
Abstract
Background
18F-FDG PET/CT provides precise information about dissemination of lymphoma lesions. Dmax, defined as distance between the two lesions that were farthest apart by PET/CT, was found to be a promising predictor of Diffuse large B-cell lymphoma (DLBCL) outcome in a small size of clinical trial data. We analyzed the impact of Dmax on the outcome of a large real-world DLBCL cohort.
Methods
Data of newly diagnosed DLBCL at the Third Affiliated Hospital of Soochow University were retrospectively collected. Baseline Dmax, clinical data and survival information were recorded. A metabolic parameter, metabolic bulk volume (MBV), was also measured to verify the independent impact of Dmax.
Results
Optimal cut-off values for Dmax and MBV were 45.34 cm and 21.65 cm3. With a median follow-up of 32 months, Dmax significantly impacted progression-free survival (PFS) and overall survival (OS) in 253 DLBCL patients. For Dmaxlow and Dmaxhigh groups, estimated 3-year OS were 87.0% and 53.8% (p < 0.001), while 3-year PFS were 77.3% and 37.3% (p < 0.001). And for MBVlow and MBVhighgroups, 3-year OS were 84.5% and 58.8% (p < 0.001), and 3-year PFS were 68.7% and 50.4% (p = 0.003). Multivariate analysis identified Dmax and Eastern Cooperative Oncology Group performance status (ECOG PS) independently associated with PFS and OS, while MBV only independently associated with OS. A Dmax revised prognostic index (DRPI) combining Dmax and ECOG PS identified an ultra-risk DLBCL population with 3-year PFS of 31.7% and 3-year OS of 38.5%. The area under the curve (AUC) showed that this model performed better than International prognostic Index (IPI).
Conclusion
Dmax is a new and promising indicator to investigate dissemination of lymphoma lesions associated with the outcome of DLBCL. It significantly contributes to stratification of patients with disparate outcomes.
Trial registration
This research has been retrospectively registered in the Ethics Committee institutional of the Third Affiliated Hospital of Soochow University, and the registration number was approval No. 155 (approved date: 31 May 2022).
Similar content being viewed by others


Background
Diffuse large B cell lymphoma (DLBCL) represents almost 30% of non-Hodgkin lymphoma (NHL) [1], which is responsible for 544,000 new cases and 260,000 deaths in 2020 [2]. Despite the remarkable success of immune-chemotherapy of RCHOP (Rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone), outcomes remain variable among patients. Long time survival has been achieved in approximately two-thirds of the patients [3], but prognosis is dismal for patients failed the first-line treatment, with 7% complete response and 6 months overall survival (OS) [4].The International prognostic Index (IPI), consisting of age, Eastern Cooperative Oncology Group performance status (ECOG PS), Ann Arbor stage, serum lactate dehydrogenase (LDH), and extranodal involvement, was induced in 1993 [5]. Since then, massive attempts have been made to adjust the scoring system to better delineate patients with inferior outcome [6,7,8]. Ultimately, National Comprehensive Cancer Network -IPI (NCCN-IPI), with the same clinical parameters but detailed grading of each risk factor, demonstrated the best performance to estimate the highest and lowest risk groups. Nevertheless, none of these scoring systems can identify a subgroup with less than 50% of long-term survival [9].
18F-labeled fluorodeoxyglucose positron emission tomography with computed tomography (18F-FDG PET/CT) is highly sensitive for detecting DLBCL lesions. By PET/CT, more accurate methods to identify patients with early treatment failure have been recognized. Mounting evidence ensured the irreplaceable role of PET/CT for staging in a variety of NHLs, including DLBCL, making it an essential part in DLBCL patients management [10]. PET/CT provided accurate disease mapping with distinct lesions across the whole body, which of the most concern are the metabolic features of lymphoma. The most commonly used parameter is the standardized uptake value (SUV) at sites of disease [11]. Other metabolic parameters, including metabolic tumor volume (MTV) and metabolic bulk volume (MBV), were also recognized as independent predictors for DLBCL prognosis [12,13,14]. MBV was proved to be significantly associated with MTV [14], and different studies demonstrated its satisfactory performance in predicting survival not inferior sometimes even superior than MTV [13,14,15]. Considering diffusion of disease lesions a challenge for radiomic analysis of lymphoma, the accurate prediction of outcome and relatively easy access made MBV a potentially more valuable marker to assess metabolic feature of lymphoma. Besides the metabolic uptake of the disease, the dissemination of the disease lesions presented in PET/CT was also an ignorable information. Recently, a new PET/CT metric describing tumor dissemination defined as the distance between the 2 farthest lesions, named Dmax [16], was proved to be a promising predictor associated with inferior outcome of DLBCL [11, 16]. As a semi-quantitative dissemination indicator, Dmax presented strong prognostic value independent of IPI and MTV in elderly patients ranging from 60 to 80 [11]. And to date, the clinical value of Dmax and the correlation with the clinical characteristics in a large number of DLBCL cohort across whole age spectrum has not been fully explored.
Here, we develop a new approach based on 3-dimensional imaging to detect Dmax, and sought to investigate the dissemination presented by Dmax in a real-world data to evaluate whether baseline Dmax demonstrated prognostic value in a large retrospective cohort of DLBCL, and whether it may improve the prediction of prognosis in DLBCL patients, especially for identification of those high-risk patients. And meanwhile, we measured the metabolic volume of the largest lesion, MBV, to evaluate its impact on the outcome of DLBCL patients as a potentially surrogate indicator determining the metabolic feature. Thereby we try a new model combining PET/CT indicators and clinical predictors to better stratify DLBCL patients, especially for the ultra-risk population.
Methods
Study population and clinical data
Data of newly diagnosed DLBCL patients at the Third Affiliated Hospital of Soochow University’s institutional DLBCL cases between May 2012 and November 2021 were retrospectively collected. PET/CT was not practiced as routine examination before 2015 in our institution, thus there were only 11 patients included between 2012 and 2015, who were excluded from the analysis. Meanwhile, more patients underwent PET/CT baseline assessment over time. Pathological diagnosis was strictly based on the morphological and immunohistological criteria of the World Health Organization classification, and all special DLBCL subtypes, including primary cutaneous B-cell lymphoma, primary mediastinal large B-cell lymphoma, primary DLBCL of the central nervous system and transformed DLBCL, were excluded.
This study was performed in accordance with the Declaration of Helsinki and approved by the Ethics Committee institutional of the Third Affiliated Hospital of Soochow University. The requirement for written patient consent was waived as a retrospective study. All identifiers were removed after the completion of our analyses to protect patient privacy. Baseline clinical characteristics including age, gender, LDH, B symptoms, ECOG PS and Ann Arbor stage, Hans classification, Bulky disease (≥ 7.5 cm), were recorded during admission. To allow for the measurement of baseline Dmax, only patients with a baseline PET/CT and more than one suspicious lymphoma lesion were included.
Baseline Dmax and MBV and Quality control of 18F-FDG PET/CT scans
Imaging was performed with a 64-MDCT PET/CT scanner (Biograph mCT, Siemens Healthcare). The imaging agent was FDG (radiochemical purity, > 95%). All patients fasted for at least 8 h before the PET/CT examination, and their serum glucose level was less than 11 mmol/L. After intravenous injection of FDG at 4.44 MBq/kg, the patients rested in a quiet, warm, sheltered environment for 45–60 min. After urinating, the patients underwent PET/CT. Automatic exposure control (CARE Dose 4D, Siemens Healthcare) was used for CT. Tube current was automatically adjusted according to the body’s shape, anatomic structure and tissue density. Tube voltage was 100 kV; pitch, 0.8; single layer rotation time, 0.5 s; slice thickness, 3 mm. The PET mode was 3D. The scan range was skull base to upper femur, and the acquisition time was 2 min per bed. Images were reconstructed (SyngoTrueD system, Siemens Healthcare) to produce cross-sectional, coronal, and sagittal tomographic images and 3D projection images.
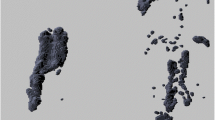
PET/CT images were viewed on a post-processing video display provided by the equipment manufacturer. All measurement was independetly carried out by two nuclear medicine physicians by images 3D reconstructed. Regional volumes were identified automatically by the software, and then checked visually to confirm pathological lesions. For the lesions with controversial values, it is determined through discussion in combination with the medical history. Neither nuclear medicine physician had any information about the patient’s clinical prognosis. The dissemination feature, Dmax, was extracted as suggested by Cottereau et al. [16], defined as the distance between the two lesions that were farthest apart. The nuclear medicine physician selected each hypermetabolic lesion by clicking on its projection using a graphical user interface. Through three-dimensional reconstruction, the center of the lesion was automatically determined, and the distances between all paired lesions were directly obtained by the system, of which the largest distance was recorded as Dmax (Fig. 1a).

Measurement of Dmax and differences of Dmax and MBV.
(a) Using the 3-dimensional imaging reconstructed, Dmax is defined as the spatial distance between the two lesions that are farthest apart. (b) Example patient with high Dmax and low MBV, experienced early relapsed and death. (c) Example patient with low Dmax and high MBV, remained remission at follow-up time
In addition, MBV was measured semi-automatically with an SUV based automatic contour program using reconstructed images (Syngo TrueD System Siemens Healthcare) and defined as the metabolic volume of the largest lesion as previously reported [13, 14]. Nuclear medicine physicians clicked on the projection of each hypermetabolic lesion in the graphical user interface, and the system automatically generated the contour around the target lesion within the boundary and defined metabolic volume with voxel within the contour boundary presenting a 41% SUVmax threshold. The maximum value was recorded as MBV (Supporting information Fig. S1). Examples of PET images (maximum-intensity projections) of patients with differences Dmax and MBV were shown in Fig. 1, illustrating the different feature with high Dmax but low MBV (Fig. 1b) and low Dmax but high MBV (Fig. 1c).
Data from the two nuclear medicine physicians were tested by intraclass correlation efficient (ICC), showing fairly high concordance between their measurements for both MBV (0.992, p < 0.001) and Dmax (0.989, p < 0.001) respectively.
Follow-up and endpoints
All patients were followed up until March 31, 2022 or the death of patients through making telephone calls and rechecking medical records. OS was defined as the interval of time between pathological diagnosis and death from any cause or the last follow-up, and PFS as the interval of time between pathological diagnosis and progression of the tumor for any aspect,death from any reason, or the last follow-up. The survival status of all patients was confirmed through death records or telephone call to immediate family (in the case of patients death during the follow-up) or to the patients themselves.
Statistical analysis
Categorical variables were recorded as numbers (percentages) and continuous variables as and median (interquartile range, IQR). All the individual factors of IPI were categorized by conventional criteria. χ2 test were used to analyze the differences for clinical factors. Dmax and MBV were transformed into a categorical variable by MaxStat analysis (titled as Maximally Selected Rank Statistics). The univariate association between PFS and OS were analyzed by Cox proportional hazard model. The Kaplan–Meier method was used to calculate survival curves. The variables with significance in univariable analysis were kept in the multivariate analysis. All the statistical tests were two-sided, with the statistical significance set at p < 0 0.05.
All data were calculated by IBM SPSS 21.0 (IBM Inc., Armonk, USA), R software (version 4.0.3; http://www.Rproject.org) and Stata version 15.0.
Results
A total of 284 patients were retrospectively collected with baseline PET/CT scan before treatment engagement. Of them, 253 patients have more than one lesion to determine Dmax (Fig. 2). The mean baseline Dmax was 37.37 cm across the whole cohort (median 30.83 cm, range 2.47–93.13), while the mean MBV was 106.71 cm3 (median 18.25 cm3, range 0.50-597.91).

Flowchart of patients by Dmax analysis
PET/CT, positron emission tomography/computed tomography; DLBCL, Diffuse large B cell lymphoma
Dmax was significantly associated with PFS (HR 1.019, 95% CI: 1.012–1.027, p < 0.001) and OS (HR 1.023, 95 CI: 1.013–1.033, p < 0.001) of DLBCL patients as a continuous value. Similar results of PFS (HR 1.002, 95% CI 1.001–1.004, p = 0.005) and OS (HR 1.003, 95% CI 1.001–1.005, p < 0.001) were also reported for MBV as a continuous value. Multivariable analysis further identified Dmax as an independent factor for both PFS (HR 1.011, 95% CI 1.001–1.022, p = 0.026) and OS (HR 1.016, 95% CI 1.003–1.029, p = 0.017) when all the clinical indicators and MBV were included in the model. Meanwhile, MBV presented as an independent predictor for OS (HR 1.002, 95% CI 1.000-1.005, p = 0.029) but not PFS (HR 1.001, 95% CI 0.999–1.003, p = 0.160) (Table S1).
According to the maximal chi-square method, 45.34 cm and 21.65 cm3 were the optimal cut-off values respectively for the Dmax and MBV that distinguished between different prognostic groups for OS most effectively (Table 1; Fig. 3). Applying these results, patients were respectively divided into two groups of Dmax and MBV as for those greater than the cut-off values refined as Dmaxhigh or MBVhigh group. The analysis besides were all based on the new definition.

Cut-off points of Dmax and MBV defined by using maximally selected log-rank statistics
The estimated optimal cut-off point of Dmax was 45.34 cm (A), and optimal cut-off point of MBV was 21.65cm3 (B) MBV, metabolic bulk volume
Clinical characteristics and Dmax of DLBCL patients
Baseline demographic and clinical characteristics are shown in Table 2. During a median follow-up of 32 months, 94 (37.2%) patients experienced overt disease progression, and 64 (25.3%) of them ultimately succumbed to the disease. Median PFS and OS was 88 months and not reached respectively. Estimated 3-year OS and 3-year PFS was 72.8% and 60.4% for the whole population. Of the entire cohort, 106 (41.9%) patients were clarified as Dmaxhigh group, and 115 (45.5%) as MBVhigh group. Meanwhile, distinguished Dmax and MBV have poor correlation considering the fairly low correlation coefficient (Supporting information Table S2). Median age was 65 years (range13-91), and no significant difference of Dmax was claimed between with the elder (> 60) and younger (≤ 60) patients. Staging were analyzed based on two different methods, verifying 158 (62.5%) advanced stage (stage III/IV) based on Ann Arbor stage, 166 (65.6%) advanced stage (stage III/IV) based on Lugano stage. Both were shown associated with higher Dmax. The other two individual IPI factors including elevated LDH (> 250 U/L), extranodal involvement (> 1) were also significantly associated with Dmax, subsequently yielded the association of higher IPI score with high Dmax.
Univariable analysis
Univariable analysis for prognosis of all the clinical factors in the entire cohort was shown in Table 3. The five individual IPI indexes were identified as being prognostic for inferior PFS and OS: elderly age, elevated LDH level, advanced stage, etxtranodal lesions > 1 and ECOG PS ≥ 2. Patients with high Dmax or MBV also experienced high risk of progression and death. PFS and OS did not differ differently by Cell-of-origin (COO) determined by immunohistochemistry.
For the 106 patients with high Dmax, median PFS was 22 months (95% CI 8.137–35.863), and median OS was 58 months (95% CI 31.116–84.884), and were significantly worse than the patients presented with low Dmax, whose median PFS and OS were 88 months and not reached during the follow-up time. For Dmaxlow and Dmaxhigh group, estimated 3-year OS were 87.0% and 53.8%, while 3-year PFS were 77.3% and 37.3%, respectively (Fig. 4a, b). Meanwhile, 3y-OS was 84.5% and 58.8%, 3y-PFS was 68.7% and 50.4% for MBVlow and MBVhigh patients, respectively.

Kaplan–Meier estimates of PFS and OS according to baseline Dmax and risk stratification
(A) PFS for all DLBCL patients, (B) OS for all DLBCL patients, (C) PFS in patients with advanced stage based on Ann Arbor system, (D) OS in patients with advanced stage based on Ann Arbor system, (E) PFS for patients according to DRPI, (F) OS for patients according to DRPI.
DLCBL, Diffuse large B cell lymphoma; DRPI, Dmax revised prognostic index; OS, overall survival; PFS, progression-free survival
Based on Ann Arbor system, 95 patients were staged as stage II, and only 1 case was defined as Dmaxhigh. This patient did not experience any disease events during the following-up time. For the 158 patients of advanced stage, 104 of them are grouped as Dmaxhigh, whose outcome was significantly worse than the other 54 Dmaxlow patients. Median PFS was 20 months (95% CI 8.005–31.995) and not reached, and median OS was 45 months (95% CI 17.973–72.027) and not reached, and estimated 3-year PFS was 63.8% and 35.4%, 3-year OS was 81.9% and 52.6% for Dmaxhigh and Dmaxlow group patients of advanced stage, respectively (Fig. 4c, d).
Multivariable analysis
Combining all the factors potentially associated with PFS or OS, the multivariable analysis ensured the independent significance of Dmax, as well as ECOG PS on both PFS and OS (Table 3). Age and high MBV was an independent risk factor for OS but not for PFS, and advanced Ann Arbor stage was an independent inferior factor only for PFS. Besides, when included Lugano stage instead of Ann Arbor stage, Dmax remained its independent impact on PFS and OS, but Lugano stage seemed did not have independent significance on both PFS and OS (Supporting information Table S3). For the 158 patients presented as advanced stage of Ann Arbor, Dmax and ECOG PS were the remaining two independent risk factors for PFS and OS, while MBV only impacted significantly on OS (Table 4).
IPI and Dmax were all independently significant risk factors for PFS and OS, and Dmax was shown to be a strong independent risk factor independent of IPI score (Supporting information Table S4).
Combination of baseline Dmax optimizes prediction of patient outcomes
Considering the independent significant impact of ECOG PS and Dmax for PFS and OS, a new prediction model defined as Dmax revised prognostic index (DRPI) was established based on these two factors. One point was recorded for each factor of ECOG PS ≥ 2 and high Dmax. Patients were divided into three groups: low-risk group with 0 point, intermediate-risk groupwith 1 point and high-risk group with 2 points. Significant differences was observed between the different groups, which showed estimated 3-year PFS was 82.0%, 47.2% and 31.7%, and 3-year OS was 91.9%, 65.8% and 38.5%, respectively (Fig. 4e, f). The DRPI was significantly associated with outcome, yielding an area under the curve (AUC) of 76.6%, which indicated a better performance than both IPI and NCCN-IPI in this group of DLBCL patients (Fig. 5).

Receiver operating characteristic curves for OS for DRPI, IPI and NCCN-IPI prediction models
AUC, area under the curve; DRPI, Dmax revised prognostic index; IPI, International prognostic Index; NCCN, National Comprehensive Cancer Network, OS, overall survival
Discussion
The current research revealed the strong and significant prognostic value for DLBCL patients of baseline Dmax, a semi-quantitative dissemination parameter calculated by PET/CT. Prognosis of patients with high baseline Dmax was very frustrating, whose 3y-PFS and 3y-OS were only 37.3% and 53.8%, respectively. Accounting for more than one-third of all DLBCL patients, Dmaxhigh patients presented with a more than 30-point reduction of both 3-year PFS and OS compared with the Dmaxlow patients. The impact maintained irrespective of the Stage based on both Ann Arbor and Lugano system. Multivariable analysis confirmed the independent prognostic value of Dmax, as well as ECOG PS. A new clinical model based on these two factors also presented better performance than IPI and NCCN-IPI in predicting OS of DLBCL patients.
The heterogeneity of DLBCL still posed a great threat for the treatment and outcome of the patients. DLBCL typically had no primary sites and could affect any part of the whole body. Until now, there were no practical clinical indicators that could precisely describe the diffusion degree of the disease. The only clinical indicator implicating the dissemination to certain extent was stage of the disease, which was generally carried out based on Ann Arbor system. This modality of anatomic stage has been adopted for over half a century, presuming the equivalent prognosis for patients with simultaneous involvement of upper and (or) lower diaphragm [17]. In 2014, the system was revised with more attention to extranodal lesions [18]. Whether as a continuous or categorical variable, Dmax presented as an independent prognostic factor for both PFS and OS of DLBCL patients, while Ann Arbor stage only independently impact PFS not OS. Meanwhile, Dmax was still an independent predictor for PFS and OS even for patients of advanced stage of both systems. For the 258 patients presenting more than one lesions in our study, only eight patients altered from early stage based on Ann Arbor system to advanced stage identified by Lugano stratification. Lugano system was not independently associated with neither PFS nor OS. This also implicated that the extent of disease dissemination has a greater impact on the disease prognosis than the extranodal involvements considering DLBCL as a systemic disease.
PET/CT is a routine and currently state-of-the-art modality for detecting lesions of DLCBL without omission owing to its high sensitivity, making it possible to develop a more accurate parameter to describe disease dissemination. The application of PET/CT led to changes in stage for 10-30% patients of lymphoma, usually upstaging, [19] resulting in alterations in clinical management of 3-25% patients [20]. Improved delineation of disease involvement provided by PET/CT, even for early stage patients, suggested the magnitude of change exceeds stage migration. The tumor burden and metabolic characteristics of lymphoma measured by PET/CT have long been realized as prognostic factors for DLBCL. MTV was independent prognostic value for the disease despite variations in measurement methods and cut-off values in massive reports, [21,22,23,24] and was proved to have linear spline relationship with survival of DLBCL patients [12]. MBV was also pronounced as independent predictor for PFS and OS, and can serve as a good substitute for MTV [13, 14]. MBV was firstly reported as MTV of the largest tumor lesion, and was proved to be associated with both PFS and OS of DLBCL. When combined with MTV, ECOG PS and bulky disease, MBV was proved to be independently associated with OS, while MTV only with PFS [13]. MBV was significantly correlated with MTV, and for patients discordance between the MBV and MTV, MBV seemed to be more predictable for PFS. Another study declared the independent impact of MBV on both PFS and OS of stage II/III DLBCL patients [15].
In our research, patients with low MBV presented significant superior PFS and OS. Although subsequent evidence did not identify MBV as an independent prognostic factor for PFS, it still revealed MBV as an independent predictor of OS in DLBCL patients. Given the difficulty of MTV measurements in clinical practice, MBV remained valuable in lymphoma as a conventionally obtainable volumetric FDG parameter. Further researches would be needed for the exploration of MBV and MTV, as well as other metabolic parameters provided by PET/CT. Meanwhile, the bulky disease did not show independent impact on both PFS and OS, further clarified the metabolic feature provided by PET/CT more valuable for clinical outcome.
Dmax was firstly identified by Cottereau et al. in a small size of 95 DLBCL patients from LNH073B study. Compared with other three different dissemination parameters, including Dmaxbulk (defined as the maximal distance between the largest lesion and any other lesion), SPREADbulk (the sum of the distances of the bulky lesion from all other lesions) and SPREADpatient (the largest value, over all lesions, of the sum of the distances from a lesion to all the others), Dmax was the only independent predictor for both PFS and OS [16]. The author further investigated Dmax in REMARC clinical trial cohort containing 301 DLBCL patients aged 60–80 years and verified its independent predictive value in elderly patients. In our research, Dmax was a strong predictor for the outcome of DLBCL, consistent with their results. Further indicating Dmax as a promising parameter to assess the dissemination of lymphoma lesions. Impressively, high standardized Dmax combined with high MTV and ECOG PS revealed to be associated with high risk of CNS relapse for the elderly [11]. Since then, different retrospective researches have demonstrated the promising value of Dmax for lymphoma. A systematic review claimed the dissemination of disease assessed by Dmax significantly associated with the outcome of many different types of lymphoma, including HL, DLBCL, Peripheral T-cell Lymphomas (PTCL) and Angioimmunoblastic T-cell lymphoma (AITL) [25]. As a simple and intuitive indicator, Dmax is a very easilly assessed dimensional feature, and is less influenced by “technical” features. Combination of Dmax and different radiomics and clinical makers released significant improvement of patients risk-stratification of lymphoma [25]. Combination of MTV and Dmax could recognize the high-risk patients presenting 4y-PFS and 4y-OS of 41% and 66% respectively in previous report [11], while in our research, combination of the two independent predictors of Dmax and ECOG PS, could help us identify ultra-risk patients with 3y-PFS and 3y-OS of only 31.7% and 38.5%. Nevertheless, the predictive value and the association of Dmax with other clinical predictors has not been explored in a large DLBCL cohort of all ages. Another model consisted of Dmaxbulk and the natural logarithms of MTV and of SUVpeak presented better performance than IPI to predict 2-year time to progression (TTP) [26]. The metabolic feature of DLBCL defined by MTV has poor correlation with Dmax [16], consistent with our results of MBV and Dmax, indicating Dmax as a unique and predictive characteristic of DLBCL.
This is the first large-scale study to investigate the predictive value of dissemination feature in DLBCL at all ages, which also combined it with currently used clinical predictors, making it the most comprehensive study so far. Meanwhile, the two staging systems were all included in our research to further confirm the prognostic value of Dmax as an indicator of disease dissemination characteristics. Moreover, to determine the exact distance of Dmax, new approach based on 3D reconstructed was applied here, providing more direct and precise method to evaluate the parameter.
The international index has been practiced for nearly thirty years, and emergence of new technologies have notably improved the understanding of the disease. As PET/CT has already been widely used as a routine examination during clinical management of DLBCL, combination of the extensive and new disease information provided by PET/CT with the clinical data brought dramatic improvement to the risk stratification and treatment management. A new model established here on two independent predictors, including Dmax and ECOG PS, performed better prediction for OS than IPI and NCCN-IPI, paving the way for future exploration of new stratification. This new model divided patients into three distinct risk groups with 3-year OS gapping more than 25%. For the patients in the ultra-risk group, manifesting high Dmax more than 45.34 cm, ECOG PS ≥ 2, nearly two thirds of them ultimately died within 3 years, corresponding with 5-year OS for high-risk group in IPI of 43% and NCCN-IPI of 38% [7].
As for the biomarker, chemokine CXCR4 plays an essential role in tumor dissemination and progression [27], and is associated with inferior outcome [28, 29]. In vivo models, decreased lymphoma dissemination was pronounced associated with prolonged animal survival via diverse mechanisms mainly through inhibition of Human germinal center-associated lymphoma (HGAL) [30]. Wide application of PET/CT makes it feasible to evaluate Dmax in clinical practice, and it is rather desirable for further investigation for the dissemination characteristics of the disease of both clinical manifestations and biological markers, which might help us to further comprehend the essentials of the disease.
Our research had some inevitable limitations as a single-center retrospective study. As PET/CT was not mandatory at baseline evaluation, some biases of the patients are not inevitable in patients’ economic status and physician preference, resulting in some selection bias of the patients. The follow-up time was relatively short considering the long survival of the disease, and the relatively small number of patients diagnosed before 2015 may further impact the results of survival analysis. The results lack external validation to confirm its value, and also need to be validated in a larger population from prospective multi-center studies.
Conclusion
In conclusion, the semi-quantitative factor of disease dissemination Dmax, is a robust and independent predictor of survival outcomes for DLBCL. High Dmax at baseline was significantly associated with inferior PFS and OS in patients. Baseline Dmax combined with ECOG PS could improve risk stratification for DLBCL patients, especially for identification of ultra-risk DLBCL patients. Dmax can be a promising indicator to evaluate the dissemination feature of lymphoma and incorporating dissemination feature can significantly improve the clinical management.
Data availability
The datasets generated and/or analysed during the current study are not publicly available due being generated based on information collected during clinical care but are available from the corresponding author on reasonable request.
Abbreviations
- DLBCL:
-
Diffuse large B cell lymphoma
- NHL:
-
Non-Hodgkin lymphoma
- RCHOP:
-
Rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone
- OS:
-
Overall survival
- IPI:
-
International prognostic Index
- ECOG PS:
-
Eastern Cooperative Oncology Group performance status
- LDH:
-
Lactate dehydrogenase
- PFS:
-
Progression-free survival
- 18F-FDG PET/CT:
-
18F-labeled fluorodeoxyglucose positron emission tomography with computed tomography
- MTV:
-
Metabolic tumor volume
- HL:
-
Hodgkin lymphoma
- TTP:
-
Time to progression
- MBV:
-
Metabolic bulk volume
- IQR:
-
Interquartile range
- COO:
-
Cell-of-origin
- DRPI:
-
Dmax revised prognostic index
- HGAL:
-
Human germinal center-associated lymphoma
- AUC:
-
Area under the curve
- CI:
-
Confidence interval
- HR:
-
Hazard ratio
- PTCL:
-
Peripheral T-cell Lymphomas
- AITL:
-
Angioimmunoblastic T-cell lymphoma
References
Sehn LH, Salles G. Diffuse large B-Cell lymphoma. N Engl J Med. 2021;384(9):842–58.
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and Mortality Worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–49.
Coiffier B, Thieblemont C, Van Den Neste E, Lepeu G, Plantier I, Castaigne S, Lefort S, Marit G, Macro M, Sebban C, et al. Long-term outcome of patients in the LNH-98.5 trial, the first randomized study comparing rituximab-CHOP to standard CHOP chemotherapy in DLBCL patients: a study by the Groupe d’Etudes des Lymphomes de l’Adulte. Blood. 2010;116(12):2040–5.
Crump M, Neelapu SS, Farooq U, Van Den Neste E, Kuruvilla J, Westin J, Link BK, Hay A, Cerhan JR, Zhu L, et al. Outcomes in refractory diffuse large B-cell lymphoma: results from the international SCHOLAR-1 study. Blood. 2017;130(16):1800–8.
International Non-Hodgkin’s Lymphoma Prognostic Factors P. A predictive model for aggressive non-hodgkin’s lymphoma. N Engl J Med. 1993;329(14):987–94.
Sehn LH, Berry B, Chhanabhai M, Fitzgerald C, Gill K, Hoskins P, Klasa R, Savage KJ, Shenkier T, Sutherland J, et al. The revised International Prognostic Index (R-IPI) is a better predictor of outcome than the standard IPI for patients with diffuse large B-cell lymphoma treated with R-CHOP. Blood. 2007;109(5):1857–61.
Zhou Z, Sehn LH, Rademaker AW, Gordon LI, Lacasce AS, Crosby-Thompson A, Vanderplas A, Zelenetz AD, Abel GA, Rodriguez MA, et al. An enhanced International Prognostic Index (NCCN-IPI) for patients with diffuse large B-cell lymphoma treated in the rituximab era. Blood. 2014;123(6):837–42.
Dlouhy I, Karube K, Enjuanes A, Salaverria I, Nadeu F, Ramis-Zaldivar JE, Valero JG, Rivas-Delgado A, Magnano L, Martin-Garcia D, et al. Revised International Prognostic Index and genetic alterations are associated with early failure to R-CHOP in patients with diffuse large B-cell lymphoma. Br J Haematol. 2022;196(3):589–98.
Ruppert AS, Dixon JG, Salles G, Wall A, Cunningham D, Poeschel V, Haioun C, Tilly H, Ghesquieres H, Ziepert M, et al. International prognostic indices in diffuse large B-cell lymphoma: a comparison of IPI, R-IPI, and NCCN-IPI. Blood. 2020;135(23):2041–8.
Barrington SF, Trotman J. The role of PET in the first-line treatment of the most common subtypes of non-hodgkin lymphoma. Lancet Haematol. 2021;8(1):e80–e93.
Cottereau AS, Meignan M, Nioche C, Capobianco N, Clerc J, Chartier L, Vercellino L, Casasnovas O, Thieblemont C, Buvat I. Risk stratification in diffuse large B-cell lymphoma using lesion dissemination and metabolic tumor burden calculated from baseline PET/CT(dagger). Annals of Oncology: Official Journal of the European Society for Medical Oncology. 2021;32(3):404–11.
Mikhaeel NG, Heymans MW, Eertink JJ, de Vet HCW, Boellaard R, Duhrsen U, Ceriani L, Schmitz C, Wiegers SE, Huttmann A et al. Proposed new dynamic prognostic index for diffuse large B-Cell lymphoma: International Metabolic Prognostic Index. J Clin Oncol. 2022:JCO2102063.
Delaby G, Hubaut MA, Morschhauser F, Besson A, Huglo D, Herbaux C, Baillet C. Prognostic value of the metabolic bulk volume in patients with diffuse large B-cell lymphoma on baseline (18)F-FDG PET-CT. Leuk Lymphoma. 2020;61(7):1584–91.
Zhang X, Chen L, Jiang H, He X, Feng L, Ni M, Ma M, Wang J, Zhang T, Wu S, et al. A novel analytic approach for outcome prediction in diffuse large B-cell lymphoma by [(18)F]FDG PET/CT. Eur J Nucl Med Mol Imaging. 2022;49(4):1298–310.
Jin H, Jin M, Lim CH, Choi JY, Kim SJ, Lee KH. Metabolic bulk volume predicts survival in a homogeneous cohort of stage II/III diffuse large B-cell lymphoma patients undergoing R-CHOP treatment. Front Oncol. 2023;13:1186311.
Cottereau AS, Nioche C, Dirand AS, Clerc J, Morschhauser F, Casasnovas O, Meignan M, Buvat I. (18)F-FDG PET dissemination features in diffuse large B-Cell lymphoma are Predictive of Outcome. J Nucl Med. 2020;61(1):40–5.
Cheson BD, Horning SJ, Coiffier B, Shipp MA, Fisher RI, Connors JM, Lister TA, Vose J, Grillo-Lopez A, Hagenbeek A, et al. Report of an international workshop to standardize response criteria for non-hodgkin’s lymphomas. NCI Sponsored International Working Group. J Clin Oncol. 1999;17(4):1244.
Cheson BD, Fisher RI, Barrington SF, Cavalli F, Schwartz LH, Zucca E, Lister TA, Alliance AL, Lymphoma G, Eastern Cooperative Oncology G, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-hodgkin lymphoma: the Lugano classification. J Clin Oncol. 2014;32(27):3059–68.
Cheson BD. Role of functional imaging in the management of lymphoma. J Clin Oncol. 2011;29(14):1844–54.
Metser U, Prica A, Hodgson DC, Mozuraitis M, Eberg M, Mak V, Green B, Singnurkar A, Dudebout J, MacCrostie P, et al. Effect of PET/CT on the management and outcomes of participants with Hodgkin and aggressive Non-Hodgkin Lymphoma: a Multicenter Registry. Radiology. 2019;290(2):488–95.
Ceriani L, Gritti G, Cascione L, Pirosa MC, Polino A, Ruberto T, Stathis A, Bruno A, Moccia AA, Giovanella L, et al. SAKK38/07 study: integration of baseline metabolic heterogeneity and metabolic tumor volume in DLBCL prognostic model. Blood Adv. 2020;4(6):1082–92.
Mikhaeel NG, Smith D, Dunn JT, Phillips M, Moller H, Fields PA, Wrench D, Barrington SF. Combination of baseline metabolic tumour volume and early response on PET/CT improves progression-free survival prediction in DLBCL. Eur J Nucl Med Mol Imaging. 2016;43(7):1209–19.
Tout M, Casasnovas O, Meignan M, Lamy T, Morschhauser F, Salles G, Gyan E, Haioun C, Mercier M, Feugier P, et al. Rituximab exposure is influenced by baseline metabolic tumor volume and predicts outcome of DLBCL patients: a Lymphoma Study Association report. Blood. 2017;129(19):2616–23.
Schmitz C, Huttmann A, Muller SP, Hanoun M, Boellaard R, Brinkmann M, Jockel KH, Duhrsen U, Rekowski J. Dynamic risk assessment based on positron emission tomography scanning in diffuse large B-cell lymphoma: post-hoc analysis from the PETAL trial. Eur J Cancer. 2020;124:25–36.
Albano D, Treglia G, Dondi F, Calabro A, Rizzo A, Annunziata S, Guerra L, Morbelli S, Tucci A, Bertagna F. (18)F-FDG PET/CT maximum tumor dissemination (Dmax) in lymphoma: a New Prognostic factor? Cancers (Basel). 2023;15(9).
Eertink JJ, van de Brug T, Wiegers SE, Zwezerijnen GJC, Pfaehler EAG, Lugtenburg PJ, van der Holt B, de Vet HCW, Hoekstra OS, Boellaard R, et al. (18)F-FDG PET baseline radiomics features improve the prediction of treatment outcome in diffuse large B-cell lymphoma. Eur J Nucl Med Mol Imaging. 2022;49(3):932–42.
Balkwill F. Cancer and the chemokine network. Nat Rev Cancer. 2004;4(7):540–50.
Moreno MJ, Bosch R, Dieguez-Gonzalez R, Novelli S, Mozos A, Gallardo A, Pavon MA, Cespedes MV, Granena A, Alcoceba M, et al. CXCR4 expression enhances diffuse large B cell lymphoma dissemination and decreases patient survival. J Pathol. 2015;235(3):445–55.
Chen J, Xu-Monette ZY, Deng L, Shen Q, Manyam GC, Martinez-Lopez A, Zhang L, Montes-Moreno S, Visco C, Tzankov A, et al. Dysregulated CXCR4 expression promotes lymphoma cell survival and independently predicts disease progression in germinal center B-cell-like diffuse large B-cell lymphoma. Oncotarget. 2015;6(8):5597–614.
Jiang X, Lu X, Gentles AJ, Zhao D, Wander SA, Zhang Y, Natkunam Y, Slingerland J, Reis IM, Rabinovich B, et al. HGAL inhibits lymphoma dissemination by interacting with multiple cytoskeletal proteins. Blood Adv. 2021;5(23):5072–85.
Acknowledgements
None.
Funding
This work was supported partly by Foundation of Changzhou Sci&Tech Program (Grant No. CJ20200118, CJ20210075), Changzhou High-Level Medical Talents Training Project (NO:2016ZCLJ024), and Key project of Jiangsu Province Health Committee (ZD2021043).
Author information
Authors and Affiliations
Contributions
Weiying Gu and Fei Wang conceived this study’s design and Yuetao Wang supervised the project. Silu Cui collected and analysed information of PET/CT image. Xiaoliang Shao, Jianfeng Wang and Yaqi Liu gave help to collect imaging information. Luo Lu and Yanhua Yue, Bai He, Feng Yan gave help to collect clinical information of DLBCL patients. Bai He, Feng Yan and Yang Cao gave help for the follow-up of patients. Fei Wang, Silu Cui and Luo Lu performed the analysis of the results. Fei Wang and Silu Cui edited the first manuscript and Weiying Gu and Yuetao Wang revised it. Finally, all authors reviewed this article. All authors reviewed the manuscript and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The present study was performed in accordance with the Declaration of Helsinki. Research protocol of this study was approved by the Ethics Committee institutional of the Third Affiliated Hospital of Soochow University (approval No. 155, approved date: 31 May 2022). The informed consent requirement for this study was waived with the agreement of the Ethics Committee institutional of the Third Affiliated Hospital of Soochow University, because the study was conducted retrospectively and the opportunity to refuse was guaranteed.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Figure S1
Measurement of MBV. MBV (cm3) was defined as the product of the cross-sectional area of the larger section of the largest lesion and section thickness. MBV, metabolic bulk volume. Table S1 Multivariable analysis of PFS and OS of DLBCL patient considering Dmax and MBV as continuous values. Table S2 Spearman correlation analysis of Dmax and MBA groups. Table S3 Multivariable analysis of PFS and OS of DLBCL patients staged based on Lugano System. Table S4 Multivariable analysis of IPI and Dmax
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, F., Cui, S., Lu, L. et al. Dissemination feature based on PET/CT is a risk factor for diffuse large B cell lymphoma patients outcome. BMC Cancer 23, 1165 (2023). https://doi.org/10.1186/s12885-023-11333-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-023-11333-z