
Abstract
Background
Lung cancer is one of the most lethal tumors with a poor survival rate even in those patients receiving new therapies. Metabolism is considered one of the hallmarks in carcinogenesis and lipid metabolism is emerging as a significant contributor to tumor metabolic reprogramming. We previously described a profile of some lipid metabolism related genes with potential prognostic value in advanced lung cancer.
Aim
To analyze clinical and pathological characteristics related to a specific metabolic lipid genomic signature from patients with advanced lung cancer and to define differential outcome.
Methods
Ninety samples from NSCLC (non-small cell lung cancer) and 61 from SCLC (small cell lung cancer) patients were obtained. We performed a survival analysis based on lipid metabolic genes expression and clinical characteristics. The primary end point of the study was the correlation between gene expression, clinical characteristics and survival.
Results
Clinical variables associated with overall survival (OS) in NSCLC patients were clinical stage, adenocarcinoma histology, Eastern Cooperative Oncology Group (ECOG), number and site of metastasis, plasma albumin levels and first-line treatment with platinum. As for SCLC patients, clinical variables that impacted OS were ECOG, number of metastasis locations, second-line treatment administration and Diabetes Mellitus (DM). None of them was associated with gene expression, indicating that alterations in lipid metabolism are independent molecular variables providing complementary information of lung cancer patient outcome.
Conclusions
Specific clinical features as well as the expression of lipid metabolism-related genes might be potential biomarkers with differential outcomes.
Similar content being viewed by others


Introduction
Lung cancer is the leading cause of cancer-related death worldwide. It is also the main cause of cancer death among men and the second among women [1]. Almost 90% of cases are due to tobacco exposition but the incidence in non-smokers is increasing [2]. Some other environmental agents such as radon, asbestos, ionizing radiation and some diseases such as pulmonary fibrosis and HIV (Human Immunodeficiency Virus) have been described as possible risk factors for lung cancer [3]. Over the last few years the influence of diet is gaining importance as a risk factor for cancer, but data regarding lung cancer is highly variable. Several prior studies suggest the protective effect of fruits and vegetables while others point to an increased risk of lung cancer in patients taking beta carotene supplements [4].
About 80–85% lung cancer cases are non-small cell lung cancer (NSCLC), with the most representative subtypes being adenocarcinoma and squamous cell tumors. Small cell lung cancer (SCLC) cases account for 10–15% of all lung malignant neoplasms.
Although some relevant studies suggest lung cancer mortality reduction by performing periodical computerized tomography [5, 6], at present this screening is not incorporated into clinical practice. Therefore, the main preventive strategy is smoking cessation, especially in groups with increasing incidence such as youth and women [5, 7]. Most new lung cancer cases are diagnosed in advanced stages and the outcome is poor.
Survival is influenced by clinical, pathologic and molecular factors. Clinical stage is the most important prognostic factor with better outcome for earlier stages. Performance status at diagnosis, determined by ECOG scale, and loss of weight are also relevant prognostic factors [8]. Chemotherapy, immunotherapy and biological treatments have also a growing impact in modifying natural history of lung cancer, mainly, NSCLC.
Some genetic alterations such as activating mutations in the gene encoding EGFR (epidermal growth factor receptor), MET (mesenchymal-to-epithelial transition protein), BRAF (v-raf murine sarcoma viral oncogene homolog B1), or RET (rearranged during transfection) and ROS1 (c-ros oncogene 1) rearrangements, are response predictive factors to targeted therapy [9] improving both quality of life and survival. PD-L1 (programmed death-ligand 1) expression in tumor cells and infiltrating peritumoral lymphocytes and tumor mutation burden (TMB) have been proposed as predictive markers of response to immune check-point inhibitors. Both targeted therapy and immune check-point control inhibitors have drastically changed lung cancer treatment landscape in the last decade.
Tumor cells can adapt their ability to metabolize nutrients to obtain energy even in a low-energy situation. Although most of knowledge in this area concerns carbohydrate metabolism, lipid metabolism is becoming increasingly important. Cancer cells might increase de novo lipogenesis (Fig. 1). Some enzymes involved in this process such as Acetyl-CoA thioesterase (ACOT) [10] may be over expressed in cases of poor prognosis lung cancer. Fatty acid synthase (FAS) also plays a major role in adipogenesis and some FAS-expressing tumors have poorer outcomes due to higher recurrence rates [11].

De novo lipogenesis in adipose tissues. TCA: tricarboxylic cycle. ACL: ATP-citrate lyase. ACC: acetyl-coA carboxylase. FAS: fatty acid synthase. SCD1: stearoyl-CoA desaturase-1
Adipocytes metabolism becomes quicker when tumor cells are present and secrete metabolic substrates such as fatty acids and glycerol. These will in turn be used by tumor cells to ensure growth and survival [12].
Most studies suggest a relationship between high plasma cholesterol levels and lung cancer incidence [13]. In addition, there is growing evidence about the association between obesity and risk of different types of cancer such as breast postmenopausal tumors, colorectal, endometrial, pancreatic, biliary tract cancer, etc.…However, data on lung cancer is not conclusive, and there are even some reports that suggest an inverse association between BMI (body mass index) and lung cancer risk [14]. On the other hand, obesity is associated with an immunosuppressive phenotype and proinflammatory status that could lead to better response to immune check-point inhibitors treatment in lung cancer patients [15].
We previously described a signature of a lipid metabolism-related genes panel with prognostic value biomarkers in NSCLC and SCLC [16, 17]. In this work, we enrich previous molecular data with an analysis of clinical features, histologic characteristics and relevant laboratory parameters, as well as clinical outcomes of patients with advanced lung cancer.
Materials and methods
Patient´s selection
A total of 151 formalin-fixed, paraffin-embedded (FEPE) samples were obtained from a sample of NSCLC and SCLC patients from the Medical Oncology Department of Infanta Sofía University Hospital (San Sebastián de los Reyes, Madrid). Patients were enrolled from November 1, 2008 to September 31, 2017 and all cases were stage IIIB (no candidates to radical radiation) or IV. They were treated according to clinical international guidelines. Clinical, analytical and pathological data was collected from electronic medical reports. FFPE samples were studied by an anatomic pathologist confirming > 80% of tumor cells. The study was approved by the IMDEA Food Research Ethics Committee. Overall survival (OS) was defined from the date of diagnosis to the date of patient death and progression-free survival (PFS) was defined from the data of start of chemotherapy to the date of progression.
Clinical variables included were age, gender, clinical stage, histology (adenocarcinoma, squamous cell and small cell or “oat cell”), EGFR/ALK (Anaplastic lymphoma kinase) mutation status, ECOG performance status (0–1 vs 2–4), loss of weight and BMI. Laboratory parameters involved in cholesterol and glucose metabolism such as albumin, total, HDL (high-density lipoprotein) and LDL (low-density lipoprotein)-cholesterol levels were included. Relevant comorbidities were also analyzed, mainly, those related to metabolism like diabetes mellitus (DM) and dyslipidemia (DL). We also described tumor burden, metastasis location as well as number of metastatic sites and chemotherapy regimen. It should be noted that all patients included were treated before 2017, (pre-immunotherapy era) therefore first line treatments were based on platinum agents instead of chemo-immunotherapy combination or immunotherapy.
Gene selection
We designed a Taq-Man Low-Density Array formed of 22 lipid metabolism-related genes as previously described [16]. Gene expression assay was performed in HT-7900 Fast-Real-time PCR. These genes were selected due to their role as regulators of cell metabolism, major steps of interconnection among lipid pathways and their reported role as potential prognostic biomarkers in several types of cancer [18].
Statistical analysis
The primary endpoint of the study was the relationship between gene expression and survival: OS and PFS. We also assessed the potential association between clinical and histologic patient features and outcomes. The Kaplan–Meier method was used to estimate OS curves, and Cox regression analysis was used to test the association between OS, PFS and clinical variables. Absolute values and percentages were used to describe qualitative variables while mean and median were used for quantitative variables. Range and standard deviation were used as dispersion measures. Overall survival and progression-free survival has been represented using the Kaplan–Meier method and univariate and multivariate Cox regression analysis were used to assess the association between overall survival and clinical variables. Bootstrapping with 1000 samples was used to calculate an optimism-corrected C-statistic. Statistical significance was defined as p-value < 0.05. The Bonferroni method was applied for multiple test correction of the p-values.
Results
Clinical characteristics of 151 lung cancer patients included are summarized in Table 1.
We present all collected data split according to lung cancer subtype: NSCLC and SCLC.
Non-small cell lung cancer
Ninety patients with NSCLC were included. Median age was 64 years. The majority were males (75%) and more than a half smokers (52%) or former smokers (34%). Half of patients (51%) had ECOG performance status of 1 and 18%, 24%, 3.3% and 3.7% had ECOG of 0, 2, 3 and 4 respectively. Around 70% had stage IV NSCLC and bones were the most common site of metastasis.
Median BMI was 25. Regarding comorbidities, 19% of all patients had DM and 27% DL, all of them were on statins treatment.
Less than 4% of patients had a driver mutation, thus platinum-based chemotherapy was used in first line in almost all NSCLC patients; being carboplatin/docetaxel and carboplatin/paclitaxel/bevacizumab the most widely used regimens (Table 2).
The previous survival analysis performed in a series of 90 NSCLC patients had showed significant association with OS for three genes: Acyl-CoA synthetase long-chain family member 3 (ACSL3), Nidogen 1 (NID1) and Resistin (RETN) [16]. Results are summarized in Table 3.
Clinical variables statistically associated with both better PFS and OS, were clinical stage, adenocarcinoma histology, ECOG 0–1, number and site of metastasis and plasma albumin levels. Statins treatment for dyslipidemia only demonstrated a significant impact on PFS while first line treatment based on platinum combination, had a significant relationship with better OS (Table 4). None of the patients included received immunotherapy because it had not been approved in this setting at the moment of recruitment.
We assessed the potential relationship between expression of these genes statistically associated with OS in NSCLC and clinical features without finding any significant result. We also ran a multiple regression analysis to test for the effect of one variable while correcting for differences in other variables (Table 5).
P-Value from the likelihood ratio test that compares this model with a similar one without genetic variables is 0.00012. Therefore, relationship between gene expression and OS is statistically significant and adds predictive capacity to our model.
Small cell lung cancer
Data from 61 patients with SCLC were analyzed. Most of them were males (73%), with a median age of 65 years. More than sixty percent of patients (67%) were smokers and 24% former smokers. Median BMI was 20 and more than a half of patients had ECOG PS of 0–1 (80%) while the rest had ECOG 2 (13%), 3 (2,7%) and 4 (2.7%). Patients with diabetes were 19% and almost all of them were on metformin treatment, while all dyslipidemic patients (59%) were being treated with statins. Most patients included (78%) had stage IV disease and most common site of metastasis was the liver followed by central nervous system. Almost every patient received platinum-etoposide as first line treatment (Table 6). Median PFS was 3.6 months and median OS was 6 months.
We had also tested the panel of 22 lipid metabolism genes in a set of 61 SCLC samples and found statistically significant association with OS for 2 genes: Alpha-Methylacyl-CoA Racemase (AMACR) and Perilipin 1 (PLIN1) [17]. Results are summarized in Table 7.
While ECOG and number of metastatic locations had a relevant impact on OS, second line chemotherapy administration, DM and metformin treatment were statistically associated with both PFS and OS (Table 8).
We also assessed the association between expression of genes significantly associated with OS in SCLC and clinical features without statistically significant results.
Finally, we tested the inclusion of second-line treatment (highly significant in the descriptive analysis) in our previously published model [17], which included an AMACR + PLIN1 genetic risk score as well as gender, age, stage, smoking status and metabolic health as predictor variables. In this model, p-value for second-line treatment was 0.0012 (Table 9).
In addition, we validated both models using Bootstrap resampling, to assess whether the inclusion of second-line treatment provided additional predictive value. The optimism-corrected c-index was 0.701 for the previous model and 0.731 for the current one, indicating a slight increase in predictive power without overfitting.
Discussion
In the present study 86% and 91% of patients with NSCLC and SCLC, respectively, were smokers or former smokers. This is consistent with data from occidental countries, where the rate of lung cancer patients with active tobacco use is 90% [19]. Nearly all patients treated with chemotherapy used a platinum based regimen, according to clinical guides [20]. Fifteen percent of NSCLC and 1% of SCLC patients did not receive any oncologic specific treatment at all due to poor ECOG at diagnosis. This difference might be explained because of a higher chemo sensitivity and heavier symptom burden in SCLC vs NSCLC. In clinical practice, we have observed a clear clinical benefit from chemotherapy in SCLC, even in those patients with an important ECOG deterioration due to cancer [21].
Non-small cell lung cancer
Lung cancer mortality remains high despite recent major advances in oncology and precision medicine is one of the most promising strategies to improve survival. This requires firstly establishing specific prognostic groups to discriminate those patients with different outcome. Lipid metabolism has been raised as a potential target for cancer diagnosis, prognosis and treatment [22] and lipid metabolism alterations have been described as prognostic biomarkers in several types of cancer [23].
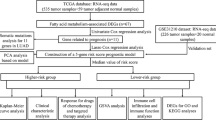
In our previous work, we had found that ACSL3, NID1 and RETN expression were associated with poor survival and as we showed in preclinical tests, patients could benefit of antitumor properties of statin administration. In addition, to validate these results, we also performed a parallel analysis based on ACSL3, NID1, and RETN expression in larger series of NSCLC samples from The Cancer Genome Atlas (TCGA) study, ACSL and RETN expression had an overall survival risk effect [16]. There is some preclinical evidence related to our data.
ACSLs are responsible for activating long-chain fatty acids and are frequently deregulated in cancer. They are mainly expressed in the endoplasmic reticulum and lipid droplets. Among the 5 mammalian ACSL families ACSL3 has been detected in several types of cancer and high expression correlates with worse prognosis in patients with melanoma and triple negative breast cancer [24] and might be involved in prostate carcinogenesis [25].
NID1 is a glycoprotein found in basement membranes. It is essential for structural integrity through connecting the collagen IV and laminin networks, increasing stability. Other authors have investigated the impact of NID1 in cancer suggesting a potential negative prognostic role but prospective data are lacking and, in the end, results are inconclusive. Alecovic et al.analyzed secretome of lung metastasis sublines of human breast cancer and found that overexpression of NID1 increased lung metastasis and reduced survival [26] while Ferrero et al.showed that secretion of NID1 from endothelial cells inhibited migration of human breast cancer cells SK-BR-3 [27].
Finally, RETN is a member of the cysteine-rich proteins family secreted from adipocytes and monocytes in humans and may play a role in modulating cancer pathogenesis. Previous studies found that expression increases along with the progression of some tumors including breast, prostate, colon, gastric and endometrial cancers [28]. It also promotes metastasis in chondrosarcoma and breast tumors [29, 30]. As mentioned in our previous work we demonstrated that RETN expression has a negative impact on OS in NSCLC patients. There are few data on this topic but almost all the results are consistent with our study. Zhao CC et al.assessed RETN expression in 70 pairs of lung adenocarcinomas and normal tissues and analyzed in vitro cell behavior, clinical characteristics of tumors and outcomes. They found that resistin expression was significantly associated with increased tumor size, clinical stage and lymph node metastasis, and negatively associated with PFS and OS [31]. Therefore, resistin could be a potential target for NSCLC.
In addition to our finding of a potential lipid metabolism related signature, some classical clinical and pathologic features were associated to OS. In the present analysis OS was associated with clinical stage, ECOG at diagnosis, histology, plasma albumin levels, distant metastasis and number of metastatic sites. These findings are consistent with literature. Clinical stage and performance status are the most important prognostic factors. Survival is higher for early stages with 2 years OS rate of 90% for patients with stage I tumors and around 10% for patients with stage IV [32] and patients with robust PS (performance status) live longer than those with ECOG 1 or superior [33].
Tumor burden could also influence the outcomes; patients with oligometastatic disease are more likely to undergo local aggressive treatments such as radiotherapy or surgical removal of metastasis, which could result in both longer disease-free interval and overall survival [34]. Regarding chemotherapy, platinum-treated patients had the longer OS in this series. In daily clinical practice these patients are usually younger, have ECOG PS 0 or 1 and adequate organ function without significant comorbidities. Thus, this scenario could have an impact on treatment effectiveness and survival.
Histology has a controverted role in NSCLC prognosis. While there are some data suggesting that patients with early stage lung adenocarcinoma live longer [35], most of studies attribute longer survival to patients with resected squamous cell carcinoma [36]. However, patients with advanced lung adenocarcinoma have better outcomes than squamous cell carcinoma, especially if a driver mutation is detected.
Regarding laboratory parameters, we found that serum albumin is a marker of nutritional status and can be affected by situations of inflammation. Pro-inflammatory cytokines have an impact on albumin synthesis and could contribute to low albumin levels in situations of chronic inflammation such as cancer. Adequate albumin levels are described as a prognostic factor in several types of malign tumors including lung cancer [37]. Consistently, in our series, normal serum albumin was associated with longer survival.
Smoking and loss of weight at diagnosis can also influence prognosis [37]. Additionally increased lipolysis in adipose tissues leads to cachexia, affecting 60% of lung cancer patients. Therefore, cachexia has also been proposed as a potential prognostic factor [38]. However, we did not find a significant association between neither of these parameters and survival, probably due to the small sample size.
In these days, there is a growing interest in learning about the role of statins in lung cancer. Although treatment with statins has not yet demonstrated an impact on survival in randomized clinical trials, a growing body of preclinical and observational research suggests that they have a potential as a therapeutic strategy in lung cancer [39]. Our study did not show statistically significant improvement in OS but patients who were treated with statins tend to have better clinical outcome.
We also conducted several preclinical tests to assess the anticancer effect of statins in human NSCLC cells and observed that simvastatin significantly modulated genes related to lipid metabolism and induced apoptosis activation [16]. Thus statins might have a role as targeted treatment in selected NSCLC patients.
Neither the expression of ACSL3, NID1 or RETN was associated with any clinical features. However, clinical stage and performance status at diagnosis are already recognized prognostic factors and, as we described in the main analysis, they had a statistically association with OS. Surprisingly, although gene expression had a significantly influence on outcome, it was not related to these features, supporting the hypothesis that the expression of these genes is an independent prognostic factor.
Small cell lung cancer
A relevant lipid metabolism signature was also described in SCLC setting. As we previously showed, we found statistically significant association with better OS for two genes: Alpha-Methylacyl-CoA Racemase (AMACR) and Perilipin 1 (PLIN1) [17].
AMACR is an enzyme localized in both mitochondria and peroxisomes involved in peroxisome oxidation. There are previous studies that report an association of AMACR expression with better SCLC prognosis. Shilo K et al.reported a series of 72 SCLC where 51% were positive for AMACR. These patients had better survival than those with AMCR-negative tumors [40]. However, differences in AMCR expression have not been associated to outcomes in NSCLC [41].
PLIN1 is a protein that coats lipid droplets in adipocytes protecting them from the action of lipase. It is localized on the surface of intracellular lipid droplets. Phosphorylation of perilipin is essential for the mobilization of fats in adipose tissue and when it is unphosphorylated, blocks lipolysis [42]. It has been reported as a biomarker in some tumors such as breast, low-grade glioma, hepatocellular carcinoma and sarcoma, with a relevant prognostic value in breast tumors, but to date there was no data on lung cancer.
Besides genetic expression, we assessed the relationship between clinical and pathologic features and outcomes in SCLC. Although clinical stage and functional status are recognized prognostic factors, there are no conclusive data in the literature on the influence of other clinical parameters on survival.
In this study ECOG performance status at diagnosis, number of metastatic sites, second line treatment and DM had an impact on overall survival. Performance status and loss of weight are the most important patient-dependent prognostic factors in SCLC [8]. We were not able to find a relationship between loss of weight and survival but it could be easily explained by the fact that the proportion of patients with weight loss in our series was minimal and all of them had NSCLC. As stated above, patients with better functional status tend to live longer [33] and they usually receive full-dose treatments, with no delays, which could contribute to better outcomes. Patients who maintain good ECOG beyond progression are candidates for second-line treatment. In this study only 11 patients received second-line chemotherapy but it was still associated with statistically significant longer OS, reaching 30 months in some cases. Furthermore, it was a statistically significant variable in the multiple regression test, and by adding it, we were able to improve the predictive capacity of our previous model. However, sample size is limited and we should consider a positive selection of patients with fewer symptoms, better response to prior chemotherapy and better ECOG performance status. The most important prognostic factor in SCLC is clinical stage at diagnosis [43]. We were unable to show this relationship in our study, possibly because of underrepresentation of stage III tumors in our series.
Although we found a relationship between pre diagnosis DM and OS, there is no prospective data supporting it as a prognostic factor in SCLC, however there are quite observational studies that suggest a negative impact of DM on survival in NSCLC [44]. Metformin, an oral antidiabetic drug, has been proposed as an adjuvant therapeutic agent in lung cancer treatment because of its potential antiproliferative effect against tumor cells. Anyway, to date the results are controversial [45]. More studies are needed to confirm these findings.
Serum albumin levels have been described as a prognostic factor in SCLC [46, 47] but, opposite to NSCLC, in this SCLC sample we did not find a statistically significant impact on survival. This could have been influenced by the fact that no SCLC patient in this group had loss of weight at diagnosis which could have led to a selection bias for well-nourished patients.
As in NSCLC, there was not a significant association between AMACR and PLIN1 expression and clinical parameters, confirming again that they might be prognostic biomarkers for all patients with SCLC regardless of clinical phenotype.
Our results are largely consistent with previously reported data, therefore, even if it is a retrospective series with limited sample, it could be considered representative and might help to generate hypothesis to select prognostic groups that may benefit from specific therapeutic strategies.
Conclusions
Lipid metabolism alterations are relevant in lung cancer development. ACSL3, NID1 and RETN expression could be independent negative prognostic markers in NSCLC while AMCR and PLIN1 might be related to better outcomes in SCLC. These results indicate that NSCLC and SCLC display different lipid-related metabolic profiles, which could complement the prognostic value of classical clinical characteristics. In addition, these findings could be important for developing potential novel treatment strategies based on the regulation of lipid metabolism.
Availability of data and materials
All data generated or analyzed during this study are included in these published articles:
Paula Fernandez L, Merino M, Colmenarejo G, Moreno-Rubio J, Sanchez-Martinez R, Quijada-Freire A, et al. Metabolic enzyme ACSL3 is a prognostic biomarker and correlates with anticancer effectiveness of statins in non-small cell lung cancer. Molecular Oncology. 2020;14(12):3135–52.
Fernandez LP, Merino M, Colmenarejo G, Moreno Rubio J, Gonzalez Pessolani T, Reglero G, et al. Metabolic Health Together with a Lipid Genetic Risk Score Predicts Survival of Small Cell Lung Cancer Patients. Cancers. 2021;13(5).
References
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca-a Cancer J Clin. 2021;71(3):209–49.
Rivera GA, Wakelee H. Lung Cancer in Never Smokers. Adv Exp Med Biol. 2016;893:43–57.
Mouronte-Roibas C, Leiro-Fernandez V, Fernandez-Villar A, Botana-Rial M, Ramos-Hernandez C, Ruano-Ravina A. COPD, emphysema and the onset of lung cancer. A systematic review Cancer Letters. 2016;382(2):240–4.
Tanvetyanon T, Bepler G. Beta-carotene in multivitamins and the possible risk of lung cancer among smokers versus former smokers - A meta-analysis and evaluation of national brands. Cancer. 2008;113(1):150–7.
Aberle DR, Adams AM, Berg CD, Black WC, Clapp JD, Fagerstrom RM, et al. Reduced Lung-Cancer Mortality with Low-Dose Computed Tomographic Screening. N Engl J Med. 2011;365(5):395–409.
Yousaf-Khan U, van der Aalst C, de Jong PA, Heuvelmans M, Scholten E, Lammers J-W, et al. Final screening round of the NELSON lung cancer screening trial: the effect of a 2.5-year screening interval. Thorax. 2017;72(1):48–56.
Walter JE, Heuvelmans MA, de Jong PA, Vliegenthart R, van Ooijen PMA, Peters RB, et al. Occurrence and lung cancer probability of new solid nodules at incidence screening with low-dose CT: analysis of data from the randomised, controlled NELSON trial. Lancet Oncology. 2016;17(7):907–16.
Paesmans M, Sculier JP, Lecomte J, Thiriaux J, Libert P, Sergysels B, et al. Prognostic factors for patients with small cell lung carcinoma - Analysis of a series of 763 patients included in 4 consecutive prospective trials with a minimum follow-up of 5 years. Cancer. 2000;89(3):523–33.
Hirsch FR, Scagliotti GV, Mulshine JL, Kwon R, Curran WJ, Wu Y-L, et al. Lung cancer: current therapies and new targeted treatments. Lancet. 2017;389(10066):299–311.
Hung J-Y, Chiang S-R, Liu K-T, Tsai M-J, Huang M-S, Shieh J-M, et al. Overexpression and proliferation dependence of acyl-CoA thioesterase 11 and 13 in lung adenocarcinoma. Oncol Lett. 2017;14(3):3647–56.
Visca P, Sebastiani V, Botti C, Diodoro MG, Lasagni RP, Romagnoli F, et al. Fatty acid synthase (FAS) is a marker of increased risk of recurrence in lung carcinoma. Anticancer Res. 2004;24(6):4169–73.
Li F-F, Zhang H, Li J-J, Cao Y-N, Dong X, Gao C. Interaction with adipocytes induces lung adenocarcinoma A549 cell migration and tumor growth. Mol Med Rep. 2018;18(2):1973–80.
Yang JJ, Yu D, Takata Y, Smith-Warner SA, Blot W, White E, et al. Dietary Fat Intake and Lung Cancer Risk: A Pooled Analysis. J Clin Oncol. 2017;35(26):3055.
Smith L, Brinton LA, Spitz MR, Lam TK, Park Y, Hollenbeck AR, et al. Body Mass Index and Risk of Lung Cancer Among Never, Former, and Current Smokers. Jnci-J Natl Canc Inst. 2012;104(10):778–89.
GelibterOcchipinti AM, Pisegna S, Cortellini A, Cortesi E, Marchetti P. Status of correlation between BMI and response to immunocheck-point inhibitor in advanced non-small-cell lung cancer. Lung Cancer Manag. 2020;9(2):LMT26.
Paula Fernandez L, Merino M, Colmenarejo G, Moreno-Rubio J, Sanchez-Martinez R, Quijada-Freire A, et al. Metabolic enzyme ACSL3 is a prognostic biomarker and correlates with anticancer effectiveness of statins in non-small cell lung cancer. Mol Oncol. 2020;14(12):3135–52.
Fernandez LP, Merino M, Colmenarejo G, Moreno Rubio J, Gonzalez Pessolani T, Reglero G, et al. Metabolic Health Together with a Lipid Genetic Risk Score Predicts Survival of Small Cell Lung Cancer Patients. Cancers. 2021;13(5):1112.
Vargas T, Moreno-Rubio J, Herranz J, Cejas P, Molina S, Gonzalez-Vallinas M, et al. ColoLipidGene: signature of lipid metabolism-related genes to predict prognosis in stage-II colon cancer patients. Oncotarget. 2015;6(9):7348–63.
Warren GW, Cummings KM. Tobacco and lung cancer: risks, trends, and outcomes in patients with cancer. Am Soc Clin Oncol Educ Book Am Soc Clin Oncol Annu Meet. 2013;33:359–64.
Hanna NH, Temin S, Masters G. Therapy for Stage IV Non-Small-Cell Lung Cancer Without Driver Alterations: ASCO and OH (CCO) Joint Guideline Update Summary. Jco Oncology Practice. 2020;16(8):E844–8.
Bahij R, Jeppesen SS, Olsen KE, Halekoh U, Holmskov K, Hansen O, et al. Outcome of treatment in patients with small cell lung cancer in poor performance status. Acta Oncol. 2019;58(11):1612–7.
Beloribi-Djefaflia S, Vasseur S, Guillaumond F. Lipid metabolic reprogramming in cancer cells. Oncogenesis. 2016;5:1–10.
Vargas T, Moreno-Rubio J, Herranz J, Cejas P, Molina S, Mendiola M, et al. 3 ’ UTR polymorphism in ACSL1 gene correlates with expression levels and poor clinical outcome in colon cancer patients. PLoS One. 2016;11(12):1–15.
Jeong HM, Kim RN, Kwon MJ, Oh E, Han J, Lee SK, et al. Targeted exome sequencing of Korean triple-negative breast cancer reveals homozygous deletions associated with poor prognosis of adjuvant chemotherapy-treated patients. Oncotarget. 2017;8(37):61538–50.
Wilson S, Fan L, Sahgal N, Qi J, Filipp FV. The histone demethylase KDM3A regulates the transcriptional program of the androgen receptor in prostate cancer cells. Oncotarget. 2017;8(18):30328–43.
Aleckovic M, Wei Y, LeRoy G, Sidoli S, Liu DD, Garcia BA, et al. Identification of Nidogen 1 as a lung metastasis protein through secretome analysis. Genes Dev. 2017;31(14):1439–55.
Ferraro DA, Patella F, Zanivan S, Donato C, Aceto N, Giannotta M, et al. Endothelial cell-derived nidogen-1 inhibits migration of SK-BR-3 breast cancer cells. Bmc Cancer. 2019;19:312.
Hlavna M, Kohut L, Lipkova J, Bienertova-Vasku J, Dostalova Z, Chovanec J, et al. Relationship of resistin levels with endometrial cancer risk. Neoplasma. 2011;58(2):124–8.
Lee Y-C, Chen Y-J, Wu C-C, Lo S, Hou M-F, Yuan S-SF. Resistin expression in breast cancer tissue as a marker of prognosis and hormone therapy stratification. Gynecol Oncol. 2012;125(3):742–50.
Tsai C-H, Tsai H-C, Huang H-N, Hung C-H, Hsu C-J, Fong Y-C, et al. Resistin promotes tumor metastasis by down-regulation of miR-519d through the AMPK/p38 signaling pathway in human chondrosarcoma cells. Oncotarget. 2015;6(1):258–70.
Zhao C-C, Chen J, Niu R-F, Liu Y, Zhang C-G. Increased resistin suggests poor prognosis and promotes development of lung adenocarcinoma. Oncol Rep. 2018;40(6):3392–404.
Goldstraw P, Chansky K, Crowley J, Rami-Porta R, Asamura H, Eberhardt WEE, et al. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J Thorac Oncol. 2016;11(1):39–51.
Kawaguchi T, Takada M, Kubo A, Matsumura A, Fukai S, Tamura A, et al. Performance Status and Smoking Status Are Independent Favorable Prognostic Factors for Survival in Non-small Cell Lung Cancer A Comprehensive Analysis of 26,957 Patients with NSCLC. J Thorac Oncol. 2010;5(5):620–30.
Patel PR, Yoo DS, Niibe Y, Urbanic JJ, Salama JK. A call for the aggressive treatment of oligometastatic and oligo-recurrent non-small cell lung cancer. Pulmonary med. 2012;2012:480961-.
Sterlacci W, Tzankov A, Veits L, Oberaigner W, Schmid T, Hilbe W, et al. The Prognostic Impact of Sex on Surgically Resected Non-Small Cell Lung Cancer Depends on Clinicopathologic Characteristics. Am J Clin Pathol. 2011;135(4):611–8.
Strand TE, Rostad H, Moller B, Norstein J. Survival after resection for primary lung cancer: a population based study of 3211 resected patients. Thorax. 2006;61(8):710–5.
Miura K, Hamanaka K, Koizumi T, Kitaguchi Y, Terada Y, Nakamura D, et al. Clinical significance of preoperative serum albumin level for prognosis in surgically resected patients with non-small cell lung cancer Comparative study of normal lung, emphysema, and pulmonary fibrosis. Lung Cancer. 2017;111:88–95.
Jafri SHR, Previgliano C, Khandelwal K, Shi R. Cachexia Index in Advanced Non-Small-Cell Lung Cancer Patients. Clinical Medicine Insights-Oncology. 2015;9:87–93.
Xia D-K, Hu Z-G, Tian Y-F, Zeng F-J. Statin use and prognosis of lung cancer: a systematic review and meta-analysis of observational studies and randomized controlled trials. Drug Des Dev Ther. 2019;13:405–22.
Shilo K, Dracheva T, Mani H, Fukuoka J, Sesterhenn IA, Chu W-S, et al. alpha-methylacyl CoA racemase in pulmonary adenocarcinoma, squamous cell carcinoma, and neuroendocrine tumors - Expression and survival analysis. Arch Pathol Lab Med. 2007;131(10):1555–60.
Erdogan Y, Demirag F, Duyar SS, Yilmaz A, Yazici U, Aydogdu K. Clinical significance of the expression of Alpha-methylacyl-CoA Racemase in Squamous Cell Carcinoma and Adenocarcinoma of the Lung. Acta Chir Belg. 2013;113(4):263–9.
Sztalryd C, Brasaemle DL. The perilipin family of lipid droplet proteins: Gatekeepers of intracellular lipolysis. BBA-Mol Cell Biol L. 2017;1862(10):1221–32.
Lassen U, Osterlind K, Hansen M, Dombernowsky P, Bergman B, Hansen HH. Long-term survival in small-cell lung-cancer - posttreatment characteristics in patients surviving 5 to 18+ years - an analysis of 1,714 consecutive patients. J Clin Oncol. 1995;13(5):1215–20.
Bi G, Yao G, Bian Y, Xue L, Zhang Y, Lu T, et al. The Effect of Diabetes Mellitus on Prognosis of Patients with Non-Small-Cell Lung Cancer: A Systematic Review and Meta-Analysis. Ann Thorac Cardiovasc Surg. 2020;26(1):1–12.
Levy A, Doyen J. Metformin for non-small cell lung cancer patients: Opportunities and pitfalls. Crit Rev Oncol Hematol. 2018;125:41–7.
Sculier J-P, Chansky K, Crowley JJ, Van Meerbeeck J, Goldstraw P, Int Staging Committee P. The impact of additional prognostic factors on survival and their relationship with the anatomical extent of disease expressed by the 6th edition of the TNM classification of malignant tumors and the proposals for the 7th edition. J Thorac Oncol. 2008;3(5):457–66.
Yang N, Han X, Yu J, Shu W, Qiu F, Han J. Hemoglobin, albumin, lymphocyte, and platelet score and neutrophil-to-lymphocyte ratio are novel significant prognostic factors for patients with small-cell lung cancer undergoing chemotherapy. J Cancer Res Ther. 2020;16(5):1134–9.
Acknowledgements
not applicable
Funding
This research was funded by grants to ARM from the Ministerio de Ciencia e Innovación, Spain (PID2019-110183RB-C21), Ramon Areces Foundation (CIVP19A5937) and Regional Government of Community of Madrid (P2018/BAA-4343-ALIBIRD2020-CM and NutriSION-CM Y2020/BIO-6350), REACT EU Program (FACINGLCOVID-CM project, Comunidad de Madrid and The European Regional Development Fund (ERDF) European Union) and EU Structural Funds.
Author information
Authors and Affiliations
Contributions
Conceptualization, MMS, LPF, ARM and MS; Data curation LPF, JMR, GC and ARM; Formal analysis, MMS, LPF and ARM; Funding acquisition, LPF and ARM; Methodology, MMS, LPF, JMR, GC, ARM and MS; Software, GC; Supervision, LPF, EC, ARM; Validation, MMS and MS; Writing – original draft, MMS, LPF, EC, ARM and MS; Writing – review & editing, MMS, LPF, ARM and MS. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of IMDEA Food (Ethical code: IMD: PI-0013). Patient consent was waived due to the retrospective nature of the study. Requirement for informed consent was waived by the IMDEA Food Research Ethics Committee. (Ethical code: IMD: PI-0013).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Merino Salvador, M., Fernández, L.P., Moreno-Rubio, J. et al. Clinical features and lipid metabolism genes as potential biomarkers in advanced lung cancer. BMC Cancer 23, 36 (2023). https://doi.org/10.1186/s12885-023-10509-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-023-10509-x