. Cox proportional hazards regression analysis with backward stepwise variable selection was used to extract independent predictors, while variables with collinearity were not included in the same model simultaneously. The new model was built by backward stepwise variable selection, with entry criteria set at the P < 0.05 level. To compare the performance of different models, the area under the curve (AUC) values were calculated, and the model with the highest AUC value was considered the final model. The β regression coefficients were multiplied by six and rounded to the nearest unit to obtain the score of the variable. The sum of the scores for each variable constituted the final score for each patient. Both TBS stratification and patient mortality risk stratification were carried out using x-tile software, a retrospective analysis tool. Statistical analysis was performed using R software (version 4.3.1, www.r-project.org). A two-sided P value less than 0.05 was considered statistically significant. The R packages used in this study are listed in Supplementary Table 1.
Model evaluation and validation
To determine the accuracy of the predictive model, we used two methods: the area under the time-dependent receiver operating characteristic (ROC) curve and the concordance index (c-index). The ROC curve measures the predictive ability of the model over time, while the c-index estimates the probability that the predicted results match the actual results. Calibration, on the other hand, refers to the agreement between estimated and actual risk. We depicted the calibration curves to evaluate calibration. Another important consideration in clinical practice is the issue of benefits. We analyzed the benefits of the model using decision curve analysis (DCA) by comparing it to default strategies of treating all or no patients.
We evaluated the model using the above methods on both the training cohort and validation cohorts, comparing them with other models, like 6&12 score [5], HAP score [12], mHAP score [13], mHAPII score [14], mHAPIII score [15], and pre-TACE-Predict Model [16].
Results
Characteristics of training and validation cohorts
A total of 644 patients met the eligibility criteria and were included in the final cohort and randomized into training (N1 = 452, 70%) and validation (N2 = 192, 30%) cohorts (Fig. 1). The baseline characteristics of the two cohorts were comparable, and there was no significant difference between patients (Table 1). 85% of the enrolled patients were male, 15% were female, and the median age was 59.5 years old. HBV was the main cause of the patients, accounting for 79%, and 75% of patients had liver cirrhosis. The liver function grading was mainly distributed in A5, A6, and B7. In terms of tumor characteristics, the median of the maximum diameter of HCC was 6.1 cm (IQR: 3, 9.7), and most patients did not have portal vein invasion or extrahepatic metastasis. TBS was almost evenly distributed among the low, medium, and high groups. In a subgroup analysis based on the BCLC stage, significant differences in OS were observed among high, medium, and low TBS patients in the BCLC stage B/C group. Patients with high TBS had the worst prognosis in the BCLC stage B/C group (Supplementary Fig. 1B). However, it is important to note that TBS did not significantly affect BCLC stage 0/A stage (Supplementary Fig. 1A). The median OS for the training cohort was 33 months (95% CI: 29, 39), and 32 months (95% CI: 30, NA) for the internal validation cohort (Fig. 3).

Kaplan-Meier survival curves of the training cohort and validation cohort
Building a prognostic model in training cohort
Before constructing our model, we conducted univariate and multivariate analyses of prognostic factors in our inclusive population. Based on the results of univariate analysis (Table 2), BCLC-stage, CNLC-stage, Child-Pugh score, tumor size, tumor number, tumor burden score, tumor extent, tumor capsule, types of PVI, bone meta, ascites, and AFP were correlated with OS (p < 0.05). Subsequently, we completed the correlation analysis. We defined a correlation coefficient greater than 0.7 as a strong correlation. We found a strong correlation between BCLC-stage and CNLC-stage, tumor size and TBS, tumor number and tumor capsule, and BCLC-stage and types of PVI (Fig. 4). For factors with strong correlation, we selected only one from each group for permutation and combination with other factors. Then we performed multiple stepwise regression analyses and ultimately selected the model with the highest AUC value obtained as our final model (Table 2).
After a backward stepwise removal of variables, four remained significant for OS: Child-Pugh score, TBS, Tumor extent, and Types of PVI (p < 0.05). We constructed the model using two methods integrating these predictors. One used the nomogram to predict the 1-, 2-, 3-, and 5-year OS (Supplementary Fig. 2), and the other used the calculated β values (regression coefficient) of variables derived from stepwise Cox regression analysis multiplied by 6 and rounded to get a new score (Table 3). Comparing the AUC values of the two models, it was found that the second assignment scoring model had a higher AUC value (Supplementary Figs. 4 and 10A). Therefore, we selected the second model as our final model.

Correlation heat map between various factors
Performance assessment and validation
ROC analysis and c-index are commonly used as a stick to evaluate the predictive performance of clinical research, namely discrimination [25, 26]. The AUCs for 1-, 2-, 3-, and 5-year OS in the training cohort were 0.847, 0.803, 0.777, and 0.768, respectively (Fig. 10A and C). Similarly, in the validation cohort, the AUCs for 1-, 2-, 3-, and 5-year OS were 0.862, 0.845, 0.788, and 0.733, respectively (Fig. 10B and D). The C-indexes for OS prediction in the training and validation cohorts were 0.75 and 0.75 respectively. The curve of the c-index of the training and validation cohorts over time is shown in Fig. 5. The values for 1-, 2-, 3-, and 5-year were 0.787, 0.738, 0.732, and 0.715 for the training cohort, while the validation cohort were 0.803, 0.766, 0.745 and 0.732, respectively. Another evaluation method is calibration, which compares the predicted survival rate to the actual survival rate. The calibration curve visually demonstrates the accuracy of the model’s predictions [27]. Figure 6 showed that the predicted OS results of the 1-, 2-, 3-, and 5-year survival have good consistency with actual observations both in the training and validation cohorts. In addition to measures such as discrimination and calibration, DCA is an important verification tool for evaluating the clinical benefits of a model and comparing multiple models to determine the best decision-making model [28]. Figure 7 shows that our model has a significant net clinical benefit in predicting survival.
HCC patients were classified into three levels using x-tile based on the total score obtained: low-risk group (0–7), medium-risk group (8–12), and high-risk group (greater than 13). Kaplan-Meier curves of the two cohorts are shown in Fig. 8. For the low, the medium OS was 44 months (95% CI, 39-NA); for the medium and the high, the medium OS was 18 months (95% CI, 16–27) and 8 months (95% CI, 6–13), respectively (p < 0.0001). In the validation cohort, the median OS was 52 months (95% CI, 43–63) for the low-risk group, 24 months (95% CI, 16-NA) for the medium-risk group, and 13 months (95% CI, 6-NA) for the high-risk group (p < 0.0001). In the training cohort, there was a significant statistical difference in OS among three different risk stratification groups for BCLC stage 0/A patients (log-rank p < 0.0001, Fig. 9A), and for BCLC stage B/C (log-rank p < 0.0001, Fig. 9B). The same results were obtained in the validation group (Supplementary Fig. 3).

Time-dependent concordance index curve of the new model in the training and validation cohort. (A) The c-index for the training cohort. (B) The c-index for the validation cohort

The plots of calibration of 1-year, 2-year, 3-year, and 5-year overall survival. Calibration curves of my model in training cohort (A). Calibration curves of my model in the validation cohort (B). The dotted lines represent the ideal predictive model, and the solid red line represents the observed model

Clinical decision curve analysis for the training cohort (A) and validation cohort (B) for clinical benefits. The black line represents the net benefit of the strategy of treating all patients. The gray line represents the net benefit of the strategy of treating no patients

Kaplan-Meier survival curves of patients with HCC stratified by the new model in the training cohort (A) and in the validation cohort (B)

Kaplan-Meier survival curves of patients in the training cohort stratified by the new model in the BCLC 0/A (A) and BCLC B/C (B)
Comparison of different scoring systems
As previously mentioned, both AUC and c-index are used to evaluate discrimination ability. DCA provides a clear demonstration of the net clinical benefits of models for patients. We calculated the results of several other models, including 6&12 score [5], HAP score [12], mHAP score [13], mHAPII score [14], mHAPIII score [15], and pre-TACE-Predict Model [16]. Our model consistently had AUC values higher than 0.80 for both 1-year and 2-year in both cohorts, surpassing the AUC values of other models. In the training cohort, the AUC values of the 3-year and 5-year were higher than 0.75, outperforming other models. Similarly, in the validation cohort, our model had higher AUC values for 3-year and 5-year compared to most models (Fig. 10C and D).
The C-indexes of these models were also calculated. The HAP, mHAP, and mHAPII models had C-index values below 0.7 in the training cohort, while our model consistently had C-index values above 0.7, surpassing other models (Fig. 5). Regarding the validation cohort, the C-index values of 6&12, HAP, mHAP, and mHAPIII were all below 0.7. Our prediction model was above 0.7 and performed better than other models.
Our predictive model showed a better ability to predict survival compared to the all-patients dead scheme and the no-patients dead scheme, as shown by the DCA curve in Fig. 7. The DCA curve demonstrated that our model yielded greater net benefit improvement compared to other prognostic evaluation systems.

Time-dependent ROC curve for predicting OS at 1-, 2-, 3-, and 5-year in the training cohort (A) and in the validation cohort (B). Comparison of time-dependent AUC values of different prediction models at 1-, 2-, 3-, and 5-year in the training cohort (C) and the validation cohort (D)
Discussion
The high malignancy, rapid progression, and poor prognosis have seriously threatened the lives and health of our people. TACE is the most commonly used treatment method for mid-term HCC [3, 4]. However, TACE is also applied to patients suffering from unresectable early HCC and those with liver-confined advanced diseases [5,6,7]. However, due to differences in tumor burden and liver reserve function, patients often have different prognosis [5, 8,9,10]. This heterogeneity makes prognosis prediction challenging, therefore making treatment decisions for these patients remains difficult. Despite the development of numerous prognostic models to predict the effectiveness of TACE treatment, there is currently no standardized policy to determine which patients can benefit from TACE. The objective of this study is to construct and verify a new model for predicting the prognostic role of HCC patients receiving TACE.
When the Milan Criteria (MC) was first proposed in 1996, they quickly became the cornerstone for selecting and managing liver cancer patients. However, due to the variable tumor burden, significant differences in treatment choices may be present for patients who exceed MC. To address this, up-to-7 criteria and up-to-11 criteria for evaluating the burden of liver cancer have been proposed. These two models combine the maximum nodule diameter and the number of nodules, with a total of no more than 7 or 11. Unlike the traditional method of using the maximum diameter and the number of nodules as the burden of liver cancer, TBS has recently been proposed to minimize the heterogeneity of cancer patients. Duvoux’s team proposed a French AFP liver transplantation model consisting of maximum tumor diameter, number of tumors, and AFP level, with transplant eligibility of ≤ 2 points. As long as the AFP is ≤ 100 (0 points) and the maximum tumor diameter is ≤ 3 cm (0 points), the patient can be put on the waiting list regardless of the number of tumors in the patient [29], which means that patients can easily be on the waiting list, provided they have micronodular HCC and are AFP negative. However, a later study by Mazzotta found that there was a significant difference in 3-year and 5-year survival among those with AFP ≤ 2 grouped with a cutoff of 5 after entering the waiting list and before undergoing liver transplantation [30]. Tumor diameter and number were found to have important prognostic value in liver transplant patients. TBS is an index that combines them to reduce the bias in prognostic estimation due to the truncated values described above. TBS is a promising tool for predicting the outcomes of HCC patients after liver transplantation. A study by Moris D et al. showed that patients with high TBS had worse OS and recurrence free survival. When the study superimposed TBS on the Milan standard, it was found that patients with higher TBS values within the Milan standard had a higher risk of recurrence [23]. Further research is needed to determine whether our TBS-based model can be extended to patients with other treatment options. It has been proven to have excellent prognostic discrimination in colorectal liver metastasis, liver cancer resection, and liver transplant patients [20, 22, 23, 31].
In this study, we performed an OS analysis on the TBS values of all the patients included. The results showed that it could distinguish the OS of liver cancer patients receiving TACE, consistent with previous research results [21].
In subgroup analysis based on BCLC stage, it was found that patients with high TBS had the worst prognosis in the BCLC B/C. However, TBS did not play a role in the early BCLC stage. According to the definition of BCLC, BCLC 0/A refers to a single nodule or multiple small nodules. So even if the patient is in the high or medium TBS group, the increase in TBS is mostly caused by isolated large nodules, TACE treatment still has a nice effect on the tumor-feeding artery, leading to a good prognosis, similar to the conclusions obtained in previous studies [21].
We then added tumor extent (Mutilobar vs. Unilobar) and PVI level (no or below branches or above branches) to the TBS to jointly form tumor features. Combining with the Child-Pugh score, we constructed a prognostic prediction model that demonstrated excellent survival prediction performance. As the Child-Pugh score, TBS, tumor distribution increase, and the grade of PVI increases, the survival prognosis of patients will deteriorate. We validated the model in the training and validation cohorts using AUC and C-index, and the validation cohort had even better discriminative ability with higher AUC and C-index values. We also used a nomogram-like approach to estimate patient survival based on patient scores, which created a graphical statistical prognostic model that can predict the probability of death over time (Supplementary Fig. 5) [32, 33]. From this, we can see that as patient scores increase, the survival rate gradually deteriorates. In clinical practice, we can infer the survival rate of patients at different times in their basic clinical data. Moreover, we divided HCC patients into three different risk groups based on the predicted risk of death using the model. There was a significant difference in survival among the three groups in both the training and validation cohorts. Additionally, survival analysis on the training and validation cohorts showed that our model has prognostic stratification ability for both early and advanced HCC. With the continuous development of clinical trials of new drugs [34, 35], our model could guide the identification of patients who may not benefit from TACE treatment, allowing for timely shifts to systematic or evidence-based treatment when poor patient survival outcomes were estimated. Therefore, our prediction model may have sufficient external utility and potential for further clinical application in the future.
Our scoring system includes risk factors consistent with previous research. TBS represents the maximum diameter of the tumor and the number of intrahepatic tumors. To our knowledge, our study was the first to incorporate TBS into the TACE treatment prognosis model for HCC, providing solid evidence that TBS has good discrimination ability as a tumor burden indicator. PVI and tumor extension represent the invasiveness of tumor biology [36,37,38,39]. Unlike other prognostic models for solid tumors, liver reserve function plays an important role in disease analysis and prognosis of patients. The Child-Pugh score represents liver reserve status and evaluates liver tolerance to TACE, widely used in liver reserve function evaluation and predictive systems [4, 40, 41]. The traditional liver cancer monitoring indicator AFP did not have significant prognostic value in this study. It remained a controversial biomarker for liver cancer, as many patients exhibit negative AFP and its sensitivity and specificity are not high, similar to some previous research findings [42, 43]. Our analysis showed that our scoring system predicted the survival of TACE-treated patients better than other scoring systems. The model has the highest discriminatory ability to predict OS due to its maximum AUC value and c-index while providing relatively higher clinical net benefits for patients from the DCA results. Above all, our model has the following advantages. Firstly, it includes simple clinical indicators that are easily obtainable. Secondly, it can be applied to patients outside of TACE guidance standards. Lastly, the probability of specific survival time can be provided to clinical doctors.
As our model demonstrates prognostic stratification significance for HCC patients receiving TACE at different stages, it is important to note that for HCC patients treated with other methods, such as surgery, radiofrequency, liver transplantation, etc., they cannot be validated from our inclusion population due to limitations in inclusion and exclusion criteria. For patients undergoing surgical resection treatment, OS gradually deteriorates with increasing TBS. Regardless of the BCLC stage, there was no difference in OS between patients with similar TBS groups (BCLC-A/medium TBS and BCLC-B/medium TBS, P = 0.930; BCLC-A/high TBS and BCLC-B/high TBS, P = 0.175). Patients with BCLC-B HCC with medium TBS have better OS than those with BCLC-A with high TBS [22].
This study has certain limitations that should be considered when interpreting the results. Like all retrospective studies, there may be selection bias in determining which patients receive TACE treatment. Moreover, most of the included patients had HBV infection-related liver cancer, so we still need more external validation when extrapolating the results to other etiological populations. Additionally, the validation group used in our research is from the same institution, so external data validation from multiple centers is necessary. Lastly, this study only focused on patients receiving TACE as their initial treatment. Studying patients who have previously received other treatments, such as surgery or radiofrequency ablation, may broaden the application scope of the model.
Conclusion
In summary, this study developed a simple, clinically relevant, and easily accessible model to predict the prognosis of patients receiving TACE treatment, which includes three tumor features and one liver function indicator. One of the indicators, TBS, is entering the TACE prognostic model for the first time. From the model prediction, high-risk patients may not benefit from TACE treatment and should consider alternative treatments. This model has been validated in the validation cohort and performs well compared to other prognostic systems, but it still needs to be prospectively validated in a larger cohort to confirm the suitability of our findings.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- HCC:
-
Hepatocellular carcinoma
- TACE:
-
Transarterial chemoembolization
- TBS:
-
Tumor burden score
- AUC:
-
Area under the curve
- c-index:
-
Consistency index
- DCA:
-
Decision curve analysis
- PVI:
-
Portal vein invasion
- OS:
-
Overall survival
- AFP:
-
Alpha-fetoprotein
- HBV:
-
Hepatitis B virus
- BCLC:
-
Barcelona Clinic Liver Cancer
- CNLC:
-
China liver cancer staging
- CT:
-
Computed tomography
- MRI:
-
Magnetic resonance imaging
- cTACE:
-
Conventional TACE
- DEB-TACE:
-
Drug-eluting beads TACE
- IQR:
-
Interquartile range
- ROC:
-
Receiver operating characteristic
References
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global Cancer statistics 2020: GLOBOCAN estimates of incidence and Mortality Worldwide for 36 cancers in 185 countries. Cancer J Clin. 2021;71(3):209–49.
Chen W, Zheng R, Baade PD, Zhang S, Zeng H, Bray F, Jemal A, Yu XQ, He J. Cancer statistics in China, 2015. Cancer J Clin. 2016;66(2):115–32.
Lu J, Zhao M, Arai Y, Zhong BY, Zhu HD, Qi XL, de Baere T, Pua U, Yoon HK, Madoff DC, et al. Clinical practice of transarterial chemoembolization for hepatocellular carcinoma: consensus statement from an international expert panel of International Society of Multidisciplinary Interventional Oncology (ISMIO). Hepatobiliary Surg Nutr. 2021;10(5):661–71.
Reig M, Forner A, Rimola J, Ferrer-Fàbrega J, Burrel M, Garcia-Criado Á, Kelley RK, Galle PR, Mazzaferro V, Salem R, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–93.
Wang Q, Xia D, Bai W, Wang E, Sun J, Huang M, Mu W, Yin G, Li H, Zhao H, et al. Development of a prognostic score for recommended TACE candidates with hepatocellular carcinoma: a multicentre observational study. J Hepatol. 2019;70(5):893–903.
Xu L, Peng ZW, Chen MS, Shi M, Zhang YJ, Guo RP, Lin XJ, Lau WY. Prognostic nomogram for patients with unresectable hepatocellular carcinoma after transcatheter arterial chemoembolization. J Hepatol. 2015;63(1):122–30.
Bargellini I, Sacco R, Bozzi E, Bertini M, Ginanni B, Romano A, Cicorelli A, Tumino E, Federici G, Cioni R, et al. Transarterial chemoembolization in very early and early-stage hepatocellular carcinoma patients excluded from curative treatment: a prospective cohort study. Eur J Radiol. 2012;81(6):1173–8.
Chang Y, Jeong SW, Young Jang J, Jae Kim Y. Recent Updates of Transarterial Chemoembolilzation in Hepatocellular Carcinoma. International journal of molecular sciences 2020, 21(21).
Mao S, Shan Y, Yu X, Huang J, Fang J, Wang M, Fan R, Wu S, Lu C. A new prognostic model predicting hepatocellular carcinoma early recurrence in patients with microvascular invasion who received postoperative adjuvant transcatheter arterial chemoembolization. Eur J Surg Oncology: J Eur Soc Surg Oncol Br Association Surg Oncol. 2023;49(1):129–36.
Li J, Li C, Zhu G, Yang J, Zhang Y, Yu Z, Xia J. A novel nomogram to predict survival of patients with hepatocellular carcinoma after transarterial chemoembolization: a tool for retreatment decision making. Annals Translational Med. 2023;11(2):68.
Müller L, Stoehr F, Mähringer-Kunz A, Hahn F, Weinmann A, Kloeckner R. Current strategies to identify patients that will benefit from TACE treatment and future directions a practical step-by-step guide. J Hepatocellular Carcinoma. 2021;8:403–19.
Kadalayil L, Benini R, Pallan L, O’Beirne J, Marelli L, Yu D, Hackshaw A, Fox R, Johnson P, Burroughs AK, et al. A simple prognostic scoring system for patients receiving transarterial embolisation for hepatocellular cancer. Annals Oncology: Official J Eur Soc Med Oncol. 2013;24(10):2565–70.
Pinato DJ, Arizumi T, Allara E, Jang JW, Smirne C, Kim YW, Kudo M, Pirisi M, Sharma R. Validation of the hepatoma arterial embolization prognostic score in European and Asian populations and proposed modification. Clin Gastroenterol Hepatology: Official Clin Pract J Am Gastroenterological Association. 2015;13(6):1204–1208e1202.
Park Y, Kim SU, Kim BK, Park JY, Kim DY, Ahn SH, Park YE, Park JH, Lee YI, Yun HR, et al. Addition of tumor multiplicity improves the prognostic performance of the hepatoma arterial-embolization prognostic score. Liver International: Official J Int Association Study Liver. 2016;36(1):100–7.
Cappelli A, Cucchetti A, Cabibbo G, Mosconi C, Maida M, Attardo S, Pettinari I, Pinna AD, Golfieri R. Refining prognosis after trans-arterial chemo-embolization for hepatocellular carcinoma. Liver International: Official J Int Association Study Liver. 2016;36(5):729–36.
Han G, Berhane S, Toyoda H, Bettinger D, Elshaarawy O, Chan AWH, Kirstein M, Mosconi C, Hucke F, Palmer D, et al. Prediction of Survival among patients receiving Transarterial Chemoembolization for Hepatocellular Carcinoma: a response-based Approach. Hepatology (Baltimore MD). 2020;72(1):198–212.
Kim DS, Kim BK, Lee JS, Lee HW, Park JY, Kim DY, Ahn SH, Kim SU. Validation of Pre-/Post-TACE-Predict models among patients with Hepatocellular Carcinoma receiving Transarterial Chemoembolization. Cancers 2021, 14(1).
Bourlière M, Pénaranda G, Adhoute X, Bronowicki JP. The six-and-twelve score for TACE treatment: does it really help us? J Hepatol. 2019;71(5):1051–2.
Bannangkoon K, Hongsakul K, Tubtawee T. Validation of the ALBI-TAE model and comparison of seven scoring systems for predicting survival outcome in patients with intermediate-stage hepatocellular carcinoma undergoing chemoembolization. Cancer Imaging: Official Publication Int Cancer Imaging Soc. 2023;23(1):51.
Sasaki K, Morioka D, Conci S, Margonis GA, Sawada Y, Ruzzenente A, Kumamoto T, Iacono C, Andreatos N, Guglielmi A, et al. The Tumor Burden score: a New Metro-ticket Prognostic Tool for Colorectal Liver metastases based on Tumor size and number of tumors. Ann Surg. 2018;267(1):132–41.
Ho SY, Liu PH, Hsu CY, Ko CC, Huang YH, Su CW, Lee RC, Tsai PH, Hou MC, Huo TI. Tumor burden score as a new prognostic marker for patients with hepatocellular carcinoma undergoing transarterial chemoembolization. J Gastroenterol Hepatol. 2021;36(11):3196–203.
Tsilimigras DI, Moris D, Hyer JM, Bagante F, Sahara K, Moro A, Paredes AZ, Mehta R, Ratti F, Marques HP, et al. Hepatocellular carcinoma tumour burden score to stratify prognosis after resection. Br J Surg. 2020;107(7):854–64.
Moris D, Shaw BI, McElroy L, Barbas AS. Using Hepatocellular Carcinoma Tumor Burden score to Stratify Prognosis after Liver Transplantation. Cancers 2020, 12(11).
Camp RL, Dolled-Filhart M, Rimm DL. X-tile: a new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin cancer Research: Official J Am Association Cancer Res. 2004;10(21):7252–9.
Harrell FE Jr., Lee KL, Mark DB. Multivariable prognostic models: issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat Med. 1996;15(4):361–87.
Walker SP. The ROC curve redefined - optimizing sensitivity (and specificity) to the lived reality of Cancer. N Engl J Med. 2019;380(17):1594–5.
Sun Y, Li Z, Liu X, Cao S, Liu X, Hu C, Tian Y, Xu J, Wang D, Zhou X, et al. A Nomogram for Prediction of Survival in patients after Gastrectomy within enhanced recovery after surgery (ERAS): a single-Center Retrospective Study. Med Sci Monitor: Int Med J Experimental Clin Res. 2020;26:e926347.
Van Calster B, Wynants L, Verbeek JFM, Verbakel JY, Christodoulou E, Vickers AJ, Roobol MJ, Steyerberg EW. Reporting and interpreting decision curve analysis: a guide for investigators. Eur Urol. 2018;74(6):796–804.
Duvoux C, Roudot-Thoraval F, Decaens T, Pessione F, Badran H, Piardi T, Francoz C, Compagnon P, Vanlemmens C, Dumortier J, et al. Liver transplantation for hepatocellular carcinoma: a model including α-fetoprotein improves the performance of Milan criteria. Gastroenterology. 2012;143(4):986–94. e983; quiz e914-985.
Mazzotta AD, Pascale A, Cano L, Rosmorduc O, Allard MA, Sa Cunha A, Adam R, Cherqui D, Vibert E, Golse N. Number of hepatocellular carcinoma nodules in patients listed for liver transplantation within alpha-fetoprotein score: a new prognostic risk factor. Transpl International: Official J Eur Soc Organ Transplantation. 2021;34(5):954–63.
Lima HA, Moazzam Z, Endo Y, Alaimo L, Shaikh C, Munir MM, Resende V, Guglielmi A, Marques HP, Cauchy F, et al. TBS-Based preoperative score to predict non-transplantable recurrence and identify candidates for Upfront Resection Versus Transplantation for Hepatocellular Carcinoma. Ann Surg Oncol. 2023;30(6):3363–73.
Balachandran VP, Gonen M, Smith JJ, DeMatteo RP. Nomograms in oncology: more than meets the eye. Lancet Oncol. 2015;16(4):e173–180.
Iasonos A, Schrag D, Raj GV, Panageas KS. How to build and interpret a nomogram for cancer prognosis. J Clin Oncology: Official J Am Soc Clin Oncol. 2008;26(8):1364–70.
Llovet JM, Kelley RK, Villanueva A, Singal AG, Pikarsky E, Roayaie S, Lencioni R, Koike K, Zucman-Rossi J, Finn RS. Hepatocellular carcinoma. Nat Reviews Disease Primers. 2021;7(1):6.
Sangro B, Sarobe P, Hervás-Stubbs S, Melero I. Advances in immunotherapy for hepatocellular carcinoma. Nat Reviews Gastroenterol Hepatol. 2021;18(8):525–43.
Li Z, Zhao M, Qi X, Tang Y, Cheng S. Mechanisms of portal vein tumour thrombus formation and development in patients with hepatocellular carcinoma. J Cell Mol Med. 2023;27(15):2103–11.
Shi J, Lai EC, Li N, Guo WX, Xue J, Lau WY, Wu MC, Cheng SQ. Surgical treatment of hepatocellular carcinoma with portal vein tumor thrombus. Ann Surg Oncol. 2010;17(8):2073–80.
Shuqun C, Mengchao W, Han C, Feng S, Jiahe Y, Guanghui D, Wenming C, Peijun W, Yuxiang Z. Tumor thrombus types influence the prognosis of hepatocellular carcinoma with the tumor thrombi in the portal vein. Hepatogastroenterology. 2007;54(74):499–502.
Zhou XH, Li JR, Zheng TH, Chen H, Cai C, Ye SL, Gao B, Xue TC. Portal vein tumor thrombosis in hepatocellular carcinoma: molecular mechanism and therapy. Clin Exp Metastasis. 2023;40(1):5–32.
Bruix J, Sherman M. Management of hepatocellular carcinoma: an update. Hepatology (Baltimore MD). 2011;53(3):1020–2.
Knavel Koepsel EM, Smolock AR, Pinchot JW, Kim CY, Ahmed O, Chamarthy MRK, Hecht EM, Hwang GL, Kaplan DE, Luh JY, et al. ACR appropriateness Criteria® Management of Liver Cancer: 2022 update. J Am Coll Radiology: JACR. 2022;19(11s):390–s408.
Hu X, Chen R, Wei Q, Xu X. The Landscape of Alpha Fetoprotein in Hepatocellular Carcinoma: where are we? Int J Biol Sci. 2022;18(2):536–51.
Hanif H, Ali MJ, Susheela AT, Khan IW, Luna-Cuadros MA, Khan MM, Lau DT. Update on the applications and limitations of alpha-fetoprotein for hepatocellular carcinoma. World J Gastroenterol. 2022;28(2):216–29.
Funding
This study was supported in part by the National Natural Science Foundation of China (Grant No. 81972233). Also supported by Major scientific and technological innovation project of Wenzhou Science and Technology Bureau (Grant No. ZY2021009).
Author information
Authors and Affiliations
Contributions
Jiawei Lin is the first author. Jiawei Lin and Jie Li contributed to the study design and previous literature search. Yifan Kong, Junhui Yang, and Yunjie Zhang contributed equally to this work. Jiawei Lin, Jie Li, Yifan Kong, Junhui Yang, and Yunjie Zhang collected data and analyzed it. Jiawei Lin contributed to the writing of the manuscript. Guoqing Zhu, Zhijie Yu and Jinglin Xia performed the analysis with constructive discussions. Jinglin Xia is the correspondent author. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study conformed to the ethical guidelines of the 1975 Declaration of Helsinki and has been approved by the Ethics Committee of the First Affiliated Hospital of Wenzhou Medical University. Written informed consent for publication was obtained from all participants.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lin, J., Li, J., Kong, Y. et al. Construction of a prognostic model for hepatocellular carcinoma patients receiving transarterial chemoembolization treatment based on the Tumor Burden Score. BMC Cancer 24, 306 (2024). https://doi.org/10.1186/s12885-024-12049-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-024-12049-4