
Abstract
Background
Breast cancer incidence is rising globally, while mortality rates show a geographical heterogenous pattern. Early detection and treatment have been proven to have a profound impact on breast cancer prognosis. The aim of his study was to compare breast cancer incidence, mortality, and survival rates in two contrasting corners of Europe, Sweden and Crete, to better understand cancer determinants with focus on disease burden and sociocultural factors.
Methods
Breast cancer data from Sweden and Crete was derived from registries. Incidence and mortality were expressed as Age-Standardized Incidence Rates (ASIR), Age-Standardized Mortality Rates (ASMR).
Findings
Breast cancer incidence has for decades risen in Sweden and on Crete. In 2019, ASIR was 217.5 in Sweden and 58.9 on Crete, (p < 0.001). Mortality rates showed opposite trends. ASMR in Sweden was reduced from 25.5 to 16.8 (2005-2019) while on Crete, ASMR increased from 22.1 to 25.3. A successive rise in survival rate in Sweden with a 5-year survival rate of 92% since 2015, but a converse development on Crete with 85% 5-year survival rate the same year.
Interpretation
The incidence of breast cancer is slowly rising in both studied regions, but mortality increases on Crete in contrast to Sweden with sinking mortality rates. The interpretation of these findings is that differences in health care systems and health policies including differences in early detection like screening programs and early treatment, as well as sociocultural factors in the two countries might play an important role on the differences found in breast cancer burden.
Similar content being viewed by others


Background
The frequency of breast cancer rises in almost every region globally and in all age groups [1]. Recent data shows for the first time that breast cancer is the most frequently diagnosed cancer in women worldwide [2]. The total number of deaths from breast cancer constituted 15% of all cancer-related deaths globally in 2018 [3]. For females, breast cancer is the deadliest form of cancer disease, and the global burden of breast cancer increases in both premenopausal and postmenopausal age groups [3, 4]. In Sweden, breast cancer currently accounts for 30% of all cancer cases of women [5] and the corresponding data for Greece is 27.5% [6]. The implication of breast cancer disease also includes aspects of psychosocial health and quality of life [7].
Radiation is the most established risk factor for breast cancer, generating DNA-damage in breast tissue [8]. However, around 5-10% of all breast cancer cases are linked to heredity [9]. General underlying mechanisms of breast cancer have been coupled to the estrogen pathway, i.e., long-term exposure of female sex-hormones due to factors such as early menarche and late menopause, nullipara, high age at first child etc. [10], but also the increase in life expectancy per se [2]. Suggested potential non-estrogenic risk factors with various degree of scientific evidence are alcohol consumption, physical inactivity [11], and psychosocial factors such as social stress [12, 13]. Also, in a salutogenic perspective, dietary factors such as the Mediterranean diet has been extensively studied, although with shifting results [14]. Earlier comparative studies between Sweden and Greece from our group have shown differences in morbidity, both from cancer and cardiovascular disease [15]. There are differences in the health care systems and structures but also in health care utilization, drug prescription, perceived health, health literacy and risk perceptions between the populations of these two regions in Europe [16, 17].
According to current knowledge, early detection with early, effective treatment are the fundamental factors improving breast cancer prognosis [2, 18]. In Sweden, a national screening program for early detection of breast cancer is used since the 1980’s, and since 2015, a national streamlined standardized course of investigation is implemented to reduce time-intervals during the diagnostical process [19]. In Greece, a national screening program is also available but not fully implemented in practice till today, since there is no systematic approach in monitoring, reminding or following-up individuals at risk. Breast cancer screening is considered opportunistic [20].
With an explorative, epidemiological, and comparative view, we will in this study scrutinize trends in breast cancer data on Crete and in Sweden over the years. Cancer statistics of this epidemiological kind has previously not been available for Crete, only hospitalization data [15]. The aim of this study was to analyze and compare breast cancer incidence, mortality, and survival rates in Sweden and on Crete, Greece. By contrasting two corners of Europe representing the Scandinavian countries and the Mediterranean, we anticipate that such comparative view could assist both planners for health care services and clinical researchers to better understand cancer determinants with focus on cancer burden and sociocultural factors in various European settings, a topic on the epicenter of the current health policy discussion.
Materials and methods
Study design and data material
The study is an epidemiological, register study of national and regional data. ASIR corresponds to age-standardized incidence rate (per 100.000 inhabitants) and ASMR to age-standardized mortality rate (per 100.000 inhabitants). The incidence was calculated by a direct standardization approach according to the WHO/European standard population. The Swedish data collection was extracted from open registries of Swedish National Board of Health and Welfare (for ASIR) and NORDCAN (for ASMR), their collaborative database with WHO with age-standardization according to International Cancer Survival Standard [21]. The data included in this study constitutes of new breast cancer cases (for ASIR) among women of the total Swedish population. Age interval was 20-74 years, diagnosis ICD C50.X (in situ excluded) [21]. The Cretan population-based data derives from the regional cancer registry of Crete [22, 23]. In this study, the 5- and 10- year survival rate, respectively, are stated as a rolling average of three consecutive years (− 1-year-1+). The estimates of breast cancer survival, i.e. 5- and 10-years survival, are calculations of prognosis, based on the last 5 or 10 years, respectively. The clarification of breast cancer is the same for Sweden and Crete, and the methodological processing of data has been equivalent for both countries.
The coverage of the Swedish national cancer register is extremely high, approximately around 99%, and the survival estimates are even higher [24]. The Cretan breast cancer data used in this study derives from The Cancer Registry of Crete and had 98.5% completeness, 96.4% reliability, 100% timeliness and 99% continuity. The two studied populations of two corners of Europe should be studied in relation to corresponding local health care setting. In Table 1, descriptive characteristics of the breast cancer care system are illustrated.
Statistical analyses
We calculated mean ASIR and mean ASMR per 100.000 population. The calculations of p-values for the Swedish and the Cretan incidence and mortality data were based on aggregated data per 100.000 inhabitants, which means these calculations are approximations. P-values were overall estimated by z test one sample, since there was no information on population variance and the standard deviation was used in this model. Specifically, the z test one sample was performed to compare the ASIR, ASMR, 5- and 10-year survival rates within Sweden and Crete, respectively. For comparisons of the rates between the two countries, the z test two samples were used.
Results
In 2019, ASIR was 58.9 in Crete and 217.5 in Sweden, varying statistically significant between the two regions (p < 0.001). On the contrary, ASMR was 25.5 in Crete and 16.8 in Sweden (p = 0.04).
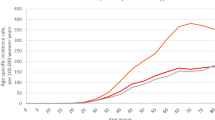
Over the last 15 years, the incidence rate of breast cancer in Sweden has successively tendered to rise from ASIR 158.1 in 2005 to 217.5 in 2019 (p = 0.12). The mortality rate, in turn, has shown a falling trend over the years, ASMR being 25.5 in 2005 and 16.8 in 2019 (p = 0.001). On Crete, ASIR is on a lower level in general compared to Sweden (p < 0.001), presented in Fig. 1, but similarly display a rising trend during the last 1.5 decade, with ASIR 55.3 in 2005 and 58.9 in 2019 (p = 0.002). The Cretan mortality rate, however, show a deviant pattern with a rising ASMR from 22.1 in 2005 to 25.3 in 2019 (p = 0.003) as seen in Fig. 2. Before 2007, Crete had an ASMR 22.1, while in Sweden the ASMR was 25.5 (p = 0.01). Nevertheless, after the year 2005, the Cretan mortality rates show a successively rising trend, while Swedish mortality rates have been descending.

ASIR for breast cancer and trends on Crete compared to Sweden over the last decades

ASMR for breast cancer and trends on Crete compared to Sweden over the last decades
As regards survival, increasing trends of survival rates has been seen in Sweden in contrast to decreasing trends on Crete, but this difference is not statistically significant (p = 0.98). Specifically, 5-year survival in Sweden from 1995 to 2019 ranged from 84.8 to 92.0% (p = 0.02), with a 5-year survival > 90% during the last decade, illustrated in Fig. 3. Conversely, 5-year survival in Crete, ranged from 86.4 to 85.1% during the same period. Regarding the 10-year survival rate, presented in Fig. 4, Swedish data ranged from 76.9% in 1995 to 87.1% in 2019 (p = 0.02). Over time, regional 10-year survival data in Crete ranged from 77.1 to 75.8% for the same period (p = 0.04).

5-year survival (%) for breast cancer and trends on Crete compared to Sweden during the decades around the millennium

10-year survival (%) for breast cancer and trends on Crete compared to Sweden during the decades around the millennium
Discussion
The main findings in this study show a rising breast cancer incidence in both Crete and Sweden, however, a paradox is that mortality rate in Crete has increased last decade, while in Sweden, breast cancer mortality decreased. This is a striking difference in the pattern of breast cancer burden for populations of these two regions on the European continent. Regarding survival rates, trends of survival in Sweden have increased over time in contrast to a lack of improvement - and even small decline - in survival on Crete since 1995.
The findings in this study must be seen against a multifactorial background where both health care systems as well as life-style factors and salutogenic factors might play important roles. Breast cancer mortality and survival are tightly related. It is generally stated, that one of the most important, modifiable, known parameters with influence on prognosis is early detection as a prerequisite for early, effective treatment with medical drugs and interventions that is already known to work [18].
In many European countries like the Scandinavian countries, Germany, Italy, Spain, Poland and others, there has been a marked reduction in the breast cancer mortality rates (between 8 and 19%) for the last years. This reduction has in general been attributed to earlier detection and improved treatment [11]. However, in Greece, a national mammography screening program has yet to be fully implemented [20]. There is yet no nationally formulated strategy for early detection of breast cancer in Greece.
Several factors are involved in the process leading to diagnosis, from the individuals own detection and insight at the debut of symptoms, to the availability and utilization of local health care. Mammographic screening on a population level is an established method to approach early detection of breastcancer before clinical symptoms occur [25]. In Sweden, 60% of all breast cancer cases are detected through the national screening program for women between 40 and 74 years of age [21, 26]. In countries with a tradition of mammography screening of breast cancer, an increase in incidence rates and a decrease in mortality rates have been evident for decades [27]. This may point to an increased incidence related to improved diagnostics but may also stem from risk of overdiagnostic. Nevertheless, potential overdiagnostic may complicate the interpretation of epidemiological health statistics. In a metaanalysis from 2012, the overdiagnostics was estimated to be 11% during lifetime for a woman invited to the screening program, and 19% during the specific time-period of inclusion in the screening program [28]. However, in many countries the incidence rise began before the mammography screening programs were implemented, also seen in countries who introduced screening programs relatively late [27]. In different populational settings, different challenges are distinguished related to features of the population [29]. The mammography screening of women, at least for the age-group 50-69 years, is one way to significantly reduce mortality rates of breast cancer [25], but mammography screening is also under an ongoing debate [30].
Another way into early diagnosis, is to make the diagnostical process per se more effective. In Sweden, a time-regulated, standardized, health care process is used when symptoms leading to high suspicion of breast cancer. Through this process, from the referral of the patient to a specialized oncological hospital unit, the individual has priority to required examinations and the time space between examinations and clinical consultations are strictly time-regulated [19].
The structure of the health care systems and the availability of health care differ between the studied regions, but there are also similarities, as illustrated in Table 1. In a time perspective, the Greek economy experienced a long period of recession during the period 2007-2015, with retrenchments in health care [31]. After the Greek recession, factors like quality of treatment as well as funding and access to health care have been stated a particular challenge of the society [32]. Interestingly, these years of economic recession overlaps the period of declination of the 10-year survival in Greece.
Sociocultural aspects with discrepancies in perceptions of health and disease may be factors of concern regarding general health literacy among the populations studied [17, 33]. In a study of Cretan women, several reasons for not using mammography were identified, like poor knowledge of the benefits of mammography screening, lack of physician recommendation, costs, embarrassment, fear of pain during the procedure and fear of a serious diagnosis [33]. Sociocultural aspects regarding doctor-patient relations and areas associated with high personal integrity, like the clinical investigations of the female breast, might play a role in patient-compliance. Communicative factors, such as language barriers, might also be factors of concern.
The strength of the study is that both the Swedish and Cretan data derives from solid and reliable registers. In Sweden, there is a historical tradition of registries with one of the world’s oldest cancer registries, started in 1958, with a national coverage [21]. The reporting of all new cancer cases is obligatory by law in Sweden, both from physician in charge as well as the responsible unit for pathological and cytological laboratory. In this way, the Swedish Cancer registry cover approximately around 99% of all cases and in 2015 an investigation showed that 100% of the reported cases were verified with cytology or histology, pointing to a valid and accurate measure [24]. National cancer registry is not yet available for the whole country of Greece, but for the region of Crete. The Cancer Registry of Crete has reached high numbers of data quality by following the European Network of Cancer Registries (ENCR) quality standards, which evaluate four dimensions (i.e., completeness, reliability, timeliness, and continuity). A limitation in this study is that the Greek data is only available from a specific region of the country, the island of Crete. The Swedish screening tool might introduce some bias. According to Swedish National Quality Registry of Breast Cancer (NKBC), every tumor of the breast found through screening is treated even if the knowledge is scarce about how the tumor would have developed with time if left untreated [27]. This perception may have influence on the incidence as well as the mortality data, possibly contributing to higher number of cases found, and consequently lower mortality rate in Sweden.
In conclusion, this study shows a contrasting pattern of breast cancer burden between two corners of the same European continent. Although the incidence is slowly rising in both regions, the mortality is increasing on Crete in contrast to Sweden where the mortality trend is decreasing. The findings further reveal a rising survival rate in Swedish breast cancer patients, while the survival trends on Crete are falling. An interpretation of these findings is that differences in health care systems and health policies as well as sociocultural factors between the two countries might play an important role on the outcome of breast cancer. The findings also indicate the need for a national breast cancer strategy in Greece, possibly with a national screening program and a streamlined, standardized course of investigation to improve early diagnostical processes and early treatment.
Availability of data and materials
The Swedish data is official and available at NORDCAN/WHO and the Swedish National Board of Health and Welfare. The Cretan datasets generated during and analyzed during the current study are not publicly available due to Greek official regulations but are available from the corresponding author on reasonable request.
References
Lima M, Kehm RD, Terry MB. Global breast cancer incidence and mortality trends by region, age-groups and fertility patterns. EClinicalMedicine. 2021;38:100985 Part of The Lancet Discovery Science.
IARC/The International Agency for Research on Cancer. WHO/World Health Organization. Available at: https://www.who.int/news/item/03-02-2021-breast-cancer-now-most-common-form-of-cancer-who-taking-action. Accessed 13 Mar 2021.
IARC/WHO fact sheet Breast Cancer. 2018. Available from: Latest global cancer data: cancer burden rises to 18.1 million new cases and 9.6 million cancer deaths in 2018. Available at: www.iarc.who.int/wp-content/uploads/2018/09/pr263_E.pdf. Accessed 27 Feb 2021.
Heer E, Harper A, Escandor N, Sung H, McCormack V, Fidler-Benaoudia MM. Global burden and trends in premenopausal and postmenopausal breast cancer: a population-based study. Lancet Glob Health. 2020;8(8):e1027–37.
Cancer in Sweden. Regionala Cancercentrum i Samverkan. Register data of prevalence and mortality during the years 1970-2017. 2020. p. 5. Available at: https://cancercentrum.se/globalassets/vara-uppdrag/statistik/cancer_i_sverige_registerdata_forekomst_dodlighet_1970-2017.pdf. Accessed 10 Sept 2021.
Sifaki-Pistolla D. Cancer Registry of Crete. Cancer data and statistics. Available from: https://gco.iarc.fr/today/data/factsheets/populations/300-greece-fact-sheets.pdf. Accessed 15 Dec 2021.
NCCN/National Comprehensive Cancer Network. Clinical practice guidelines in oncology. Stress management. Version 2.2021 – January 5, 2021. Available at https://www.nccn.org/patients/guidelines/cancers.aspx. Accessed 9 Sept 2021.
Henderson TO, Amsterdam A, Bhatia S. Systematic review: surveillance for breast cancer in women treated with chest radiation for childhood, adolescent, or young adult cancer. Ann Intern Med. 2010;152(7):444–55 W144-54.
Chang-Claude J. Inherited genetic susceptibility to breast cancer. Review. IARC Sci Publ. 2001;154:177–90.
Hinkula M, Pukkala E, Kyyronen P, Kauppila A. Grand multiparity and the risk of breast cancer: population-based study in Finland. Cancer Causes Control. 2001;12(6):491–500.
World Cancer Research Fund International. Breast-Cancer-Survivors-2014-Report.pdf Available at: wcrf.org. Accessed 29 Mar 2022.
Palesh O, Butler LD, Koopman C, Giese-Davis J, Carlson R, Spiegel D. Stress history and breast cancer recurrence. J Psychosom Res. 2007;63(3):233–9.
Koene RJ, Prizment AE, Blaes A, Konety SH. Shared risk factors in cardiovascular disease and cancer. Circulation. 2016;133(11):1104–14.
Moral R, Escrich E. Influence of olive oil and- its components on breast cancer: molecular mechanisms. Molecules. 2022;27(2):477.
Davidson K, Lionis C, Koutis A, et al. Differential cancer morbidity towards year 2000 in a population disease outlook across Europe. I. The female gender. Anticancer Res. 1997;17(1B):541–54.
Trigoni M, Mahoney MC, Moschandreas J, Tsiftsis D, Koumantakis E, Lionis C. Approaches to breast cancer screening among primary care physicians in rural areas of Crete, Greece. J Cancer Educ. 2011;26(3):490–6.
Koppner J, Chatziarzenis M, Faresjö T, et al. Stress and perceived health among primary care visitors in two corners of Europe: Scandinavia and Greece. Int J Health Geogr. 2020;19(1):55.
WHO. Essential Medicines List eEML - Electronic Essential Medicines List (essentialmeds.org) Date accessed for breast cancer December 2, 2021.
Streamlined standardized course of investigation. Breast cancer. Regional cancer centre in cooperation (In Swedish) Standardiserat vårdförlopp. Bröstcancer. Regionala cancercentrum i samverkan. 2019. Available at: svf-brostcancer.pdf. Accessed 29 Nov 2021.
Dimitrakaki C, Boulamatsis D, Mariolis A, Kontodimopoulos N, Niakas D, Tountas Y. Use of cancer screening services in Greece and associated social factors: results from the nation-wide Hellas Health I survey. Eur J Cancer Prev. 2009;18(3):248–57.
Swedish National Board of Health and Welfare. Cancer in numbers. 2018. Available at: (socialstyrelsen.se/en/) Page 16. IARC/NORDCAN. Available at: NORDCAN (iarc.fr). Accessed 9 Sept 2021.
Sifaki-Pistolla D. Towards developing evidence-based GIS-driven infrastructure for cancer surveillance in Greece. Eur J Pub Health. 2016;26(Supplement 1).
Chatzea VE, Sifaki-Pistolla D, Koinis F, et al. Cancer incidence and mortality trends in Crete, Greece during the last two decades (1992-2013): results from the cancer registry of Crete. Ann Oncol. 2017; Available at: www.crc.uoc.gr.
Eden M, Harrison S, Griffin M, et al. Impact of variation in cancer registration practice on observed international cancer survival differences between International Cancer Benchmarking Partnership (ICBP) jurisdictions. Cancer Epidemiol. 2019;58:184–92.
International Agency for Research on Cancer. IARC handbooks of cancer prevention, volume 15: breast cancer screening. Lyon: IARC; 2016. Accessed 27 Oct 2021
Nyström L, Andersson I, Bjurstam N, Frisell J, Nordenskjöld B, Lars Rutqvist E. Long-term effects of mammography screening: updated overview of the Swedish randomised trials. Review. Lancet. 2002;359(9310):909–19.
National Quality Registry of Breast Cancer. Regional cancer centre in cooperation (Regionala cancercentrum i samverkan): Nationellt vårdprogram Bröstcancer (NKBC); 2020. (In Swedish). Available at: https://statistik.incanet.se/brostcancer. Accessed 29 Nov 2021
Independent UK Panel on Breast Cancer Screening. The benefits and harms of breast cancer screening: an independent review. Review. Lancet. 2012;380(9855):1778–86.
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424.
Autier P, Boniol M. Mammography screening: a major issue in medicine. Eur J Cancer. 2018;90:34–62.
Tsiachristas A, Lionis C, Yfantopoulos J. Bridging knowledge to develop an action plan for integrated care for chronic disease in Greece. Int J Integr Care. 2015;15:e040.
Kyriopoulos I, Nikoloski Z, Mossialos E. Financial protection in health among the middle-aged and elderly: evidence from the Greek economic recession. Health Policy. 2021;125(9):1256–66.
Trigoni M, Griffiths F, Tsiftsis D, et al. Mammography screening: views from women and primary care physicians in Crete. BMC Womens Health. 2008;8:20.
Acknowledgements
The Swedish team would like to thank Niklas Toorell, data controller at the Swedish National Board of Health and Welfare, who delivered expertness regarding the Swedish national registries. The authors from the Cancer Registry of Crete would like to acknowledge and sincerely thank the multidisciplinary team and the registrars of the registry, who contributed to the data collection of the past decades, data classification and performance of quality controls. In addition, we appreciate the support of the Region of Crete and the Directors of each hospital department and death registry per municipality in Crete. Our memory at this time goes to Prof. John Vlachonicolis, one of the founders of the Cretan Cancer Registry. Unfortunately, Prof. Vlachonicolis passed away few years ago before seeing the progress of the registry that is clearly reflected in this paper.
Funding
Open access funding provided by Linköping University. No funding reported.
Author information
Authors and Affiliations
Contributions
All authors contributed to the discussion and interpretation of study results. M.R. made the study design and the Swedish ethical application, planned data collection procedures in the Swedish setting, carried out the Swedish data collection. D.S.P. contributed to the study design, planned data collection procedures in the Cretan setting, carried out the data analyses and contributed to the writing of the draft. A.S. contributed to the study design, supervised the data analyses, and revised the draft. G.V. contributed to the Cretan data collection. T.F. supervised the overall process of study design, the Swedish data collection and data analyses and revised the draft. Å.F. supervised the overall process of study design, the Swedish data collection and data analyses and revised the draft. C.L. supervised the overall process of study design, the Cretan data collection and data analyses and revised the draft. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All data from Sweden and Greece was retrieved from official national and regional statistical registers. For Swedish data, the study was approved by the Swedish Ethical Review Authority Dnr 2021-01202. For Cretan data, the Cancer Registry of Crete holds a license from the Hellenic Data Protection Authority (Protocol number: 960/11-08-2009) and has adopted the rules for collecting, managing, and processing sensitive and personal data. The subjects in the registers gave initially their informed consent to be included in the registers. The authors confirm that all methods were performed in accordance with the relevant guidelines and regulations. All authors approved the final version before submission and gave their consent for publication.
Consent for publication
Not applicable.
Competing interests
All authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Roginski, M., Sifaki-Pistolla, D., Stomby, A. et al. Paradoxes of breast cancer incidence and mortality in two corners of Europe. BMC Cancer 22, 1123 (2022). https://doi.org/10.1186/s12885-022-10243-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-022-10243-w