
Abstract
Background
The purpose was to examine the effect of negative lymph nodes (NLN) number on survival in stage III colon cancer. To reduce the interference of acute inflammation, we included patients with stage III colon cancer who had undergone elective surgery and excluded those who had tumor perforation, obstruction, ischemia, or massive tumor bleeding.
Methods
This retrospective cohort study included 2244 patients with stage III colon cancer between 1995 and 2016 at a single center. The effect of NLN on 5-year relapse-free survival (RFS), 5-year overall survival (OS), and comparison of multivariate factors was assessed according to tumor locations.
Results
The two optimal cutoff values of NLN for proximal and distal colon, namely 27 and 12, were determined by plotting the time-dependent receiver operating characteristic curve. Overall, 499 of 891 and 1020 of 1353 patients with right-side and left-side colon cancer, respectively, had high NLN. In right-side colon cancer, patients with high NLN (≥ 27) had superior OS (74.9% vs. 62.7%, P < 0.001) and RFS (75.0% vs. 61.9%, P < 0.001) than did those with low NLN. Moreover, in left-side colon cancer, patients with high NLN (≥12) experienced significantly superior OS (80.8% vs. 68.6%, P < 0.001) and RFS (77.3% vs. 66.2%, P < 0.001) than did those with low NLN. Among the different subgroups of stage III colon cancer, the high NLN group showed significantly superior RFS and OS in stage IIIB (RFS: 77.0% vs. 68.0%, P = 0.001; OS: 78.6% vs. 67.9%, P < 0.001) and IIIC (RFS: 58.2% vs. 44.1%, P = 0.001; OS: 65.7% vs. 51.1%, P < 0.001) colon cancer. However, in stage IIIA colon cancer, high NLN only showed survival benefit in OS (91.5% vs. 89.8%, P = 0.041). Multivariate analyses confirmed that high NLN, high carcinoembryonic antigen (≥ 5 ng/mL) level, and stage IIIC status are three independent prognostic factors in both the proximal and distal colon.
Conclusions
NLN is a crucial prognostic factor for stage III colon cancer in various tumor locations or in the subgroups of stage III disease. In advanced stage III colon cancer, the importance of NLN and its role in anti-cancer immune response could be highlighted.
Similar content being viewed by others


A brief description
This study explored the relationship of negative lymph nodes (NLN) to the long-term outcome of stage III colon cancer. The impact of increasing number of NLN on survival prognosis was noted either in stage III colon cancer or in their subgroups.
Background
Colorectal cancer (CRC) is the fourth most prevalent and the third most deadly cancer according to GLOBOCAN 2018 data [1]. After curative surgery, the tumor, node, and metastasis (TNM) stage, which is determined on the basis of the extent of tumor invasion and the status of lymph node metastasis and distant metastasis, is considered one of the most predictable prognostic factors [2]. In recent years, many studies have determined parameters associated with the lymph node status of CRC, including the number of lymph node harvest in stage II disease, metastatic lymph node ratio, and the number of negative lymph node (NLN) in stage III disease [3,4,5,6,7,8,9]. Some investigators believe that the more accurate stage of CRC could have resulted from increased lymph node examination, improved treatment quality, and advancement in surgical intervention or pathological evaluation. The number of NLN as a prognostic factor still is interesting when we consider the possible association between a patient’s immune response and their survival. Current evidence indicates that a suppressive cancer microenvironment formed due to interactions between tumor cells and other cells of the matrix, such as immune and nonimmune cells, is crucial for cancer development and progression [10,11,12]. Recently, a robust score quantification method for immune response was developed for clinical cancer classification. A low risk of cancer relapse was noted in patients with a high Immunoscore, which was quantified usingthe densities of CD3+ and cytotoxic CD8+ T cells in the tumor region and invasive margin. Patients’cancer recurrence at 5 years was 8, 19, and 32% in high, intermediate, and low Immunoscore groups [13].
Märkl et al. noted that lymph node size is a prognostic factor in node-negative colon cancer. The activation status of lymph nodes may be responsible for outcome differences associated with the number of lymph node yield in stage II colon cancer [14, 15]. Therefore, increased host’s immune response to tumors in CRC patients was hypothesized to be associated with a high number of NLN. In a large study performed using the Surveillance, Epidemiology, and End Result program (SEER) database, the association between the number of NLN and the prognosis of stage III colon cancer was analyzed [9]. In multivariate Cox regression, patients with the number of NLN ≥13 presented with significant survival advantage than did those with the number of NLN < 13. Up to date, few studies have analyzed the survival effect of the different numbers of NLN between right-side and left-side stage III colon cancer. Because a significant difference was noted in the number of lymph node yield in right-side and left-side colon cancer [16], the number of NLN for prognosis prediction could be different based on the location of stage III colon cancer. We conducted this retrospective study to assess the survival effect of the number of NLN on stage III colon cancer and its association with patients’ clinicopathological characteristics.
Patients and methods
Data sources
In total, 3034 patients with pathologic stage III colon cancer who underwent curative surgical resection at Chang Gung Memorial Hospital between 1995 and 2016 were initially enrolled in our analysis. Because an association existed between local or systemic inflammatory response syndrome and lymphadenopathy, only patients with stage III colon cancer without cancer obstruction, cancer perforation, ischemic colitis resulting from obstruction, or combinations of the aforementioned conditions were included in the present analysis. Finally, we excluded 790 patients and analyzed 2244 patients because of our study aim setting. Patients’ clinical and pathology data were collected prospectively and retrieved from the tumor registry of division of colon and rectal surgery. Follow-up data for survival were collected retrospectively according to medical record or interview. The last date of follow-up was February 28, 2020. In our data, no patient underwent preoperative radiotherapy or neoadjuvant chemotherapy. After selection, all matched cases had a mean follow-up of 64.5 months and a maximal follow-up of 154 months.
The clinicopathological data of each patient comprised their age; sex; preoperative laboratory data including Complete Blood Count/Differential Count carcinoembryonic antigen (CEA), and serum albumin; and cancer type, grade and TNM stage based on the Cancer Staging Manual, seventh edition, of American Joint Committee on Cancer. Tumor locations were divided into right side or proximal colon (proximal to the splenic flexure) and left side or distal colon (distal to the splenic flexure). All patients’ blood samples were obtained on admission for surgery. Appropriate approval for this observation study was obtained from the Institutional Review Board of the Chang Gung Medical Foundation (201701456B0).
Survival follow-up and statistical analyses
In the study, categorical characteristics were compared using Pearson’s chi-squared test in right-side and left-side colon cancer. The survival difference was estimated using the Kaplan–Meier method, and a comparison was performed using the log-rank test. Overall survival (OS) was defined as the interval between the date of cancer diagnosis and the time of any-cause death. Relapse-free survival (RFS) was defined as the time from curative surgery to the disease relapse date. The 5-year OS and RFS were considered primary end points. The confounders were controlled for by using a Cox regression model in multivariate analysis. All statistical analyses were performed using SPSS version 17 (SPSS Inc., Chicago, IL, USA). All P values were two tailed and considered statistically significant if they were < 0.05.
The association of NLN with oncology outcome in stage III colon cancer is unclear. Therefore, we analyzed the time-dependent receiver operating characteristic (ROC) curve to determine the optimal marginal value in our data. We focused on the ROC of NLN counts to determine patients’ RFS because colon cancer relapses are associated with patients’ overall survival [17]. The area under the ROC curve for the right-side colon was 0.610 (95% confidence interval [CI]: 0.572–0.648, P < 0.001), and that for the left-side colon was 0.602 (95% CI: 0.569–0.634, P < 0.001). According to the results of the ROC curve for 5-year RFS, the cutoff values of NLN in right-side and left-side colon cancer were 27 and 12, respectively (Fig. 1).

The time-dependent receiver operating characteristic (ROC) curve of the negative lymph node (NLN) counts for 5-year relapse-fee survival (RFS). Area under the ROC curve in right-side colon: 0.610 (95% confidence interval [CI]: 0.572–0.648, P < 0.001); area under the ROC curve for left-side colon: 0.602 (95% CI: 0.569–0.634, P < 0.001)
Results
Patient characteristics
The overall clinical characteristics of 2244 patients were as follows: patients’ median age at colon cancer diagnosis was 63 years (range, 22–99 years), and 50.4% of patients were men. The 891 right-side colon cancers tended to be more common in women (53.4%) than those in men (46.6%). In contrast to the gender distribution in right-side colon cancer, males (52.8%) were prominent than females (47.2%) in left-side colon cancer (P = 0.004, data not shown in Table). In pathology and tumor locations of all stage III colon cancers, right-side colon cancer accounted for 39.7% of enrolled patients. Among enrolled patients, 35.6 and 77.6% had abnormal CEA (≥5 ng/mL) and received adjuvant chemotherapy, respectively. The median numbers of examined lymph node (ELN), positive lymph node (PLN), and NLN were 26 (range, 2–154), 2 (range, 1–36), and 22 (range, 0–150), respectively, in the cohort of this study. The number of lymph node yield met the quality target(i.e. ≥12) in 94% of enrolled patients.
According to different tumor locations, the mean number and standard deviation of ELN were significantly higher in right-side colon cancer than in left-side colon cancer (35 ± 18 vs. 26 ± 15, P < 0.001). According to a previous study for reference data of the neutrophil-to-lymphocyte ratio (NLR) in Asia, an NLR of ≥2.87 was defined as abnormal [18]. The mean and standard deviation of NLR were 3.4 ± 3.3 and 2.9 ± 2.6 in stage III right-side and left-side colon cancer, respectively (P < 0.001).
To analyze the effect of the number of NLN on survival in stage III colon cancer, we defined optimal cutoff values for the number of NLN according to different tumor locations because significantly more ELN was noted in the right-side than in the left-side colon. Correlations between the NLN groups of different colon cancer locations and clinicopathological characteristics are summarized in Table 1. Overall, 499 of 891 and 1020 of 1353 patients with proximal and distal colon cancer, respectively, had high NLN. Patients with right-side as well as left-side colon cancer with a high number of NLN had a high proportion of pathological TNM − N1 stage. In right-side colon cancer, patients who received adjuvant chemotherapy after curative surgery (85.4% vs. 74.7, P < 0.001) and had adequate ELN (lymph node harvest ≥12, 100% vs. 89.6%, P < 0.001) were more in the high NLN group than in the low NLN group. Moreover, similar findings were presented in left-side colon cancer: adjuvant chemotherapy implementation (82.9% vs. 74.6%, P = 0.001) and adequate ELN proportion (number ≥ 12, 100.0% vs. 74.5%, P < 0.001) was significantly different between these two NLN groups.
Survival analyses
In this study, the 5-year RFS and OS of right-side colon cancer were 62.3 and 69.4% and those of left-side colon cancer were 65.4 and 75.7%, respectively. In stage III colon cancer with high and low NLN, patients with a high number of NLN (≥27) in right-side colon cancer experienced a significantly better 5-year OS (74.9% vs. 62.7%, P < 0.001) and 5-year RFS (75.0% vs. 61.9%, P < 0.001) than did those with a low number of NLN (Fig. 2). Furthermore, similar results were noted in left-side colon cancer; that is, patients with a high number of NLN (≥12) experienced a significantly superior 5-year OS (80.8% vs. 68.6%, P < 0.001) and 5-year RFS (77.3% vs. 66.2%, P < 0.001) than did those with a low number of NLN (Fig. 3).

5-year relapse-fee survival (RFS) and 5-year overall survival (OS) for stage III colon cancer in right-side colon. Kaplan-Meier curve was according to number of nonmetastatic lymph nodes (NLN ≥27 vs. < 27)

5-year relapse-fee survival (RFS) and 5-year overall survival (OS) for stage III colon cancer in leftt-side colon. Kaplan-Meier curve was according to number of nonmetastatic lymph nodes (NLN ≥12 vs. < 12)
In a multivariate analysis of Cox regression for 5-year RFS and 5-year OS (Tables 2 and 3), the effect of a high number of NLN (≥27) in right-side colon cancer was independent of age, sex, CEA level, NLR, subgroups of stage III colon cancer, histology type and grade, and implementation of adjuvant chemotherapy after curative resection (RFS, hazard ratio [HR]: 0.613, 95% confidence interval [CI]: 0.463–0.812, P = 0.001; OS, HR: 0.626, 95% CI: 0.487–0.804, P < 0.001). Furthermore, a high number of NLN (≥12) in left-side colon cancer presented as an independent prognostic factor for RFS (HR: 0.705, 95% CI: 0.549–0.906, P = 0.006) and OS (HR: 0.655, 95% CI: 0.522–0.823, P < 0.001). A preoperative CEA level ≥ 5 ng/mL, a high number of NLN (≥27 in the right-side colon and ≥ 12 in the left-side colon), and TNM stage IIIC disease were three independent prognostic factors for RFS and OS in right-side and left-side stage III colon cancer.
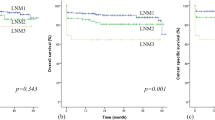
We further analyzed the effect of a high number of NLN on different subgroups of the whole stage III colon cancer, including stage IIIA, IIIB, and IIIC. Patients with a high number of NLN had significantly superior 5-year RFS and OS in stage IIIB (RFS: 77.0% vs. 68.0%, P = 0.001; OS: 78.6% vs. 67.9%, P < 0.001) and IIIC (RFS: 58.2% vs. 44.1%, P = 0.001; OS: 65.7% vs. 51.1%, P < 0.001) colon cancer (Fig. 4). In stage IIIA colon cancer, a high number of NLN showed survival benefit in only 5-year OS (91.5 vs. 89.8%, P = 0.041).

5-year relapse-fee survival (RFS) and 5-year overall survival (OS) for subgroup of stage III colon cancer, including stage IIIa, IIIb and IIIc. Kaplan-Meier curve was according to high NLN (NLN ≥12 in left-side colon or NLN ≥27 in right-side colon)
Discussions
In the present study, an increased number of NLN (≥27 and ≥ 12 for right-side and left-side colon cancer, respectively) was significantly associated with increased 5-year RFS and OS of stage III colon cancer. Subgroup analysis results for stage IIIA, IIIB, and IIIC colon cancer showed that a high number of NLN was not significantly prognostic in only 5-year RFS of stage IIIA colon cancer. In stage IIIB and IIIC colon cancer, patients with a high number of NLN had significantly superior 5-year RFS than did those with a low number of NLN. The similar results were also reported by Paul et al. and Quan et al. who have recommended that the role of NLN in survival prognosis was prominent in right-side colon, stage IIIB and IIIC disease [9, 19]. These findings may highlight the influence of host immune response at different tumor invasion levels. The effect of lymph nodes dissection on prognosis has been acknowledged in the past decade. Age, tumor size, and advanced T stage are independent factors affecting the number of ELNs in colon cancer [20]. Age < 65 years and deep tumor invasion may result in strong antigenic immune activity and a strong inflammatory response. Furthermore, in our data, a high number of NLN was significantly associated with age < 65 years and T3/T4 invasion level. Tekkis et al. suggested a positive association between increased ELN and patients’ immunologic reactions depending on their age [21]. In the preoperative clinical stage and postoperative pathological stage, the degree of difficulty in evaluating or harvesting lymph nodes is influenced by lymph node size. Therefore, reactive lymph nodes probably increase the number of ELN in standard curative surgery.
In stage III colon cancer, the NLN has been found to be a prognostic factor, like the metastatic lymph node ratio [7, 9, 19]. Moreover, this independent effect of NLN was even reported in overall survival of stage IV colon cancer [22]. In previous studies on colorectal cancer, only approximately 26 of 100 lymph nodes greater than 10 mm had metastatic cancer [14, 23], meaning that most large lymph nodes were not associated with cancer. Therefore, lymph node size and number may be crucial in anticancer immune response. Patterns of NLN for colorectal cancer, which include follicular, parafollicular, and sinus histiocytosis, were regarded to be predictors of host immunity and associated with an improved prognosis [24]. Large tumor size and deep invasion are thought to induce an antigenic effect; consequently, lymphatic hyperplasia may be commonly found in regional lymph nodes. A high lymphatic reaction may increase the likelihood of lymph node enlargement. If many reactive lymph nodes are in a patient’s surgical specimen, a higher number of NLN can be detached early or easily. Additionally, lymphocyte infiltration into the tumor margin and central part was shown to be high in patients with a high NLN. Crohn-like reaction, which was the discrete aggregation of lymphoid white blood cells, some with germinal centers and surrounding fibrosis, was commonly found around some colorectal adenocarcinomas in the absence of a clinical or pathological diagnosis of Crohn disease [22]. This mechanism can further explain the different effects of high NLN on different cancer stages of our present study. In more advanced stage III colon cancer, the importance of anticancer immune response could be highlighted more significantly. That was probably why the positive effect of increased NLN was more significant on 5-year RFS and OS in stage IIIB/IIIC disease than it was on survival in stage IIIA disease.
In the multivariate Cox proportional hazard model of the present study, the high number of NLN in left-side and right-side colon cancer was an independent prognostic factor for RFS and OS. The cancer-relapse risk decreased more with a high number of NLN in right-side colon cancer than in left-side colon cancer (38.7% vs. 29.5%). Generally, the prognosis of left-side colon cancer was excellent compared with right-side colon cancer, and this advantage might weaken the statistic power in NLN analysis. According to immune response theory, greater number of NLN indicated better host immune defense. In the present study, up to 95 and 89.1% right-side and left-side colon cancer, respectively, were stage IIIB/IIIC. Therefore, the prognostic value of high NLN probably was enhanced and highlighted in right-side stage III colon cancer. In the present study, we examined only stage III colon cancer without any emergent conditions, including perforation, obstruction, ischemia, and massive tumor bleeding to minimize the effect of acute inflammation. We considered that the status of NLN of stage III colon cancer could reflect the real prognostic role for RFS and OS. Therefore, both 5-year RFS and OS were higher in the present study than in other reports, and differences in inclusion and exclusion criteria might have influenced this difference [19, 25, 26]. Besides, the classification of NLN is usually debatable. Unlike the CEA level or TNM stage system, the cutoff value of NLN still lacks a uniform standard. Moreover, exploring reference data, such as a study for NLR from a big healthy population, is challenging [18]. The ROC analysis is usually used to find the most discriminative cutoff value in such studies, and different threshold values were noted in previous published data, including 9 [19] and 13 [9, 22]. Because the distribution of lymph nodes in the mesocolon varies according to colon cancer location, the number of lymph node harvest in colon cancer surgery is usually higher in the right-side than in the left-side colon [27]. The single-threshold value of NLN possibly did not present the potential difference in lymph node harvest, which could be associated with different colonic locations (e.g., proximal colon cancer vs. distal colon cancer), different curative procedures (e.g., right hemicolectomy vs. anterior resection), and age or sex. Therefore, different cutoff numbers of NLN were considered for right-side and left-side colon cancer in our analysis.
Our study has several limitations because of retrospective observation design. First, the coding error and case ascertainment might be possible even we tried to do it best. The retrospective studies always caused bias during data collection and enrollment. The second, although a bigger sample size and adequate follow-up time could be reached during a longer period of data collection, the interference of changes in the treatment strategy and staging system were also present during follow-up. The detailed effects of these changes could not be analyzed in the present study. Third, although we explained our result regarding host immune response in patients with high or low NLN, we did not have microscopic data to support our findings—for example, lymphocyte infiltration and densities of CD3+ and cytotoxic CD8+ T cells. This was a major limitation for our study. The fourth, as discussed above, the two optimal cutoff values of NLN for proximal and distal colon, namely 27 and 12, were determined by plotting the time-dependent ROC curve. The standard cutoff value of NLN was still difficult to establish through such studies. More studies for this issue will be needed in the future.
In addition to the aforementioned limitations, likely unmeasured confounding factors are present in this study. We did not have data regarding tumor molecular subtypes in the present study, including microsatellite instability-high (MSI/dMMR) tumors, RAS, and B-Raf (BRAF) gene mutations. MSI/dMMR occurs due to germline or somatic mutation, which was found in 15–25% of patients [28]. For colorectal cancer, compared with microsatellite stable status, the presence of MSI/dMMR equates to a better prognosis. The mechanism for this is likely associated with immune cell infiltration into the tumor microenvironment [29]. Although MSI/dMMR is a positive prognostic factor for stage II colon cancer after curative resection, the prognostic impact of MSI/dMMR status remains controversial in patients with stage III colon cancer who have received postoperative adjuvant chemotherapy [30,31,32]. In some conditions, for example, proximal colon cancer or adjuvant chemotherapy with multiple regimens, patients with stage III colon cancer and MSI/dMMR tumors who received oxaliplatin-based adjuvant chemotherapy had better survival outcomes [33, 34]. Moreover, the presence of BRAF status, which occurs in approximately 10% of colorectal cancer, has been considered a predictive marker in the survival of patients with metastatic colorectal cancer because the mutation status correlates with lower therapeutic response to chemotherapy with or without target agents [35]. To our knowledge, the findings concerning the prognostic impact of BRAF mutation in nonmetastatic colon cancer are inconsistent. In a pooled analysis for patients with stage III colon cancer after curative surgery, Taieb et al. noted that BRAF mutation was associated with a relatively short time to relapse, relatively short survival after relapse, and short OS in patients with microsatellite stable status. However, this condition was not noted in patients with MSI/dMMR tumors [36]. On the basis of our data, we could not determine the effect of mixing a good prognostic factor (MSI/dMMR status) and a bad one (BRAF mutation).
Conclusions
Our data suggested that the high NLN was a positive prognostic factor for stage III colon either in different tumor locations or in subgroups of stage III disease. In advanced stage III colon cancer, the importance of high NLN and their role in anticancer immune response could be highlighted.
Availability of data and materials
The data included in this study was never presented either as an oral or post presentation before. The raw data supporting our findings cannot be shared because the use of raw data was limited from previous IRB permit.
Abbreviations
- CRC:
-
Colorectal cancer
- TNM:
-
The tumor, node, and metastasis stage
- NLN:
-
Negative lymph node
- SEER:
-
the Surveillance, Epidemiology, and End Result program
- CEA:
-
Carcinoembryonic antigen
- OS:
-
Overall survival
- RFS:
-
Relapse-free survival
- ROC:
-
the time-dependent receiver operating characteristic
- ELN:
-
Examined lymph node
- PLN:
-
Positive lymph node
- NLR:
-
Neutrophil-to-lymphocyte ratio
- MSI/dMMR:
-
Microsatellite instability-high
- RAS:
-
from rat sarcoma virus, a family of related proteins that are expressed in all animal cell lineages and organs
- BRAF:
-
B-Raf
References
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424.
Sobin LH, Gospodarowicz MK, Wittekind C. TNM classification of malignant tumors, 7th edn. Chichester: Wiley; 2009.
Le Voyer TE, Sigurdson ER, Hanlon AL, Mayer RJ, Macdonald JS, Catalano PJ, et al. Colon cancer survival is associated with increasing number of lymph nodes analyzed: a secondary survey of intergroup trial INT-0089. J Clin Oncol. 2003;21(15):2912–9.
Vather R, Sammour T, Kahokehr A, Connolly AB, Hill AG. Lymph node evaluation and long-term survival in stage II and stage III colon cancer: a national study. Ann Surg Oncol. 2019;16(3):585–93.
Kotake K, Honjo S, Sugihara K, Hashiguchi Y, Kato T, Kodaira S, et al. Number of lymph nodes retrieved is an important determinant of survival of patients with stage II and stage III colorectal cancer. Jpn J Clin Oncol. 2012;42(1):29–35.
Shinto E, Ike H, Hida JI, Kobayashi H, Hashiguchi Y, Kajiwara Y, et al. Marked impact of tumor location on the appropriate cutoff values and the prognostic significance of the lymph node ratio in stage III colon cancer: a multi-institutional retrospective analysis. J Gastroenterol. 2019;54(7):597–607.
Berger AC, Sigurdson ER, LeVoyer T, Hanlon A, Mayer RJ, Macdonald JS, et al. Colon cancer survival is associated with decreasing ratio of metastatic to examined lymph nodes. J Clin Oncol. 2005;23(34):8706–12.
Chin CC, Wang JY, Yeh CY, Kuo YH, Huang WS, Yeh CH. Metastatic lymph node ratio is a more precise predictor of prognosis than number of lymph node metastases in stage III colon cancer. Int J Color Dis. 2009;24(11):1297–302.
Johnson PM, Porter GA, Ricciardi R, Baxter NN. Increasing negative lymph node count is independently associated with improved long-term survival in stage IIIB and IIIC colon cancer. J Clin Oncol. 2006;24(22):3570–5.
Pedrazzani C, Mantovani G, Fernandes E, Bagante F, Luca Salvagno G, Surci N, et al. Assessment of neutrophil-to-lymphocyte ratio, platelet-tolymphocyte ratio and platelet count as predictors of long-term outcome after R0 resection for colorectal cancer. Sci Rep. 2017;7(1):1494.
Gregory AD, Houghton AM. Tumor-associated neutrophils: new targets for cancer therapy. Cancer Res. 2011;71(7):2411–6.
Yin J, Markert JM, Leavenworth JW. Modulation of the Intratumoral immune landscape by oncolytic herpes simplex virus Virotherapy. Front Oncol. 2017;7:136.
Pagès F, Mlecnik B, Marliot F, Bindea G, Ou FS, Bifulco C, et al. International validation of the consensus Immunoscore for the classification of colon cancer: a prognostic and accuracy study. Lancet. 2018;391(10135):2128–39.
Märkl B, Rößle J, Arnholdt HM, Schaller T, Krammer I, Cacchi C, et al. The clinical significance of lymph node size in colon cancer. Mod Pathol. 2012;25(10):1413–22.
Märkl B, Schaller T, Kokot Y, Endhardt K, Kretsinger H, Hirschbühl K, et al. Lymph node size as a simple prognostic factor in node negative colon cancer and an alternative thesis to stage migration. Am J Surg. 2016;212(4):775–80.
Stanisavljević L, Søndenaa K, Storli KE, Leh S, Nesvik I, Gudlaugsson E, et al. The total number of lymph nodes in resected colon cancer specimens is affected by several factors but the lymph node ratio is independent of these. APMIS. 2014;122(6):490–8.
O'Connell MJ, Campbell ME, Goldberg RM, Grothey A, Seitz JF, Benedetti JK, et al. Survival following recurrence in stage II and III Colon Cancer: findings from the ACCENT data set. J Clin Oncol. 2008;26(14):2336–41.
Wu L, Zou S, Wang C, Tan X, Yu M. Neutrophil-to-lymphocyte and platelet-to-lymphocyte ratio in Chinese Han population from Chaoshan region in South China. BMC Cardiovasc Disorders. 2019;19:125.
Quan Q, Zhu M, Liu S, Chen P, He W, Huang Y, et al. Positive impact of the negative lymph node count on the survival rate of stage III colon cancer with pN1 and right-side disease. J Cancer. 2019;10(4):1052–9.
Tsai HL, Huang CW, Yeh YS, Ma CJ, Chen CW, Lu CY, et al. Factors affecting number of lymph nodes harvested and the impact of examining a minimum of 12 lymph nodes in stage I-III colorectal cancer patients: a retrospective single institution cohort study of 1167 consecutive patients. BMC Surg. 2016;16:17.
Tekkis P, Smith JJ, Heriot AG, Darzi AW, Thompson MR, Stamatakis JD, et al. A national study on lymph node retrieval in resectional surgery for colorectal cancer. Dis Colon Rectum. 2006;49:1673–83.
He WZ, Xie QK, Hu WM, Kong PF, Yang L, Yang YZ, et al. An increased number of negative lymph nodes is associated with a higher immune response and longer survival in colon cancer patients. Cancer Manag Res. 2018;10:1597–604.
Rössler O, Betge J, Harbaum L, Mrak K, Tschmelitsch J, Langner C. Tumor size, tumor location, and antitumor inflammatory response are associated with lymph node size in colorectal cancer patients. Mod Pathol. 2017;30:897–904.
Brynes RK, Hunter RL, Vellios F. Immunomorphologic changes in regional lymph nodes associated with cancer. Arch Pathol Lab Med. 1983;107:217–21.
Tsikitis VL, Larson DL, Wolff BG, Kennedy G, Diehl N, Qin R, et al. Survival in stage III colon cancer is independent of the total number of lymph nodes retrieved. J Am Coll Surg. 2009;208(1):42–7.
Wang J, Kulaylat M, Rockette H, Hassett J, Rajput A, Dunn KB, et al. Should total number of lymph nodes be used as a quality of care measure for stage III colon cancer? Ann Surg. 2009;249(4):559–63.
Bilimoria KY, Palis B, Stewart AK, Bentrem DJ, Freel AC, Sigurdson ER, et al. Impact of tumor location on nodal evaluation for colon cancer. Dis Colon Rectum. 2008;51:154–61.
Vogelaar FJ, Erning FNV, Reimers MS, Linden HV, Pruijt H, Brule AJCVD, et al. The prognostic value of microsatellite instability, KRAS, BRAF and PIK3CA mutations in stage II colon cancer patients. Mol Med. 2016;21(1):1038–46.
Deschoolmeester V, Baay M, Lardon F, Pauwels P, Peeters M. Immune cells in colorectal Cancer: prognostic relevance and role of MSI. Cancer Microenviron. 2011;4(3):377–92.
Ribic CM, Sargent DJ, Moore MJ, Thibodeau SN, French AJ, Goldberg RM, et al. Tumor microsatellite-instability status as a predictor of benefit from fluorouracil-based adjuvant chemotherapy for colon cancer. N Engl J Med. 2003;349:247–57.
Sargent DJ, Marsoni S, Monges G, Thibodeau SN, Labianca R, Hamiltonet SR, et al. Defective mismatch repair as a predictive marker for lack of efficacy of fluorouracil-based adjuvant therapy in colon cancer. J Clin Oncol. 2010;28:3219–26.
Samowitz WS, Curtin K, Ma KN, Schaffer D, Coleman LW, Leppert M, et al. Microsatellite instability in sporadic colon cancer is associated with an improved prognosis at the population level. Cancer Epidemiol Biomark Prev. 2001;10:917–23.
Sinicrope FA, Mahoney MR, Smyrk TC, Thibodeau SN, Warren RS, Bertagnolli MM, et al. Prognostic impact of deficient DNA mismatch repair in patients with stage III colon cancer from a randomized trial of FOLFOX-based adjuvant chemotherapy. J Clin Oncol. 2013;31:3664–72.
Shaib WL, Zakka KM, Jiang R, Yan M, Alese OB, Akce M, et al. Survival outcome of adjuvant chemotherapy in deficient mismatch repair stage III colon cancer. Cancer. 2020;126(18):4136–47.
De Roock W, Claes B, Bernasconi D, De Schutter J, Biesmans B, Fountzilas G, et al. Effects of KRAS, BRAF, NRAS, and PIK3CA mutations on the efficacy of cetuximab plus chemotherapy in chemotherapy-refractory metastatic colorectal cancer: a retrospective consortium analysis. Lancet Oncol. 2010;11(8):753–62.
Taieb J, Le Malicot K, Shi Q, Penault-Llorca F, Bouché O, Tabernero J, et al. Prognostic value of BRAF and KRAS mutations in MSI and MSS stage III colon cancer. J Natl Cancer Inst. 2016;109(5):djw272. https://doi.org/10.1093/jnci/djw272.
Acknowledgments
This manuscript was edited by Wallace Academic Editing. We also thank the Cancer Registry of the Chang Gung Medical Foundation for helping with data collection.
Code availability
Not applicable for this section.
Funding
No funding was received for this study.
Author information
Authors and Affiliations
Contributions
YHK and JFY had full access to all the data in the study and take responsibility for the integrity of the data and accuracy of the data analysis. Study concept and design: YHK and CCC. Acquisition of data: YHK, JFY, HYH, CCC and JMC. Drafting of the manuscript: YHK and HYH. Critical revision of the manuscript for important intellectual content: CCC and HYH. Statistical analysis: YHK and CHC. Administrative, technical, or material support: CCC. Study supervision: CCC and HYH. All authors have read the manuscript and approved the final draft submitted.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
We have to provide complete informed consent for every patient before he or she will undergo cancer treatment in our hospital. There was an appropriate waiver of IRB for this retrospective analysis. The IRB exempted us from the informed consent for patients’ participation in this study because our study was retrospective design for their survival data. Patients’ clinical and pathology data were collected prospectively into the tumor registry of division of colon and rectal surgery when patients received colorectal cancer treatment. We applied for the appropriate ethics approval for tumor registry and obtained it from the Institutional Review Board (IRB) of Chang Gung Memorial Hospital. The further follow-up data for survival were collected retrospectively according to medical record or interview.
Consent for publication
Not Applicable for this section.
Competing interests
All authors have declared no competing interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kuo, YH., You, JF., Hung, HY. et al. Number of negative lymph nodes with a positive impact on survival of stage III colon cancer; a retrospective observation study for right side and left side colon. BMC Cancer 22, 126 (2022). https://doi.org/10.1186/s12885-021-09154-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-021-09154-z