
Abstract
Background
The aim of the study was to investigate the risk of human papillomavirus (HPV) genotyping particularly vaccine genotypes and multiple infections for cervical precancer and cancer, which might contribute to developing genotype-specific screening strategy and assessing potential effects of HPV vaccine.
Methods
The HPV genotypes were identified using the Seq HPV assay on self-collected samples. Hierarchical ranking of each genotype was performed according to positive predictive value (PPV) for cervical intraepithelial neoplasia 2/3 or worse (CIN2+/CIN3+). Multivariate logistic regression model was used to estimate the odds ratios (ORs) with 95% confidence interval (CI) of CIN2+ according to multiplicity of types and vaccine types.
Results
A total of 2811 HPV-positive women were analyzed. The five dominant HPV genotypes in high-grade lesions were 16/58/52/33/18. The overall ranking orders were HPV16/33/35/58/31/68/18/ 56/52/66/51/59/45/39 for CIN2+ and HPV16/33/31/58/45/66/52/18/35/56/51/68/59/39 for CIN3+. The risks of single infection versus co-infections with other types lower in the hierarchy having CIN2+ were not statistically significant for HPV16 (multiple infection vs. single infection: OR = 0.8, 95%CI = 0.6-1.1, P = 0.144) or other genotypes (P > 0.0036) after conservative Bonferroni correction. Whether HPV16 was present or not, the risks of single infection versus multiple infection with any number (2, ≥2, or ≥ 3) of types for CIN2+ were not significantly different. In addition, HPV31/33/45/52/58 covered by nonavalent vaccine added 27.5% of CIN2, 23.0% of CIN3, and 12.5% of cancer to the HPV16/18 genotyping. These genotype-groups were at significantly higher risks than genotypes not covered by nonavalent vaccine. Moreover, genotypes covered by nonavalent vaccine contributed to 85.2% of CIN2 lesions, 97.9% of CIN3 and 93.8% of cancers.
Conclusions
Partial extended genotyping such as HPV33/31/58 but not multiplicity of HPV infections could serve as a promising triage for HPV-positive self-samples. Moreover, incidence rates of cervical cancer and precancer were substantial attributable to HPV genotypes covered by current nonavalent vaccination.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Cervical cancer is a common malignant disease that threatens the health of women, caused 311,365 deaths worldwide in 2018 [1]. Efforts should be attached to further reduce the burden of cervical disease and eventually achieve the goal of eliminating cervical cancer [2]. High-risk human papillomavirus (hrHPV) was found to be a necessary cause of cervical cancer [3], leading to the development of HPV-based screening and vaccine for cervical cancer prevention and control. Fortunately, many of HPV infections cause minor cytology abnormalities progress to cervical precancers, and only a subset of precancers become invasive cancers [4, 5]. Information on type-specific risks for cervical diseases may help monitor effectiveness of HPV vaccine, and may aid in the individualized triage plans, particularly for HPV-based screening on self-samples [6].
Although current US guidelines recommend HPV16/18 genotyping as a triage option in HPV-positive women [7], HPV16/18 genotyping fails to detect cervical lesions associated with other genotypes. Whether extended genotypes (hrHPV genotypes except for HPV16/18) should be considered for triage or not is still well worth investigating. Recently, we showed in a large study that 75.8% of abnormal cytology and 50.9% HSIL cytology were attributed to other hrHPV infection among HPV-positive women, and 62.7%/43.9% of CIN2/CIN3+ were caused by other hrHPV infection over 3-year follow-up [8]. Moreover, the introduction of vaccines could lead to the eradication of HPV16/18 [9,10,11], better understanding of extended genotyping provides information for establishing favorable screening policies following the introduction of vaccines [12].
Genotype-specific reports often include information about multiple infections (more than one types of HPV infection) with the application of full genotyping assays. To our knowledge, the role and mechanisms of HPV coinfection in cervical carcinogenesis are still not fully understood [13]. Coinfections were reported more likely to have cytologic abnormality than those with single infections [14]. However, the histologic correlation and clinical significance of multiple infections remain debatable [15, 16]. Additionally, estimating the impact of a vaccine is difficult due to the presence of multiple infections.
HPV vaccine is a powerful tool in cervical cancer prevention [17]. Although three HPV vaccines are available in mainland China, none of them has been incorporated into the National Immunization Program yet. In addition, the current vaccines do not protect against all hrHPV types. With the approval and development of HPV vaccine in China, there is an urgent need for extensive studies to clarify cervical carcinogenesis of full genotypes, and to predict the potential efficacy of available vaccines on the reduce of cervical lesions since the ultimate goal of the vaccine is not to prevent HPV infection, but to prevent the occurrence of cervical cancers and precancers.
HPV testing done with a clinically validated PCR-based assay had similar accuracy on self-samples and clinician-samples in our and other large clinical trials [18,19,20,21]. Thus, HPV self-sampling could be used as a primary screening approach in routine screening to increase screening coverage. Based on a large cervical screening program using SeqHPV assay on self-samples, this study was aimed to (a) assess distribution of HPV genotypes in different histologic grades, and determine risks of individual genotypes for detection of cervical diseases, (b) to investigate the role of multiple HPV infections, (c) to evaluate potential impacts of available vaccines by risk determination of HPV genotypes covered by current vaccines, thus providing a basis for HPV vaccine implementation and cervical screening strategy.
Methods
Study population and design
Between Nov 2018 and Dec 2019, we conducted a population-based cervical screening project using HPV testing on self-collected samples as the primary screening, which was well-organized at 12 counties in Henan Province, Central China, with 187,000 non-pregnant women aged 30-64 years being screened. Large-scale cervical screening program was not performed in the past 3 years in these counties. This cervical screening program spans 3 years. Of the total 187,000 from 12 counties in the large cervical cancer screening program, we selected 3 counties including 73,699 women to carry out this prospective observational study. The three counties are connected geographically, and the secondary screening strategy of these three adjacent counties was different from that of other counties. Thus, the current study was nested into this large cervical screening program, a total of 73,699 women who consented for participation via signature on registration website from three adjacent counties were enrolled into this study (Enrolled women). More details were reported in our recent published articles [22, 23].
The study protocol was conformed to the Declaration of Helsinki, and the digital informed consent was approved by the Institutional Ethics Committee of Peking University Shenzhen Hospital (PUSH, No. 2018035) and local institutions based on the prior approval from Institutional Ethics Committee of BGI-Shenzhen for the digital informed consent form and its signature manner. Information that could identify individual participant was fully anonymized during or after data collection. The current analysis focuses on women with complete data on HPV genotyping and biopsy-based histologic results from this large population.
Screening procedures
After successful registration for participation and information registration via the mobile device, eligible woman was asked to collect a cervicovaginal specimen with a cyto-brush by herself, following the instruction on a graph-text guide. Special instruction would be offered by the on-site provider if any woman had difficulty in understanding the sampling guide. The samples were rubbed on the solid media transport card (FTA card) by placing it in the middle of the application area and rolling it one full rotation, the self-collected samples were sent to the Center of BGI Health Clinical Laboratory, Wuhan, China for SeqHPV assay. Women with negative HPV result were advised to regular screening after 3 years, while those with positive HPV results were called back for triage and collected cervical samples with a cyto-brush before colposcopy or visual inspection under acetic acid (VIA) for p16INK4a immuno-cytology and liquid based cytology (LBC) test, LBC was used for research purpose but not patient care. Before referral of subjects with HPV-positive results for colposcopy, the study group from PUSH provided training of all the management protocol procedures for local gynecologists and pathologists. Women were referred for colposcopy/biopsy if they were: (a) positive of HPV16 and/or 18; (b) positive for both other types and VIA; or (c) other HPV-positive, VIA negative but abnormal of p16 staining (Fig. 1). Patients with pathological diagnosis of cervical intraepithelial neoplasia 2 or worse (CIN2+) were recommended to be treated according to the clinical diagnosis and treatment procedures of PUSH (Fig. 1).

Flowchart of the screening protocol. VIA, visual inspection under acetic acid; LBC, liquid-based cytology. Genotyping for HPV16/18, VIA, and p16 immunostaining were used for triage sequentially
HPV genotyping
All self-collected samples were prepared for SeqHPV assay (HPV genotyping based on sequencing, BGI Shenzhen, Shenzhen, China), an HPV genotyping assay using multiplex PCR and next generation sequencing [24]. The accuracy and reproducibility of Seq HPV assay for primary cervical cancer screening have been validated in SHENCCAST II [24] and CHIMUST [20] in comparison with the FDA-approved tests such as HC-2 and Cobas 4800 HPV assay. Moreover, SeqHPV assay has been approved by China Food and Drug Administration (CFDA). By designing a series of unique primers, the multiple index PCR system amplifies the approximately 150 bp of the HPV L1 gene with high-throughput capacities and type-specific output, and capable of processing greater than 4500 samples in 24 h [20, 24]. Seq HPV assay individually identifies 14 types of hrHPV (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68) and two types of low-risk HPV (lrHPV, HPV6 and 11).
Colposcopy-directed biopsy and histologic diagnoses
Colposcopy-directed biopsy was completed within 6 months after primary HPV screening according to a protocol modified from the quadrant-based Preventive Oncology International (POI) protocol [25]. According to the protocol, random biopsies would be taken at 2, 5, 8, and 11 o’clock for patients without visible lesion, while multiple biopsies would be taken at the VIA-indicated lesion site(s) plus the opposite quadrant of the transformation-zone for women with visible lesion(s). Histologic diagnoses were obtained according to the colposcopy-directed biopsy, and the highest diagnosis was recorded in women who had more than one tissue specimens (colposcopy orientation, random, or endocervical curettage). When it’s difficult to identify CIN2 and CIN3, p16 immunostaining was conducted. Histologic results were divided into normal (including cervicitis, and HPV infection without sign of CIN), CIN1, CIN2, CIN3 (including adenocarcinoma in situ, AIS), and cervical cancers (including squamous cell carcinoma, and adenocarcinoma). The slides were reviewed by pathologists of local hospital primarily and further confirmed by the senior gynecological pathologists from PUSH. Any discordant result between study pathologists and local pathologists was finalized by consensus review. Pathologists were blinded to LBC, p16, and HPV genotyping, but not to HPV positive outcome.
Statistical analysis
Biopsy-confirmed CIN2+ (including CIN2/3, AIS and cervical cancers) and CIN3+ (including CIN3, AIS and cervical cancers) were used as the study endpoints. CIN2+ is compared to normal and CIN1; CIN3+ is compared to normal + CIN1 + CIN2. The Mantel-Haenszel Chi-square test was carried out to investigate any linear trend in proportions. HPV6 and HPV11 are considered low vs. hrHPV. Positive predictive values (PPVs) for CIN2+/CIN3+ were calculated to estimate the risk of disease for each hrHPV genotype, and hierarchical rankings of hrHPV genotypes for CIN2+/CIN3+ were formed based on sequentially maximizing the PPV for the new genotype, each preceding genotype was excluded when calculating the risk of the subsequent genotype [11]. The model assumes that the risk of disease in subjects co-infected multiple genotypes is determined by the highest-risk genotype. Cumulative sensitivity and specificity for increasing numbers of genotypes ordered by the hierarchy were calculated.
Since CIN2+ (including CIN2/3 and cancers) is the threshold of clinical treatment and has a greater number than CIN3+, vaccine type groups were calculated according to genotypes ordered by the hierarchy for CIN2+. The risks of CIN2+ in relation to type groups covered by vaccines, and the risks of multiple infection versus single infection by individual type were assessed by using multiple logistic regression model. Odds ratios (ORs) with 95% confidence interval (CI) were adjusted for potential confounders such as age, screening sites, and HPV infection pattern (Indicating three infection categories, including lrHPV, hrHPV, and hrHPV+lrHPV). A prior study indicates that co-infection with lrHPV interferes with the rate of progression to cervical cancer [26], thus lrHPV was included into the analysis of ORs. P-values from multiple comparisons were adjusted by conservative Bonferroni correction. Both hierarchical and proportional attribution models were used for the estimation of vaccine coverage for histologic diagnosis [27, 28]. Analyses were conducted using SPSS software (IBM Corporation, version 24.0) and Stata/SE 15.1 software. All analyses were two-sided, P-value < 0.05 was considered statistically significant.
Results
Characteristics of study population and patients including
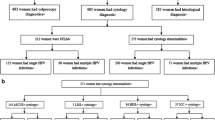
Overall, 7.95% (5843/73,537) and 7.62% (5600/73,537) women were detected to be HPV-positive and hrHPV-positive respectively, and 243 (0.33%) cases had “only lrHPV” infection (Fig. 2). A total of 3027 HPV positive women did not undergo colposcopy-directed biopsy, and 5 cases had an unsatisfactory histology were excluded. After excluding incomplete data, a total of 2811 women were eventually included in the analysis (Fig. 2). The median age of the study population was 48 years (range: 30 to 64 years). Among them, 2735 cases were hrHPV positive, and seventy-six cases had only lrHPV infection, and 2371 were diagnosed of ≤CIN1, 189 of CIN2, 235 of CIN3 (4 of AIS), and 16 of cancers (Table 1). The number of HPV types and that of hrHPV types were not associated with the severity of cervical lesions (HPV types, Ptrend = 0.625; hrHPV types, Ptrend = 0.803, Table 1).

Flow diagram of study population selection. HPV, human papillomavirus; lrHPV, low-risk HPV; hrHPV, high-risk HPV
Distribution of HPV genotypes and multiple HPV infection among different histologic grades
In 2811 HPV positive women, HPV16 (36.3%), HPV52 (13.8%), HPV18 (13.4%), HPV58 (12.9%), and HPV51 (8.4%) were the five most common genotypes. In women within CIN1, the 5 most prevalent hrHPV types were HPV16 (34.2%), HPV52 (15.4%), HPV58 (15.2%), HPV18 (13.3%), and HPV68 (8.6%); while HPV16 (63.4%), HPV58 (15.0%), HPV52 (10.3%), HPV33 (8.8%), and HPV18 (7.0%) were the dominant subtypes in the CIN2+ lesions (Fig. 3, Table S1). The prevalence of HPV16 was positively correlated with the severity of cervical lesions (30.7% in normal, 34.2% in CIN1, 63.4% in CIN2+, Ptrend < 0.0001). Similar results were found for HPV33 (4.3% in normal, 6.4% in CIN1, 8.8% in CIN2+, Ptrend < 0.0001). Distribution of multiple infections in women was as follows: 26.9% of multiple hrHPV infections in overall population (Fig. 3A), 25.3% in normal pathology, 32.2% in CIN1, and 29.3% in CIN2+, respectively (Fig. 3B-D). The proportions of each HPV type involved in multiple infections ranged from 1.0% for HPV11 to 12.6% for HPV16.

Prevalence of single and multiple infection among (A) all pathologic grades; (B) normal pathology; (C) CIN1; (D) CIN2+
Hierarchical classification for HPV genotypes and cumulative PPV/ sensitivity/ specificity for CIN2+/CIN3+
The risk determination of each genotype for detecting CIN2+ and CIN3+ was estimated by a hierarchical ranking of multiple infections, which resulted in similar hierarchies for CIN2+ and CIN3+. The overall ranking orders were HPV16, 33, 35, 58, 31, 68, 18, 56, 52, 66, 51, 59, 45 and 39 for CIN2+ (Table 2) and HPV16, 33, 31, 58, 45, 66, 52, 18, 35, 56, 51, 68, 59 and 39 for CIN3+ (Table 3). The PPV for CIN2+ was greatest for HPV16, being 27.4%. The PPV of HPV33 for CIN2+ was slightly lower at 26.0% univariately, and when multiple infections with HPV16 were excluded, it was 23.5%. Similar results were showed for CIN3+. HPV18 was ranked low in the 7th/8th place for CIN2+/CIN3+ respectively. Cumulative sensitivities and 1-specificities for CIN2+/CIN3+ as the number of hierarchical HPV types were sequentially increased are showed in Tables 2 and 3. The ROC curves for cumulative sensitivities and 1-specificities after adjusting for type hierarchy were plotted in Fig. S1, the areas under the ROC curves were 0.75 for CIN3+ and 0.71 for CIN2+ respectively.
Relative risk of multiple infection vs. single infection for CIN2+
When multiple infections were present, hrHPV type with the highest PPV within the hierarchy was used for each woman, the risk of multiple infections versus single infections for CIN2+ was not statistically significant for women infected with HPV16 (OR = 0.8, 95%CI = 0.6-1.1, p = 0.144). After excluding individuals coinfected with types higher in the hierarchy, the odds of multiple infections versus single infections having CIN2+ were not statistically significant for all the other genotypes after conservative Bonferroni correction (P > 0.0036, Table 4). Furthermore, we didn’t observe a significant OR of CIN2+ according to multiple infections versus single infections when HPV16 was present, with ORs of 1.1 (95%CI = 0.8-1.4), 0.9 (95%CI = 0.6-1.4) and 1.0 (95%CI = 0.8-1.3) for women infected with 2, ≥3, and ≥ 2 genotypes, respectively. Similar results were found when HPV16 was not present (Table 5).
Vaccine coverage and potential impact of vaccines
Table 3 shows the vaccine coverage of histologic abnormality assessed by the hierarchical or proportional attribution models. The hierarchical model showed that HPV6/11/16/18 covered by 4-valent vaccine potentially contributed to 57.7% of CIN2 lesions, 74.9% of CIN3 and 81.3% of cancers. While HPV6/11/16/18/31/33/45/52/58 covered by nonavalent vaccine was potentially responsible for 85.2% of CIN2 lesions, 97.9% of CIN3 and 93.8% of cancers. In addition, only 3 cases of CIN2 were attributed to lrHPV (Table 6). Similar results were found for the proportional model. Moreover, compared with HPV35/39/51/56/59/66/68 not covered by the nonavalent vaccine, HPV16/18 covered by all vaccines showed the highest risk for CIN2+, with a significant OR of 4.6 (95%CI = 3.2-6.7, P < 0.001), followed by HPV31/33/45/52/58 covered by the nonavalent vaccine with a significant OR of 2.5 (95%CI = 1.7-3.7, P < 0.001) (Table 5).
Discussion
HPV testing on self-samples is easily centralized through a dry transport card, and centralization reduces the overall cost of the laboratory equipment [29]. This cross-sectional study was conducted efficiently in a large-scale population and consumed only about half a year by using Seq HPV assay owing to its high-throughput capacity, high sensitivity, and low cost per case [24]. The successful implementation of cervical screening program based on HPV testing on self-samples provides a crucial guidance for the prevention and control of cervical cancer particularly in low-resource areas.
Due to the risk variation of different genotypes, information on cervical lesions conferred by specific genotypes is helpful for optimizing genotype-based screening strategy [12, 30]. However, the existence of multiple infections complicated type-specific risk assessment. In the current study, ranking of HPV types by PPVs provided similar hierarchies for CIN2+ and CIN3+, with HPV16/33 posing the greatest risk. Cuzick et al. reported a ranking based on PPVs for CIN3+ with HPV16/33 to be the highest ranks in a referral population [31]. Adcock et al. confirmed HPV16, 33, and 31 posing the greatest risks for precancers [6]. Notably, the risks of CIN2+/CIN3+ among women infected HPV18 were ranked low in the 7th/8th place. This is somewhat surprising but in line with mounting evidences [6, 32]. Despite the low risk of HPV18 in the study, detection of HPV18 in cervical cancers is second only to HPV16 in prior studies [13, 33].
To date, HPV16/18 genotyping has been well established as a triage tool for HPV-positive women in guidelines [7]. However, due to the low sensitivity of HPV16/18 as a triage relative to cytology triage [34], there is still an uncertainty regarding the extent to which adding hrHPV genotypes beyond HPV16/18 into the triage could enhance disease detection. Moreover, deciding which types to include in a triage strategy must weigh the absolute risk of cervical disease related to genotypes [35]. Both HPV31 and HPV58 ranked high for CIN2+/CIN3+, which is consistent with prior studies [36, 37]. Notably, detection of a specific genotype predicts risk of precancers, but cannot differentiate between a transient infection and detectable lesions [35]. Thus genotyping alone might not be accuracy enough to be the sole triage test [34], and the AUCs of genotypes were only 0.71 for CIN2+ and 0.75 for CIN3+. However, when present, HPV33/31/58 may be given a priority when deciding upon the need for immediate colposcopy similarly to HPV16, which reduces the follow-up burden. In addition, HPV39/59/51, ranked low both for CIN2+/CIN3+, may be considered as ‘intermediate risk’ types, which was similar to prior studies [6, 11, 12]. When present, HPV39/59/51 types, which did not appreciably contribute to relevant cervical lesions, might be permitted follow-up in 1 year with the expectation of viral clearance. For the remaining hrHPV types, information of other tests such as LBC or p16 immunocytology may be obtained for referring.
The findings above support the crucial role of extended genotyping in cervical screening [8], and provide evidence for the development of new technology for the detection of HPV types. In addition, this study was conducted at three counties in Henan Province, China with a shortage of cytologists. HPV genotypes are obtained automatically with HPV results, thus particularly useful for the settings where lack cytology results such as HPV-based screening on self-samples or at rural areas. Moreover, when the information on separate genotype is identified, more detailed management and appropriate follow-up strategies can be established at an earlier time for individuals according to genotypes.
In this study, multiple HPV infections were common with 26.9% found in overall study population. Numerous previous studies have reported similar results, ranging from 11.4 to 40.0% [6, 10, 32, 36]. Multiple HPV infection is attributed to certain factors, such as age, smoking, sexually activity, lifetime number of sexual partners, and immunodeficiency [10, 36]. Nevertheless, currently the impact of multiple infection on the risk of cervical lesions has not been established yet. Whether these infections occur by chance or as a result of interactions between HPV genotypes is still conflicting [10, 15]. Herrero et al. showed that co-infections may be associated with HPV persistence, and increase the duration of infection and the risk of cervical diseases [38]. Still overwhelming studies showed no impact [6, 15, 39]. Recently Iacobone et al. confirmed that HPV coinfections were significantly associated with lower risk of CIN2+, whereas single infections were more likely in cervical cancers and precancers [40]. Another study tested hrHPV by Cobas4800 assay showed that HPV16 co-infected with other types appeared to have a lower risk of CIN3+ than single HPV16 infection [16]. Although Cobas4800 assay has the ability to detect 14 types of hrHPV, it is impossible to distinguish the separate types except for HPV16/18. Therefore, hrHPV coinfection has not been fully and adequately explored, especially among the pool 12 types of hrHPV.
The current study, using a full genotyping assay-Seq HPV assay, revealed that women infected with HPV16 only had no significantly different risk for CIN2+ than those co-infected with HPV16 and other types. Similar results were found for the other genotypes excluding HPV16. However, data regarding the risk of CIN2+ associated with other genotypes excluding HPV16 should be interpreted with caution due to the either relatively low prevalence or the limited number of CIN2+ cases. Interestingly, the inclusion of coinfection with HPV types lower in the hierarchy added little to the risk prediction for CIN2+, possibly due to the fact that genotype with the highest PPV largely determines the risk in multiple infections and the impact of the additional genotypes is small [6]. Likewise, generally having a multiple infection conferred no additional risk for single HPV infection both in the presence or absence of HPV16, which was in accordance with a prior study [39]. But these findings must be interpreted cautiously and further confirmed via longitudinal studies, and the potential mechanisms warrant further investigation.
Updated evidence on coverage and carcinogenesis of vaccination genotypes is also essential for assessing potential impacts of HPV vaccines [13, 36], particularly in China prior to a National Immunization Program. In this study, HPV16/58/52/33/18/31 were the dominant genotypes in cervical precancers or cancers, which was consistent with prior studies [12, 41]. Moreover, hrHPV types covered by the nonavalent vaccine were associated with significantly higher risk for CIN2+ than hrHPV types not covered by the vaccine. Fortunately, similar to a worldwide study [42], most cervical cancers were potentially responsible for nonavalent vaccine in the study population. Notably, addition of HPV 6/11 did add only 3 cases of CIN2 but no CIN3+, hence cervical cancer screening may not include testing for lrHPV types. However, vaccine targeted HPV 6/11 prevents most of external genital wart cases [17].
Our findings may help healthcare authorities assess the impact of vaccination programs, providing a basis for the application of tailored HPV vaccines in Central China. Quadrivalent HPV vaccination was associated with a substantially reduced risk of invasive cervical cancer [43]. Huh et.al. reported that the nonavalent vaccine showed efficacy against cervical lesions related to HPV31/33/45/52/58 and similar efficacy toward HPV 6/11/16/18 as the 4-valent vaccine [17]. If our estimations are true, and high coverage vaccination can be implemented quickly, combined with the low proportion of cervical diseases and low risk of HPV types not covered by the nonavalent vaccine in the current study, vaccine intervention would achieve a great effect on prevention and eventual elimination of cervical cancer.
There are several limitations of this study. Firstly, the study population may not represent the general screening population. The selection of HPV-positive women who were referred for colposcopy was based on sequential indicators-HPV16/18, VIA, and p16 staining, not randomly, and management guidelines were not always followed by screen-positive women exactly. Additionally, there were no measures to check CIN2+ among those with HPV-negative results, thus the false negative rate is unknown. These facts reflecting a real-life situation in routine cervical screening programs rather than in a clinical trial. Another caveat is that HPV distribution according to cytological abnormalities wasn’t added since LBC was conducted on the p16 preservative liquid, which hasn’t been validated clinically yet; However, the association between genotypes and histologic abnormalities is more meaningful. In addition, we acknowledge that a cross-sectional data has limited power to predict the role of genotypes and multiple infections on disease progression or regression. Actually, the baseline disease detection in this study was comparable to what was detected in a longitudinal study [6]. Finally, the hierarchical and proportional attribution models used may not completely match the true causal assignment due to two major drawbacks [32]. First, they assume that every woman has a single lesion. Second, they may overestimate the effect of vaccination genotypes that are relatively common in the general population and coincidentally detected in lesions [27].
The strength of this study lies in the large sample size from a well-organized, population-based cervical screening program which ensures the strong statistical strength and enhances the suitability. Moreover, all enrolled women had a definite histologic diagnosis through colposcopy-directed biopsy, and the slides were verified by senior gynecological pathologists from PUSH, which ensures the accuracy and reliability of the outcomes. Histology diagnoses are well accepted as the gold standard for cervical diagnosis and best endpoint which could gain great implications in clinical practice [16]. Furthermore, primary HPV screening was completed at about 1 month, which eliminates the impact of time span on HPV prevalence. In addition, due to the prospective nature of this study, the missing results of Seq HPV assay or histology were minimized.
Conclusions
Genotyping by Seq HPV assay was valuable in improving risk stratification of HPV-positive self-samples, with HPV33/31/58 types ranked high risk and HPV39/59/51 types ranked low risk both for CIN2+/CIN3+. Coinfection with HPV types lower in the hierarchy conferred little to the risk for CIN2+ associated with single hrHPV infection. Moreover, incidence rates of cervical cancer and precancer were substantial attributable to HPV types covered by nonavalent vaccine. This study provides critical insights into vaccine strategies, and establishes the foundation for the development of genotype-specific screening approaches on self-samples, which is particularly useful for cervical screening in rural settings.
Availability of data and materials
The data that support the findings of this study are included in the manuscript, or available on request from the corresponding author.
Abbreviations
- CI:
-
Confidence interval
- CIN:
-
Cervical intraepithelial neoplasia
- CIN2+/CIN3 + :
-
CIN 2/3 or worse
- HPV:
-
Human papillomavirus
- hrHPV:
-
High-risk human papillomavirus
- LBC:
-
Liquid-based cytology
- OR:
-
Odds ratio
- PCR:
-
Polymerase chain reaction
- PPV:
-
Positive Predictive Value
- PUSH:
-
Peking University Shenzhen Hospital
- ROC:
-
Receiver operator characteristic
- HSIL:
-
High-grade Squamous Intraepithelial Lesion
- FTA:
-
Flinders Technology Associates
References
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424.
WHO. A cervical cancer-free future: First-ever global commitment to eliminate a cancer Https://www.Who.Int/News/Item/17-11-2020-A-Cervical-Cancer-Free-Future-First-Ever-Global-Commitment-To-Eliminate-A-Cancer.
Walboomers J, Jacobs M, Manos M, Bosch F, Kummer J, Shah K, et al. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J Pathol. 1999;189(1):12–9.
Schiffman M, Wentzensen N, Wacholder S, Kinney W, Gage JC, Castle PE. Human papillomavirus testing in the prevention of cervical cancer. J Natl Cancer Inst. 2011;103(5):368–83.
Kjaer SK, Frederiksen K, Munk C, Iftner T. Long-term absolute risk of cervical intraepithelial neoplasia grade 3 or worse following human papillomavirus infection: role of persistence. J Natl Cancer Inst. 2010;102(19):1478–88.
Adcock R, Cuzick J, Hunt WC, McDonald RM, Wheeler CM. Role of HPV genotype, multiple infections and viral load on the risk of high-grade cervical neoplasia. Cancer Epidemiol Biomark Prev. 2019;28(11):1816–24.
Huh WK, Ault KA, Chelmow D, Davey DD, Goulart RA, Garcia FA, et al. Use of primary high-risk human papillomavirus testing for cervical cancer screening: interim clinical guidance. Gynecol Oncol. 2015;136(2):178–82.
Song F, Du H, Xiao A, Wang C, Huang X, Liu Z, et al. Type-specific distribution of cervical hrHPV infection and the association with cytological and histological results in a large population-based cervical Cancer screening program: baseline and 3-year longitudinal data. J Cancer. 2020;11(20):6157–67.
Matsumoto K, Yaegashi N, Iwata T, Yamamoto K, Aoki Y, Okadome M, et al. Reduction in HPV16/18 prevalence among young women with high-grade cervical lesions following the Japanese HPV vaccination program. Cancer Sci. 2019;110(12):3811–20.
Chaturvedi AK, Katki HA, Hildesheim A, Rodríguez AC, Quint W, Schiffman M, et al. Human papillomavirus infection with multiple types: pattern of coinfection and risk of cervical disease. J Infect Dis. 2011;203(7):910–20.
Del Mistro A, Adcock R, Carozzi F, Gillio-Tos A, De Marco L, Girlando S, et al. Human papilloma virus genotyping for the cross-sectional and longitudinal probability of developing cervical intraepithelial neoplasia grade 2 or more. Int J Cancer. 2018;143(2):333–42.
Nygård M, Hansen B, Kjaer S, Hortlund M, Tryggvadóttir L, Munk C, et al. Human papillomavirus genotype-specific risks for cervical intraepithelial lesions. Hum Vaccin Immunotherapeutics. 2021;17(4):972–81.
Monsonego J, Cox JT, Behrens C, Sandri M, Franco EL, Yap PS, et al. Prevalence of high-risk human papilloma virus genotypes and associated risk of cervical precancerous lesions in a large U.S. screening population: data from the ATHENA trial. Gynecol Oncol. 2015;137(1):47–54.
Dickson EL, Vogel RI, Geller MA, Downs LS. Cervical cytology and multiple type HPV infection: a study of 8182 women ages 31-65. Gynecol Oncol. 2014;133(3):405–8.
Schmitt M, Depuydt C, Benoy I, Bogers J, Antoine J, Arbyn M, et al. Multiple human papillomavirus infections with high viral loads are associated with cervical lesions but do not differentiate grades of cervical abnormalities. J Clin Microbiol. 2013;51(5):1458–64.
Wu P, Xiong H, Yang M, Li L, Wu P, Lazare C, et al. Co-infections of HPV16/18 with other high-risk HPV types and the risk of cervical carcinogenesis: a large population-based study. Gynecol Oncol. 2019;155(3):436–43.
Huh WK, Joura EA, Giuliano AR, Iversen OE, de Andrade RP, Ault KA, et al. Final efficacy, immunogenicity, and safety analyses of a nine-valent human papillomavirus vaccine in women aged 16-26 years: a randomised, double-blind trial. Lancet. 2017;390(10108):2143–59.
Polman NJ, Ebisch RMF, Heideman DAM, Melchers WJG, Bekkers RLM, Molijn AC, et al. Performance of human papillomavirus testing on self-collected versus clinician-collected samples for the detection of cervical intraepithelial neoplasia of grade 2 or worse: a randomised, paired screen-positive, non-inferiority trial. Lancet Oncol. 2019;20(2):229–38.
Belinson JL, Wang G, Qu X, Du H, Shen J, Xu J, et al. The development and evaluation of a community based model for cervical cancer screening based on self-sampling. Gynecol Oncol. 2014;132(3):636–42.
Du H, Duan X, Liu Y, Shi B, Zhang W, Wang C, et al. Evaluation of Cobas HPV and SeqHPV assays in the Chinese multicenter screening trial. J Low Genit Tract Dis. 2021;25(1):22–6.
Song F, Du H, Wang C, Huang X, Wu R. The effectiveness of HPV16 and HPV18 genotyping and cytology with different thresholds for the triage of human papillomavirus-based screening on self-collected samples. PLoS One. 2020;15(6):e0234518.
Song F, Belinson JL, Yan P, Huang X, Wang C, Hui D, et al. Wu R: Evaluation of p16INK4a immunocytology and human papillomavirus (HPV) genotyping triage after primary HPV cervical cancer screening on self-samples in China. Gynecol Oncol. 2021;162(2):322–30.
Song F, Yan P, Huang X, Wang C, Qu X, Du H, et al. Triaging HPV-positive, cytology-negative cervical cancer screening results with extended HPV genotyping and p16(INK4a) immunostaining in China. BMC Infect Dis. 2021;21(1):400.
Yi X, Zou J, Xu J, Liu T, Liu T, Hua S, et al. Development and validation of a new HPV genotyping assay based on next-generation sequencing. Am J Clin Pathol. 2014;141(6):796–804.
Belinson JL, Pretorius RG. A standard protocol for the colposcopy exam. J Low Genit Tract Dis. 2016;20(4):e61–2.
Sundstrom K, Ploner A, Arnheim-Dahlstrom L, Eloranta S, Palmgren J, Adami HO, et al. Interactions between high- and low-risk HPV types reduce the risk of squamous cervical Cancer. J Natl Cancer Inst. 2015;107(10):djv185.
Venetianer R, Clarke MA, van der Marel J, Tota J, Schiffman M, Dunn ST, et al. Identification of HPV genotypes causing cervical pre-Cancer using tissue-based genotyping. Int J Cancer. 2020;146(10):2836–44.
Cornall A, Brotherton J, Callegari E, Tan F, Saville M, Pyman J, et al. Assessment of attribution algorithms for resolving CIN3-related HPV genotype prevalence in mixed-genotype biopsy specimens using laser capture microdissection as the reference standard. Vaccine. 2020;38(40):6312–9.
Belinson J, Qiao YL, Pretorius R, Zhang WH, Elson P, Li L, et al. Shanxi Province cervical Cancer screening study: a cross-sectional comparative trial of multiple techniques to detect cervical neoplasia. Gynecol Oncol. 2001;83(2):439–44.
Demarco M, Egemen D, Raine-Bennett TR, Cheung LC, Befano B, Poitras NE, et al. A study of partial human papillomavirus genotyping in support of the 2019 ASCCP risk-based management consensus guidelines. J Low Genit Tract Dis. 2020;24(2):144–7.
Cuzick J, Ho L, Terry G, Kleeman M, Giddings M, Austin J, et al. Individual detection of 14 high risk human papilloma virus genotypes by the PapType test for the prediction of high grade cervical lesions. J Clin Virol. 2014;60(1):44–9.
Zhao S, Zhao X, Hu S, Lu J, Duan X, Zhang X, et al. Distribution of high-risk human papillomavirus genotype prevalence and attribution to cervical precancerous lesions in rural North China. Chin J Cancer Res. 2019;31(4):663–72.
Sanjose S. Quint WGV, Alemany L, Geraets DT, Klaustermeier JE, Lloveras B, Tous S, Felix a: human papillomavirus genotype attribution in invasive cervical cancer a retrospective cross-sectional worldwide study. Lancet Oncol. 2010;11(11):1048–56.
Stoler MH, Baker E, Boyle S, Aslam S, Ridder R, Huh WK, et al. Approaches to triage optimization in HPV primary screening: extended genotyping and p16/Ki-67 dual-stained cytology - retrospective insights from ATHENA. Int J Cancer. 2019;146(9):2599–607.
Cuschieri K, Ronco G, Lorincz A, Smith L, Ogilvie G, Mirabello L, et al. Eurogin roadmap 2017: triage strategies for the management of HPV-positive women in cervical screening programs. Int J Cancer. 2018;143(4):735–45.
So KA, Lee IH, Lee KH, Hong SR, Kim YJ, Seo HH, et al. Human papillomavirus genotype-specifc risk in cervical carcinogenesis. J Gynecol Oncol. 2019;30(4):e52.
Zhao XL, Hu SY, Zhang Q, Dong L, Feng RM, Han R, et al. High-risk human papillomavirus genotype distribution and attribution to cervical cancer and precancerous lesions in a rural Chinese population. J Gynecol Oncol. 2017;28(4):e30.
Herrero R, Castle PE, Schiffman M, Bratti MC, Hildesheim A, Morales J, et al. Epidemiologic profile of type-specific human papillomavirus infection and cervical neoplasia in Guanacaste, Costa Rica. J Infect Dis. 2005;191(11):1796–807.
Wentzensen N, Schiffman M, Dunn T, Zuna RE, Gold MA, Allen RA, et al. Multiple human papillomavirus genotype infections in cervical cancer progression in the study to understand cervical cancer early endpoints and determinants. Int J Cancer. 2009;125(9):2151–8.
Iacobone AD, Bottari F, Radice D, Preti EP, Franchi D, Vidal Urbinati AM, et al. Distribution of high-risk human papillomavirus genotypes and multiple infections in Preneoplastic and neoplastic cervical lesions of unvaccinated women. J Low Genit Tract Dis. 2019;23(4):259–64.
Sundström K, Dillner J. How many human papillomavirus types do we need to screen for? J Infect Dis. 2021;223(9):1510–11.
Serrano B, Alemany L, Tous S, Bruni L, Clifford GM, Weiss T, et al. Potential impact of a nine-valent vaccine in human papillomavirus related cervical disease. Infect Agent Cancer. 2012;7(1):38.
Lei J, Ploner A, Elfström K, Wang J, Roth A, Fang F, et al. HPV vaccination and the risk of invasive cervical Cancer. N Engl J Med. 2020;383(14):1340–8.
Acknowledgments
We would like to appreciate clinical and laboratory personnel participated in this cervical cancer screening project at PUSH and local hospitals in Henan Province, China, and all the women participated in this study.
Funding
The work was supported by Shenzhen High-level Hospital Construction Fund (No. YBH2019-260); Shenzhen Key Medical Discipline Construction Fund (No. SZXK027); Sanming Project of Medicine in Shenzhen (No. SZSM202011016). No funders were involved in the design and conduct of the study; data collection, analysis, and interpretation; and preparation of the manuscript or decision to submit the article for publication.
Author information
Authors and Affiliations
Contributions
RFW, XFQ and HD were responsible for conception, design and quality control of this study. FBS and PSY conducted data curation, analyzed and interpreted the data, and were major contributor in writing the manuscript. XH and CW participated in investigation and statistical analysis. RFW, XFQ and HD reviewed and edited the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Institutional Ethics Committee of Peking University Shenzhen Hospital (PUSH, No.2018035). The study protocol was conformed to the Declaration of Helsinki, and the digital informed consent was approved by the Institutional Ethics Committee of PUSH (No. 2018035) and local institutions based on the prior approval from Institutional Ethics Committee of BGI-Shenzhen for the digital informed consent form and its signature manner. Digital informed consent was obtained from all participants including consent for publication.
Consent for publication
Digital informed consent was obtained from all participants including consent for publication.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Song, F., Yan, P., Huang, X. et al. Roles of extended human papillomavirus genotyping and multiple infections in early detection of cervical precancer and cancer and HPV vaccination. BMC Cancer 22, 42 (2022). https://doi.org/10.1186/s12885-021-09126-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-021-09126-3