
Abstract
Background
Not all patients with unresectable hepatocellular carcinoma (uHCC) benefit from treatment with immune checkpoint inhibitors and molecular-targeted agents. The aim of this retrospective study was to assess the efficacy and safety of pembrolizumab plus lenvatinib plus hepatic arterial infusion chemotherapy (HAIC) versus pembrolizumab plus lenvatinib in selected populations of patients with treatment-naive uHCC exhibiting programmed cell death ligand-1 (PD-L1) staining.
Methods
Consecutive patients with treatment-naive uHCC exhibiting PD-L1 staining who were treated with pembrolizumab plus lenvatinib plus HAIC (PLH) or pembrolizumab plus lenvatinib (PL) were retrospectively identified from our medical centres from 2018 to 2021. HAIC involved oxaliplatin, fluorouracil, and leucovorin (FOLFOX). Follow-up occurred every 3 weeks for 1 year and then every 6 weeks thereafter. The primary endpoints included overall survival (OS) and progression-free survival (PFS). Secondary endpoints were the frequency of key adverse events (AEs).
Results
In total, 248 treatment-naive patients were retrospectively reviewed, 78 of whom were ineligible on the basis of the current criteria. Thus, 170 patients (PLH: n = 84, median age 52 years [range, 42–67]; PL: n = 86, 53 years [range, 43–69]) were eligible for the analysis. The median follow-up was 18.6 months (range, 1–26). At the final follow-up, the median OS was 17.7 months (95% confidence interval [CI], 15.2–18.3) in the PLH group versus 12.6 months (95% CI, 11.1–13.7) in the PL group (hazard ratio [HR] 0.52; 95% CI, 0.36–0.75; p = 0.001). A significant difference was also detected in the median PFS (10.9 months [95% CI, 8.7–11.4] for PLH vs. 6.8 months (95% CI, 5.2–7.4) for PL; HR 0.61, 95% CI, 0.43–0.85; p = 0.001). Significant differences in the rate of the key AEs were noted between groups (79.8% for PLH vs. 62.8% for PL, p = 0.015), but these AEs were controllable.
Conclusions
Among selected populations of patients with treatment-naive uHCC exhibiting PD-L1 staining, the PLH regimen may substantially improve the survival benefits compared with the PL regimen with a controllable safety profile.
Similar content being viewed by others


Background
Hepatocellular carcinoma (HCC) accounts for approximately 90% of all primary liver cancers and is the 4th leading cause of cancer-related death [1]. In China, HCC is primarily attributed to chronic inflammation resulting from hepatitis B virus infection [2]. Most patients are newly diagnosed with unresectable disease. Thus, treatment options are limited, and the prognosis is poor [2, 3]. The management of uHCC with inherent “immune escape” remains controversial [3, 4]. Several regimens [5,6,7,8] have been revealed to improve the survival of patients with uHCC. However, based on previously routine radiotherapy and/or chemotherapy, the majority of these patients exhibit a poor prognosis and ultimately die from uHCC within 1–2 years, resulting in a push for the development of other feasible therapies [9, 10].
uHCC tends to be characterized by intrinsic immunosuppression and overexpression of immune checkpoints, which mainly involve the programmed death 1 (PD-1) pathway and the cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) pathway [11, 12]. Although the management of uHCC is precipitously evolving with numerous new therapeutic options, immunotherapy still plays a key role even in combination regimens [13,14,15]. Importantly, PD-1 pathway blockade with immune checkpoint inhibitors has emerged as a promising option to potentially delay the progression of tumours and improve survival benefit [16, 17]. Pembrolizumab, a highly selective IgG4-kappa humanized monoclonal antibody against the PD-1 receptor, can release the antitumour activity of pre-existing tumour-specific T-cell immunity and has been approved as a second-line agent for uHCC patients who cannot tolerate or experience disease progression during or following treatment with drugs targeting the Raf/Mek/Erk pathway on the basis of the Keynote-224 trial [12]. The immunomodulatory effect of lenvatinib (a receptor tyrosine kinase inhibitor) on tumour microenvironments might contribute to antitumour activity when combined with PD-1 signalling inhibitors in HCC [18, 19]. Combining pembrolizumab with a lenvatinib regimen for uHCC has been reported in a multicentre, open-label trial [16] of 104 patients with uHCC that assessed the clinical outcomes of pembrolizumab plus lenvatinib. In this trial, the median overall survival (OS) and median progression-free survival (PFS) were 22 months and 8.6 months, respectively. Grade ≥ 5 adverse events (AEs) occurred in 3% of patients. Their conclusion revealed that the combination has promising antitumour activity in uHCC with an anticipated safety profile.
Although pembrolizumab plus lenvatinib has been demonstrated to improve survival benefits for patients with uHCC, the regimen of pembrolizumab plus lenvatinib in combination with hepatic arterial infusion chemotherapy (HAIC) is not commonly employed in uHCC. Whether the incorporation of HAIC into pembrolizumab plus lenvatinib results in improved survival in patients with uHCC remains an open question to date; however, the efficacy of HAIC has been the focus of debate due to high response rates and encouraging survival rates for uHCC patients [20]. Furthermore, given that pembrolizumab represents diverse anticancer activities for a subset of uHCC [21], the need to stratify patients based on PD-1 expression status and the actual antitumour efficacy of pembrolizumab plus lenvatinib plus HAIC, even in a biomarker-selected HCC setting, has not been evaluated. In this study, we performed a multicentre retrospective study to assess the efficacy and safety of pembrolizumab plus lenvatinib plus HAIC versus pembrolizumab plus lenvatinib in selected populations of patients with treatment-naive uHCC exhibiting programmed death ligand 1 (PD-L1) staining.
Methods
Data
Consecutive patients with treatment-naive uHCC whose tumours expressed PD-L1 and who initially underwent the pembrolizumab plus lenvatinib plus HAIC (PLH) or pembrolizumab plus lenvatinib (PL) regimen from March 1, 2018, to March 31, 2021, for whom baseline data were available, were retrospectively identified from the First Affiliated Hospital, Sun Yat-sen University, the Sun Yat-sen Memorial Hospital of Sun Yat-san University, Henan Provincial Tumor Hospital, the Affiliated Cancer Hospital of Zhengzhou University and Zhongshan Hospital, Fudan University. A review of the patient’s medical records was executed independently by the four authors (B X, Pf W, Zy Land Xy H) to extract endpoint data. Inclusion criteria were as follows: imaging and/or histologically confirmed HCC; an HCC classification of Barcelona Clinic Liver Cancer (BCLC) B or C; unresectable evaluated by two or more experienced surgical specialists; Child-Pugh A or B; PD-L1 expression staining (combined positive score [CPS] ≥1) as determined by an FDA-approved test; PD-L1 expression was assessed using the PD-L1 IHC 22C3 pharmDx assay (Agilent Technologies) [16]; Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1; at least one measurable target lesion by the modified Response Evaluation Criteria in Solid Tumours (mRECIST); anti-HBV therapy was required; and appropriate bone marrow function. Major exclusion criteria involved absent baseline data; previous agent(s) targeting T-cell costimulation or checkpoint pathways; no evaluable CPS; previous tumour-related interventions (such as hormonal therapy, chemotherapy, radiofrequency ablation, radiotherapy, microwave coagulation therapy, or surgery); discontinuation of PLH or LH, irrespective of drug-related AEs; cachexia; severe medical system diseases (such as systemic inflammatory response syndrome, hepatic encephalopathy, stubborn anaemia, or abnormal blood coagulation); surgical emergency (such as intestinal obstruction, intestinal perforation, or gastrointestinal haemorrhage); multiple organ dysfunction syndrome; other malignant tumours; and psychosis.
Study design and treatment
A retrospective multicentre study was conducted in which eligible patients had received either the PLH or PL regimen for the treatment of uHCC exhibiting PD-L1 expression staining. The decision to manage using PLH or PL was made by medical experts on a case-by-case basis. In the PLH group, patients were administered 200 mg pembrolizumab intravenously once every 3 weeks [12] and 8–12 mg lenvatinib once daily orally [22] followed by HAIC every 3 weeks. HAIC consisted of 85 mg/m2 oxaliplatin from hour 0 to 2 on day 1; 400 mg/m2 fluorouracil bolus at hour 3 and 2400 mg/m2 fluorouracil over 46 h on days 1 and 2; and 400 mg/m2 leucovorin from hour 2 to 3 on day 1 as reported by He et al. [8]. In the PL group, patients were administered 200 mg pembrolizumab intravenously once every 3 weeks and 8–12 mg lenvatinib once daily orally. Treatment was continued until disease progression, intolerable toxicity, withdrawal, or death.
Outcomes and assessments
The primary endpoints were OS and PFS. OS was defined as the time of initiation of medication to death from any cause, and PFS, defined as the time of initiation of medication to disease progression or death from any cause, whichever came first. Tumour response was assessed in accordance with RECIST version 1.1 and mRECIST per independent imaging review. Analysis of patterns of response was performed based on computed tomography (CT) or magnetic resonance imaging (MRI). The diagnosis of extrahepatic metastasis was primarily based on CT or MRI. In some cases, the diagnosis of extrahepatic metastasis was based on positron emission tomography-CT (PET-CT). Secondary endpoints were the rate of major AEs that were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.03. The major AE evaluations were performed continuously throughout the follow-up period. Information regarding these AEs was collected from the time of initiation of PLH or PL therapy. PD-L1 expression was analysed using immunohistochemistry. The measurement of tumour PD-L1 expression staining was consistent with a previous description [11]. Follow-up was performed every 3 weeks for 1 year and then every 6 weeks thereafter to monitor endpoint parameters until disease progression, intolerable AEs, or death. CT or MRI was performed every 6 weeks. Additional follow-up was permitted when clinically indicated.
Statistical analysis
Normally distributed continuous variables were compared by t-test, and abnormally distributed continuous variables were compared using the Mann-Whitney U test. Categorical variables were compared by Pearson’s χ2 test or Fisher’s exact test. Survival was estimated using the Kaplan-Meier method with a log-rank test. All variables with p < 0.05 in univariate analyses were incorporated into multivariate analyses. Univariate and multivariate analyses were performed using the Cox proportional hazards model. Here, age, ECOG performance status, HCC aetiology, Child-Pugh A or B, Albumin–Bilirubin (ALBI) grade (1/> 1), liver cirrhosis, PD-L1 expression, tumour thrombus, extrahepatic metastasis, and number of metastatic sites were used as covariates, and intervention served as the time-dependent factor. The median follow-up was calculated using the reverse Kaplan-Meier method. A two-tailed p-value of < 0.05 was used as a threshold for significance. Statistical analyses were performed primarily using SPSS 26.0 (IBM, Inc., NY). The survival curves for both groups were outlined using GraphPad Prism 8.0 (La Jolla, California, USA).
Results
Demographic characteristics
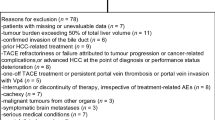
We identified 248 consecutive patients with treatment-naive uHCC exhibiting PD-L1 staining who underwent the PLH or PL regimen, of whom 78 were excluded based on the current criteria. Finally, a total of 170 patients who met the criteria were included in the study, of whom 84 received the PLH regimen and 86 received the PL regimen, as presented in Fig. 1. Table 1 summarizes the patient’s clinical characteristics. The median age was 52 years (range, 42–67) in the PLH group and 53 years (range, 43–69) in the PL group. BCLC status was B in 26.2% and C in 73.8% of patients receiving PLH versus B in 24.4% and C in 75.6% of patients receiving PL (p = 0.791). The PD-L1 CPS was 1–20 in 50.0%, 20–50 in 32.1%, and 50–100 in 17.9% of patients receiving PLH versus 1–20 in 52.3%, 20–50 in 27.9%, and 50–100 in 19.8% of patients receiving PL (p = 0.906). Absent tumour thrombus, branch of portal vein thrombus, and main portal vein thrombus were 41.7%, 38.142.8%, and 36.9%15.5% in the PLH group versus 36.0%, 43.051.2%, and 33.7%12.8% in the PL group, respectively (p = 0.695). The two cohorts were well balanced in the present study. The duration of drugs was 15 months (range, 1–33) in the PLH group and 12 months (range, 2–33) in the PL group. The median number of treatment cycles was 25 (range, 1–36) for patients undergoing PLH and 17 (range, 1–37) for those who underwent PL.

Flow diagram exhibiting the methods applied to identify objects to assess the efficacy and safety of pembrolizumab plus lenvatinib plus hepatic arterial infusion chemotherapy (HAIC) versus pembrolizumab plus lenvatinib in selected populations of patients with treatment-naive uHCC exhibiting programmed cell death ligand-1 (PD-L1) staining
Efficacy
The median follow-up was 18.6 months (range, 1–26). Tumour response in patients experiencing PLH or PL were showed in Table 2. Between-group remarkable distinctions were detected in objective response rate (ORR) (all p < 0.05). In the PLH group, ORR was 46.4% (95% CI, 29.3–54.6%) by RECIST version 1.1 and 59.5% (95% CI, 42.7–58.7%) by mRECIST. In the PL group, ORR was 30.2% (95% CI, 22.5–44.7%) by RECIST version 1.1 and 41.9% (95% CI, 33.7–57.1%) by mRECIST. At the final follow-up, 121 (71.2%) deaths occurred (53 [63.1%] PLH-treated patients vs. 68 [79.1%] PL-treated patients). The 3-, 6-, and 12-month OS rates were 92.7, 86.5, and 64.7%, respectively, in PLH-treated patients and 92.9, 81.9, and 51.3%, respectively, in PL-treated patients. A borderline significant distinction was observed in the median OS between the two cohorts (17.7 months [95% CI, 15.2–18.3] in the PLH-treated cohort vs. 12.6 months [95% CI, 11.1–13.7] in the PL-treated cohort), as shown in Fig. 2. PLH had a remarkable improvement in the median OS compared with PL, and PLH might be associated with a significant 48% lower risk of death than PLH (HR 0.52, 95% CI, 0.36–0.75; p = 0.001). A noteworthy difference of 5.1 months in the median OS was noted, and the superiority of PLH over PL tended to be positive, as the separation of the two curves continued until the final follow-up. Moreover, a distinct dissimilarity in the median PFS between the two cohorts was observed (10.9 months [95% CI, 8.7–11.4] in the PLH-treated cohort vs. 6.8 months [95% CI, 5.2–7.4] in the PL-treated cohort [HR 0.61, 95% CI, 0.43–0.85; p = 0.001]), as shown in Fig. 3. Of the 170 patients, treatment interruption occurred in 23 (13.5%) patients mainly due to tumour progression (17 of 84 patients in the PLH-treated cohort vs. 6 of 86 patients in the PL-treated cohort, p = 0.026). Although more cases suffered tumour progression in the PLH-treated cohort, a remarkable delay was observed in the time interval for tumours to progress in this cohort, which may be associated with the significantly longer PFS.

Kaplan-Meier curves for overall survival. The median overall survival was 17.7 months (95% confidence interval [CI], 15.2–18.3) for PLH and 12.6 months (95% CI, 11.1–13.7) for PL (HR 0.52, 95%CI, 0.36–0.75; p = 0.001). *The hazard ratio was calculated using a Cox proportional hazards model, with the age, ECOG performance status, time since diagnosis, HCC aetiology, Child-Pugh A or B, Liver cirrhosis, PD-L1 expression, tumor thrombus, central nervous system metastasis, and number of metastatic sites used as covariates and therapy as the time-dependent factor

Kaplan-Meier curves for progression-free survival. The median progression-free survival was 10.9 months (95% confidence interval [CI], 8.7–11.4) for PLH and 6.8 months (95% CI, 5.2–7.4) for PL (HR 0.61, 95%CI, 0.43–0.85; p = 0.001). *The hazard ratio was calculated using a Cox proportional hazards model, with the age, ECOG performance status, time since diagnosis, HCC aetiology, Child-Pugh A or B, Liver cirrhosis, PD-L1 expression, tumor thrombus, central nervous system metastasis, and number of metastatic sites used as covariates and therapy as the time-dependent factor
For patients with BCLC (B), median OS was 17.8 months (95% CI, 16.4–18.9) for PLH and 14.4 months (95% CI, 12.8–15.9) for PL (HR 0.61, 95%CI, 0.26–1.43; p = 0.359); median PFS was 13.5 months (95%CI, 12.1–14.7) for PLH and 8.4 months (95% CI, 7.6–9.5) for PL (HR 0.55, 95%CI, 0.22–1.35; p = 0.004) (Fig. 4). For patients with BCLC (C), median OS was 17.6 months (95% CI, 15.9–18.6) for PLH and 11.8 months (95% CI, 10.4–12.7) for PL (HR 0.47, 95%CI, 0.31–0.71; p = 0.007); median PFS was 8.9 months (95% CI, 7.3–9.8) for PLH and 6.7 months (95% CI, 5.4–7.6) for PL (HR 0.64, 95%CI, 0.44–0.94; p = 0.027) (Fig. 5).

Kaplan-Meier curves for subgroup analysis in selected populations of treatment-naive advanced HCC patients with Barcelona Clinic Liver Cancer B between groups

Kaplan-Meier curves for subgroup analysis in selected populations of treatment-naive advanced HCC patients with Barcelona Clinic Liver Cancer C between groups
We performed a subgroup comparison based on the CPS scores. For patients with PD-L1 CPS ≥50, the median OS was 18.1 months in the PLH-treated cohort compared with 13.3 months in the PL-treated cohort (HR 0.75; p = 0.003). For patients with PD-L1 CPS ≥20, the median OS was 17.5 months in the PLH-treated cohort compared with 12.2 months in the PL-treated cohort (HR 0.26; p = 0.002). For patients with PD-L1 CPS ≥1, the median OS was 16.7 months in the PLH-treated cohort compared with 11.7 months in the PL-treated cohort (HR 0.48, p = 0.001). The higher the CPS implying the occurrence of a strong immune response to pembrolizumab, the more likely the patients will benefit from pembrolizumab.
Univariate and multivariate analysis for survival
Tables 3 and 4 demonstrate the univariate and multivariate analyses for survival. Multivariate analysis demonstrated that the therapeutic regimen was an independent risk factor for both OS (HR 3.649; 95% CI, 1.592–6.074; p = 0.001) and PFS (HR 2.315; 95% CI, 1.211–3.629; p = 0.001). Multivariate analysis showed that Child-Pugh (B), and number of metastatic sites (≥3) were risk factors for OS and that AFP ≥ 400 ng/ml was a risk factor for PFS.
Safety
During the entire follow-up, the frequency of the key AEs is presented in Table 5. At the final follow-up, no significant differences in the rate of each AE were noted between groups. Treatment-related serious AEs (≥ grade 3) occurred in 6 patients (4 in the PLH versus 2 in the PL group, p = 0.391). No treatment-related deaths occurred in either cohort. The most common treatment-related AEs included alanine aminotransferase or aspartate aminotransferase elevation, total bilirubin elevation, decreased platelet, hypertension, fever, fatigue, decreased albumin, leukocytopenia, pain, nausea, and diarrhea, which were mostly grade 1/2. In the PLH group, the frequency of the key AEs of all grades was 79.8% (137 AEs in 67 patients). In the PL group, the frequency of the key AEs of all grades was 62.8% (104 AEs in 54 patients). A higher rate of key AEs was detected in the PLH group than in the PL group (79.8% vs. 62.8%, p = 0.015), but these AEs were controllable.
Discussion
The findings from the present retrospective study showed that the incorporation of HAIC into the pembrolizumab plus lenvatinib regimen may result in markedly longer PFS for selected populations of patients with treatment-naive uHCC exhibiting PD-L1 staining and significantly longer OS than the pembrolizumab plus lenvatinib regimen with a controllable safety profile. The survival curves among these patients included at an early survival benefit for patients treated using pembrolizumab plus lenvatinib plus HAIC that continued until the final follow-up with a noteworthy 5.1-month difference in median OS.
The findings of the present study are broadly consistent with a retrospective study [2] of 70 patients with advanced HCC that assessed the antitumour efficacy of HAIC combined with PD-1 inhibitors plus lenvatinib in patients with advanced HCC. In the retrospective review, the median OS (15.9 vs. 8.6 months, respectively; HR 0.60, 95% CI, 0.43–0.83; p = 0.0015) and median PFS (8.8 vs. 5.4 months, respectively; HR 0.74, 95% CI, 0.55–0.98; p = 0.0320) were higher in the HAIC plus PD-1 inhibitors plus lenvatinib group compared with the PD-1 inhibitors plus lenvatinib group. Their conclusion demonstrated that the superiority of antitumour efficacy in the HAIC plus PD-1 inhibitors plus lenvatinib regimen over that in the PD-1 inhibitors plus lenvatinib regimen was significant. Although the mechanisms of response and resistance to the pembrolizumab plus lenvatinib regimen remain unclear [16], an explanation as to why a higher median OS (15.9 months) was detected may be that under the premise of pembrolizumab plus lenvatinib use, the earlier the HAIC is utilized, the greater the survival is detected for these patients with uHCC [18, 19]. Previous studies [23, 24] have shown that it is effective in early tumours, which may be attributed to the local tumour-killing effect of HAIC. However, for unresectable tumours, the role of HAIC is limited [9]. One hypothesis is that unresestable tumours have a mature mechanism to evade recognition by CD8+ T cells [16]. This mature mechanism is highly related to the immune escape of tumour cells [17]. This could explain why unresectable tumours are resistant to conventional chemotherapy. Those with early HCC undergoing HAIC therapy have a marked, durable response, implying some derive short-term benefit from HAIC [23].
Child-Pugh stage as a risk factor for survival may be associated with prognosis in patients with uHCC, implying that patients with poor liver function might fail to benefit from triple combination therapy given that survival is limited by liver function [11, 12]. Accordingly, hepatic lesion control is conducive to improving prognosis to a certain extent [11]. Although the efficacy of the pembrolizumab plus lenvatinib regimen in extending survival is encouraging [16], distinct differences have been detected in the duration of HAIC therapy [2]. Management of advanced uHCC by inhibiting or blocking the activation of tumour signal transduction pathways is a strategy to address malignant tumours, and it may represent a trend [8, 25, 26]. Pembrolizumab, a highly selective IgG4-kappa humanized monoclonal antibody targeting PD-1, is indicated for the management of patients with advanced microsatellite instability-high or mismatch repair deficiency, and PD-L1-positive expression is associated with improved survival [12, 17]. Lenvatinib inhibits the kinase activities of vascular endothelial growth factor receptors that are associated with pathogenic angiogenesis and tumour growth [16]. Lenvatinib indirectly decreases the number of total PD-1 receptors by reducing the number of cancer cells, reinforcing the effect of pembrolizumab by promoting cancer cells to enter into “a dormant state” [2, 15]. This synergistic effect of pembrolizumab and lenvatinib may represent the basis for HAIC’s effectiveness in managing advanced HCC.
uHCC frequently suffers from the overexpression of immune checkpoints, which is associated with tumour immune escape [3, 17]. Targeting this characteristic, pembrolizumab monotherapy has been shown to have a robust clinical benefit in patients with uHCC [12, 17]. However, no strategies to prevent immune checkpoint inhibitor resistance have been reported. Thus, systemic combination therapy in both first- and second-line settings for the management of patients with uHCC has become a recent strategy [3, 17, 27, 28]. Recently, atezolizumab (an anti-PD-L1 antibody) plus bevacizumab has been approved for the first-line management of uHCC in view of encouraging effectiveness from the IMbrave150 trial [27], which showed the estimated rate of survival at 12 months was 67.2% (95% CI, 61.3–73.1). Durvalumab is a humanized IgG antibody that binds PD-L1 and can block the interaction of PD-1 and PD-L1, eliminating inhibition of CD8+ T cell responses [29]. Durvalumab plus an anti-CTLA-4 antibody showed that the median OS reached 18 months in patients with uHCC [28]. A single-centre retrospective review [25] assessing ipilimumab plus anti-PD-1 inhibitor in patients with advanced HCC with progression on previous immune checkpoint inhibitors demonstrated that the median OS was 10.9 months (95% CI, 3.99–17.8), the median time-to-progression was 2.96 months (95% CI, 1.61–4.31), and the median duration of response was 11.5 (range, 2.76–30.3) months.
In the retrospective review, with patients who had treatment-naive uHCC exhibiting PD-L1 staining, no unpredicted AEs attributed to PLH or PL combination therapy were observed. Although the duration of PLH or PL combination therapy may be inconsistent in some patients, the inconsistent duration in these patients did not have contributed to the remarkable differences in the rates of key AEs. The rate of key AEs was similar to those seen in other studies [30, 31] of pembrolizumab combined with lenvatinib in patients with uHCC, implying that the toxicity profile of PLH or PL combination therapy tends to be controllable. AEs related to PLH or PL were in accordance with the well-known AEs reported in previous studies [2, 16, 32, 33].
There are several limitations to this final analysis. First, the retrospective nature of the present study has inherent biases. Survival results might have been affected by relatively small patient numbers, heterogeneous populations, selection biases, and subsequent management. The lack of revalidation of diagnostic procedures and a central blinded review may result in the overestimation of survival curves. Patients with depression, those who are potentially suicidal, or those performing acts of self-harm at home were not involved in the study. The final aetiological analysis of the deaths was not complete, which may lead to an underestimation of the survival curves. Second, mutational and other gene expression signatures and patient stratification based on primary HCC location were not performed in this study. Third, patients included in this study were limited to those patients with treatment-naive HCC exhibiting PD-L1 staining; hence, these results should not be generalized to all patients with HCC.
Conclusion
The results described here may support the growing body of evidence showing that the incorporation of HAIC into pembrolizumab plus lenvatinib is associated with improved survival benefits in selected populations of patients with treatment-naive uHCC exhibiting PD-L1 staining. Nevertheless, because the present study was only a retrospective review, we could not arrive at any definitive conclusion regarding the utilization of pembrolizumab plus lenvatinib plus HAIC in the management of uHCC. A prospective multicentre study is being planned to validate these findings.
Availability of data and materials
The datasets used and/or analyzed during the current study fails to be publicly available because of privacy regulations but are available from the corresponding author on reasonable request.
Abbreviations
- HCC:
-
hepatocellular carcinoma
- HAIC:
-
hepatic arterial infusion chemotherapy
- PD-L1:
-
programmed cell death ligand-1
- PLH:
-
pembrolizumab plus lenvatinib plus HAIC
- PL:
-
pembrolizumab plus lenvatinib
- FOLFOX:
-
oxaliplatin, fluorouracil, and leucovorin
- OS:
-
overall survival
- PFS:
-
progression-free survival
- AEs:
-
adverse events
- HR:
-
hazard ratio
- CI:
-
confidence interval
- PD-1:
-
programmed cell death protein-1
- CTLA-4:
-
cytotoxic T-lymphocyte-associated protein 4
- BCLC:
-
Barcelona Clinic Liver Cancer
- CPS:
-
combined positive score
- ECOG:
-
Eastern Collaborative Oncology Group
- RECIST:
-
Response Evaluation Criteria in Solid Tumors
- ALBI:
-
albumin–bilirubin
- CT:
-
computed tomography
- MRI:
-
magnetic resonance imaging
References
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. https://doi.org/10.3322/caac.21492.
Mei J, Tang YH, Wei W, Shi M, Zheng L, Li SH, et al. Hepatic arterial infusion chemotherapy combined with PD-1 inhibitors plus Lenvatinib versus PD-1 inhibitors plus Lenvatinib for advanced hepatocellular carcinoma. Front Oncol. 2021;11:618206. https://doi.org/10.3389/fonc.2021.618206.
Zhang W, Song ZH, Xiao JP, Liu XH, Luo Y, Yang ZK, et al. Blocking the PD-1/PD-L1 axis in dendritic cell-stimulated cytokine-induced killer cells with pembrolizumab enhances their therapeutic effects against hepatocellular carcinoma. J Cancer. 2019;10(11):2578–87. https://doi.org/10.7150/jca.26961.
Fessas P, Kaseb A, Wang YH, Saeed A, Szafron D, Jun T, et al. Post-registration experience of nivolumab in advanced hepatocellular carcinoma: an international study. J Immunother Cancer. 2020;8(2):e001033. https://doi.org/10.1136/jitc-2020-001033.
Lin CC, Hung CF, Chen WT, Lin SM. Hepatic arterial infusion chemotherapy for advanced hepatocellular carcinoma with portal vein thrombosis: impact of early response to 4 weeks of treatment. Liver Cancer. 2015;4(4):228–40. https://doi.org/10.1159/000367737.
Onishi H, Nouso K, Nakamura S, Katsui K, Wada N, Morimoto Y, et al. Efficacy of hepatic arterial infusion chemotherapy in combination with irradiation for advanced hepatocellular carcinoma with portal vein invasion. Hepatol Int. 2015;9(1):105–12. https://doi.org/10.1007/s12072-014-9592-y.
Song DS, Song MJ, Bae SH, Chung WJ, Jang JY, Kim YS, et al. A comparative study between sorafenib and hepatic arterial infusion chemotherapy for advanced hepatocellular carcinoma with portal vein tumor thrombosis. J Gastroenterol. 2015;50(4):445–54. https://doi.org/10.1007/s00535-014-0978-3.
He MK, Li QJ, Zou RH, Shen JX, Fang WQ, Tan GS, et al. Sorafenib plus hepatic arterial infusion of Oxaliplatin, fluorouracil, and Leucovorin vs Sorafenib alone for hepatocellular carcinoma with portal vein invasion a randomized clinical trial. Jama Oncology. 2019;5(7):953–60. https://doi.org/10.1001/jamaoncol.2019.0250.
Ikeda M, Shimizu S, Sato T, Morimoto M, Kojima Y, Inaba Y, et al. Sorafenib plus hepatic arterial infusion chemotherapy with cisplatin versus sorafenib for advanced hepatocellular carcinoma: randomized phase II trial. Ann Oncol. 2016;27(11):2090–6. https://doi.org/10.1093/annonc/mdw323.
Kudo M, Izumi N, Sakamoto M, Matsuyama Y, Ichida T, Nakashima O, et al. Liver Canc study grp J. survival analysis over 28 years of 173,378 patients with hepatocellular carcinoma in Japan. Liver Cancer. 2016;5(3):190–7. https://doi.org/10.1159/000367775.
El-Khoueiry AB, Sangro B, Yau T, Crocenzi TS, Kudo M, Hsu CN, et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): an open-label, non-comparative, phase 1/2 dose escalation and expansion trial. Lancet. 2017;389(10088):2492–502. https://doi.org/10.1016/S0140-6736(17)31046-2.
Zhu AX, Finn RS, Edeline J, Cattan S, Ogasawara S, Palmer D, et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): a non-randomised, open-label phase 2 trial. Lancet Oncol. 2018;19(7):940–52. https://doi.org/10.1016/S1470-2045(18)30351-6.
Feun LG, Li YY, Wu CJ, Wangpaichitr M, Jones PD, Richman SP, et al. Phase 2 study of pembrolizumab and circulating biomarkers to predict anticancer response in advanced, unresectable hepatocellular carcinoma. Cancer. 2019;125(20):3603–14. https://doi.org/10.1002/cncr.32339.
Kambhampati S, Bauer KE, Bracci PM, Keenan BP, Behr SC, Gordan JD, et al. Nivolumab in patients with advanced hepatocellular carcinoma and child-Pugh class B cirrhosis: safety and clinical outcomes in a retrospective case series. Cancer. 2019;125(18):3234–41. https://doi.org/10.1002/cncr.32206.
Liu ZN, Li XJ, He XQ, Xu YC, Wang X. Complete response to the combination of Lenvatinib and Pembrolizumab in an advanced hepatocellular carcinoma patient: a case report. BMC Cancer. 2019;19(1):1062. https://doi.org/10.1186/s12885-019-6287-8.
Finn RS, Ikeda M, Zhu ANX, Sung MW, Baron AD, Kudo M, et al. Phase Ib Study of Lenvatinib Plus Pembrolizumab in Patients With Unresectable Hepatocellular Carcinoma. J Clin Oncol. 2020;38(26):2960–+.
Finn RS, Ryoo BY, Merle P, Kudo M, Bouattour M, Lim HY, et al. Pembrolizumab As Second-Line Therapy in Patients With Advanced Hepatocellular Carcinoma in KEYNOTE-240: A Randomized, Double-Blind, Phase III Trial. J Clin Oncol. 2020;38(3):193–+.
Chen YC, Ramjiawan RR, Reiberger T, Ng MR, Hato T, Huang YH, et al. CXCR4 inhibition in tumor microenvironment facilitates anti-programmed death Receptor-1 immunotherapy in Sorafenib-treated hepatocellular carcinoma in mice. Hepatology. 2015;61(5):1591–602. https://doi.org/10.1002/hep.27665.
Cheng AL, Hsu C, Chan SL, Choo SP, Kudo M. Challenges of combination therapy with immune checkpoint inhibitors for hepatocellular carcinoma. J Hepatol. 2020;72(2):307–19. https://doi.org/10.1016/j.jhep.2019.09.025.
Lyu N, Lin Y, Kong Y, Zhang Z, Liu L, Zheng L, et al. FOXAI: a phase II trial evaluating the efficacy and safety of hepatic arterial infusion of oxaliplatin plus fluorouracil/leucovorin for advanced hepatocellular carcinoma. Gut. 2018;67(2):395–6. https://doi.org/10.1136/gutjnl-2017-314138.
Ryoo BY, Merle P, Kulkarni AS, Cheng AL, Bouattour M, Lim HY, et al. Health-related quality-of-life impact of pembrolizumab versus best supportive care in previously systemically treated patients with advanced hepatocellular carcinoma: KEYNOTE-240. Cancer. 2021;127(6):865–74. https://doi.org/10.1002/cncr.33317.
Kudo M, Finn RS, Qin S, Han KH, Ikeda K, Piscaglia F, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163–73. https://doi.org/10.1016/S0140-6736(18)30207-1.
Nouso K, Miyahara K, Uchida D, Kuwaki K, Izumi N, Omata M, et al. Liver Cancer study grp J. effect of hepatic arterial infusion chemotherapy of 5-fluorouracil and cisplatin for advanced hepatocellular carcinoma in the Nationwide survey of primary liver Cancer in Japan. Br J Cancer. 2013;109(7):1904–7. https://doi.org/10.1038/bjc.2013.542.
Iwamoto H, Niizeki T, Nagamatsu H, Ueshima K, Nomura T, Kuzuya T, et al. Survival Benefit of Hepatic Arterial Infusion Chemotherapy over Sorafenib in the Treatment of Locally Progressed Hepatocellular Carcinoma. Cancers (Basel). 2021;13(4):646.
Wong JSL, Kwok GGW, Tang V, Li BCW, Leung R, Chiu J, et al. Ipilimumab and nivolumab/pembrolizumab in advanced hepatocellular carcinoma refractory to prior immune checkpoint inhibitors. J Immunother Cancer. 2021;9(2):e001945. https://doi.org/10.1136/jitc-2020-001945.
Yau T, Kang YK, Kim TY, El-Khoueiry AB, Santoro A, Sangro B, et al. Efficacy and Safety of Nivolumab Plus Ipilimumab in Patients With Advanced Hepatocellular Carcinoma Previously Treated With Sorafenib The CheckMate 040 Randomized Clinical Trial. JAMA Oncol. 2020;6(11):e204564. https://doi.org/10.1001/jamaoncol.2020.4564.
Finn RS, Qin S, Ikeda M, Galle PR, Ducreux M, Kim TY, et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N Engl J Med. 2020;382(20):1894–905. https://doi.org/10.1056/NEJMoa1915745.
Kelley RK, Sangro B, Harris WP, Ikeda M, Okusaka T, Kang YK, et al. Efficacy, tolerability, and biologic activity of a novel regimen of tremelimumab (T) in combination with durvalumab (D) for patients (pts) with advanced hepatocellular carcinoma (aHCC). J Clin Oncol. 2020;38(15_suppl):4508. https://doi.org/10.1200/JCO.2020.38.15_suppl.4508.
Bang YJ, Golan T, Dahan L, Fu SQ, Moreno V, Park K, et al. Ramucirumab and durvalumab for previously treated, advanced non-small-cell lung cancer, gastric/gastro-oesophageal junction adenocarcinoma, or hepatocellular carcinoma: an open-label, phase Ia/b study (JVDJ). Eur J Cancer. 2020;137:272–84. https://doi.org/10.1016/j.ejca.2020.06.007.
Wu CJ, Hung YW, Lee PC, Lee CJ, Chen MH, Chao Y, et al. Real-world experience of pembrolizumab plus lenvatinib in unresectable hepatocellular carcinoma in Taiwan. J Clin Oncol. 2020;38(15):e16627. https://doi.org/10.1200/JCO.2020.38.15_suppl.e16627.
Ikeda M, Sung MW, Kudo M, Kobayashi M, Baron AD, Finn RS, et al. A phase 1b trial of lenvatinib plus pembrolizumab in patients with unresectable hepatocellular carcinoma. Asia Pac J Clin Oncol. 2018;14:105.
Motzer R, Alekseev B, Rha SY, Porta C, Eto M, Powles T, et al. Lenvatinib plus Pembrolizumab or Everolimus for Advanced Renal Cell Carcinoma. N Engl J Med. 2021;384(14):1289–300.
Kawazoe A, Fukuoka S, Nakamura Y, Kuboki Y, Wakabayashi M, Nomura S, et al. Lenvatinib plus pembrolizumab in patients with advanced gastric cancer in the first-line or second-line setting (EPOC1706): an open-label, single-arm, phase 2 trial. Lancet Oncol. 2020;21(8):1057–65. https://doi.org/10.1016/S1470-2045(20)30271-0.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
Song Chen and Bo Xu participated in the data collection and prepared the manuscript. Zhiqiang Wu, Pengfei Wang, Zhiyong Liu, and Xiaoyong Huang participated in the statistical analysis and the preparation of study protocols. Yanqing Wu provided guidance in analyzing the dataset and contributed to writing the manuscript. Weiguang Yu, Tengfei Li, and Wenbo Guo was a major contributor in writing the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
All methods were carried out according to the relevant guidelines and regulations of the institutional and/or national research committee and the 1964 Helsinki declaration. This study was strictly retrospective and involving the collection of existing data and records and therefore the need for informed consent was waived by the Institutional Review Board (IRB) of the First Affiliated Hospital, Sun Yat-sen University. This study was approved by the IRB of the First Affiliated Hospital, Sun Yat-sen University (IRB18–2246).
Consent for publication
Not applicable.
Competing interests
The authors declare that there is no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chen, S., Xu, B., Wu, Z. et al. Pembrolizumab plus lenvatinib with or without hepatic arterial infusion chemotherapy in selected populations of patients with treatment-naive unresectable hepatocellular carcinoma exhibiting PD-L1 staining: a multicenter retrospective study. BMC Cancer 21, 1126 (2021). https://doi.org/10.1186/s12885-021-08858-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-021-08858-6