
Abstract
Background
The skeletal muscle index (SMI), which is calculated as the ratio of skeletal muscle area at the third lumbar vertebral level divided by height squared, has been considered a prognostic factor in patients with breast cancer. However, the prognostic impact of changes in SMI during treatment remains unclear. This study aimed to evaluate the influence of SMI changes in patients with breast cancer undergoing neoadjuvant chemotherapy (NAC).
Methods
We reviewed patients with breast cancer who underwent NAC and subsequent surgery for breast cancer between 2010 and 2017. The rate of SMI change during NAC was calculated, and the association between SMI changes and prognosis was retrospectively analyzed.
Results
In total, 141 patients were evaluated. 48 (34.0%), 53 (37.6%), and 40 (28.4%) patients exhibited increased (≥ 3%), maintained (− 3% <, < 3%), and decreased (− 3% ≥) SMI during NAC, respectively. The decreased SMI group showed significantly poorer disease-free survival than the maintained and increased SMI groups (hazard ratio [HR] 8.29, p < 0.001 for the decreased vs. increased SMI groups; HR 3.49, p < 0.001 for the decreased vs. maintained SMI groups). Moreover, decreased SMI was an independent risk factor for disease-free survival in multivariate analysis (HR 3.68, p < 0.01).
Conclusions
Skeletal muscle loss during NAC predicts poor prognosis. Our results underscore the importance of monitoring and maintaining skeletal muscle mass during NAC.
Similar content being viewed by others

Background
Neoadjuvant chemotherapy (NAC) has become a standard treatment option for patients with locally advanced but operable breast cancer [1]. NAC can downstage a primary tumor and axillary lymph nodes, which enables us to perform breast-conserving surgery in patients who might need a mastectomy at initial diagnosis. Furthermore, different from adjuvant chemotherapy, NAC also offers important clinical information, including response to chemotherapeutic agents and pathological complete response (pCR) rate, which has been demonstrated to be a prognostic marker in human epidermal growth factor receptor type 2 (HER2)-positive or triple-negative (TN) breast cancer [2]. In addition, NAC allows the evaluation of dynamic changes in the systemic conditions of patients who have a primary tumor during treatment. We previously demonstrated that a decrease in the prognostic nutritional index (PNI), which represents systemic nutritional and immunological status, during NAC had a prognostic impact in patients with breast cancer [3]. Hence, NAC may have the potential to provide other prognostic markers with respect to changes in patients’ status during treatment.
The influence of body weight and composition on patient outcomes has been a focus in the field of breast cancer studies. Previous studies have indicated that high body mass index (BMI) was associated with poor prognosis in patients with breast cancer [4, 5]. Conversely, some studies have shown no correlation between BMI and patient outcomes in breast cancer [3, 6]. This uncertainty underlying the influence of BMI is possibly, at least in part, because of the fact that BMI cannot account for the difference between adipose tissue and muscles and thus cannot evaluate the exact body composition. Certainly, the proportions of visceral fat, subcutaneous fat, and skeletal muscle vary significantly between individuals with the same BMI [7]. Thus, there is an unmet need for more accurate markers for estimating body composition, and skeletal mass volume was established as one of the markers for this [8].
Sarcopenia, defined as a condition with loss of muscle mass in older adults [9], is correlated with poor survival in various solid malignancies, including breast cancer [8, 10,11,12,13,14,15,16]. In addition to the importance of sarcopenia at the beginning of cancer treatment, skeletal muscle loss during palliative chemotherapy has recently been shown to be associated with reduced survival in patients with gastrointestinal cancer [17,18,19,20,21,22]. However, there is currently limited knowledge of changes in muscle mass during NAC and their impact on prognosis in patients with breast cancer. Generally, breast cancer is more likely to occur in younger patients than other types of cancer, such as lung, gastric, and colorectal cancers [23]. Furthermore, unlike patients undergoing palliative chemotherapy for other types of cancer, those treated with NAC for breast cancer have early-stage cancer. Hence, patients with breast cancer undergoing NAC are not likely to be sarcopenic at diagnosis [3]. Accordingly, it is possible that the effect of skeletal muscle index (SMI) changes in patients with breast cancer undergoing NAC is not equivalent to that in patients with other types of cancer undergoing palliative chemotherapy.
This study aimed to investigate the prognostic impact of changes in skeletal muscle mass during NAC in patients with breast cancer. To this end, we evaluated the changes in SMI during NAC in patients and investigated their association with patient outcomes.
Methods
Patients and study design
This retrospective study assessed patients with breast cancer with a performance status (Eastern Cooperative Oncology Group performance status [24]) of 0 who underwent NAC and subsequent surgery at Shinshu University Hospital between February 2010 and December 2017. The inclusion criteria were as follows: (1) patients who had pathologically confirmed breast cancer by core needle biopsy and (2) those who underwent computed tomography (CT) or 18F-fluorodeoxyglucose positron emission tomography/CT (18F-FDG-PET/CT) within both 4 weeks of initiation of NAC and surgery following NAC. Patients who could not complete NAC owing to chemotoxicity or disease progression during NAC (n = 14) were excluded. A total of 141 patients were included in this study. This study conformed to the provisions of the Declaration of Helsinki (64th WMA General Assembly, Fortaleza, Brazil, October 2013). The study was approved by the local ethics committee on the clinical investigation of Shinshu University (no. 5037). Because this was a retrospective study of anonymized data, the need for informed consent was waived.
Data collection
Clinical information, including age, height, body weight, sex, menopausal status, clinical stage at diagnosis, histological type, histological grade (HG), estrogen receptor (ER) status, progesterone receptor (PgR) status, HER2 status, lymph node metastasis, NAC regimens, surgical procedure, pathological responses to NAC, and presence of recurrence, were collected from the patients’ medical records. ER, PgR, and HER2 statuses were examined in samples collected by pretreatment core needle biopsy. Subtypes of breast cancer were defined as follows: luminal (ER or PgR positive and HER2 negative), luminal HER2 (ER or PgR positive and HER2 positive), HER2-enriched (ER and PgR negative, HER2 positive), and TN (ER, PgR, and HER2 negative). HG was determined according to the Scarff–Bloom–Richardson grading system. Lymph node metastasis was determined by fine-needle aspiration cytology (FNA), but some patients were considered positive for lymph node metastasis without FNA if abnormal swelling of lymph nodes in CT findings or strong uptake of 18F-FDG on PET/CT findings was apparent. Disease-free survival (DFS) was defined as the time from surgery to the date of detection of locoregional relapse or distant metastases, whichever occurred first. Overall survival (OS) was assessed from the day of surgery to the date of death from any causes.
Skeletal muscle area (SMA) was measured using CT or 18F-FDG-PET/CT images before NAC and surgery. 18F-FDG PET/CT scans were taken at the Ichinose Neurosurgical Hospital (Matsumoto, Nagano, Japan) with a standard technique using a Discovery ST Elite Performance scanner (GE Healthcare Japan, Tokyo, Japan). Attenuation-corrected images were reconstructed in the coronal plane. SMA was measured as the cross-sectional area of the surrounding muscles (i.e., psoas, paraspinals, transversus abdominis, rectus abdominis, and internal and external obliques) by semi-automatic tracing using images at the third lumbar vertebral level (L3) visualized within a range of − 29 to 150 Hounsfield units using the EV Insite R (PSP Corporation, Tokyo, Japan) system and expressed in cm2. SMI was calculated as the ratio of SMA divided by height squared (m2), whereas BMI was calculated as the patient’s body weight (kg) divided by height squared (m2). The percent change in SMI and BMI was calculated as the percent change in each parameter after NAC from that at pretreatment. The serum albumin (Alb) (g/dl) and neutrophil-to-lymphocyte ratio (NLR), which was calculated as the total neutrophil count divided by the total lymphocyte counts, were also obtained from pre- and post-NAC blood examination. The change of Alb and NLR value during NAC were calculated as each value on post-NAC minus that on pre-NAC.
NAC regimens and surgical methods
Two different NAC regimens were used: (1) triweekly administered anthracycline-based fluorouracil-epirubicin-cyclophosphamide (FEC) (500 mg/m2 fluorouracil, 100 mg/m2 epirubicin, and 500 mg/m2 cyclophosphamide) regimen, except for one patient who had been treated with an EC (60 mg/m2 epirubicin and 600 mg/m2 cyclophosphamide) regimen in another hospital and was transferred to our hospital for surgery, and (2) taxane regimens, including triweekly administered docetaxel (DTX) 75 mg/m2 or weekly administered paclitaxel (PTX) 80 mg/m2. Four cycles of DTX or PTX was administered following four cycles of EC/FEC. In HER2-positive patients, 6 mg/kg (triweekly) or 2 mg/kg (weekly) trastuzumab was administered simultaneously with a taxane regimen. For the EC/FEC regimen, dexamethasone (12 mg) and granisetron hydrochloride (3 mg) or palonosetron hydrochloride (0.75 mg) were infused intravenously before the administration of chemotherapeutic agents. Together with these drugs, aprepitant (125 mg) was orally administered to avoid chemotherapy-induced nausea and vomiting since 2011. Concomitantly, dexamethasone (8 mg) was administered orally one and 2 days after treatment. In addition, aprepitant (80 mg) or granisetron hydrochloride (2 mg) was orally administered from 1 day after treatment for two (aprepitant) or five (granisetron hydrochloride) consecutive days. For PTX and DTX treatment, 8 mg of dexamethasone was administered intravenously prior to treatment. In addition, for patients treated with DTX, 8 mg of dexamethasone was administered 1 day before treatment and 1 day and 2 days after treatment (a total of 3 days) orally. Surgery was performed within 4–7 weeks after NAC completion. All patients underwent axillary lymph node dissection. The efficacy of NAC was pathologically examined in surgical specimens, and pCR was defined as no evidence of residual invasive carcinoma in the breast tissue, regardless of the axillary lymph node status.
Adjuvant trastuzumab, endocrine, and radiation therapy after surgery
Following surgery, extensional adjuvant trastuzumab (initially 8 mg/kg, followed by 6 mg/kg) was administered every 3 weeks for 12 months to patients with HER2-positive breast cancer. Whole breast irradiation of 50–60 Gy was performed for patients who underwent breast-conserving surgery, whereas chest wall and regional lymph node irradiation of 50–60 Gy was performed for patients with more than three nodal metastases on postoperative pathological examinations or preoperative imaging examinations, including ultrasonography, magnetic resonance imaging, or 18F-FDG-PET/CT. In addition, postmenopausal patients with positive ER or PgR status were treated with aromatase inhibitors for more than 5 years, whereas premenopausal patients were treated with tamoxifen or tamoxifen with luteinizing hormone-releasing hormone agonist.
Statistical analyses
Categorical variables were analyzed using the chi-squared test, whereas continuous variables were analyzed using two-sided t-tests or one-way analysis of variance with Tukey’s multiple comparisons. Survival curves were estimated using the Kaplan–Meier method, and significant differences in survival were assessed using the log-rank test. Univariate and multivariate analyses with a Cox proportional hazards model were performed to determine the significant factors associated with OS. Multivariate analysis was performed for parameters with p < 0.05 in the univariate analysis. All statistical analyses were performed using StatFlex version 6 (Artech Co., Ltd., Osaka, Japan) and GraphPad Prism 8.0.2 (GraphPad Software, CA, USA), and p < 0.05 was considered statistically significant.
Results
Baseline patient characteristics
The clinicopathological characteristics of the 141 patients enrolled in this study are shown in Table 1. The mean age of patients (± standard deviation) was 52.3 ± 10.1 years, and all the patients were female. Seventy-nine (56.0%) patients were premenopausal, whereas 62 (44.0%) patients were postmenopausal. With regard to the histological type of breast cancer, 127 (90.1%) patients had invasive ductal carcinoma, and 14 (9.9%) patients had special types. As for HG, 38 (27.0%), 69 (48.9%), and 29 (20.6%) patients had breast cancer with HG 1, 2, and 3, respectively. Regarding the subtype of breast cancer, 75 (53.2%) cases were luminal, 30 (21.3%) cases were luminal HER2, 16 (11.3%) cases were HER2-enriched, and 20 (14.2%) cases were TN breast cancer. Axillary lymph nodes were involved in 122 (86.5%) patients. Regarding the clinical stage at diagnosis, 89 (63.1%) and 52 (36.9%) patients had stage II and III breast cancer, respectively. Fifty-seven (40.4%) patients were treated with EC/FEC followed by weekly PTX and/or trastuzumab, while 84 (59.6%) patients were with EC/FEC followed by triweekly DTX and/or trastuzumab. After NAC, mastectomy was performed in 107 (75.9%) patients, whereas partial resection of the breast was performed in 34 (24.1%) patients. pCR was obtained in 29 (20.6%) patients. The mean SMI before NAC (pre-SMI) was 46.5 ± 7.6, whereas that after NAC (post-SMI) was 46.3 ± 8.0. The mean BMI before NAC (pre-BMI) was 22.4 ± 3.7, and that after NAC (post-BMI) was 22.4 ± 3.7. The percent changes in SMI and BMI were − 27.7 to 19.6 and − 22.9 to 34.2, respectively. Regarding Alb and NLR, the mean values before NAC were 4.50 ± 0.30 and 2.53 ± 1.54, whereas those after NAC were 4.07 ± 0.36 and 3.03 ± 1.61, respectively. The changes in Alb and NLR were − 1.1 to 0.6 and − 5.20 to 6.00, respectively. The percent change in SMI was shown to have a slight inverse correlation with changes in both Alb and NLR values (Additional file 1: Fig. S1a, b). On the other hand, the percent change in SMI showed a tendency to have a positive correlation with the percent change in SMI (Additional file 1: Fig. S1c). The median follow-up period after surgery was 70 (range, 3–131) months, and 33 (23.4%) patients developed recurrence. Among these recurrences, locoregional relapses (chest wall, supraclavicular lymph nodes, or parasternal lymph nodes) were observed in 5 (3.5%) patients, while distant metastases (bone, lung, liver, or brain) occurred in 28 (19.9%) patients.
Association between skeletal muscle index (SMI) or body mass index (BMI) and recurrence
To analyze the influence of skeletal muscle mass and body weight on disease recurrence, we divided patients into two groups according to the presence of recurrence and compared pre- and post-SMI and BMI. There were no significant differences in either pre-SMI or pre-BMI between patients with recurrence and those without recurrence (p = 0.91 for pre-SMI, p = 0.70 for pre-BMI) (Additional file 2: Fig. S2a, b). In contrast, after NAC, patients who developed recurrence exhibited significantly lower post-SMI (p = 0.010), whereas post-BMI did not show a difference between the two groups (p = 0.88) (Additional file 2: Fig. S2c, d).
Association between changes in SMI during neoadjuvant chemotherapy (NAC) and patient outcomes
As we found a significant difference in post-SMI between patients with and without recurrence after NAC, we focused on the changes in SMI during NAC in individual patients and their correlation with DFS and OS. To address this, we divided the patients into three groups (increased: ≥ 3% increase, maintained: − 3% <, < 3% change, decreased: − 3% ≥ decrease in SMI during NAC) according to the percent change in SMI. As shown in Fig. 1, 48 (34.0%), 53 (37.6%), and 40 (28.4%) patients exhibited increased, maintained, and decreased SMI, respectively. The clinicopathological characteristics of the decreased, maintained, and increased SMI groups are shown in Table 2 and Table 3. Menopausal status, histological type, HG, subtype, lymph node metastasis, clinical stage, NAC regimen, surgical procedure were not significantly different among the three groups, whereas the increased SMI group had a significantly lower mean age (p = 0.03) and higher pCR rate (p = 0.03) than the maintained and decreased SMI groups. Recurrence was significantly more prevalent in the decreased SMI group than in the maintained and decreased SMI groups (p = 0.04). Distant metastases were frequently developed in the decreased SMI group (45.0%) compared to the maintained (13.2%) and decreased (6.3%) SMI groups although there was no significant difference (p = 0.32). As shown in Table 3, pre-Alb, post-Alb, and change in Alb during NAC were not significantly different among the three groups. Although there was no statistically significant difference, pre-NLR and post-NLR values were the highest in the decreased SMI group (pre: 2.77 ± 2.13, post: 3.40 ± 1.79), and gradually decreased toward the maintained (pre: 2.49 ± 1.38, post: 3.02 ± 1.59) and increased (pre: 2.38 ± 1.04, post: 2.72 ± 1.44) SMI groups. Furthermore, the change in NLR was the highest in the decreased SMI group (0.62 ± 1.99) and showed a decreasing trend toward the maintained (0.54 ± 1.74) and increased (0.20 ± 1.31) SMI groups in this order. Regarding BMI, although pre-BMI and post-BMI were not significantly different between the three groups, percent change in BMI was highest in the increased SMI group (0.91 ± 5.74) and gradually decreased toward the maintained (− 0.22 ± 3.96) and decreased (− 1.11 ± 8.26) SMI groups.

Percent Change in SMI during NAC of individual patient. Increased was defined as more than 3% increase, maintained as within − 3 to 3% change, and decreased as more than 3% decrease, respectively. Circle indicates the patient who developed recurrence. SMI: Skeletal muscle index, NAC: Neoadjuvant chemotherapy
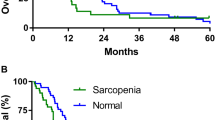
The decreased SMI group had significantly poorer DFS than the maintained and increased groups (hazard ratio [HR] 8.29, 95% confidence interval [CI] 3.63–18.9, p < 0.001 for the decreased vs. increased SMI group; HR 3.49, 95% CI 1.65–7.36, p < 0.001 for the decreased vs. maintained SMI group) (Fig. 2). In addition, a trend for poorer DFS was found in the maintained SMI group than in the increased SMI group, although the difference was not statistically significant (HR 2.30, 95% CI 0.77–6.84, p = 0.15) (Fig. 2). In line with the DFS, the OS was significantly shorter in the decreased SMI group than in the maintained and increased SMI groups (HR 19.8, 95% CI 6.43–60.6, p < 0.001 for the decreased vs. increased SMI group; HR 3.41, 95% CI 1.29–8.95, p = 0.013 for the decreased vs. maintained SMI group) (Fig. 2).

Kaplan–Meier curves for DFS (left) and OS (right) according to changes in SMI (increased, maintained, and decreased). DFS, HR 8.29; 95%CI 3.63–18.9; p < 0.001 for decreased vs. increased, HR 3.49; 95%CI 1.65–7.36; p < 0.001 decreased vs. maintained, HR 2.30; 95%CI 0.77–6.84; p = 0.15 maintained vs. increased. OS, HR 19.8; 95%CI 6.43–60.6; p < 0.001 for decreased vs. increased, HR 3.41; 95%CI 1.29–8.95; p = 0.013 decreased vs. maintained, HR 4.98; 95%CI 0.99–24.5; p = 0.11, maintained vs. increased). DFS: Disease-free survival, OS: Overall survival, SMI: Skeletal muscle index, NAC: Neoadjuvant chemotherapy, HR: Hazard ratio, CI: Confidence interval
Association between SMI change during NAC and patient outcomes on various clinical factors
To investigate whether the effect of SMI change on prognosis is dependent on various clinical factors, including menopausal status (premenopausal vs. postmenopausal), pretreatment clinical stage (stage II vs. stage III), and subtype of breast cancer, we divided the patients according to these factors and compared the DFS among the decreased, maintained, and increased SMI groups with each factor. We found that the decreased SMI group showed poorer DFS than the maintained and increased SMI groups regardless of menopausal status and clinical stage (Additional file 3: Fig. S3; Additional file 4: Table S1). With regard to subtype, the decreased SMI group showed significantly worse DFS than the increased SMI group in patients with luminal (p < 0.001), HER2-enriched (p = 0.020), and TN (p = 0.039) breast cancer. Of the 30 patients with luminal HER2 breast cancer, only two developed recurrence. Possibly due to the lack of patients who had recurrence, we did not find statistical significance in DFS between the decreased and increased groups in this subtype. However, one patient who exhibited disease recurrence was in the decreased group (Additional file 5: Fig. S4, Additional file 4: Table S1).
Next, we investigated whether the kind of taxane regimen (PTX or DTX) would affect the prognosis or impact of SMI change, and found that there was no significant difference in DFS between the patients treated with PTX and those treated with DTX (HR 0.95, 95% CI 0.47–1.91, p = 0.89) (Additional file 6: Fig. S5). Furthermore, irrespective of taxane regimen, the decreased SMI group exhibited poorer DFS than the maintained and increased SMI groups (Additional file 7: Fig. S6, Additional file 4: Table S1).
Univariate and multivariate analyses
To confirm the significance of changes in SMI on DFS, univariate and multivariate analyses were performed. Univariate analysis revealed that a decrease in SMI was significantly associated with poorer DFS (HR 3.46, 95% CI 1.56–7.65, p < 0.01). The other factors that correlated with poorer DFS were postmenopausal (HR 2.15, 95% CI 1.07–4.34, p = 0.03), luminal HER2 (HR 0.20, 95% CI 0.04–0.88, p = 0.03), pre-NAC clinical stage III (HR 2.18, 95% CI 1.10–4.32, p = 0.02), and pCR (HR 0.22, 95% CI 0.05–0.95, p = 0.04). On multivariate analysis using the Cox hazards model, SMI decrease was an independent predictive factor for poorer DFS (HR 3.68, 95% CI 1.54–9.01, p < 0.01) (Table 4).
Discussion
The present study demonstrates that skeletal muscle loss during NAC is significantly associated with poor prognosis and is an independent predictor of DFS in patients with breast cancer. In addition, the results of this study suggest that SMI decrease might be a prognostic marker of patient outcomes irrespective of menopausal status, clinical stage, and subtype of breast cancer. To the best of our knowledge, this is the first study to demonstrate that loss of skeletal muscle is a prognostic factor in patients with breast cancer who underwent NAC.
Accumulating evidence suggests that patients with cancer who underwent palliative chemotherapy were likely to lose skeletal muscle mass in various solid malignancies, including gastric, colorectal, and lung cancers [17,18,19, 22, 25, 26]. Furthermore, recent studies in patients with esophageal cancer have shown that not only palliative chemotherapy but also NAC comprising fluorouracil, cisplatin, and adriamycin or fluorouracil, cisplatin, and DTX could decrease SMI [25, 27, 28]. However, as for breast cancer, there have been no studies demonstrating the loss of SMI during NAC. In this regard, the results of this study showed that 27.4% of all patients lost more than 3% of SMI during NAC, which provides a novel insight that anthracycline and taxane-based NAC for breast cancer can induce skeletal muscle loss.
Skeletal muscle atrophy has been known to be caused by both reduction of protein synthesis and protein degradation in various diseases and body conditions [29]. Three possible mechanisms underlying muscle loss during chemotherapy have been considered: (1) decreased food intake due to gastrointestinal adverse effects, (2) reduced physical activity secondary to general fatigue, and (3) direct effect of chemotherapy on muscles [26]. Furthermore, as another mechanism, the indirect effect of chemotherapy on muscle alteration via immune cells was suggested [30]. Wang et al. showed that T cells could attenuate muscle mass loss during cancer progression [31]. In contrast, circulating neutrophils in patients with cancer have been shown to induce skeletal muscle degeneration [30, 32]. Although the severity varies in each patient, chemotherapy generally causes neutropenia and lymphopenia [33] and thus can indirectly affect muscle alteration. In this regard, a decrease in NLR may prevent muscle loss during NAC. This notion is consistent with our results, showing that percent change in SMI had a moderate negative correlation with the change in NLR value, indicating that patients with decreased SMI tended to have increased NLR during NAC. On the other hand, the results of the present study demonstrate that the percent change in SMI did not have a positive correlation with change in serum Alb. This suggests that NAC-induced malnutritional status might not be the main cause of muscle loss. Therefore, although further investigations are needed, the present study indicates that the muscle loss during NAC for patients with breast cancer may be due, at least in part, to the indirect effects of chemotherapy on muscles via immune cells.
Although emerging evidence suggests that pretreatment SMI is a prognostic marker for patients with breast cancer [8, 10, 13, 14, 34,35,36,37], the clinical significance of changes in SMI during treatment in an individual patient remains unknown. In this regard, our results provide a novel finding that a decrease in SMI during NAC might have a negative effect on prognosis in patients with breast cancer. Similar to this study, we previously demonstrated that a decrease in PNI during NAC for patients with breast cancer was associated with worse prognosis, but not pretreatment PNI [3]. Furthermore, other studies have shown that changes in NLR during NAC correlated with the efficacy of NAC and patient survival [38,39,40]. These reports, together with the results of the present study, highlight the importance of monitoring the dynamic changes in systemic nutritional conditions and body composition throughout the treatment course.
The results of our study indicate that SMI loss would have high availability as a prognostic factor in patients with breast cancer who underwent NAC. First, poorer outcomes in patients with decreased SMI were observed irrespective of menopausal status and pretreatment clinical stage. Thus, the usefulness of SMI loss as a prognostic factor was indicated regardless of the hormonal conditions of patients, patient age, and tumor burden at the beginning of NAC. Second, poorer outcomes in patients with decreased SMI were observed regardless of the subtype. Generally, the skeletal muscle volume of patients with breast cancer may be independent of tumor characteristics determined by ER and HER2 expression, especially in the early stages [4]. The results of the present study are consistent with this notion and indicate that SMI change can predict patient outcomes irrespective of tumor biology itself. Altogether, our results suggest that SMI loss during NAC can be a prognostic marker in any age, stage, or subtype. However, majority of patients enrolled in this study had luminal type breast cancer, and the number of HER2-positive or TN breast cancer was limited. Luminal type breast cancer is known to show limited response to chemotherapy; hence, it is difficult to accomplish pCR, whereas HER2-positive or TN breast cancer has high sensitivity to chemotherapy as a subset of these subtypes can be pathologically eliminated (pCR) by NAC [2]. Thus, the impact of SMI change on response to chemotherapy varies according to the subtype. Regarding the influence of SMI change on DFS of patients who underwent NAC, although a similar trend was observed among luminal, HER2-enriched, and TN breast cancer in this study, further large-scale studies are required to determine the importance of SMI change in each subtype of breast cancer.
Our results highlight the importance of SMI maintenance during NAC. To date, phase III studies (ROMANA1 and ROMANA 2) have demonstrated that pharmacotherapies with anamorelin (a ghrelin receptor agonist) significantly increased lean body mass in patients with non-small cell lung cancer who underwent chemotherapy [41]. However, multimodal approaches are required to dissolve multifactorial symptoms, such as SMI loss [42]. Indeed, a phase III trial (NCT02330926) is currently ongoing to test whether a multimodal intervention, including exercise, nutritional support, and anti-inflammatory medication, plus standard care can improve the treatment outcome of patients with cancer, the results of which are awaited.
This study has some limitations. First, it was a retrospective analysis with a relatively small study population in a single institution from one Asian country. Second, the NAC regimens were not uniform among patients because the study period spanned several years when the treatment regimens were changed. Furthermore, majority of patients enrolled in this study had luminal subtype breast cancer and were perimenopausal. Thus, estrogen-related effect can have some impact on the results of this study. Although our results indicate that a decrease in SMI is associated with poor outcomes irrespective of menopausal status and subtype, we could not determine the impact of estrogen-driven factors from our results. Chemotherapy-induced menopause also should be taken into consideration. To overcome these limitations and validate our results, further investigations are required. In particular, a prospective multicountry study is warranted to diversify our findings to more heterogenous populations with different races/ethnicities and environmental backgrounds.
Conclusions
The findings of the present study indicate that skeletal muscle loss during NAC can be a prognostic marker in patients with breast cancer. If this observation is confirmed in larger prospective studies from other countries, it could provide the basis of the importance to monitor and maintain skeletal muscle mass during NAC.
Availability of data and materials
The data supporting the findings of this work are available from the corresponding author upon reasonable request.
Abbreviations
- Alb:
-
Serum albumin level
- BMI:
-
Body mass index
- DTX:
-
Docetaxel
- EC:
-
Epirubicin and cyclophosphamide
- ER:
-
Estrogen receptor
- FNA:
-
Fine-needle aspiration cytology
- FEC:
-
Fluorouracil epirubicin and cyclophosphamide
- HER2:
-
Human epidermal growth factor receptor type 2
- HG:
-
Histological grade
- NAC:
-
Neoadjuvant chemotherapy
- NLR:
-
Neutrophil-to-lymphocyte ratio
- pCR:
-
Pathological complete response
- PgR:
-
Progesterone receptor
- PNI:
-
Prognostic nutritional index
- PTX:
-
Paclitaxel
- ROC:
-
Receiver operating characteristics
- SMA:
-
Skeletal muscle area
- SMI:
-
Skeletal muscle index
- TN:
-
Triple negative
References
Kaufmann M, von Minckwitz G, Bear HD, Buzdar A, McGale P, Bonnefoi H, et al. Recommendations from an international expert panel on the use of neoadjuvant (primary) systemic treatment of operable breast cancer: new perspectives 2006. Ann Oncol. 2007;18:1927–34.
von Minckwitz G, Untch M, Blohmer JU, Costa SD, Eidtmann H, Fasching PA, et al. Definition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. J Clin Oncol. 2012;30:1796–804.
Oba T, Maeno K, Takekoshi D, Ono M, Ito T, Kanai T, et al. Neoadjuvant chemotherapy-induced decrease of prognostic nutrition index predicts poor prognosis in patients with breast cancer. BMC Cancer. 2020;20:160.
Kogawa T, Fujii T, Fouad TM, Liu DD, Harano K, Masuda H, et al. Impact of change in body mass index during neoadjuvant chemotherapy and survival among breast cancer subtypes. Breast Cancer Res Treat. 2018;171:501–11.
Kwan ML, Chen WY, Kroenke CH, Weltzien EK, Beasley JM, Nechuta SJ, et al. Pre-diagnosis body mass index and survival after breast cancer in the after breast Cancer pooling project. Breast Cancer Res Treat. 2012;132:729–39.
Obermair A, Kurz C, Hanzal E, Bancher-Todesca D, Thoma M, Bodisch A, et al. The influence of obesity on the disease-free survival in primary breast cancer. Anticancer Res. 1995;15:2265–9.
Davis MP, Panikkar R. Sarcopenia associated with chemotherapy and targeted agents for cancer therapy. Ann Palliat Med. 2019;8:86–101.
Zhang XM, Dou QL, Zeng Y, Yang Y, Cheng ASK, Zhang WW. Sarcopenia as a predictor of mortality in women with breast cancer: a meta-analysis and systematic review. BMC Cancer. 2020;20:172.
Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48:16–31.
Villaseñor A, Ballard-Barbash R, Baumgartner K, Baumgartner R, Bernstein L, McTiernan A, et al. Prevalence and prognostic effect of sarcopenia in breast cancer survivors: the HEAL study. J Cancer Surviv. 2012;6:398–406.
Shachar SS, Williams GR, Muss HB, Nishijima TF. Prognostic value of sarcopenia in adults with solid tumours: a meta-analysis and systematic review. Eur J Cancer. 2016;57:58–67.
Pamoukdjian F, Bouillet T, Lévy V, Soussan M, Zelek L, Paillaud E. Prevalence and predictive value of pre-therapeutic sarcopenia in cancer patients: a systematic review. Clin Nutr. 2018;37:1101–13.
Huh J, Park B, Lee H, An YS, Jung Y, Kim JY, et al. Prognostic value of skeletal muscle depletion measured on computed tomography for overall survival in patients with non-metastatic breast Cancer. J Breast Cancer. 2020;23:80–92.
Deluche E, Leobon S, Desport JC, Venat-Bouvet L, Usseglio J, Tubiana-Mathieu N. Impact of body composition on outcome in patients with early breast cancer. Support Care Cancer. 2018;26:861–8.
Caan BJ, Cespedes Feliciano EM, Prado CM, Alexeeff S, Kroenke CH, Bradshaw P, et al. Association of Muscle and Adiposity Measured by computed tomography with survival in patients with nonmetastatic breast Cancer. JAMA Oncol. 2018;4:798–804.
Aleixo GFP, Shachar SS, Deal AM, Nyrop KA, Muss HB, Chen YT, et al. The association of body composition parameters and adverse events in women receiving chemotherapy for early breast cancer. Breast Cancer Res Treat. 2020;182:631–42.
Stene GB, Helbostad JL, Amundsen T, Sørhaug S, Hjelde H, Kaasa S, et al. Changes in skeletal muscle mass during palliative chemotherapy in patients with advanced lung cancer. Acta Oncol. 2015;54:340–8.
Sasaki S, Oki E, Saeki H, Shimose T, Sakamoto S, Hu Q, et al. Skeletal muscle loss during systemic chemotherapy for colorectal cancer indicates treatment response: a pooled analysis of a multicenter clinical trial (KSCC 1605-a). Int J Clin Oncol. 2019;24:1204–13.
Daly LE, ÉB NB, Power DG, Cushen SJ, James K, Ryan AM. Loss of skeletal muscle during systemic chemotherapy is prognostic of poor survival in patients with foregut cancer. J Cachexia Sarcopenia Muscle. 2018;9:315–25.
Blauwhoff-Buskermolen S, Versteeg KS, de van der Schueren MA, den Braver NR, Berkhof J, Langius JA, et al. Loss of muscle mass during chemotherapy is predictive for poor survival of patients with metastatic colorectal Cancer. J Clin Oncol. 2016;34:1339–44.
Miyamoto Y, Baba Y, Sakamoto Y, Ohuchi M, Tokunaga R, Kurashige J, et al. Negative impact of skeletal muscle loss after systemic chemotherapy in patients with Unresectable colorectal Cancer. PLoS One. 2015;10:e0129742.
Park SE, Choi JH, Park JY, Kim BJ, Kim JG, Kim JW, et al. Loss of skeletal muscle mass during palliative chemotherapy is a poor prognostic factor in patients with advanced gastric cancer. Sci Rep. 2020;10:17683.
Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2021. CA Cancer J Clin. 2021;71:7–33.
Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, McFadden ET, et al. Toxicity and response criteria of the eastern cooperative oncology group. Am J Clin Oncol. 1982;5:649–55.
Miyata H, Sugimura K, Motoori M, Fujiwara Y, Omori T, Yanagimoto Y, et al. Clinical assessment of sarcopenia and changes in body composition during neoadjuvant chemotherapy for esophageal Cancer. Anticancer Res. 2017;37:3053–9.
Kodera Y. More than 6 months of postoperative adjuvant chemotherapy results in loss of skeletal muscle: a challenge to the current standard of care. Gastric Cancer. 2015;18:203–4.
Yip C, Goh V, Davies A, Gossage J, Mitchell-Hay R, Hynes O, et al. Assessment of sarcopenia and changes in body composition after neoadjuvant chemotherapy and associations with clinical outcomes in oesophageal cancer. Eur Radiol. 2014;24:998–1005.
Saeki H, Nakashima Y, Kudou K, Sasaki S, Jogo T, Hirose K, et al. Neoadjuvant Chemoradiotherapy for patients with cT3/nearly T4 esophageal Cancer: is sarcopenia correlated with postoperative complications and prognosis? World J Surg. 2018;42:2894–901.
Foletta VC, White LJ, Larsen AE, Léger B, Russell AP. The role and regulation of MAFbx/atrogin-1 and MuRF1 in skeletal muscle atrophy. Pflugers Arch. 2011;461:325–35.
VanderVeen BN, Murphy EA, Carson JA. The impact of immune cells on the skeletal muscle microenvironment during Cancer Cachexia. Front Physiol. 2020;11:1037.
Wang Z, Zhao C, Moya R, Davies JD. A novel role for CD4+ T cells in the control of cachexia. J Immunol. 2008;181:4676–84.
Shigeto K, Kawaguchi T, Koya S, Hirota K, Tanaka T, Nagasu S, et al. Profiles combining muscle atrophy and neutrophil-to-lymphocyte ratio are associated with prognosis of patients with stage IV gastric Cancer. Nutrients. 2020;12.
Shitara K, Matsuo K, Oze I, Mizota A, Kondo C, Nomura M, et al. Meta-analysis of neutropenia or leukopenia as a prognostic factor in patients with malignant disease undergoing chemotherapy. Cancer Chemother Pharmacol. 2011;68:301–7.
Solomayer EF, Braun EM, Zimmermann JSM, Radosa JC, Stroeder J, Endrikat J, et al. Muscle mass loss in patients with metastatic breast cancer. Arch Gynecol Obstet. 2019;300:201–6.
Song EJ, Lee CW, Jung SY, Kim BN, Lee KS, Lee S, et al. Prognostic impact of skeletal muscle volume derived from cross-sectional computed tomography images in breast cancer. Breast Cancer Res Treat. 2018;172:425–36.
Shachar SS, Deal AM, Weinberg M, Nyrop KA, Williams GR, Nishijima TF, et al. Skeletal muscle measures as predictors of toxicity, hospitalization, and survival in patients with metastatic breast Cancer receiving Taxane-based chemotherapy. Clin Cancer Res. 2017;23:658–65.
Cespedes Feliciano E, Chen WY. Clinical implications of low skeletal muscle mass in early-stage breast and colorectal cancer. Proc Nutr Soc. 2018;77:382–7.
Kim JY, Jung EJ, Kim JM, Lee HS, Kwag SJ, Park JH, et al. Dynamic changes of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio predicts breast cancer prognosis. BMC Cancer. 2020;20:1206.
Choi H, Noh H, Cho IJ, Lim ST, Han A. Changes in neutrophil to lymphocyte ratio (NLR) during neoadjuvant treatment correlated with patients' survival. Breast Cancer. 2020;27:871–9.
Dan J, Tan J, Huang J, Zhang X, Guo Y, Huang Y, et al. The dynamic change of neutrophil to lymphocyte ratio is predictive of pathological complete response after neoadjuvant chemotherapy in breast cancer patients. Breast Cancer. 2020;27:982–8.
Temel JS, Abernethy AP, Currow DC, Friend J, Duus EM, Yan Y, et al. Anamorelin in patients with non-small-cell lung cancer and cachexia (ROMANA 1 and ROMANA 2): results from two randomised, double-blind, phase 3 trials. Lancet Oncol. 2016;17:519–31.
Solheim TS, Laird BJ. Evidence base for multimodal therapy in cachexia. Curr Opin Support Palliat Care. 2012;6:424–31.
Acknowledgements
We would like to thank Editage (www.editage.com) for English language editing.
Funding
This work was not funded by any grant.
Author information
Authors and Affiliations
Contributions
MA and TO designed the study. MA, TO, NK, HM, TC, AS, TS, KO, MO, TI, TK, KM collected the clinical data. MA and TO performed the statistical analysis. The draft manuscript was prepared by MA, TO and KI. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Medical Ethics Committee on Clinical Investigation of Shinshu University (no. 5037). Patients were provided the opportunity to opt out of participation in this study via notifications displayed in the outpatient ward and the institution’s website. Unless patients reject the enrollment in this study, the requirement for written informed consent was waived by the Medical Ethics Committee on Clinical Investigation of Shinshu University. This study was conducted in accordance with the principles laid down in the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Amitani, M., Oba, T., Kiyosawa, N. et al. Skeletal muscle loss during neoadjuvant chemotherapy predicts poor prognosis in patients with breast cancer. BMC Cancer 22, 327 (2022). https://doi.org/10.1186/s12885-022-09443-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-022-09443-1