
Abstract
Background
Lung cancer is currently the most frequent cancer in Jiangsu Province, China, and the features of cancer distribution have changed continuously in the last decade. The aim of this study was to analyse the trend of the incidence of lung cancer in Jiangsu from 2009 to 2018 and predict the incidence from 2019 to 2030.
Methods
Data on lung cancer incidence in Jiangsu from 2009 to 2018 were retrieved from the Jiangsu Cancer Registry. The average annual percentage change (AAPC) was used to quantify the trend of the lung cancer age-standardized rate (ASR) using Joinpoint software. Bayesian age-period-cohort models were used to predict lung cancer incidence up to 2030.
Results
In Jiangsu, the lung cancer crude rate increased from 45.73 per 100,000 in 2009 to 69.93 per 100,000 in 2018. The lung cancer ASR increased from 29.03 per 100,000 to 34.22 per 100,000 during the same period (AAPC = 2.17%, 95% confidence interval [CI], 1.54%, 2.80%). Between 2019 and 2030, the lung cancer ASR is predicted to decrease slightly to 32.14 per 100,000 (95% highest density interval [HDI], 24.99, 40.22). Meanwhile, the ASR showed a downward trend in males and rural regions while remaining stable in females and urban regions.
Conclusion
We predict that the incidence of lung cancer in Jiangsu will decrease in the next 12 years, mainly due to the decrease in males and rural areas. Therefore, future lung cancer prevention and control efforts should be focused on females and urban regions.
Similar content being viewed by others
Introduction
Lung cancer is the leading type of cancer with the highest incidence and mortality in China and the world. It is estimated that more than 820,000 new lung cancer cases occurred in China in 2020 [1]. According to data from the Jiangsu Cancer Registry, in 2016, lung cancer was the malignant tumour with the highest incidence rate in Jiangsu Province, with ASR of 33.37/100,000, which was lower than the national average (36.46/100,000) [2, 3]. However, there is a lack of analysis and prediction on lung cancer in Jiangsu Province by sex and region. In a previous the Global Burden of Disease (GBD) study, tobacco smoking and industrially emitted ambient matter pollution were reported to be the leading risk factors for lung cancer [4]. Male smoking rates remain high in Jiangsu today; in contrast, the tobacco epidemic is less evolved and defined among females [5]. Derived from rapid growth and industrialization, air pollution is more severe in cities than in rural areas [6]. Therefore, it is important to analyse and predict lung cancer trends by sex and region.
Through mathematical models, past surveillance data can be used to predict the future cancer disease burden based on the assumption that recent incidence trends will continue to some extent in the future. In particular, Bayesian age-period-cohort models (BAPC models) have proven to be an effective tool for analysing and predicting trends of incidence [7,8,9]. The age effect accounts for the duration of exposure to risk variables. The period effect refers to circumstances that affect all persons at the same time, irrespective of age (e.g., short-term exposure, behaviour modification, therapeutic improvement). The cohort impact relates to a generational exposure [10, 11]. BAPC models are generally based on Poisson regression models, with the age effect considered as a row variable, the period effect as a column variable, and the cohort effect as the cross-effect of the age effect and the period effect, to construct a three-factor model of age, period and cohort and perform analysis and Markov chain Monte Carlo (MCMC) simulation [12, 13]. Given that, we intended to use BAPC modelling for the long-term prediction of incidence in this study.
Our study analysed and predicted the incidence of lung cancer through 2030 based on lung cancer data from Jiangsu Province from 2009 to 2018. The objectives of this study were (a) to provide an estimate of the burden of lung cancer in Jiangsu, China, using cancer registry data and (b) to provide detailed age-specific lung cancer incidence estimates through 2030.
Materials and methods
Source of the data
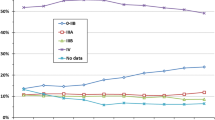
Cancer incidence data from 2009 to 2018 were obtained from the Jiangsu Cancer Registry, which is one of the largest population-based cancer registries in China. Incident cases of cancer were coded according to the International Classification of Diseases for Oncology, 3rd edition (ICD-O-3) [14] and the International Statistical Classification of Diseases 10th Revision (ICD-10) [15]. Lung cancer was defined as ICD-10 codes C34.0-C34.9. The detailed variables of each case were collected, including year and patient age at diagnosis, sex and region (rural or urban area). Age was divided into 18 subgroups, starting with 0–4 years, then 5–9 years and then in 5-year age groups up to 80–84 years, and finally 85 years or older. Based on the data-quality criteria of “Guideline for Chinese Cancer Registration” and International Agency for Research on Cancer/International Association of Cancer Registries (IARC/IACR), data quality of every cancer registry was assessed, including the validity, reliability, completeness and comparability [16]. The quality control indexes include the mortality to incidence ratio (M/I), the proportion of morphological verification (MV%), the percentage of cases identified with death certification only (DCO%) and the stability of cancer incidence. Qualified data from 16 continuous population-based cancer registries, providing a population coverage of about 17.36 million people, approximately 22.19% of the Jiangsu Province population were accepted for analysis. Seven of these registries are included in Cancer Incidence in Five Continents (CI5) Vol XI.
Statistical analysis
Quantifying the incidence trend of lung cancer
To synthetically evaluate average trends that include multiple intervals, the average annual percentage change (AAPC) was used to quantify the temporal trends of the age-standardized lung cancer incidence rate (ASR) in 2009–2018 and 2019–2030, which indicate the past trends and future trends, respectively. The ASR was calculated according to the direct method using the World Standard Population as proposed by Segi [17]. The AAPC was estimated by Joinpoint 4.9.0.1 [18]. A maximum number of 2 joinpoints were allowed for the ASR. A regression line was fitted to the natural logarithm of the rates, i.e., y = α + βx + ε, where y = ln (ASR) and x = calendar year, and the AAPC was calculated as 100 × (exp(β)-1) [19].
Bayesian age-period-cohort model
The temporal trends in age-adjusted incidence rates were modelled using the BAPC method. In the following, let i = 1…, I denote the index of the age group, j = 1…, J denote the index of the period, k = 1…, and K denote the index of the birth cohort. Given that age and period are measured on different scales (incidence data are given per year, but the age group covers 5 years), the cohort index is k = k (i, j) = 5*(I-i) + j. In classical APC literature, the APC model is often regarded as a log-linear Poisson model [20]. As an alternative, a binomial logit model can be formulated (both models are approximately identical): The counts of incidences yij in age group i in period j follow a binomial distribution with parameters pij and nij. Here, nij is the known population size of age group i at period j, and pij is the unknown incidence probability. The logit of the incidence probability is decomposed into an intercept µ, age effect θi, period effect φj and cohort effect ψk [20,21,22].
Random walk (RW) priors of different orders are used for the APC parameters age groups, periods and cohorts effect. The RW-1 prior assumes a constant trend over the time scale, whereas the RW-2 prior assumes a linear time trend [23, 24]. The results of the iterations were used to estimate the parameter values for age, period, and cohort effects based on different RW choices through Markov chain Monte Carlo (MCMC) method iterations.
This model was implemented using the Bayesian Age-Period-Cohort Modelling and Prediction package (BAMP v.1.3.0, Institute of Biomedical Engineering, Imperial College, London, UK) [25] of R version 4.0.3 (https://www.r-project.org/). Markov chain Monte Carlo simulations were run for 1,010,000 iterations with the initial 10,000 iterations used as burn-in to minimize the effect of initial values. The median iterative values and 95% confidence intervals (using 2.5% and 97.5% of the 1,000,000 iterated results, respectively) were obtained by the MCMC simulations in the models. The posterior deviance and predictive deviances of the model were used as a measure of the goodness of fit.
Result
Lung cancer incidence in Jiangsu, 2009–2018
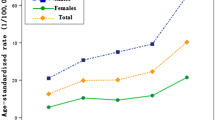
In Jiangsu, the lung cancer crude rate increased from 45.73 per 100,000 to 69.93 per 100,000, and the lung cancer ASR increased from 29.03 per 100,000 to 34.22 per 100,000 during the same period (AAPC = 2.17%, 95% CI, 1.54%, 2.80%) (Table 1). The ASR increased significantly among males (AAPC = 1.30%, 95% CI, 0.83%, 1.78%) and females (AAPC = 3.94%, 95% CI, 3.09%, 4.80%). In addition, the ASR increased significantly in urban (AAPC = 1.99%, 95% CI, 1.25%, 2.74%) and rural regions (AAPC = 2.30%, 95% CI, 1.68%, 2.92%).
Age-period-cohort analyses of the incidence in Jiangsu from 2009 to 2018
BAPC models were fitted to the overall age-specific incidence rates from 2009 to 2018. Table 2 shows the change in deviance in the sequential building of the models. The full three-factor model (age-period-cohort) was significantly better than the age-period (AP) and age-cohort (AC) models. The deviance information criterion (DIC) of the APC model was 38.79, indicating a good fit of the model compared with other submodels (143.40 for AC, 139.18 for AP). Accordingly, our subsequent estimations were based on the APC models.
Figure 1 shows the ASR of lung cancer according to age, period, and cohort effects. All observed rates were reported in 1-year periods and 5-year age groups (30 to 85 every 5 years, and 85 years and older; the age group under 30 years of age was excluded due to sparse cases). The incidence rates increased with age until 80 years in every period (Fig. 1 A). While the incidence rate remained low in the age group under 55 years and showed a stable trend with the period, it increased with the period among age groups above 55 years. The greatest increase was among those aged 80 years and older. (Fig. 1B). Cohort trends suggested that the cohort effects increased across age groups but decreased sharply within each period (Fig. 1 C, 1D).

Incidence of lung cancer per 100,000 by age, period and cohort effect (A: age trend by period; B: period trend by age; C: cohort trend by age; D: cohort trend by period)
Predicted lung cancer incidence in Jiangsu, 2019–2030
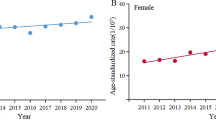
Considering the different distributions of lung cancer with respect to sex and region, we predicted the ASR stratified by sex and region with the use of the BAPC model. The predicted incidence rates from 2019 to 2030 are shown in Table 3 separately and by male and female populations and urban and rural regions. The ASR of lung cancer will decrease slightly to 32.14 per 100,000 (95% HDI, 24.99, 40.22) during this period (AAPC=-0.55%, 95% CI, -0.69%, -0.41%) (Table 3; Fig. 2). A downward trend is expected for both sexes, but it will be more pronounced in males (AAPC=-0.89%, 95% CI, -1.11%, -0.68%) than in females (AAPC=-0.02%, 95% CI, -0.28%, 0.24%) (Table 3; Fig. 3 A, 3B). Meanwhile, the incidence of lung cancer is expected to decrease in both urban and rural regions, but this trend is more pronounced in rural regions (AAPC=-1.72%, 95% CI, -2.17%, -1.26%) than in urban regions. (AAPC=-0.42%, 95% CI, -0.55%, -0.30%) (Table 3; Fig. 3 C, 3D).

Observed and predicted lung cancer incidence from 2009–2030 in Jiangsu (The open dots represent the observational values, and the blue dashed line denotes the 95% highest density interval of prediction values. The predictive mean value is shown as a black solid line. The vertical dashed line indicates where the prediction starts.)

Observed and predicted lung cancer incidence from 2009–2030 in both sexes and urban and rural areas of Jiangsu (A: males; B: females; C: urban; D: rural)
Discussion
In the current study, we analysed the temporal trends and a prediction of future trends in lung cancer incidence rates for the next decades in Jiangsu. Several messages can be derived from our study. By applying BAPC models, we found that the trends of incidence were mainly driven by ageing effects. The incidence rates of lung cancer have increased in the past decade; in contrast, they will show a downward trend in the next 12 years (2019–2030). The future downward trend will be consistent in males and in rural regions, while incidence rates will be stable in females and in urban regions.
The incidence of lung cancer was higher in males than in females in Jiangsu. This is consistent with the results of previous studies at the national and provincial levels [26, 27]. The reasons for the higher incidence in males are probably due to the different smoking rates between males and females: 44.0% of males and 1.6% of females smoked in Jiangsu in 2017 [5]. The duration of smoking should be considered the strongest determinant of lung cancer risk in smokers [28]. Previous studies have shown that occupational exposure is also a major risk factor for lung cancer [29, 30]. Due to their occupational choices, males are exposed to jobs with greater exposure to risk factors [31]. This may also lead to a higher incidence of lung cancer in males. However, the upward trend of lung cancer incidence was more pronounced in females than in males. Passive smoking and cooking smoke in the indoor environment may be responsible for the increased incidence in females [26, 32]. Furthermore, females have a higher risk of developing lung cancer than males when they are also smokers [33].
The incidence of lung cancer was higher in more developed regions than in less developed regions worldwide [1, 34]. However, our study showed that there was a higher incidence of lung cancer in rural regions than in urban regions. Moreover, the increase in lung cancer incidence in rural regions was also higher than that in urban regions. This may be related to the rising prevalence of smoking among rural men and an increase in their daily cigarette consumption [35]. In addition, the higher incidence in rural areas may be related to the differences in environment and lifestyle, such as urban-rural differences in solid fuel use and domestic water use [36, 37]. At the same time, atmospheric monitoring networks and management tools are becoming increasingly sophisticated in urban areas, while rural areas are relatively poorly equipped [38].
With BAPC models, we were able to identify the effects of age, period, and cohort on the outcome of cancer incidence, which is the first step in exploring the causal processes of the disease [25]. Age is often the main factor in BAPC analysis, as it accounts for consistent extrinsic factors, such as the accumulative exposure to factors [39]. The period effect accounts for all factors that affect every person during a time period in history, such as pollution or medical interventions [40]. The cohort effect accounts for events that affect generations, such as malnutrition of children during wars or changing habits [12, 41]. Our results show that the age effect on lung cancer incidence was seen mainly in the elderly population, which might be related to China’s ageing population [42]. In addition, the age effect is likely explained by age-related causes, such as accumulative exposures of the body to carcinogens over time and the accretion of mutations [43, 44]. The period effect may be related to the more severe air pollution and high smoking rate in China in recent years [45, 46]. Meanwhile, the cohort effect may be related to a higher level of education and awareness of disease prevention and control in the newer birth cohort [47].
The BAPC model provided very reliable and stable estimations for disease prediction [48,49,50]. Based on the assumption that past age, period, and cohort trends would continue, we made lung cancer projections for the next 12 years in Jiangsu Province. Our results show that the age-standardized incidence of lung cancer in Jiangsu will continue to decrease until 2030. This trend was maintained in men and rural areas, while it was not seen in women and urban areas. Although the disease burden of lung cancer in Jiangsu Province is lower than at the national level [51], it shows similar trends both at the national level and at the provincial level [7, 8, 52, 53]. This may be related to the more pronounced ageing population trends in women and more developed regions [54, 55], in addition to air pollution in urban areas, which also contributes to the high incidence of lung cancer [45, 56]. Additionally, in recent years, the biological basis of higher genetic susceptibility and oestrogen exposure in females has attracted the attention of researchers [57, 58].
The main risk factors for lung cancer include smoking, atmospheric pollution and occupational exposure [59, 60]. As China is currently the largest producer and consumer of tobacco, the government should introduce policies to limit and reduce smoking rates, such as increasing taxes on tobacco and banning smoking in public places [61]. Air pollution is also an issue that deserves attention, as air pollutants are now classified as major carcinogens [62]. According to the Report on the State of the Ecology and Environment in China 2020, 40.1% of cities in China failed to meet national air quality standards [38]. This requires the government to strengthen atmospheric control, encourage low-carbon travel and reduce carbon emissions. For occupational exposures, regular health check-ups, such as low-dose computed tomography scans, can provide better prevention of lung cancer.
To the best of our knowledge, we were able to predict the lung cancer incidence up to 2030, providing evidence for future policy-making. Several limitations should be noted before interpreting our results. First, underreporting and failure of diagnosis can occur in cancer registration, particularly in less developed areas, and therefore some of these lung cancer estimates may suffer from underestimation [63]. Secondly, these estimates of future incidence should not be overinterpreted, as they were based on the incidence data from only a short time period.
Conclusion
In summary, a consistent decrease is expected in the incidence of lung cancer during the next decades. The decrease in incidence will be more pronounced in males and rural regions but will be stable in females and urban regions. The results will be helpful in understanding the current situation of lung cancer in Jiangsu in depth and will provide essential information for health-related staff to monitor and control the disease.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AAPC:
-
average annual percentage change
- ASR:
-
age-standardized rate
- CI:
-
confidence interval
- HDI:
-
highest density interval
- BAPC:
-
Bayesian age-period-cohort
References
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209–49. doi:https://doi.org/10.3322/caac.21660.
Han Rq, Wu M, Miao W. Malignant tumor epidemiology in Jiangsu province,2016. Shiyong Zhongliuxue Zazhi (in Chinese). 2020;34(04):291–7.
Zheng R, Zhang S, Zeng H, Wang S, Sun K, Chen R, et al. Cancer incidence and mortality in China, 2016. J Natl Cancer Cent. 2022. doi:https://doi.org/10.1016/j.jncc.2022.02.002.
Global regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1923-94. doi: https://doi.org/10.1016/s0140-6736(18)32225-6.
He C, Qu C, Xu Y. Analysis of current smoking status and influencing factors in residents (≥ 15 years old) of Jiangsu Province. Zhongguo Manxingbing Yufang Yu Kongzhi (in Chinese). 2019;27(10):744–8.
Zhao S, Liu S, Hou X, Sun Y, Beazley R. Air pollution and cause-specific mortality: A comparative study of urban and rural areas in China. Chemosphere. 2021;262:127884. doi:https://doi.org/10.1016/j.chemosphere.2020.127884.
Liu Z, Jiang Y, Fang Q, Yuan H, Cai N, Suo C, et al. Future of cancer incidence in Shanghai, China: Predicting the burden upon the ageing population. Cancer Epidemiol. 2019;60:8–15. doi:https://doi.org/10.1016/j.canep.2019.03.004.
Lin X, Bloom MS, Du Z, Hao Y. Trends in disability-adjusted life years of lung cancer among women from 2004 to 2030 in Guangzhou, China: A population-based study. Cancer Epidemiol. 2019;63:101586. doi:https://doi.org/10.1016/j.canep.2019.101586.
Smittenaar CR, Petersen KA, Stewart K, Moitt N. Cancer incidence and mortality projections in the UK until 2035. Br J Cancer. 2016;115(9):1147–55. doi:https://doi.org/10.1038/bjc.2016.304.
Eilstein D, Uhry Z, Lim TA, Bloch J. Lung cancer mortality in France. Trend analysis and projection between 1975 and 2012, using a Bayesian age-period-cohort model. Lung Cancer. 2008;59(3):282–90. doi:https://doi.org/10.1016/j.lungcan.2007.10.012.
Chien CR, Chen TH. A Bayesian model for age, period, and cohort effects on mortality trends for lung cancer, in association with gender-specific incidence and case-fatality rates. J Thorac Oncol. 2009;4(2):167–71. doi:https://doi.org/10.1097/JTO.0b013e318194fabc.
O’Brien RM. Mixed models, linear dependency, and identification in age-period-cohort models. Stat Med. 2017;36(16):2590–600. doi:https://doi.org/10.1002/sim.7305.
Liu X, Zhou M, Wang F, Mubarik S, Wang Y, Meng R, et al. Secular Trend of Cancer Death and Incidence in 29 Cancer Groups in China, 1990–2017: A Joinpoint and Age-Period-Cohort Analysis. Cancer Manag Res. 2020;12:6221–38. doi:https://doi.org/10.2147/cmar.S247648.
Jack A, Percy C, Sobin L, Whelan S. International classification of diseases for oncology. ICD-O. World Health Organization; 2000.
Organization WH. International statistical classification of diseases and related health problems 10th version. https://icd.who.int/browse10/2019/en (2016). Accessed 18 March 2022.
Mohr SB, Garland CF, Gorham ED, Grant WB, Garland FC. Ultraviolet B irradiance and incidence rates of bladder cancer in 174 countries. Am J Prev Med. 2010;38(3):296–302. doi:https://doi.org/10.1016/j.amepre.2009.10.044.
Ahmad OB, Boschi-Pinto C, Lopez AD, Murray CJ, Inoue M. Age Standardization of Rates: A New WHO Standard. 2001.
Institute NC. Joinpoint Trend Analysis Software,Version 4.9.0.1 https://surveillance.cancer.gov/joinpoint/ (2022). Accessed 18 March 2022.
Gao S, Yang WS, Bray F, Va P, Zhang W, Gao J, et al. Declining rates of hepatocellular carcinoma in urban Shanghai: incidence trends in 1976–2005. Eur J Epidemiol. 2012;27(1):39–46. doi:https://doi.org/10.1007/s10654-011-9636-8.
Holford TR. The estimation of age, period and cohort effects for vital rates. Biometrics. 1983;39(2):311–24.
Jürgens V, Ess S, Cerny T, Vounatsou P. A Bayesian generalized age-period-cohort power model for cancer projections. Stat Med. 2014;33(26):4627–36. doi:https://doi.org/10.1002/sim.6248.
Knorr-Held L, Rainer E. Projections of lung cancer mortality in West Germany: a case study in Bayesian prediction. Biostatistics. 2001;2(1):109–29. doi:https://doi.org/10.1093/biostatistics/2.1.109.
Yao Y, Stephan KE. Markov chain Monte Carlo methods for hierarchical clustering of dynamic causal models. Hum Brain Mapp. 2021;42(10):2973–89. doi:https://doi.org/10.1002/hbm.25431.
Harrington SM, Wishingrad V, Thomson RC. Properties of Markov Chain Monte Carlo Performance across Many Empirical Alignments. Mol Biol Evol. 2021;38(4):1627–40. doi:https://doi.org/10.1093/molbev/msaa295.
Schmid V, Held L. Bayesian age-period-cohort modeling and prediction-BAMP. J Stat Softw. 2007;21. doi:https://doi.org/10.18637/jss.v021.i08.
Chen W, Xia C, Zheng R, Zhou M, Lin C, Zeng H, et al. Disparities by province, age, and sex in site-specific cancer burden attributable to 23 potentially modifiable risk factors in China: a comparative risk assessment. Lancet Glob Health. 2019;7(2):e257-e69. doi:https://doi.org/10.1016/s2214-109x(18)30488-1.
Cao W, Chen HD, Yu YW, Li N, Chen WQ. Changing profiles of cancer burden worldwide and in China: a secondary analysis of the global cancer statistics 2020. Chin Med J (Engl). 2021;134(7):783–91. doi:https://doi.org/10.1097/cm9.0000000000001474.
Doll R, Peto R, Boreham J, Sutherland I. Mortality in relation to smoking: 50 years’ observations on male British doctors. BMJ. 2004;328(7455):1519. doi:https://doi.org/10.1136/bmj.38142.554479.AE.
Consonni D, De Matteis S, Lubin JH, Wacholder S, Tucker M, Pesatori AC, et al. Lung cancer and occupation in a population-based case-control study. Am J Epidemiol. 2010;171(3):323–33. doi:https://doi.org/10.1093/aje/kwp391.
Poinen-Rughooputh S, Rughooputh MS, Guo Y, Rong Y, Chen W. Occupational exposure to silica dust and risk of lung cancer: an updated meta-analysis of epidemiological studies. BMC Public Health. 2016;16(1):1137. doi:https://doi.org/10.1186/s12889-016-3791-5.
De Matteis S, Consonni D, Lubin JH, Tucker M, Peters S, Vermeulen R, et al. Impact of occupational carcinogens on lung cancer risk in a general population. Int J Epidemiol. 2012;41(3):711–21. doi:https://doi.org/10.1093/ije/dys042.
Gordon SB, Bruce NG, Grigg J, Hibberd PL, Kurmi OP, Lam KB, et al. Respiratory risks from household air pollution in low and middle income countries. Lancet Respir Med. 2014;2(10):823–60. doi:https://doi.org/10.1016/s2213-2600(14)70168-7.
Stapelfeld C, Dammann C, Maser E. Sex-specificity in lung cancer risk. Int J Cancer. 2020;146(9):2376–82. doi:https://doi.org/10.1002/ijc.32716.
Wang N, Mengersen K, Tong S, Kimlin M, Zhou M, Hu W. Global, regional, and national burden of lung cancer and its attributable risk factors, 1990 to 2017. Cancer. 2020;126(18):4220–34. doi:https://doi.org/10.1002/cncr.33078.
Chen Z, Peto R, Zhou M, Iona A, Smith M, Yang L, et al. Contrasting male and female trends in tobacco-attributed mortality in China: evidence from successive nationwide prospective cohort studies. Lancet. 2015;386(10002):1447–56. doi:https://doi.org/10.1016/s0140-6736(15)00340-2.
Yu K, Qiu G, Chan KH, Lam KH, Kurmi OP, Bennett DA, et al. Association of Solid Fuel Use With Risk of Cardiovascular and All-Cause Mortality in Rural China. JAMA. 2018;319(13):1351–61. doi:https://doi.org/10.1001/jama.2018.2151.
Cheng Y, Nathanail CP. A study of “cancer villages” in Jiangsu Province of China. Environ Sci Pollut Res Int. 2019;26(2):1932–46. doi:https://doi.org/10.1007/s11356-018-3758-4.
Environment MoEa. Report on the State of the Ecology and Environment in China 2020. http://english.mee.gov.cn/Resources/Reports/soe/SOEE2019/202204/P020220407417638702591.pdf (2022). Accessed 10 July 2022.
Wong IO, Schooling CM, Cowling BJ, Leung GM. Breast cancer incidence and mortality in a transitioning Chinese population: current and future trends. Br J Cancer. 2015;112(1):167–70. doi:https://doi.org/10.1038/bjc.2014.532.
Nasreen S, Wilk P, Mullowney T, Karp I. Age, period, and cohort effects on asthma prevalence in Canadian adults, 1994–2011. Ann Epidemiol. 2020;41:49–55. doi:https://doi.org/10.1016/j.annepidem.2019.11.005.
Rutherford MJ, Lambert PC, Thompson JR. Age-period-cohort modeling. Stata J. 2010;10(4):606–27. doi:https://doi.org/10.1177/1536867x1101000405.
Lutz W, Sanderson W, Scherbov S. The coming acceleration of global population ageing. Nature. 2008;451(7179):716–9. doi:https://doi.org/10.1038/nature06516.
Peto R, Parish SE, Gray RG. There is no such thing as ageing, and cancer is not related to it. IARC Sci Publ. 1985(58):43–53.
Campisi J. d’Adda di Fagagna F. Cellular senescence: when bad things happen to good cells. Nat Rev Mol Cell Biol. 2007;8(9):729–40. doi:https://doi.org/10.1038/nrm2233.
Yin P, Brauer M, Cohen AJ, Wang H, Li J, Burnett RT, et al. The effect of air pollution on deaths, disease burden, and life expectancy across China and its provinces, 1990–2017: an analysis for the Global Burden of Disease Study 2017. Lancet Planet Health. 2020;4(9):e386-e98. doi:https://doi.org/10.1016/s2542-5196(20)30161-3.
Shi JF, Liu CC, Ren JS, Parascandola M, Zheng R, Tang W, et al. Economic burden of lung cancer attributable to smoking in China in 2015. Tob Control. 2020;29(2):191–9. doi:https://doi.org/10.1136/tobaccocontrol-2018-054767.
Rees PH. Education’s role in China’s demographic future. Proc Natl Acad Sci U S A. 2021;118(41). doi:https://doi.org/10.1073/pnas.2115618118.
Bray F, Møller B. Predicting the future burden of cancer. Nat Rev Cancer. 2006;6(1):63–74. doi:https://doi.org/10.1038/nrc1781.
Brennan P, Bray I. Recent trends and future directions for lung cancer mortality in Europe. Br J Cancer. 2002;87(1):43–8. doi:https://doi.org/10.1038/sj.bjc.6600352.
Du Z, Chen W, Xia Q, Shi O, Chen Q. Trends and projections of kidney cancer incidence at the global and national levels, 1990–2030: a Bayesian age-period-cohort modeling study. Biomark Res. 2020;8:16. doi:https://doi.org/10.1186/s40364-020-00195-3.
Zhou M, Wang H, Zeng X, Yin P, Zhu J, Chen W, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2019;394(10204):1145–58. doi:https://doi.org/10.1016/s0140-6736(19)30427-1.
Chen WQ, Zheng RS, Zeng HM. Bayesian age-period-cohort prediction of lung cancer incidence in China. Thorac Cancer. 2011;2(4):149–55. doi:https://doi.org/10.1111/j.1759-7714.2011.00062.x.
Du J, Sun H, Sun Y, Du J, Cao W, Sun S. Assessment of age, period, and cohort effects of lung cancer incidence in Hong Kong and projection up to 2030 based on changing demographics. Am J Cancer Res. 2021;11(12):5902–16.
Peng X. China’s demographic history and future challenges. Science. 2011;333(6042):581–7. doi:https://doi.org/10.1126/science.1209396.
United Nations Department of Economic and Social Affairs PD. World Population Ageing 2020 Highlights: Living arrangements of older persons. https://www.un.org/development/desa/pd (2020). Accessed 17 March 2022.
Wang N, Mengersen K, Tong S, Kimlin M, Zhou M, Wang L, et al. Short-term association between ambient air pollution and lung cancer mortality. Environ Res. 2019;179(Pt A):108748. doi:https://doi.org/10.1016/j.envres.2019.108748.
Schwartz AG, Ray RM, Cote ML, Abrams J, Sokol RJ, Hendrix SL, et al. Hormone Use, Reproductive History, and Risk of Lung Cancer: The Women’s Health Initiative Studies. J Thorac Oncol. 2015;10(7):1004–13. doi:https://doi.org/10.1097/jto.0000000000000558.
Alberg AJ, Wallace K, Silvestri GA, Brock MV. Invited commentary: the etiology of lung cancer in men compared with women. Am J Epidemiol. 2013;177(7):613–6. doi:https://doi.org/10.1093/aje/kws444.
Hamra GB, Guha N, Cohen A, Laden F, Raaschou-Nielsen O, Samet JM, et al. Outdoor particulate matter exposure and lung cancer: a systematic review and meta-analysis. Environ Health Perspect. 2014;122(9):906–11. doi:https://doi.org/10.1289/ehp/1408092.
Aredo JV, Luo SJ, Gardner RM, Sanyal N, Choi E, Hickey TP, et al. Tobacco Smoking and Risk of Second Primary Lung Cancer. J Thorac Oncol. 2021;16(6):968–79. doi:https://doi.org/10.1016/j.jtho.2021.02.024.
Guo H, Quan G. Tobacco control in China and the road to Healthy China 2030. Int J Tuberc Lung Dis. 2020;24(3):271–7. doi:https://doi.org/10.5588/ijtld.19.0106.
Guo Y, Zeng H, Zheng R, Li S, Pereira G, Liu Q, et al. The burden of lung cancer mortality attributable to fine particles in China. Sci Total Environ. 2017;579:1460–6. doi:https://doi.org/10.1016/j.scitotenv.2016.11.147.
Wei W, Zeng H, Zheng R, Zhang S, An L, Chen R, et al. Cancer registration in China and its role in cancer prevention and control. Lancet Oncol. 2020;21(7):e342-e9. doi:https://doi.org/10.1016/s1470-2045(20)30073-5.
Acknowledgements
We gratefully thank Dr. Changfa Xia for his valuable suggestion. This work was supported by National Key Research and Development Program of China (grands 2016YFC1302502).
Funding
This work was supported by National Key Research and Development Program of China (grands 2016YFC1302502).
Author information
Authors and Affiliations
Contributions
Study conception and design: JZ and YJ; Data collection: RH, HY and YJ; Data analyses: RH and YJ; Results interpretations: all authors; Manuscript drafting: YJ; Manuscript proofing: JZ, RH, JS and XF. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study used the data from Jiangsu Cancer Registry database. The study was approved by Ethic Committee of National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College. Written informed consent was waived by Ethics Committee of Jiangsu Provincial CDC due to retrospective study design.
Consent for publication
Not applicable.
Competing interests
The authors declared no potential conflicts of interest with respect to the research, author- ship, and/or publication of this article.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Jiang, Y., Han, R., Su, J. et al. Trends and predictions of lung cancer incidence in Jiangsu Province, China, 2009–2030: a bayesian age-period-cohort modelling study. BMC Cancer 22, 1110 (2022). https://doi.org/10.1186/s12885-022-10187-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-022-10187-1