
Abstract
Background
Epidermal growth factor receptor tyrosine kinase inhibitors (EGFR-TKIs) provide a better prognosis in EGFR-mutant non-small cell lung cancer (NSCLC). Nevertheless, the outcome of leptomeningeal metastasis (LM) remains poor. In addition, due to limited access to intracranial tumour tissue, gene alterations associated with leptomeningeal metastasis from lung adenocarcinoma (LM-LUAD) are unclear.
Methods
Forty-five patients with LM-LUAD from May 2019 to June 2021 in Guangdong Sanjiu Brain Hospital were enrolled in this study. Seventy-five percent (34/45) of patients with LM harbored EGFR mutations, and patients with progressive disease (PD) of LM had 3rd-generation EGFR-TKI therapy and were defined as Cohort 1; those without 3rd-generation EGFR-TKI therapy were defined as Cohort 2. Next-generation targeted panel sequencing (NGS) was performed in each cerebrospinal fluid (CSF) sample of the two cohorts, and 9/45 LM-LUAD patients had matched plasma (PLA).
Results
The common gene alterations discovered in the CSF of LM-LUAD were EGFR mutation (34/45, 75%), TP53 (25/45, 56%), CDKN2A (9/45, 20%), ALK (7/45, 16%), CTNNB1 (6/45, 13%), MET (5/45, 11%), APC (4/45, 9%), FGF4 (4/45, 9%), FGF3 (4/45, 9%), ERBB2 (4/45, 9%), and PIK3CG (4/45, 9%). Cooccurring mutations of TP53 and EGFR were found in 49% (22/45) of patients and correlated with poor prognosis. CDKN2A was identified in 20% (9/45) of patients and presented slightly shorter overall survival (OS) than those without (7.1 versus 8.8 months, p = 0.2). Cohort 1 had more genes associated with poor prognosis, consisting of CDK4, CDKN2A, PIK3CG, or PIK3CA, and YES1 and MET were more likely to be detected in cohort 2. The alteration of EGFR was comparable between CSF and matched PLA. Incidences of gene alterations such as CDK4, CDKN2A, MET, SOX2, JAK2, BRAF, and PIK3CG were more likely to be identified in CSF. All mutant allele frequencies (MAF) were much higher in CSF than in matched PLA.
Conclusions
CSF could be a potential candidate for the genetic profiling of LM-LUAD, demonstrating the genetic characteristics of LM in EGFR-mutated lung adenocarcinoma on diverse EGFR-TKI therapies.
Similar content being viewed by others

Introduction
Lung cancer is one of the leading causes of cancer-related death [1]. The discovery of oncogenic genes, such as epidermal growth factor receptor (EGFR), anaplastic lymphoma kinase (ALK), and ROS1, has changed the therapeutic approach for selected non-small cell lung cancer (NSCLC). Epidermal growth factor receptor tyrosine kinase inhibitors (EGFR TKIs) are effective in treating patients whose tumours harbor sensitive EGFR mutations. However, the response rate varies among those people. Leptomeningeal metastasis (LM) is still a significant risk factor, and approximately 10% of advanced NSCLC patients with EGFR mutations are diagnosed with LM [2]. LM is a detrimental complication of NSCLC and is related to poor prognosis [3]. Although somatic genetic modification has been firmly established, the potential genetic alteration that accounts for the development of intracranial metastasis is still unclear. Additional efforts have revealed that cerebrospinal fluid (CSF) is close to intracranial metastasis and is more representative of brain lesions than plasma (PLA) for detecting relevant mutations [4], which makes CSF an alternative option to trace the evolution of the tumour genome. Next-generation targeted panel sequencing (NGS) panels could detect variants in multiple relevant genes and reveal the changes in percentage mutant allele frequency (MAF) with sufficient CSF samples, which could shed light on the unknown driver gene.
Methods
Patient characteristics
We retrospectively screened 200 consecutive patients diagnosed with lung adenocarcinoma at Guangdong Sanjiu Brain Hospital from May 2019 to June 2021. Among these patients, forty-five patients diagnosed with LM who underwent NGS based on CSF were ultimately included in the present study. LM was diagnosed based on typical central nervous system symptoms, i.e., headache, dizziness, etc., combined with either tumour cells identified in CSF samples or positive results in brain magnetic resonance imaging (MRI). All CSF samples were obtained through lumbar puncture with approximately 10 mL CSF collected for NGS testing. Among these 45 patients, nine also had paired PLA, and 8 ml plasma was collected for NGS simultaneously.
All patients signed informed consent, and the research protocol was approved by the Research Ethics Committee of Guangdong Three Nine Brain Hospital.
Library material
Cell-free DNA (cfDNA) from CSF and whole blood was extracted using the QIAamp DNA FFPE Tissue Kit (Qiagen) according to the manufacturer’s protocol. Next-generation target sequencing of CSF was mainly performed using the 168-gene panel. The preparation of cfDNA in CSF and the NGS sequencing library were fully described in previous research [5]. NGS samples were prepared according to a standard protocol, and sequencing data were mapped to the human genome.
Statistical analyses
Patient demographic information was reported using descriptive statistics, and Fisher’s exact test was used to analyse categorical variables. Overall survival (OS) curves were calculated using the Kaplan–Meier method from the diagnosis of leptomeningeal metastases to death or the last follow-up date. Hazard ratios were calculated with the use of a Cox proportional hazard model. P < 0.05 was deemed statistically significant. Statistical analyses and curves were generated with SPSS 21 and GraphPad Prism 6 software.
Results
Clinical characteristics of patients with LM-LUAD
The median age was 53 (range from 30 to 73 years), and 55.6% (25/45) of the patients were female in this study. In addition, 2% (1/45) of the patients had wild-type, 7% (3/45) patients had ROS1 fusions, and 16% (7/45) of patients had ALK fusions. The majority of patients in this study harbored EGFR mutations, accounting for 75% (34/45) (Table 1).
Gene landscape of 45 CSFs from LM-LUAD
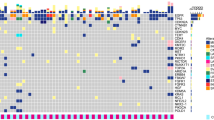
Here, we performed NGS on 45 CSF specimens from LM-LUAD to characterize the genomic mutation during the development of LM, and a handful of genetic profiles of CSF cfDNA were present (Fig. 1).

Gene landscape of 45 CSFs from LM-LUAD. Oncoprint of the multiple genetic alterations from the 45 cases is shown. The three top bars indicate the number of mutations, age, and MAF in each patient. The left side-bar presents names of the detected genes in CSF, and the right side-bar demonstrates the number of specific mutations in patients. Colour keys represent the variant type of the relative gene. MAF mutant allele frequency. CSF: cerebrospinal fluid
EGFR and TP53 are the two most frequently mutated genes in CSF samples. The most frequent mutation of EGFR demonstrated that EGFR-L858R, EGFR-19Del, EGFR-20ins, and EGFR-L861Q were 49, 20, 2, and 4%, respectively. TP53 was detected in 25 (25/45, 56%) patients, and coexisting TP53 and EGFR were found in 22 (22/45, 49%). CDKN2A was the most frequent copy number variation (CNV); copy number deletion was detected in 7 patients, copy number deletion together with gene fusion in 1 patient, and frameshift variant identified in 1 patient. CDK4 copy number gain was recognized in 8 patients (8/45, 18%), and MET copy number variation was captured in 5 patients (5/45, 11%). In addition, ERBB2, PIK3CG, and PMS2 copy number variations were identified in 4 patients, and JAK2 copy number variations were detected in three patients. Other potential metastasis genes were also captured in CSF cfDNA, including YES1, CDK6, PIK3CA, BRAF, and ROS1, which were seen in 3 patients, and PTPRD, MSH2, FGFR1, and SMAD4, which were captured in 2 patients.
OS associated with the presence or absence of related genes
Coexisting TP53/EGFR showed shorter OS than the opposing group (6.9 versus 10.3 months, p = 0.04) (Fig. 2A). In our findings, the second most common coexisting gene mutation identified was ALK fusions together with TP53, which was discovered in 2/45 (4.4%) patients who had an OS and progression-free survival (PFS) of 2 and 7.5 months on crizotinib, respectively. Taking the limited number into consideration, there was no comparison of OS benefit results in our study. CDKN2A was identified in 9/45 (20%) patients in our research. Accumulate evidence demonstrated that CDKN2A is common in cerebrospinal fluid (CSF) samples of lung adenocarcinoma patients with central nervous system (CNS) metastases, and concurrent CDKN2A with EGFR-sensitive mutations indicated inferior median intracranial PFS (iPFS). However, in our research, this known genetic alteration was not correlated with a worse prognosis compared to those without such an alteration (Fig. 2B).

OS associated with the presence or absence of related genes. Kaplan–Meier curves of patients with or without relative genes. A, with or without co-mutation of EGFR and TP53. B, presence or absence of CDKN2A. OS was defined as the time from diagnosis of leptomeningeal metastasis to death or the last follow-up time. p values were calculated using a two-sided log-rank test. Hazard ratios were calculated with the use of a Cox proportional hazard model. EGFR denotes epidermal growth factor receptor. TP53 denotes the tumour protein P53. OS overall survival. CI confidence interval. HR hazard ratio
Specific genetic signatures of the two subgroups
The top 10 genes varied among the different cohorts (Fig. 3, Table 2).

Bar charts show the distribution of the top 10 genes detected in each CSF sample in the 2 cohorts. A Cohort 1, PD of LM with 3rd generation EGFR-TKI therapy. B Cohort 2, PD to LM without 3rd generation EGFR-TKI therapy
TP53 was the most frequent alteration among the two subgroups, with detection rates of 62% (16/26) and 62.5% (5/8) in cohorts 1 and 2, respectively. EGFR amplification was the common gene in those two cohorts, with detection rates of 23% (6/26) in cohort 1 and 50% (4/8) in cohort 2. Unlike the discovered genes in cohort 1, MET, YES1, and FGF3/FGF4 copy number amplification were more likely present in cohort 2, which indicated the different pathways involved in the progressive disease of LM on various EGFR-TKI treatments. EGFR mutation (EGFRm) T790M was identified in 15% (4/26) of patients in cohort 1 and was not detected in cohort 2.
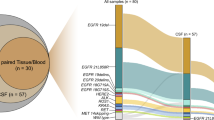
Concordance of EGFR-activating mutations in CSF samples with matched PLA
Our study demonstrated that sensitive somatic mutations, including EGFR-L858R and EGFR-19Del, are parallel to each other between CSF and matched PLA. In addition, the more frequent resistance gene TP53 was found 4 (4/9, 44%) in CSF cfDNA, much higher than that in PLA (2/9, 22%). Moreover, CDK4 (17%), CDKN2A (11%), MET, SOX2, TERT, BRAF, and PIK3CG (which have the same 6%) were detected exclusively in CSF (Fig. 4).

Concordance of EGFR-activating mutations in CSF samples with matched PLA. Oncoprint of the multiple genetic alterations from the 9 matched CSF-PLA cases are shown. The three top bars indicate the number of mutations, age, and MAF in matched samples. The left side-bar presents names of the detected genes in matched CSF-PLA pairs, and the right side-bar demonstrates the number of specific mutations in patients. Colour keys represent the variant type of the relative gene. MAF: mutant allele frequency. CSF: cerebrospinal fluid. PLA plasma
The number of variant genes was more multiple in CSF than in matched PLA samples (Fig. 5A). Most importantly, all the MAFs in CSF cfDNA samples were significantly higher than those in plasma, the average MAFs of CSF cfDNA and plasma were 52.09 and 0.44%, respectively, and there was a statistically significant difference (p < 0.01) (Fig. 5B).

The amounts of variant genes and MAFs in matched CSF-PLA samples. A Difference in the amounts of variant genes detected in CSF and matched PLA. B MAF in CSF cfDNA and matched samples were analysed by Fisher’s exact test. P < 0.05 was deemed statistically significant. MAF: mutant allele frequency. CSF: cerebrospinal fluid. PLA plasma
Discussion
The expression of EGFR components is frequent in LUAD and makes EGFR an attractive anticancer target. Patients who share EGFR mutations could benefit from EGFR-TKIs and show a markedly better prognosis, but LM is still a devastating complication showing a dismal prognosis. Although significant projects are underway to create a comprehensive map of all the responsible genes involved in the evolution and dissemination of intracranial cancer, the driver genes in intracranial tumours remain unclear. NGS panels can detect variants in multiple relevant genes [6, 7], which provides a sufficient method to characterize resistance mechanisms. In our study, NGS was utilized in 45 CSF samples and revealed the genetic landscape of LM-LUAD. Primary sensitive mutations of EGFR-L858R or EGFR-Del19 were present in 31 (69%) patients, T790M was detected in 4 (9%) patients, TP53 was present in 25 (56%) patients, and coexisting TP53 and EGFR were found in 22 (49%) CSF specimens. TP53 mutation is considered a poor prognostic factor, and cooccurring TP53/EGFR could affect the efficacy of EGFR-TKI in LUAD, leading to resistance to EGFR-TKI therapy and thus reducing OS [8, 9]. In our research, the subgroup with coexisting TP53/EGFR showed shorter OS than the opposing group (p = 0.04). This result was in agreement with the previous literature [8, 10], which reported that the concurrent is associated with poor outcomes. Molecular-level demonstrated that [11] TP53 co-mutations are relatively frequent in these selected patients and exhibit this concurrent is associated with adverse outcome of crizotinib, showing significantly shorter progression-free survival (PFS) [8]. In our findings, the second most common coexisting gene mutation identified was ALK fusion together with TP53, which was discovered in 2/45 (4.4%) patients who had an OS and PFS of 2 and 7.5 months on crizotinib, respectively. Taking the limited number into consideration, there was no comparison of OS benefit results in our study.
The expression of CDKN2A correlated with poor prognosis and reduced patient survival [6, 12], and CDKN2A was identified in 9/45 (20%) patients in our research. However, this known genetic alteration is not correlated with a worse prognosis of patients with such an alternation (p = 0.2). Genetic heterogeneity among different anatomical regions and even in single cancer samples [11] may have led to the other results shown in our study. Extensive research is still needed to further elucidate this alternation. Gene signatures of CDK4, PIK3CG, or PIK3CA mutations were associated with poor survival [11, 13]; in our research, CDK4 was identified in 8 (18%) patients, and PIK3CG was identified in 4 (9%) patients.
Further cohort analysis of EGFR mutation LM-LUAD patients identified the top 10 genes presented in each subgroup. Gene signatures consisting of CDK4, CDKN2A, PIK3CG, or PIK3CA mutations were more frequently identified in cohort 1, and all these genes are associated with poor survival [11, 13]. Unlike the genes discovered in cohort 1, MET, YES1, and FGF3/FGF4 copy number amplifications were more likely present in cohort 2. In the context that the genomic features of tumours will guide therapeutic approaches, unique genomic alternation will be fundamental to the correct molecular diagnosis and treatment. Considering the findings in cohort one, it follows that targeting the CDK4, PIK3CG, or PIK3CA signalling pathways may help treat leptomeningeal metastases.
EGFR mutation (EGFRm) T790M was identified in 15% of patients in cohort one, which is much lower than the most common cause of acquired resistance of patients receiving EGFR-TKI treatment. An underlying reason might be that extracranial T790M status is not representative of intracranial conditions. The previous findings that T790M has a lower frequency intracranially further supported this assumption [5]. Shang et al. reported that in addition to the T790M mutation, EGFR amplification is another acquired drug resistance mechanism to icotinib/gefitinib [14]. EGFR amplification was detected at 23% (6/26) in cohort 1 and 50% (4/8) in cohort two, which partly accounted for the progressive disease of LM.
In this study, we characterized the genomic alteration of cfDNA in the CSF of LM-LUAD and compared it to matched PLA samples. We demonstrated that sensitive somatic mutations, including EGFR-L858R and EGFR-19Del, are parallel between CSF and matched PLA. Moreover, CDK4, CDKN2A, MET, SOX2, TERT, BRAF, and PIK3CG were detected exclusively in CSF, which will provide potentially clinically informative alterations for intracranial lesions. Importantly, we demonstrated that CSF cfDNA has a significantly higher MAF than plasma for CNS oncogenic alterations. This result is consistent with previous research showing that CSF demonstrates the relevant modifications of the gene in intracranial tumours and should be recommended as liquid biopsies to assess the evolution of CNS tumours [15]. However, due to the limited sample size in our study, research on larger sample sizes is still needed to distinguish our results from the background of random mutation.
It is known that [16, 17] brain metastasis samples share mutations that differ from the primary tumour, suggesting that intracranial metastasis lesions are more similar to one another than to the extracranial samples and suggesting that conferring CSF is a potential approach to detect lesions in the brain. The findings in our study suggest potential genomic alterations present in leptomeninges metastases. They may shed light on the divergence of therapeutic response in some cases, helping to select the optimal treatment dictated by the molecular characteristics of brain cancer.
Altogether, we identified gene alterations that may contribute to the metastatic process of leptomeningeal, and the analysis of CSF cfDNA should be another strategy to monitor intracranial tumour evolution when tissue is scant.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–49.
Li YS, Jiang BY, Yang JJ, Tu HY, Zhou Q, Guo WB, et al. Leptomeningeal metastases in patients with NSCLC with EGFR mutations. J Thorac Oncol. 2016;11(11):1962–9.
Cagney DN, Martin AM, Catalano PJ, Redig AJ, Lin NU, Lee EQ, et al. Incidence and prognosis of patients with brain metastases at diagnosis of systemic malignancy: a population-based study. Neuro-Oncology. 2017;19(11):1511–21.
Villatoro S, Mayo-de-Las-Casas C, Jordana-Ariza N, Viteri-Ramirez S, Garzon-Ibanez M, Moya-Horno I, et al. Prospective detection of mutations in cerebrospinal fluid, pleural effusion, and ascites of advanced cancer patients to guide treatment decisions. Mol Oncol. 2019;13(12):2633–45.
Li YS, Jiang BY, Yang JJ, Zhang XC, Zhang Z, Ye JY, et al. Unique genetic profiles from cerebrospinal fluid cell-free DNA in leptomeningeal metastases of EGFR-mutant non-small-cell lung cancer: a new medium of liquid biopsy. Ann Oncol. 2018;29(4):945–52.
Li YS, Zheng MM, Jiang BY, Tu HY, Yang JJ, Zhang XC, et al. Association of Cerebrospinal Fluid Tumor DNA genotyping with survival among patients with lung adenocarcinoma and central nervous system metastases. JAMA Netw Open. 2020;3(8):e209077.
Fan Y, Zhu X, Xu Y, Lu X, Xu Y, Wang M, et al. Cell-cycle and DNA-damage response pathway is involved in leptomeningeal metastasis of non-small cell lung Cancer. Clin Cancer Res. 2018;24(1):209–16.
Wang F, Zhao N, Gao G, Deng HB, Wang ZH, Deng LL, et al. Prognostic value of TP53 co-mutation status combined with EGFR mutation in patients with lung adenocarcinoma. J Cancer Res Clin Oncol. 2020;146(11):2851–9.
VanderLaan PA, Rangachari D, Mockus SM, Spotlow V, Reddi HV, Malcolm J, et al. Mutations in TP53, PIK3CA, PTEN and other genes in EGFR mutated lung cancers: correlation with clinical outcomes. Lung Cancer. 2017;106:17–21.
O'Kane GM, Liu G, Stockley TL, Shabir M, Zhang T, Law JH, et al. The presence and variant allele fraction of EGFR mutations in ctDNA and development of resistance. Lung Cancer. 2019;131:86–9.
Brastianos PK, Carter SL, Santagata S, Cahill DP, Taylor-Weiner A, Jones RT, et al. Genomic characterization of brain metastases reveals branched evolution and potential therapeutic targets. Cancer Discov. 2015;5(11):1164–77.
Zheng MM, Li YS, Tu HY, Jiang BY, Yang JJ, Zhou Q, et al. Genotyping of cerebrospinal fluid associated with Osimertinib response and resistance for leptomeningeal metastases in EGFR-mutated NSCLC. J Thorac Oncol. 2021;16(2):250–8.
Qian J, Zhao S, Zou Y, Rahman SMJ, Senosain MF, Stricker T, et al. Genomic underpinnings of tumor behavior in in situ and early lung adenocarcinoma. Am J Respir Crit Care Med. 2020;201(6):697–706.
Shang Y, Li X, Liu W, Shi X, Yuan S, Huo R, et al. Comprehensive genomic profile of Chinese lung cancer patients and mutation characteristics of individuals resistant to icotinib/gefitinib. Sci Rep. 2020;10(1):20243.
Pentsova EI, Shah RH, Tang J, Boire A, You D, Briggs S, et al. Evaluating Cancer of the central nervous system through next-generation sequencing of cerebrospinal fluid. J Clin Oncol. 2016;34(20):2404–15.
Shih DJH, Nayyar N, Bihun I, Dagogo-Jack I, Gill CM, Aquilanti E, et al. Genomic characterization of human brain metastases identifies drivers of metastatic lung adenocarcinoma. Nat Genet. 2020;52(4):371–7.
Saunus JM, Quinn MC, Patch AM, Pearson JV, Bailey PJ, Nones K, et al. Integrated genomic and transcriptomic analysis of human brain metastases identifies alterations of potential clinical significance. J Pathol. 2015;237(3):363–78.
Acknowledgements
Not applicable.
Funding
This work was supported by the Natural Science Foundation of Guangdong Province (No. 2019A1515011943), National Natural Science Foundation of China (No. 81871865), Shanghai Science and Technology Committee Foundation (NO. 19411950300), and China Postdoctoral Science Foundation (No. 2019 M662974). The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
Hainan Yang, Lei Wen, and Yingying Pan. designed the experiments and wrote the manuscript. Changguo Shan, Weiping Hong. helped in reviewing, acquisition, analysis and interpretation of clinical data for the work. Hui Wang, Cheng Zhou. did the statistical analysis. Linbo Cai, Caicun Zhou. revised critically the manuscript for important intellectual content. All authors have read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Guangdong Sanjiu Brain Hospital. We informed the participants about the study and obtained informed consent from each patient.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yang, H., Wen, L., Pan, Y. et al. Gene alternation of cerebrospinal fluid in patients with leptomeningeal metastases of lung adenocarcinoma using next-generation sequencing. BMC Cancer 22, 580 (2022). https://doi.org/10.1186/s12885-022-09597-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-022-09597-y