
Abstract
Background
Platelet distribution width (PDW), but not platelet count, was found to more comprehensively reflect platelet activity. The present study, thus, aimed to evaluate the prognostic value of PDW to lymphocyte ratio (PDWLR) in patients with hepatocellular carcinoma (HCC) following hepatectomy.
Methods
Patients following hepatectomy were analyzed retrospectively. The Kaplan-Meier survival curves and Cox regression model were used to determine the prognostic value of PDWLR.
Results
241 patients were analyzed eventually, and stratified into low and high PDWLR groups (≤ 9.66 vs. > 9.66). Results of comparing the baseline characteristics showed that high PDWLR was significantly associated with cirrhosis, and intraoperative blood loss (all P < 0.05). In multivariate COX regression analysis, PDWLR was demonstrated as an independent risk factor for OS (HR: 1.549, P = 0.041) and RFS (HR: 1.655, P = 0.005). Moreover, PDWLR demonstrated a superior capacity for predicting prognosis compared to other indicators.
Conclusion
Preoperative PDWLR has a potential value in predicting the prognosis of HCC patients following hepatectomy, which may help in clinical decision-making for individual treatment.
Similar content being viewed by others


Introduction
Hepatocellular carcinoma (HCC) is the sixth most common cancer in the world, with rising morbidity [1]. So far, hepatectomy is still one of the optimum curative treatments for resectable HCC. However, the long-term prognosis of patients is still far from satisfactory, because nearly 70% of patients have recurrence or metastasis within 5 years after surgery [2, 3]. Therefore, it is very important and urgent to find effective preoperative biomarkers to identify a high-risk patient with a poor prognosis and provide personalized treatment to improve survival.
Platelets play multiple roles in cancer progression and metastasis. Activated platelets play a mediating role in tumor growth, invasion, abnormal angiogenesis, and metastasis [4, 5]. It has been proved that platelet elevation is associated with adverse outcomes of many different cancers, including gastric cancer, pancreatic cancer, ovarian cancer, and endometrial cancer [6,7,8,9]. Meanwhile, lymphocytes are the key cell component of immune response and participate in the anti-tumor immune process. It has been studied that the increase of tumor lymphocyte infiltration on the surface is related to the improvement of patients’ prognosis [10]. Therefore, previous studies have used platelet-to-lymphocyte ratio (PLR) as an inflammatory indicator and proved that PLR is a potentially valuable indicator for predicting adverse outcomes of HCC patients [11,12,13].
However, platelet count per se does not indicate platelet activity, but rather platelet size reflects its activity. Platelet distribution width (PDW) was found to comprehensively reflect platelet activity, which is an indicator of changes in platelet size [14]. Compared with the rapidly changing platelet count, PDW has been revealed as a better indicator to reflect the characteristics of activated platelets [15]. Recently, PDW has also been proven to be a prognostic marker of HCC, which is significantly related to the survival of HCC patients after hepatectomy [16]. However, relying solely on a single indicator such as PDW may not accurately reflect the patient’s immune response. Therefore, the purpose of this study is to investigate the potential usefulness of a new index, PDW to lymphocyte ratio (PDWLR), in predicting the prognosis of patients with HCC, to provide a more comprehensive and realistic reflection of the patient’s immune response state.
Patients and methods
Study population and inclusion criteria
From October 2014 to October 2019, a retrospective analysis was conducted on 241 HCC patients who underwent curative hepatectomy (R0) at Zhejiang Provincial People’s Hospital. The institutional review board at Zhejiang Provincial People’s Hospital approved this study (No.QT2022430) and all patients’ informed consent was obtained before surgery. The study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline. The process of this study was guided by the Declaration of Helsinki. The inclusion criteria were as follows: (1) Patients with HCC were confirmed by pathology, (2) No history of other malignant tumors, (3) No extrahepatic metastasis, (4) Patients with complete medical records, (5) Age > 18 years. The exclusion criteria were as follows: (1) Recurrent HCC, (2) Patients died within 3 months after hepatectomy, (3) Patients with immune system diseases or blood system diseases, (4) Patients with acute or chronic infection within 2 weeks, (5) Patients received any anti-tumor therapy before the operation, (6) Patients with a history of splenectomy, (7) Patients receiving anticoagulation and/or antiplatelet therapy.
Data acquisition and followed-up
The following variables were analyzed: clinical characteristics of patients: age, sex, and cirrhosis; preoperative laboratory indexes: alpha-fetoprotein (AFP), platelet (PLT) count, total bilirubin (TBIL), alanine aminotransferase (ALT), aspartate aminotransferase (AST), PT, albumin (ALB), and PDWLR; pathological features: tumor size, number, degree of differentiation, and microvascular invasion (MVI); surgical variables: intraoperative blood loss, and resection margin (< 1 cm vs. ≥ 1 cm). The preoperative laboratory indexes were collected as the latest hematological parameters one week before surgery. The calculation formula of PDWLR was: PDWLR = platelet distribution width(fl.)/lymphocyte count (109/L). All patients were followed up after hospital discharge. Postoperative surveillance included physical examination, serum AFP level, ultrasonography or contrast-enhanced computed tomography (CT) or magnetic resonance imaging (MRI) of the chest and abdomen at least once every two months in the first 6 months after liver resection, and then every three months in the following 18 months, and at 6-monthly intervals thereafter. CT, MRI, angiography, bone scan, or positron emission tomography were performed earlier when recurrence or distant metastasis was suspected. Further treatment for the recurrent tumor was evaluated at each center by multidisciplinary discussion. Overall survival (OS) is calculated as the time frame from the date of operation to either the date of death or the last follow-up date. Recurrence-free survival (RFS) is calculated as the time interval between surgery and the date of disease recurrence.
Statistical analysis
The Chi-square (χ2) test or the Fisher exact test was used to compare the classified variables. The ROC curve was used to determine the optimal cut-off value of PDWLR. The Kaplan-Meier survival curve was used to show the survival difference between the two groups and compared by log-rank test. Univariate and multivariate Cox proportional hazard regression models were performed to determine the independent prognostic factors. Time-dependent ROC was used to compare the ability of each indicator to predict prognosis. Hazard ratio (HR) and 95% confidence interval (CI) were used to describe relative risk factors. P < 0.05 was set as statistically significant. All statistical analyses were performed using SPSS version 25.0 (IBM SPSS Statistics 25.0) and the software of R 4.2.3 (http://www.r-project.org/).
Results
Baseline characteristics
This study eventually included a total of 241 patients. The optimal cut-off value of PDWLR as determined by the ROC curve was 9.66. Subsequently, all 241 patients were stratified into low PDWLR (≤ 9.66, n = 119) and high PDWLR (> 9.66, n = 122) groups. While there were no statistical differences observed in most of the relevant variables amongst the baseline characteristics between the two groups (all P > 0.05), patients with high PDWLR exhibited poorer liver function and higher incidences of cirrhosis (84.4% vs. 62.2%, P < 0.001), as well as a greater likelihood of experiencing intraoperative bleeding (41.0% vs. 27.7%, P < 0.001) (Table 1).
Survival outcomes
After a median follow-up of 54.2 months, 140 (58%) patients experienced tumor recurrence and 101 (42%) patients died. For the entire cohort, the 1-, 3-, and 5-year OS were 87%, 67%, and 57%, while the 1-, 3-, and 5-year RFS were 67%, 46%, and 35%, respectively. The low PDWLR group showed a better 1-, 3-, and 5-year OS of 90%, 74%, and 66%, respectively, compared to the high PDWLR group which had an OS of 83%, 60%, and 48%, respectively (Fig. 1A). Similarly, the low PDWLR group had a better 1-, 3-, and 5-year RFS of 76%, 54%, and 41%, respectively, compared to the high PDWLR group which had an RFS of 58%, 39%, and 29%, respectively (Fig. 1B). The log-rank test using the Kaplan-Meier survival curve indicated that high PDWLR played a negative effect on both OS and RFS for patients with HCC after hepatectomy (P = 0.006 and P = 0.002, respectively).

Curves comparisons of overall survival (A) and recurrence-free survival (B) between the two groups (calculated by log-rank test). PDWLR, platelet distribution width to lymphocyte ratio
Independent-risk factors of overall survival and recurrence-free survival
Variables with a P-value < 0.1 in the univariate Cox regression analysis were entered into the forward stepwise multivariate Cox proportional hazard regression analysis, and the results are presented in Tables 2 and 3. The findings suggested that high PDWLR was an independent risk factor for both OS (HR:1.549, 95%CI 1.018–2.357, P = 0.041) and RFS (HR:1.655, 95%CI:1.160–2.360, P = 0.005). To avoid collinearity, PLR, PDW, and PLT were analyzed separately with other variables, and the results indicated that PLR was also an independent risk factor for both OS (HR: 1.144, 95%CI: 1.009–1.513, P = 0.042) and RFS (HR: 1.109, 95%CI: 1.025–1.458, P = 0.027). However, the PDW and PLT were not found to be significant independent risk factors for OS (HR: 1.005, 95%CI: 0.876–1.305, P = 0.125; HR: 1.309, 95%CI: 0.841–1.357, P = 0.307, respectively) or RFS (HR: 1.105, 95%CI: 0.894–1.346, P = 0.061; HR: 1.108, 95%CI: 0.611–1.284, P = 0.619, respectively).
Performance to predict the prognosis
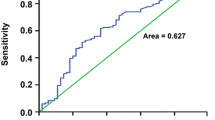
The area under the time-dependent ROC curve was calculated to determine which indicator was better at predicting survival. Initially, we evaluated the model’s ability to predict overall survival at five years, as shown in Fig. 2A. The AUC value for PDWLR was 0.651 (95% CI 0.592–0.704), indicating that it had a higher diagnostic capacity than PLR (AUC: 0.602, 95% CI 0.537–0.647), PDW (AUC: 0.557, 95% CI 0.529–0.611), and PLT (AUC: 0.536, 95% CI 0.514–0.576) (all P < 0.05). Therefore, PDWLR had the highest ability to predict overall survival compared to the other indicators at five years. Furthermore, we calculated the estimated AUC with a 95% confidence interval at different time points using time-dependent ROC curves (Fig. 2B). The results showed that the AUC of PDWLR was stable, with a median AUC of 0.648 (range 0.605–0.691).

A. Comparison of the predictive ability of postoperative overall survival at 5-year by time-dependent ROCs between the PDWLR and the other indicators. B. Median AUC of PDWLR at each time. ROCs, receiver operating characteristic curves; AUCs: areas under the curves; PDWLR, platelet distribution width to lymphocyte ratio; PLR, platelets-lymphocyte-ratio; PDW, platelet distribution width; PLT, platelet
Discussion
In this study, we discussed the correlation between PDWLR and the prognosis of HCC patients for the first time. Using ROC analysis, the best cut-off value of PDWLR for predicting the prognosis of HCC patients was determined at 9.66. Additionally, we found that PDWLR increased with poorer liver function and higher incidences of cirrhosis, as well as a greater likelihood of experiencing intraoperative bleeding. Moreover, PDWLR was identified as an independent risk factor for predicting the prognosis of HCC patients, and it has a better and more stable ability than other indicators to predict patients’ long-term survival after surgery.
Growing interest is recently being focused on the role played by the platelets in favoring HCC growth and metastasis. Platelets are disc-shaped cells that lack nuclei [16]. Since initially discovered in 1882, our knowledge regarding the critical function of platelets in hemostasis and thrombosis has grown tremendously [17]. However, beyond their role in regulating hemostasis and coagulation, multiple pieces of evidence now suggest that platelets serve much broader functions in various diseases. Recent discoveries have revealed that platelets actively participate in numerous physiological and pathological processes, including but not limited to innate and adaptive immune responses, and carcinogenesis. Thrombocytosis, considered a paraneoplastic syndrome, may occur during the natural course of neoplastic progression, frequently accompanying cancer growth and metastatic dissemination [18,19,20]. High platelet count has been correlated with poor prognosis in patients with various malignancies.
Platelets were not always considered to be a single prognostic determinant, and ratios of biochemical tests, as well as formulas including platelet count, were tested as potential predictors of prognosis in patients with HCC [21]. Lymphocytes have been shown to play an important role in cancer immune monitoring and the prevention of malignant tumor development [22]. A pro-inflammatory state can lead to impaired cell-mediated immunity and the impaired response of T lymphocytes induced by cytokines [23]. The reduction of CD4+ T helper lymphocytes may cause a poor lymphocyte-mediated immune response to tumor cells [24]. More specifically, the PLR has been investigated as a useful prognostic tool in several types of cancer, including HCC. The PLR was consistently associated with both overall and recurrence-free survivals after HCC resection, with high values being associated with poorer outcomes.
However, platelet count per se does not indicate platelet activity, but rather platelet size reflects its activity. The variability and heterogeneity of platelet volume can be reflected by PDW. When both mature and immature platelets are present in the circulation, the value of PDW increases. This indicates that an increase in PDW can lead to a higher possibility of abnormal thrombosis [25], and also indicates differentiation of megakaryocyte heterogeneity [26]. Therefore, as the tumor grows and various proinflammatory cytokines are up-regulated, these cytokines promote the maturation of heterogeneous megakaryocytes, which allows immature platelets to enter the circulation to meet the increasing demand. At the same time, the size and characteristics of these platelets are different, ultimately increasing PDW.
Thus, we propose a new indicator, PDWLR, which provides relatively accurate information about the prognosis of HCC patients, and is non-invasive and easy to obtain in clinical practice. PDW is a platelet-related marker, which reflects the activity of platelets. This is an interactive process. Tumors can secrete factors that promote the differentiation and proliferation of megakaryocytes, and increase the production and activation of platelets. Conversely, activated platelets can prevent tumor cells from being lysed, release growth factors, and promote tumor growth and metastasis [27]. Lymphocytes can affect the survival of patients through the mechanism of inhibiting tumor survival or proliferation [28]. Therefore, high PDWLR means high platelet activity and low lymphocyte count, which indicates that the prognosis of patients with HCC is poor. This is consistent with our research results.
The present study also demonstrated that PDWLR was associated with the recurrence of HCC. First, activated platelets are more likely to cover tumor cells, and tumor cells covered by platelets will escape the attack of the autoimmune system [29]. PDW is a good indicator of platelet activation. Secondly, when the immunity decreases, especially when the microenvironment where the tumor is located is immune abnormal, resulting in the corresponding lymphocytes being unable to successfully generate an immune response, the tumor will escape the surveillance from the immune system. When the tumor has immune tolerance or immune escape, it is more likely to have further progress. Therefore, patients with higher PDWLR values are more likely to relapse. This study also shows that patients with higher PDWLR are more likely to relapse. Therefore, for patients with high PDWLR, more frequent reexamination may be required after surgery to detect tumor progression and recurrence in time.
This study also has some limitations. First of all, the number of patients included is small, and this study is a single-center study. Secondly, retrospective studies inevitably lead to data collection bias. In addition, the changes in inflammatory indicators are affected by many factors, not only tumors but also different regions and races. Therefore, the reliability of our conclusion needs further research to prove.
Conclusions
The results of this study confirm that PDWLR is an independent predictor of RFS and OS in HCC patients. In addition, PDWLR is a potential prognostic indicator for HCC patients because of its simplicity and low cost in clinical practice.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- HCC:
-
hepatocellular carcinoma
- PDW:
-
platelet distribution width
- PLR:
-
platelets-lymphocyte-ratio
- ALT:
-
alanine aminotransferase
- AST:
-
aspartate transaminase
- AFP:
-
alpha-fetoprotein
- PLT:
-
platelet
- TBIL:
-
total bilirubin
- ALB:
-
albumin
- OS:
-
overall survival
- RFS:
-
recurrence-free survival
- HR:
-
hazard ratio
- CI:
-
confidence interval
References
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424.
Ng KK, Lo CM, Liu CL, Poon RT, Chan SC, Fan ST. Survival analysis of patients with transplantable recurrent hepatocellular carcinoma: implications for salvage liver transplant. Arch Surg. 2008;143(1):68–74. discussion 74.
Tabrizian P, Jibara G, Shrager B, Schwartz M, Roayaie S. Recurrence of hepatocellular cancer after resection: patterns, treatments, and prognosis. Ann Surg. 2015;261(5):947–55.
Pan Y, Wang Y, Wang Y, Xu S, Jiang F, Han Y, Hu M, Liu Z. Platelet-derived microvesicles (PMVs) in cancer progression and clinical applications. Clin Transl Oncol. 2023;25(4):873–81.
Xu H, Zheng X, Ai J, Yang L. Hemoglobin, albumin, lymphocyte, and platelet (HALP) score and cancer prognosis: a systematic review and meta-analysis of 13,110 patients. Int Immunopharmacol. 2023;114:109496.
Zhang J, Zhang L, Duan S, Li Z, Li G, Yu H. Single and combined use of the platelet-lymphocyte ratio, neutrophil-lymphocyte ratio, and systemic immune-inflammation index in gastric cancer diagnosis. Front Oncol. 2023;13:1143154.
Maloney S, Pavlakis N, Itchins M, Arena J, Mittal A, Hudson A, Colvin E, Sahni S, Diakos C, Chan D et al. The prognostic and predictive role of the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and Lymphocyte-to-Monocyte Ratio (LMR) as biomarkers in Resected Pancreatic Cancer. J Clin Med 2023, 12(5).
Patel D, Thankachan S, Sreeram S, Kavitha KP, Suresh PS. The role of Tumor-educated platelets in Ovarian cancer: a comprehensive review and update. Pathol Res Pract. 2023;241:154267.
Detopoulou P, Panoutsopoulos GI, Mantoglou M, Michailidis P, Pantazi I, Papadopoulos S, Rojas Gil AP. Relation of Mean platelet volume (MPV) with Cancer: a systematic review with a focus on Disease Outcome on twelve types of Cancer. Curr Oncol. 2023;30(3):3391–420.
Fu J, Zhang Z, Zhou L, Qi Z, Xing S, Lv J, Shi J, Fu B, Liu Z, Zhang JY, et al. Impairment of CD4 + cytotoxic T cells predict poor survival and high recurrence rates in patients with hepatocellular carcinoma. Hepatology (Baltimore MD). 2013;58(1):139–49.
Wang D, Bai N, Hu X, OuYang XW, Yao L, Tao Y, Wang Z. Preoperative inflammatory markers of NLR and PLR as indicators of poor prognosis in resectable HCC. PeerJ. 2019;7:e7132.
Chen Y, Zeng J, Guo P, Zeng J, Liu J. Prognostic significance of platelet-to-lymphocyte ratio (PLR) in Extrahepatic Metastasis of Hepatocellular Carcinoma after curative resection. Cancer Manage Res. 2021;13:1395–405.
Wu W, Wang Q, Han D, Li J, Nie Y, Guo D, Yang L, Tao K, Zhang X, Dou K. Prognostic value of preoperative inflammatory markers in patients with hepatocellular carcinoma who underwent curative resection. Cancer Cell Int. 2021;21(1):500.
Xia W, Chen W, Tu J, Ni C, Meng K. Prognostic value and clinicopathologic features of platelet distribution Width in Cancer: a Meta-analysis. Med Sci Monit. 2018;24:7130–6.
Zheng YY, Wang L, Shi Q. Mean platelet volume (MPV) and platelet distribution width (PDW) predict clinical outcome of acute ischemic Stroke: a systematic review and meta-analysis. J Clin Neurosci. 2022;101:221–7.
Guo F, Zhu X, Qin X. Platelet distribution width in Hepatocellular Carcinoma. Med Sci Monit. 2018;24:2518–23.
Koupenova M, Kehrel BE, Corkrey HA, Freedman JE. Thrombosis and platelets: an update. Eur Heart J. 2017;38(11):785–91.
Haemmerle M, Stone RL, Menter DG, Afshar-Kharghan V, Sood AK. The platelet lifeline to Cancer: challenges and opportunities. Cancer Cell. 2018;33(6):965–83.
Ashorobi D, Gohari P. Essential thrombocytosis. StatPearls. edn. Treasure Island (FL); 2023.
Lin RJ, Afshar-Kharghan V, Schafer AI. Paraneoplastic thrombocytosis: the secrets of Tumor self-promotion. Blood. 2014;124(2):184–7.
Carr BI, Guerra V, Giannini EG, Farinati F, Ciccarese F, Rapaccini GL, Di Marco M, Benvegnu L, Zoli M, Borzio F, et al. Significance of platelet and AFP levels and liver function parameters for HCC size and survival. Int J Biol Markers. 2014;29(3):e215–223.
Wang B, Hu S, Fu X, Li L. CD4(+) cytotoxic T lymphocytes in Cancer Immunity and Immunotherapy. Adv Biol (Weinh). 2023;7(4):e2200169.
Shevde LA, Joshi NN, Advani SH, Nadkarni JJ. Impaired T lymphocyte function and differential cytokine response pattern in members from cancer families. Nat Immun. 1998;16(4):146–56.
Miggelbrink AM, Jackson JD, Lorrey SJ, Srinivasan ES, Waibl-Polania J, Wilkinson DS, Fecci PE. CD4 T-Cell exhaustion: does it exist and what are its roles in Cancer? Clin Cancer Res. 2021;27(21):5742–52.
Zuo X, Kong W, Feng L, Zhang H, Meng X, Chen W. Elevated platelet distribution width predicts poor prognosis in hepatocellular carcinoma. Cancer Biomark. 2019;24(3):307–13.
Yan K, Ding B, Huang J, Dai Y, Xiong S, Zhai Z. Normal platelet counts mask abnormal thrombopoiesis in patients with chronic Myeloid Leukemia. Oncol Lett. 2015;10(4):2390–4.
Buergy D, Wenz F, Groden C, Brockmann MA. Tumor-platelet interaction in solid tumors. Int J Cancer. 2012;130(12):2747–60.
Chen Y, Tian Z. Innate lymphocytes: pathogenesis and therapeutic targets of Liver Diseases and cancer. Cell Mol Immunol. 2021;18(1):57–72.
Franco AT, Corken A, Ware J. Platelets at the interface of Thrombosis, inflammation, and cancer. Blood. 2015;126(5):582–8.
Funding
Funding for the study was provided by the Natural Science Foundation of China (No. 82302915), Zhejiang Provincial Natural Science Foundation of China under Grant (No. LQ23H160049), Health Commission of Zhejiang Province (No.2022KY532), and Zhejiang Provincial People’s Hospital (No. ZRY2020A004).
Author information
Authors and Affiliations
Contributions
Authors’ Contributions: Zhi-Han Zhong, Lei Liang, Tian-Wei Fu and Mu-Gen Dai contributed equally to this work. Dr Lei Liang and Jun-Wei Liu had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: Zhi-Han Zhong, Lei Liang, Tian-Wei Fu, and Jun-Wei Liu. Acquisition, analysis, or interpretation of data: Mu-Gen Dai, Jian Cheng, Si-Yu Liu, Tai-Wei Ye, Guo-Liang Shen. Drafting of the manuscript: Zhi-Han Zhong, and Lei Liang. Critical revision of the manuscript for important intellectual content: Cheng-Wu Zhang, and Dong-Sheng Huang. Obtained funding: Lei Liang. Administrative, technical, or material support: Si-Yu Liu, Tai-Wei Ye. Study supervision: Lei Liang, Cheng-Wu Zhang, and Dong-Sheng Huang.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the ethics committee of Zhejiang Provincial Peoples Hospital, and all participants provided informed consent for study inclusion.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhong, ZH., Liang, L., Fu, TW. et al. Prognostic value of platelet distribution width to lymphocyte ratio in patients with hepatocellular carcinoma following hepatectomy. BMC Cancer 23, 1116 (2023). https://doi.org/10.1186/s12885-023-11621-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-023-11621-8