
Abstract
Background
We examined incidence and survival in relation to age, gender, socioeconomic deprivation, rurality and trends over time. We also examined the association between volume of patients treated by hospitals and survival.
Methods
Incident cases (2001–12) were identified using comprehensive National Health Service admissions data for England, with follow-up to March 2013. Socioeconomic deprivation was based on census area of residence. Volume was assessed in a three-year subset of the data with consistent hospital provider codes.
Results
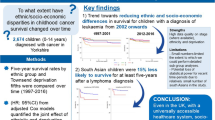
There were 2921 adults aged 18 or more years diagnosed with acute lymphoblastic leukaemia (ALL) in the 12-year time span, giving a crude annual incidence of 0.61/100,000 population. Five-year survival was 32% (1870 deaths).
Compared with patients living in least deprived areas, survival was worse for patients living in intermediate and most deprived areas, with mortality hazard ratios 21% (95% CI 8–35%) and 16% (95% CI 3–30%) higher respectively.
Hospitals treating low volumes of adults with ALL were associated with poorer survival. The adjusted mortality hazard ratio in this subset of 465 patients was 33% (95% CI 3–73%) higher in low volume hospitals.
There was no evidence of association between socioeconomic deprivation and incidence. Rurality did not appear to be associated with incidence or survival. Incidence was higher in men but there was no evidence of a gender difference in survival. Survival improved over time.
Conclusion
The associations between socioeconomic deprivation and survival and between volume and outcome for adults with ALL, if confirmed, are likely to have significant implications for the organisation of services for adults with ALL.
Similar content being viewed by others


Background
Acute lymphoblastic leukaemia (ALL) is a haematological malignancy arising from lymphoblasts. Whilst it is a relatively common malignancy in children with a higher incidence in boys, the incidence is rare in adults. The prognosis is good in childhood ALL but is poor in the adult form of the disease [1]. The epidemiology of childhood ALL has been well documented but much less has been done on the epidemiology in adults.
Socioeconomic inequalities in health are a major cause of concern and socioeconomic deprivation is associated with the incidence and prognosis of many conditions [2]. With regard to the incidence of ALL in childhood, a review of early studies found that higher incidence appeared to be associated with higher socioeconomic status [3]. However, another review which included several subsequent studies found conflicting evidence [4]. Little has been done on the incidence of ALL in adults in relation to socioeconomic deprivation and a study of young adults found no evidence of association [5].
The association between socioeconomic deprivation and survival has been examined in a number of studies on childhood ALL, with poorer survival associated with deprivation in several studies but not others [5,6,7,8,9,10]. Little research, however, has been carried out on the association between socioeconomic deprivation and survival in adults with ALL, with no significant association found in young adults [5].
The association between the volume of patients treated at a hospital and outcome has significant implications for the organisation and centralisation of services and has been investigated in relation to an increasing range of conditions, including medical and surgical care for cancer patients [11]. With regard to ALL, centres treating a high volume of childhood ALL cases were found to have better outcomes in some studies but not others [12,13,14]. However, the association between volume and outcome has not been investigated in relation to ALL in adults.
Trends over time and geographical variation are other aspects relevant to the epidemiology of ALL in adults. In one region in the UK, there appeared to be no improvement in survival of young adults diagnosed between 1990 and 2002 [5]. However, studies in other countries which included more recent years have reported improvements in survival over time [15, 16]. International and within country geographical variation in ALL incidence and survival has been examined, although mainly in children or with all ages combined [1, 5, 10]. Little, however, has been done on the differences in incidence and survival between urban and rural areas in relation to adults with ALL.
We examined the incidence and survival of adults with ALL in relation to age, gender, socioeconomic deprivation, rurality and trends over time. We also examined the association between volume of patients treated by hospital providers and survival.
Methods
Study design, area and time span
We used a population (ecological) study design to investigate incidence and a cohort study design to examine survival amongst all adult patients (aged 18 years or more at diagnosis) in England diagnosed from 2001 to 2012. Follow-up was to 31st March 2013. The study was approved by the University of Sheffield’s Research Ethics Committee. Participant consent was not necessary as this study involved the use of de-identified Hospital Episode Statistics (HES) supplied by NHS Digital. NHS Digital is an executive non-departmental public body accountable to Parliament and its statutory role is set out in the Health and Social Care Act 2012.
Data on cases
We used pseudoanonymised HES data with linked mortality data to identify cases with ALL. HES is a data warehouse containing details of all admissions to National Health Service (NHS) hospitals in England [17]. Admissions are recorded as “episodes” where an episode is a period of care under a single consultant during an admission. An admission may comprise more than one episode if a patient is transferred from the care of one consultant to another during the admission, though in practice most admissions comprise a single episode. The admission episode record includes several diagnosis and procedure code fields. We used the first seven diagnosis fields and the first 12 procedure code fields in order to use a set that was consistent throughout the study time span (there were more fields in later years). HES years follow the UK financial calendar and run from 1st April to 31st March the following year. We obtained data from 1st April 2000 to 31st March 2013. We excluded patients with a first admission with ALL in 2000 to exclude prevalent cases.
We used the International Classification of Diseases, 10th revision (ICD-10) code C91.0 to identify cases of ALL. The main advantage of using HES is complete national data capture as every adult in England who developed ALL will almost certainly have been admitted to an NHS hospital on at least one occasion for confirmation of the diagnosis and assessment for treatment and supportive care. However, there is significant scope for error in coding of leukaemia in HES.
We therefore first identified individuals (using the HES pseudoanonymised identifier) with a C91.0 code in any diagnosis field and extracted all their admission episode records. We then carried out a whole series of exploratory analyses which included examining procedure codes for chemotherapy, central line insertion, spinal fluid investigation and bone marrow examination. We also examined numbers of admissions per patient, cause of death and diagnoses likely to be miscoded as ALL. We classified the latter as “ambiguous” diagnoses, which included other leukaemias (C91.1 – C96.9) and lymphomas and myeloma (C81.0 – C90.2).
We arrived at a definition of a case as a patient with all of the following: a diagnosis of C91.0 as the primary diagnosis in at least one episode, an admission count >1; a chemotherapy code recorded in at least one episode; and a ratio of count of episodes with C91.0 code to count of episodes containing an ambiguous diagnosis code >1. Patients admitted for assessment but deemed too frail to withstand chemotherapy, or who died during or following their first admission, would have been excluded by the above definition. We therefore also included, as a separate definition, patients with C91.0 as the cause of death. These patients would also have had a C91.0 code in any diagnosis field in at least one admission episode. Records, in at least one episode, of central line insertion (65.6%), spinal fluid investigation (54.1%) or bone marrow examination (73.7%) were too incomplete to be used in the case definition, given that all patients undergoing diagnosis and treatment would have had these procedures carried out. The average number of cases identified using the above criteria was 243 per year and was comparable to the average estimated count of 240 per year from Office for National Statistics (ONS) statistics based on cancer registries [18].
Other data
We used the Income Domain of the Index of Multiple Deprivation (IMD) 2007 as an indicator of socioeconomic deprivation at the small area level [19]. The IMD is a standard deprivation indicator used by local and national government and is available at the lower layer super-output area (LSOA) level. LSOAs are census areas used in the 2001 and 2011 censuses, with approximately 1500 people per LSOA.
We used the government’s urban-rural classification to classify LSOAs as either urban or rural [20]. Mid-year population counts by five-year age band and sex at the LSOA level were also available from ONS.
Volume and outcome
HES data contain provider unit codes which we used to estimate the volume of adult patients with ALL treated at each provider hospital. Provider units have reconfigured over time on several occasions with consequent changes in codes. We had a consistent set of codes for a limited time span (1st April 2008 – 31st March 2011) available from another project, which we used for this element of the analysis [21]. Estimation of volume was based on new adult patients with ALL diagnosed during this three-year time span. Patients could have been admitted to more than one hospital during this time span and were included in the volume count of each hospital they were admitted to. We used the median to split hospitals into high and low volume hospitals.
Statistical analysis
We used Poisson regression to examine incidence, and survival plots and Cox regression to examine survival. Age (20–29 years for incidence, 18–29 years for survival, then 10-year bands to 80+ years), gender, rurality, time-period (3 four-year periods) and socioeconomic deprivation (categorised by tertile) were entered as categorical variables. The logs of population counts were entered as the offset in the Poisson regression, which was restricted to 31,672 (97.5%) of the 32,482 LSOAs in 2001 which remained unchanged in 2011. Log [−log] plots were consistent with the proportionality assumption for Cox regression. There was no overdispersion in the Poisson model.
Date of diagnosis and age at diagnosis were based on the admission date of the first admission with a C91.0 code in any diagnosis field. Survival time was calculated in years from the date of diagnosis to date of death or censored at the end of the follow-up period. Analysis of the effect of volume on survival was examined on the subset of new patients described above. Results are presented as rate ratios or hazard ratios, adjusted for all other variables, with 95% confidence intervals.
Results
Characteristics of patients
There were a total of 2921 adults aged 18 or more years diagnosed with ALL in the 12-year time span examined, giving a crude annual incidence of 0.61/100,000 population. There were 1870 deaths in 7078 person-years of follow-up time.
The characteristics of the patients are shown in Table 1. Almost a quarter of the patients were in the 18–29 year age group, 42.5% were women and 18.6% lived in rural areas. There was a median of 23 (Interquartile Range (IQR) 6–53) admissions per patient within the time period examined. A very high percentage of admission episodes for each patient had a diagnosis of ALL recorded in one of the diagnosis fields (median 95% (IQR 81–100%)), with only a very small percentage of episodes containing an ambiguous diagnosis code (median 0% (IQR 0–5%).
Incidence rate ratios
The adjusted incidence rate ratios are shown in Table 2. The incidence rate ratio was 42% (31–53%) higher in men. Compared with the 20–29 year age group, incidence was lower in patients aged 30–59 years and higher in patients aged 60+ years. There was no evidence of association of incidence with socioeconomic deprivation or rurality and no evidence of variation over the time frame examined.
Survival
Figure 1 shows the survival plot for adults diagnosed with ALL in England from 2001 to 12. The overall five-year survival for this cohort of 2921 patients was 32%. When restricted to the 2559 patients who had a record of chemotherapy, the five-year survival was 36%. The adjusted hazard ratios for mortality are shown in Table 3. These were based on analysis of all 2921 patients. Hazard ratios increased with increasing age but there was no evidence of a gender difference in survival. Compared with patients living in the least deprived areas, survival was poorer in patients living in intermediate and most deprived areas, with mortality hazard ratios 21% (8–35%) and 16% (3–30%) higher respectively. In terms of five-year survival, predicted rates for the least, intermediate and most deprived areas were 36% (33–38%), 30% (28–33%) and 31% (29–34%) respectively.

Survival plot for adults with ALL in England, 2001–12
There was no association with rurality. Survival improved over the time period examined, and the mortality hazard ratio was 30% (21–38%) lower in patients presenting in 2009–12 compared with patients presenting in 2001–04. In terms of five-year survival, predicted rates for patients presenting in 2001–04, 2005–08 and 2009–12 were 28% (26–31%), 30% (28–33%) and 39% (36–42%) respectively.
Volume-outcome association
There were 727 new patients admitted between 1st April 2008 and 31st March 2011, the period for which we had a consistent set of provider unit codes available. Of these, 465 had all their admissions to the same provider unit during this time span. The adjusted hazard ratio for mortality in this subset of 465 patients was 33% (3–73%) higher in low volume hospitals (Table 3). This analysis additionally adjusted for chemotherapy treatment as patients with no record of treatment for chemotherapy had much poorer survival.
Discussion
Whilst we found no evidence of association between socioeconomic deprivation and incidence of ALL in adults, survival with higher amongst patients living in affluent areas. Hospitals treating low volumes of adults with ALL were associated with poorer survival. Rurality did not appear to be associated with incidence or survival. Incidence was higher in men but there was no evidence of a gender difference in survival. Survival improved over time but was poor amongst older patients.
A review of early studies of childhood ALL found that higher incidence was associated with higher socioeconomic status [3]. However, a subsequent review found that the evidence was mixed, with several studies reporting lower incidence of childhood ALL in more affluent groups [4]. A more recent study found a non-significant decrease in incidence with increasing affluence in analyses combining children and adults [22]. Another study found no evidence of association between incidence and deprivation in young adults, consistent with our results for all adults [5].
With regard to survival, a national study in the UK on childhood ALL found that higher levels of socioeconomic deprivation were associated with poorer survival [9]. The authors argued that the association was not due to different treatment across social groups as the association was also seen in children enrolled in the UKALL XI trial. Our results indicate that socioeconomic inequalities in survival are also a significant cause for concern in adults with ALL and further research is required to understand and address this issue.
Our finding that mortality was higher for adults with ALL treated at hospitals treating low volumes of adult ALL patients is of concern. An early study on volume and outcome in the treatment of childhood ALL found that centres treating an average of six or more patients per year had the best long-term survival rates [12]. Although two recent childhood ALL studies found no association between volume and outcome, they only examined mortality during induction therapy [13, 14]. A study of in-hospital mortality in patients undergoing chemotherapy for acute myeloid leukaemia, a disease predominantly of adults, was the first to report that the mortality rate was significantly higher in low-volume hospitals [23]. High volume centres in general are more likely to have specialised clinical teams and more experienced staff to manage patients with specific medical conditions, which could explain better outcomes [24].
Our finding of improved survival over the time period examined is consistent with studies of adults with ALL in Germany, the USA and the Netherlands [15, 16]. We found no gender differences in survival. Others have reported that whilst survival was worse in men previously, the gender difference appears to no longer be apparent [15]. Survival, however, remains poor, especially amongst older adults and those with relapsed or refractory disease [1, 25].
Our study has a number of potential limitations which need to be considered. We used HES data which has the advantage of being a comprehensive national system and all adults with ALL are likely to have been admitted at least once to confirm the diagnosis. However, coding and data entry errors could have led to over or underascertainment of cases. We examined the data in detail in order to arrive at a set of procedures to keep errors to a minimum. The average case counts we obtained were comparable to the ONS estimates from cancer registration data. In addition, the five-year survival of 36% we observed for patients receiving chemotherapy is consistent with the five-year survival of 38% for adults in the UKALL 12 trial [26]. There may have been errors in the mid-year population estimates we used to calculate incidence rates. We used an area based measure of socioeconomic deprivation assigned to individual patients and some patients may have been misclassified. However, we used a measure based on small geographical areas which would have minimised this error as levels of socioeconomic deprivation for populations in smaller geographical units are likely to be generally more homogenous. The volume indicator was based on a relatively small number of cases because of the limited time span for which we had consistent provider unit codes, and some providers may have been misclassified by volume. However, misclassification in this context might have diluted the strength of the association. Potential errors need to be taken into account in the interpretation of our results.
Conclusions
In terms of future research and policy, further work is needed to confirm the association between higher socioeconomic deprivation and poorer survival and the observation that hospitals treating a low volume of patients were associated with poorer outcome for adults with ALL. These findings, if confirmed, are likely to have significant implications for the organisation of services for the treatment of adults with ALL.
Abbreviations
- ALL:
-
Acute lymphoblastic leukaemia
- HES:
-
Hospital episode statistics
- ICD-10:
-
International classification of diseases, 10th revision
- IMD:
-
Index of multiple deprivation
- IQR:
-
Interquartile range
- LSOA:
-
Lower layer super-output area
- NHS:
-
National Health Service
- ONS:
-
Office for national statistics
References
Katz AJ, Chia VM, Schoonen WM, Kelsh MA. Acute lymphoblastic leukemia: an assessment of international incidence, survival, and disease burden. Cancer Causes Control. 2015;26:1627–42.
Gordon D, Shaw M, Dorling D, Davey Smith G, editors. Inequalities in health. Bristol: Policy Press; 1999.
Greenberg RS, Shuster JL Jr. Epidemiology of cancer in children. Epidemiol Rev. 1985;7:22–48.
Poole C, Greenland S, Luetters C, Kelsey JL, Mezei G. Socioeconomic status and childhood leukaemia: a review. Int J Epidemiol. 2006;35:370–84.
Feltbower RG, McNally RJ, Kinsey SE, Lewis IJ, Picton SV, Proctor SJ, Richards M, Shenton G, Skinner R, Stark DP, Vormoor J, Windebank KP, McKinney PA. Epidemiology of leukaemia and lymphoma in children and young adults from the north of England, 1990-2002. Eur J Cancer. 2009;45:420–7.
McWhirter WR, Smith H, McWhirter KM. Social class as a prognostic variable in acute lymphoblastic leukaemia. Med J Aust. 1983;2:319–21.
Coebergh JW, van der Does-van den Berg A, Hop WC, van Weerden F, Rammeloo JA, van Steensel HA, van Wering ER, Kamps WA. Small influence of parental educational level on the survival of children with leukaemia in The Netherlands between 1973 and 1979. Eur J Cancer. 1996;32:286–9.
Mostert S, Sitaresmi MN, Gundy CM, Sutaryo, Veerman AJ. Influence of socioeconomic status on childhood acute lymphoblastic leukemia treatment in Indonesia. Pediatrics. 2006;118:e1600–6.
Lightfoot TJ, Johnston WT, Simpson J, Smith AG, Ansell P, Crouch S, Roman E, Kinsey SE. Survival from childhood acute lymphoblastic leukaemia: the impact of social inequality in the United Kingdom. Eur J Cancer. 2012;48:263–9.
Schillinger JA, Grosclaude PC, Honjo S, Quinn MJ, Sloggett A, Coleman MP. Survival after acute lymphocytic leukaemia: effects of socioeconomic status and geographic region. Arch Dis Child. 1999;80:311–7.
Hillner BE, Smith TJ, Desch CE. Hospital and physician volume or specialization and outcomes in cancer treatment: importance in quality of cancer care. J Clin Oncol. 2000;18:2327–40.
Stiller CA, Draper GJ. Treatment centre size, entry to trials, and survival in acute lymphoblastic leukaemia. Arch Dis Child. 1989;64:657–61.
Seif AE, Fisher BT, Li Y, Torp K, Rheam DP, Huang YS, Harris T, Shah A, Hall M, Fieldston ES, Kavcic M, Vujkovic M, Bailey LC, Kersun LS, Reilly AF, Rheingold SR, Walker DM, Aplenc R. Patient and hospital factors associated with induction mortality in acute lymphoblastic leukemia. Pediatr Blood Cancer. 2014;61:846–52.
Wilkes JJ, Hennessy S, Xiao R, Rheingold S, Seif AE, Huang YS, Vendetti N, Li Y, Bagatell R, Aplenc R, Fisher BT. Volume-outcome relationships in pediatric acute lymphoblastic leukemia: association between hospital pediatric and pediatric oncology volume with mortality and intensive care resources during initial therapy. Clin Lymphoma Myeloma Leuk. 2016;16:404–410.e1.
Pulte D, Jansen L, Gondos A, Katalinic A, Barnes B, Ressing M, Holleczek B, Eberle A, Brenner H, Cancer Survival GEKID. Working group. Survival of adults with acute lymphoblastic leukemia in Germany and the United States. PLoS One. 2014;9:e85554.
Dinmohamed AG, Szabó A, van der Mark M, Visser O, Sonneveld P, Cornelissen JJ, Jongen-Lavrencic M, Rijneveld AW. Improved survival in adult patients with acute lymphoblastic leukemia in the Netherlands: a population-based study on treatment, trial participation and survival. Leukemia. 2016;30:310–7.
NHS Digital. Hospital Episode Statistics. http://content.digital.nhs.uk/hes.
Office for National Statistics. Cancer Registration Statistics, England Statistical bulletins. https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/cancerregistrationstatisticsengland/previousReleases.
Department for Communities and Local Government. English indices of deprivation. 2012. https://www.gov.uk/government/collections/english-indices-of-deprivation.
GOV.UK. Rural Urban Classification. https://www.gov.uk/government/collections/rural-urban-classification.
O'Cathain A, Knowles E, Maheswaran R, Turner J, Hirst E, Goodacre S, Pearson T, Nicholl J. Hospital characteristics affecting potentially avoidable emergency admissions: national ecological study. Health Serv Manag Res. 2013;26:110–8.
Bhayat F, Das-Gupta E, Smith C, McKeever T, Hubbard R. The incidence of and mortality from leukaemias in the UK: a general population-based study. BMC Cancer. 2009;9:252.
Giri S, Pathak R, Aryal MR, Karmacharya P, Bhatt VR, Martin MG. Impact of hospital volume on outcomes of patients undergoing chemotherapy for acute myeloid leukemia: a matched cohort study. Blood. 2015;125:3359–60.
Ross JS, Normand SL, Wang Y, Ko DT, Chen J, Drye EE, Keenan PS, Lichtman JH, Bueno H, Schreiner GC, Krumholz HM. Hospital volume and 30-day mortality for three common medical conditions. N Engl J Med. 2010;362:1110–8.
Sive JI, Buck G, Fielding A, Lazarus HM, Litzow MR, Luger S, Marks DI, McMillan A, Moorman AV, Richards SM, Rowe JM, Tallman MS, Goldstone AH. Outcomes in older adults with acute lymphoblastic leukaemia (ALL): results from the international MRC UKALL XII/ECOG2993 trial. Br J Haematol. 2012;157:463–71.
Rowe JM, Buck G, Burnett AK, Chopra R, Wiernik PH, Richards SM, Lazarus HM, Franklin IM, Litzow MR, Ciobanu N, Prentice HG, Durrant J, Tallman MS, Goldstone AH. ECOG.; MRC/NCRI adult leukemia working party. Induction therapy for adults with acute lymphoblastic leukemia: results of more than 1500 patients from the international ALL trial: MRC UKALL XII/ECOG E2993. Blood. 2005;106:3760–7.
Acknowledgements
This work used HES data which are Copyright © 2016, Re-used with the permission of NHS Digital. All rights reserved. This work also used National Statistics / Ordnance Survey data © Crown copyright and database right 2016.
Funding
This work was supported by a grant from Amgen Ltd. The views expressed in this publication are those of the authors and not necessarily those of the funder (Amgen Ltd), which had no role in the data analysis or write up.
Availability of data and materials
The HES data used in this study may be obtained from NHS Digital [17]. IMD and urban-rural classification are available from publicly accessible websites [19, 20].
Author information
Authors and Affiliations
Contributions
RM designed the study with clinical advice and guidance from NM. RM carried out the statistical analysis and wrote the first draft which was revised by NM. Both authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Authors’ information
RM is a medically qualified Professor of Epidemiology and Public Health in the School of Health and Related Research (ScHARR) at the University of Sheffield. NM is a Consultant Haematologist at the Royal Hallamshire Hospital, Sheffield who specialises in the treatment of ALL.
Ethics approval and consent to participate
The study was approved by the University of Sheffield’s Research Ethics Committee. Participant consent was not necessary as this study involved the use of de-identified Hospital Episode Statistics supplied by NHS Digital. NHS Digital is an executive non-departmental public body accountable to Parliament and its statutory role is set out in the Health and Social Care Act 2012.
Consent for publication
Not applicable.
Competing interests
The views expressed in this publication are those of the authors and not necessarily those of the funder (Amgen Ltd), which had no role in the data analysis or write up. The authors have no financial or non-financial competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Maheswaran, R., Morley, N. Incidence, socioeconomic deprivation, volume-outcome and survival in adult patients with acute lymphoblastic leukaemia in England. BMC Cancer 18, 25 (2018). https://doi.org/10.1186/s12885-017-3975-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-017-3975-0