
Abstract
Background
Diagnosing breast cancer during the early stage may be helpful for decreasing cancer-related mortality. In Western developed countries, mammographies have been the gold standard for breast cancer detection. However, Chinese women usually have denser and smaller-sized breasts compared to Caucasian women, which decreases the diagnostic accuracy of mammography. However, breast specific gamma imaging, a type of molecular functional breast imaging, has been used for the accurate diagnosis of breast cancer and is not influenced by breast density. Our objective was to analyze the breast specific gamma imaging (BSGI) diagnostic value for Chinese women.
Methods
During a 2-year period, 357 women were diagnosed and treated at our oncology department and received BSGI in addition to mammography (MMG), ultrasound (US) and magnetic resonance imaging (MRI) for diagnostic assessment. We investigated the sensitivity and specificity of each method of detection and compared the biological profiles of the four imaging methods.
Results
A total of 357 women received a final surgical pathology diagnosis, with 168 malignant diseases (58.5 %) and 119 benign diseases (41.5 %). Of these, 166 underwent the four imaging tests preoperatively. The sensitivity of BSGI was 80.35 and 82.14 % by US, 75.6 % by MMG, and 94.06 % by MRI. Furthermore, the breast cancer diagnosis specificity of BSGI was high (83.19 % vs. 77.31 % vs. 66.39 % vs. 67.69 %, respectively). The BSGI diagnostic sensitivity for mammographic breast density in women was superior to mammography and more sensitive for non-luminal A subtypes (luminal A vs. non-luminal A, 68.63 % vs. 88.30 %).
Conclusions
BSGI may help improve the ability to diagnose early stage breast cancer for Chinese women, particularly for ductal carcinoma in situ (DCIS), mammographic breast density and non-luminal A breast cancer.
Similar content being viewed by others


Background
Breast cancer is the leading type of new cancer cases and the second leading cause of cancer related deaths in females worldwide [1]. During the past 30 years, the incidence and mortality of breast cancer in Chinese women has gradually increased and has become a primary cause of death, with more than 1.6 million people diagnosed and 1.2 million people dying of the disease each year [2, 3]. The current guidelines suggest that breast cancer screening and diagnostic imaging modalities include mammography (MMG) and ultrasound (US) for women at average risk and magnetic resonance imaging (MRI) for high-risk women [4]. These methods can detect early stage breast cancer and reduce mortality. Despite their effectiveness, these traditional imaging methods have limitations that complicate the standardization of image quality and can affect the diagnostic accuracy of the breast examination. The diagnostic accuracy of MMG is affected by mammographic breast density, with decreased sensitivity in patients with dense breasts [5]. For MRI, a variable degree of background parenchyma enhancement (BPE) of normal fibro-glandular tissue occurs. Marked BPE can cause a higher abnormal interpretation rate and may influence the accuracy of MRI [5, 6]. Notably, the mean age at diagnosis of breast cancer in China is 45–55 years, which is considerably younger than for Western females. Young women usually have a smaller proportion of fat content relative to the fibro-glandular tissue in their breasts compared to older, Chinese women, who usually have denser and smaller-sized breasts compared to Caucasian women [2]. Therefore, the traditional imaging modalities have a low diagnostic value in China.
Breast specific gamma imaging (BSGI) is a physiologic approach to breast imaging using a high resolution, small-gamma camera and a tracer agent called 99mTc-Sestamibi (MIBI), and molecular breast imaging has significantly improved in recent years with the development of breast optimized imaging [7, 8]. MIBI retention in tumor cells is determined by the cellular and mitochondrial membrane potential and the presence of an ATP-powered efflux pump, such as P-glycoprotein, which can transport foreign substances out of cells. However, unlike MMG, BSGI performance is independent of breast density [7, 9, 10]. Furthermore BPE is likely related to the blood volume and vascular permeability of normal breast tissue; therefore, it is predicted not to influence the background MIBI uptake. The sensitivity (Se) and specificity (Sp) of BSGI from a meta-analysis of 8 studies, including 2183 lesions, were 95 % (95 % CI 93–96 %) and 80 % (95 % CI 78–82 %), respectively, and were not affected by the breast density [11]. This was better than the reported sensitivity and specificity for the largest breast MRI study (n = 821), with 88.1 % (95 % CI, 84.6–91.1 %) and 67.7 % (95 % CI, 62.7–71.9 %), respectively [12]. Therefore, the Society of Nuclear Medicine (SNM) recommended BSGI particularly for breast patients with breasts technically too difficult to examine using conventional mammography, including radiodense breast tissue, implants, free silicone, or paraffin injections [13].
Chinese women have denser breasts, and recent research also indicated that women with higher breast density are at an increased risk of breast cancer, and this is one of the highest risk factors for the prediction of breast cancer risk. Therefore, a useful and accurate breast imaging method is necessary. The development of a dedicated breast gamma imaging system has overcome these limitations and has returned scintimammography to the forefront of breast imaging. This was a retrospective study analyzing BSGI performed as an adjunct imaging method for Chinese women to detect breast cancer.
Methods
Patients
The hospital ethics committee approved this study. Written informed consent was obtained from each patient. A total of 357 breast disease patients who were diagnosed and treated at the oncology department (Second Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou, China) from June 2012 to January 2015 were included in this single-institution study. Patients were first identified by reviewing the BSGI database, and 357 patients who underwent BSGI were reviewed. The including criteria were as follows: 1) female patients 18-years-old and older; 2) pathological proof of non-metastatic breast cancer; and 3) received ultrasound (US), mammography (MMG) and breast-specific gamma imaging (BSGI) before diagnosis. Clinicopathological characteristics, including age, menstrual state, histological type, grade, hormone receptors, HER2 and the clinical stage at diagnosis were obtained from the medical files at our institution and were included in a unique dedicated database.
Imaging and pathologic review
Pathologic review
The histological type and grade were defined using the World Health Organization classification system. ER and PR tumor status are normally determined by immunohistochemistry (IHC) testing. Samples that have at least 1 % of cells staining positive for ER are considered ER-positive. Breast cancer tumors are classified as HER2-positive if they are scored as a 3 or more by an IHC method defined as a uniform membrane staining for HER2 in 10 % or more of tumor cells or have demonstrated HER2 gene amplification by a fluorescence in situ hybridization (FISH) method (single probe, average HER2 copy number ≥ 6.0 signals/cell; dual probe HER2/CEP17 ratio ≥ 2.0 with an average HER2 copy number ≥ 4.0 signals/cell; dual probe HER2/CEP17 ratio ≥ 2.0 with an average HER2 copy number < 4.0 signals/cell; HER2/CEP17 ratio < 2.0 with an average HER2 copy number ≥ 6.0 signals/cell) [14].
Ultrasound review
For the ultrasound examination, we used high-end equipment (IU Elite®; Philips Healthcare, Best, Netherlands), and all findings were documented in two perpendicular planes. The ultrasound positives were defined by an expert as highly suspected and suggestive of biopsy or operation.
Mammography review
The mammographic reports of the mammography were prospectively evaluated by one radiologist and reviewed (Selenia®, Hologic, Santiago, USA). The mammographic breast density was visually estimated according to the American College of Radiology Breast Imaging-Reporting and Data System classification and classified as follows: almost entirely fat (less than 25 % of breast comprising glandular tissue), having scattered fibroglandular densities (25–50 % of breast comprising glandular tissue), heterogeneously dense (51–75 % of breast comprising glandular tissue), and extremely dense (more than 75 % of breast comprising glandular tissue). Mammography positives were defined by an expert according to BI-RADS® Assessment Categories.
MRI review
Breast MRIs were performed on a 1.5 T system (Aera®, Siemens, München, Germany). Pre-contrast images of the dynamic series were subtracted from the post-contrast images to selectively highlight the enhancing structures. No parallel imaging was applied. MRI positives were defined by an expert as highly suspected and suggestive of biopsy or operation.
BSGI review
The patients were injected with 740–925 MBq (15–20 mCi) technetium-99 m sestamibi (Shanghai GMS Pharmaceutical Co., Ltd) into an arm vein. Craniocaudal and mediolateral views were performed of both breasts using a high-resolution, small field-of-view gamma camera optimized for breast imaging. Imaging was initiated immediately after injection of the isotope. Craniocaudal and mediolateral views were performed for both breasts with approximately 10 min per view (total time, 40 min). The images were obtained with a high-resolution, small field-of-view, breast-specific gamma camera (Dilon 6800 Gamma Camera; Dilon Technologies, Newport News, VA). BSGI positives were defined by an expert as highly suspected or having a tumor-to-normal tissue ratio (TNR) > 1.82.
Data analysis
The statistical analyses were performed using SPSS, version 20. The comparison between BSGI and US, MMG and MRI, and BSGI diagnostic values for different clinicopathological variables were calculated using either χ2 tests with continuity correction or Fisher’s exact test. All statistical tests were two sided and considered significant when p ≤ 0.05.
Results
Patient characteristics
There were 357 patients documented in our study. Of these, 287 patients underwent BSGI, US, and MMG, and 166 patients underwent all four imaging tests (BSGI, US, MMG and MRI) (Fig. 1). The median age of the study patients was 48.2 y and ranged from 32 to 75 y. The distribution of breast patient pathology was 168 malignant diseases (58.5 %), which was a combination of invasive ductal carcinoma (IDC), invasive lobular carcinoma (ILC), and ductal carcinoma in situ (DCIS), and 119 benign diseases (41.5 %).

Flowchart of the study
Cut-off values of TNR and distribution in breast malignant and benign disease
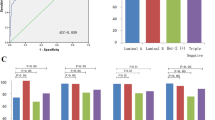
The cut-off value for TNR by sensitivity (Se), specificity (Sp) and Youden’s index (YI) analyses was 1.82 (Se:81.63 %, Sp:80.00 %, YI:61.63 %) (Fig. 2a). Our data also showed a statistically valid correlation for TNR between malignant breast diseases and benign diseases (p < 0.05). The mean TNR for the malignant group was 2.61 (95%CI 2.42–2.80), and for the benign group, the mean TNR was 1.41 (95 % CI 1.33–1.50) (Fig. 2b).

a ROC analysis for determining cut-off value of TNR in detection of breast cancer. b TNR of BSGI distribution in breast malignant and benign disease. c Sensitivity of BSGI, US, MMG and MRI for detecting breast cancer. d Sensitivity of BSGI, US, MMG and MRI for detecting DCIS
Value of BSGI, US, MMG and MRI for detecting breast cancer
The sensitivity of MRI for detecting malignant lesions reached 94.06 % (95 % CI 87.01–97.56 %) and was superior to BSGI (80.35 %, 95 % CI 73.38–85.92 %), US (82.14 %, 95 % CI 75.33–87.45 %) and MMG (75.60 %, 95 % CI 68.26–81.74 %). However, the specificity of BSGI was the highest at 83.19 % (95 % CI 74.99–89.19 %) compared to US (77.31 %, 95 % CI 68.54–84.27 %), MMG (66.39 %, 95 % CI 57.07–74.63 %) and MRI (67.69 %, 95 % CI 54.82–78.46 %). Correspondingly, the positive-predictive value for the malignancy of a lesion, accuracy and Youden’s index (YI) were the highest for BSGI (87.10, 84.82 and 63.54 %, respectively). The YI for each imaging modality highlights the outstanding diagnostic potential of BSGI (63.54 %) compared to ultrasound (59.45 %), MMG (41.99 %) and MRI (61.75 %) for our diagnostic approach (Table 1 and Fig. 2c).
There were 19 cases of DCIS. The sensitivity of BSGI for DCIS was 89.47 % (95 % CI 65.46–98.16 %) and 68.42 % for US (95 % CI 43.50–86.44 %), 57.89 % for MMG (95 % CI 33.97–78.88 %) and 84.62 % for MRI (95 % CI 53.66–97.29 %) (Fig. 2d).
When BSGI is combined with other examination techniques (MMG, US and MRI), we found that the accuracy for the detection of malignant breast lesions for BSGI combined with US was superior to BSGI + MMG or BSGI + MRI (Table 2).
The sensitivity and specificity for the detection of metastatic axillary lymph nodes by BSGI were 32 % (95 % CI 19.93–46.83 %) and 95.19 % (95 % CI 88.6–98.23 %), respectively (Table 3).
Sensitivity of BSGI, US, MMG and MRI in different traits of breast cancer
For premenopausal and postmenopausal women, the sensitivity of BSGI was not superior to breast US, MMG and MRI (Fig. 3a). The four breast density categories for breast composition are defined by the visually estimated content of fibroglandular dense tissue within the breasts. In the heterogeneously dense and extremely dense group, BSGI sensitivity was superior to MMG (82.35 % vs. 77.94 %; 85.45 % vs. 65.45 %, respectively) (Fig. 3c). For tumor grade and molecular subtype sensitivity analysis, the four imaging tests were not significantly different (Fig. 3b and d).

Sensitivity of BSGI, US, MMG and MRI in different traits of breast cancer
For the different breast cancer characteristics, the sensitivity of BSGI for detecting luminal A breast cancer was inferior at 68.63 % (95%CI 53.97–80.48 %) compared to luminal B (89.58 %, 95 % CI 76.56–96.10 %), HER-2(+) type (94.12 %, 95 % CI 69.24–99.69 %) and triple negative breast cancer (82.76 %, 95 % CI 63.51–93.47 %) (Fig. 4a). The TNR differed significantly between luminal-A and non-luminal-A breast cancer (p < .0001) (Fig. 4b).

a Sensitivity of BSGI in different characteristics of breast cancer. b TNR of BSGI distribution for different breast cancer molecular subtypes
False-positive and false-negative findings of BSGI
We had 20 cases of false-positive BSGI findings. The pathology of false-positive BSGI lesions is shown in Table 4. We also analyzed the false-negative findings according to the breast cancer traits. The majority of false-negative malignant tumors had an extensive intraductal component (11/33), were high grade (9/33) and were diagnosed as Paget’s disease (2/33).
Discussion
To our knowledge, this study is the first to evaluate the diagnostic value of breast specific gamma imaging for Chinese women. We found that BSGI could be used in a work-up of suspicious breast lesions. The visual and semi-quantitative analyses (TNR cut-off value 1.82) as combined for detecting primary breast cancer [15]. Comparison of the sensitivity and specificity of BSGI to US, MMG and MRI for breast cancer diagnosis, the values for BSGI were 80.35 and 83.19 %, respectively, and were slightly higher than for the other imaging tests (US, MMG and MRI). For Chinese breast cancer patients, approximately 73.72 % (123/168) of patients have heterogeneously dense or extremely dense breasts, and BSGI had significantly higher sensitivity compared to MMG, indicating that BSGI is rarely affected by breast density. For different molecular subtypes, non-luminal A types have a higher degree of sensitivity by BSGI examination.
Diagnostic value of BSGI
For breast cancer detection sensitivity and specificity, BSGI is superior to US and MMG, and showed equal sensitivity and high specificity compared to MRI for the diagnosis of breast lesions. According to tumor type, BSGI had good sensitivity for discriminating DCIS (89.47 %), suggesting that BSGI may play a crucial role as an adjunctive imaging modality to evaluate breast ductal carcinoma in situ. For Chinese women, almost 75 % have dense breasts, limiting MMG screening (sensitivity 75.60 %, specificity 66.39 %). BSGI was not influenced by breast density, and the sensitivity of heterogeneously dense or extremely dense breast patients was 82.35 and 85.45 %, respectively. Recently, studies indicated that the sensitivity of BSGI for detecting subcentimeter (<1 cm) breast cancer was 84 % (95 % CI 80–88 %) [16, 17]. Combined with our research, evidence suggests that BSGI, as a functional imaging test, is an extremely useful adjunct test for its ability to identify breast cancer with high diagnostic performance, and it was not influenced by menstrual state, tumor grade, or tumor size [16, 18, 19]. Due to the limitations of the examination methods, axilla are hard to test, but BSGI has a higher specificity for detecting axillary lymph node metastasis [20].
Screening mammography has been the gold standard for breast cancer detection for the past 30 years [21, 22], but recent studies have questioned this screening because it does not reduce breast cancer mortality [23]. MRI is currently recommended by the American Cancer Society in patients with high risk, but there are issues with sensitivity resulting in increased false positive rates leading to numerous benign biopsies or operations [24]. Studies demonstrated that BSGI has an equal sensitivity with a higher specificity than MRI as an adjunct imaging modality for the diagnosis of breast cancer. Additional advantages include greater ease of imaging for the patient, lower cost, and an easy read for the radiologist or surgeon [18, 25, 26]. Specifically in China, women have dense mammary glands and BSGI will show a higher value in the current paradigm of breast imaging for screening and diagnosis. First, for breast patients with BI-RADS® 0 or 3 by US and/or MMG, high risk, and/or MMG dense breasts, BSGI was a useful adjunctive imaging method to reduce the false-negative rate (missed diagnosis rate). Second, for breast patients with BI-RADS® 4 by US and/or MMG, biopsy is recommended. BSGI can reliably identify the US and/or MMG findings that are benign, which can avoid unnecessary biopsies for a majority of patients. Therefore, BSGI is highly recommended in these two situations for Chinese women.
Characterization of breast lesions with BSGI
As a functional imaging, semi-quantitative analysis is an important parameter of BSGI, which reflects the Tc-99 m MIBI uptake level. We found malignant lesions have a higher TNR than benign lesions (mean 2.61 vs. 1.41, p < .0001). This makes the semi-quantitative value of BSGI in breast cancer diagnosis possible. Interestingly, one case had a particularly high TNR, with TNR = 12.75, and we reviewed this patient’s medical files. This was a 50-year-old menopausal female, and the imaging examination is shown in Fig. 5. The pathologic diagnosis was invasive ductal carcinoma, WHO II grade. IHC tests showed that the tumor was ER negative, PR negative, HER-2 negative, and 30 % Ki-67 positive. After biopsy, this patient received standardized therapy and follow-up. At 20 months after diagnosis, this patient died because of the rapid spread of cancer with pulmonary metastasis and malignant pleural effusion. This case suggests that a high value of TNR may correlate with a poor prognosis [27].

Images for the case of breast cancer patient with TRN = 12.75. a MMG for right breast. b US for right breast and axillary. c BSGI image
For different molecular subtypes, the data show that the luminal A type has a lower TNR value (mean 2.35, 95 % CI 2.11–2.59) compared to the luminal B type (mean 2.82, 95 % CI 2.51–3.14), HER-2 positive type (mean 2.99, 95 % CI 2.24–3.73) and triple negative type (mean 2.77, 95 % CI 2.00–3.54). For BSGI diagnosis, the sensitivity of the luminal A type was the lowest (68.63 % 95 % CI 53.97–80.48 %), whereas the HER-2 positive type had the highest sensitivity (94.12 % 95 % CI 69.24–99.69 %) compared to the other subtypes (luminal B: 89.56 % 95 % CI 76.56–96.10 %; TNBC: 82.76 % 95 % CI 63.51–93.47 %). Therefore, BSGI may help classify the sub-type of an invasive ductal carcinoma in addition to its pathology.
Limitations of BSGI
BSGI has several limitations as a breast imaging modality. Patients are exposed to radiation from the BSGI test of approximately 6.29–9.44 mSv [8, 28]. BSGI may be recommended for patients with suspicious breast lesions or dense breasts by conventional methods, using lower doses and longer acquisition times [29]. Second, this is a plane test, and there may be insufficient positioning [16, 30]. Finally, BSGI was the least sensitive for detecting axillary lymph nodes.
Conclusion
In summary, BSGI showed a borderline sensitivity but a higher specificity than US/MMG/MRI for diagnosing breast lesions, and it has a high sensitivity for discriminating DCIS. BSGI may play a crucial role in discriminating breast lesions and can be used to evaluate newly diagnosed breast cancer patients with dense breasts. Semi-quantitative analysis as a parameter of BSGI may help classify the sub-type of an invasive ductal carcinoma in addition to the pathology. Because Chinese women have unique breast density, BSGI may improve the early detection of breast cancer to reduce breast cancer morbidity and mortality.
Abbreviations
BSGI, breast specific gamma imaging; MMG, mammography; MRI, magnetic resonance imaging; Se, sensitivity; Sp, specificity; US, ultrasound; YI, yueden’s index
References
Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014;64(1):9–29.
Fan L, Strasser-Weippl K, Li J-J, St Louis J, Finkelstein DM, Yu K-D, et al. Breast cancer in China. Lancet Oncol. 2014;15(7):e279–89.
Jia M, Zheng R, Zhang S, Zeng H, Zou X, Chen W. Female breast cancer incidence and mortality in 2011. China J Thorac Dis. 2015;7(7):1221–6.
Oeffinger KC, Fontham ET, Etzioni R, Herzig A, Michaelson JS, Shih YC, et al. Breast cancer screening for women at average risk: 2015 guideline update from the American cancer society. JAMA. 2015;314(15):1599–614.
Pike MC, Pearce CL. Mammographic density, MRI background parenchymal enhancement and breast cancer risk. Ann Oncol. 2013;24(8):viii37–41.
DeMartini WB, Liu F, Peacock S, Eby PR, Gutierrez RL, Lehman CD. Background parenchymal enhancement on breast MRI: impact on diagnostic performance. AJR Am J Roentgenol. 2012;198(4):W373–380.
Del Vecchio S, Salvatore M. 99mTc-MIBI in the evaluation of breast cancer biology. Eur J Nucl Med Mol Imaging. 2004;31(S1):S88–96.
Jones EA, Phan TD, Blanchard DA, Miley A. Breast-specific gamma-imaging: molecular imaging of the breast using 99mTc-sestamibi and a small-field-of-view gamma-camera. J Nucl Med Technol. 2009;37(4):201–5.
Bekis R, Degirmenci B, Aydin A, Ozdogan O, Canda T, Durak H. Correlation between 99mTc-MIBI uptake and angiogenesis in MIBI-positive breast lesions. Nucl Med Biol. 2005;32(5):465–72.
Weiss A, Anderson JE, Chang DC. Comparing the national surgical quality improvement program with the nationwide inpatient sample database. JAMA surg. 2015;150(8):815–6.
Sun Y, Wei W, Yang HW, Liu JL. Clinical usefulness of breast-specific gamma imaging as an adjunct modality to mammography for diagnosis of breast cancer: a systemic review and meta-analysis. Eur J Nucl Med Mol Imaging. 2013;40(3):450–63.
DA Bluemke GC, Chen MH, DeAngelis GA, DeBruhl N, Harms S, Heywang-Köbrunner SH, et al. Magnetic resonance imaging of the breast prior to biopsy. JAMA. 2004;292(22):2735–42.
Goldsmith SJ, Parsons W, Guiberteau MJ, Stern LH, Lanzkowsky L, Weigert J, et al. SNM practice guideline for breast scintigraphy with breast-specific gamma-cameras 1.0. J Nucl Med Technol. 2010;38(4):219–24.
Gradishar WJAB, Balassanian R, Blair SL, Burstein HJ, Cyr A, Elias AD, et al. Breast cancer version 2.2015. J Natl Compr Canc Netw. 2015;13(4):448–75.
Tan H, Jiang L, Gu Y, Xiu Y, Han L, Wu P, Zhang H, Shi H. Visual and semi-quantitative analyses of dual-phase breast-specific gamma imaging with Tc-99m-sestamibi in detecting primary breast cancer. Ann Nucl Med. 2014;28(1):17–24.
Tadwalkar RV, Rapelyea JA, Torrente J, Rechtman LR, Teal CB, McSwain AP, et al. Breast-specific gamma imaging as an adjunct modality for the diagnosis of invasive breast cancer with correlation to tumour size and grade. Br J Radiol. 2012;85(1014):e212–216.
Kessler R, Sutcliffe JB, Bell L, Bradley YC, Anderson S, Banks KP. Negative predictive value of breast-specific gamma imaging in low suspicion breast lesions: a potential means for reducing benign biopsies. Breast J. 2011;17(3):319–21.
Meissnitzer T, Seymer A, Keinrath P, Holzmannhofer J, Pirich C, Hergan K, et al. Added value of semi-quantitative breast-specific gamma imaging in the work-up of suspicious breast lesions compared to mammography, ultrasound and 3-T MRI. Br J Radiol. 2015;88(1051):20150147.
Kim BS, Moon BI, Cha ES. A comparative study of breast-specific gamma imaging with the conventional imaging modality in breast cancer patients with dense breasts. Ann Nucl Med. 2012;26(10):823–9.
Werner J, Rapelyea JA, Yost KG, Brem RF. Quantification of radio-tracer uptake in axillary lymph nodes using breast specific gamma imaging (BSGI): benign radio-tracer extravasation versus uptake secondary to breast cancer. Breast J. 2009;15(6):579–82.
Bevers TBAB, Bonaccio E, Buys S, Daly MB, Dempsey PJ, Farrar WB, et al. NCCN clinical practice guidelines in oncology: breast cancer screening and diagnosis. J Natl Compr Canc Netw. 2009;7(10):1060–96.
Tozaki M, Isomoto I, Kojima Y, Kubota K, Kuroki Y, Ohnuki K, et al. The Japanese breast cancer society clinical practice guideline for screening and imaging diagnosis of breast cancer. Breast cancer. 2015;22(1):28–36.
Friedewald SM, Rafferty EA, Rose SL, Durand MA, Plecha DM, Greenberg JS, et al. Breast cancer screening using tomosynthesis in combination with digital mammography. JAMA. 2014;311(24):2499–507.
Knuttel FMMG, van den Bosch MA, Gilhuijs KG, Peters NH. Current clinical indications for magnetic resonance imaging of the breast. J Surg Oncol. 2014;110(1):26–31.
Zhou M, Johnson N, Gruner S, Ecklund GW, Meunier P, Bryn S, et al. Clinical utility of breast-specific gamma imaging for evaluating disease extent in the newly diagnosed breast cancer patient. Am J Surg. 2009;197(2):159–63.
Johnson N, Sorenson L, Bennetts L, Winter K, Bryn S, Johnson W, et al. Breast-specific gamma imaging is a cost effective and efficacious imaging modality when compared with MRI. Am J Surg. 2014;207(5):698–701.
Yoon HJ, Kim Y, Chang KT, Kim BS. Prognostic value of semi-quantitative tumor uptake on Tc-99m sestamibi breast-specific gamma imaging in invasive ductal breast cancer. Ann Nucl Med. 2015;29(7):553–60.
Kim SJ, Kim IJ, Bae YT, Kim YK, Kim DS. Comparison of quantitative and visual analysis of Tc-99m MIBI scintimammography for detection of primary breast cancer. Eur J Radiol. 2005;53(2):192–8.
Zhou M, Johnson N, Blanchard D, Bryn S, Nelson J. Real-world application of breast-specific gamma imaging, initial experience at a community breast center and its potential impact on clinical care. Am J Surg. 2008;195(5):631–5.
Park JS, Lee AY, Jung KP, Choi SJ, Lee SM, Kyun BS. Diagnostic performance of breast-specific gamma imaging (BSGI) for breast cancer: usefulness of dual-phase imaging with (99m)Tc-sestamibi. J Nucl Med Mol Imaging. 2013;47(1):18–26.
Acknowledgments
The authors would like to thank the members of the research group for useful discussions. We also thank Dr Fang Xu, Department of Radiology, Second Affiliated Hospital, Zhejiang University School of Medicine, for her contributions.
Funding
This work was supported by grants from the Natural Science Foundation of China (81202098), the Science and Technology Department of Zhejiang Province (2012C24016), and the Zhejiang Provincial Natural Science Foundation of China (LY12H16014, LY13H160014 and LY14H160043).
Availability of data and materials
The data involved in the current study are available upon request. Anyone who is interested in the information should contact drhuangjian@zju.edu.cn.
Authors’ contributions
XY, GH and ZZ carried out the data analysis and drafted the manuscript; FQ had significant roles in the data acquisition; YC, YD carried out the quality control of data and algorithms; JH had significant roles in the study design and manuscript review; XS and XW formulated the research question, supervised the research program and edited the manuscript. HZ played a key role in implement BSGI test, revising the manuscript. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
This study was approved by Second Affiliated Hospital of Zhejiang University School of Medicine ethics committee and all the patients had given written informed consent.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Yu, X., Hu, G., Zhang, Z. et al. Retrospective and comparative analysis of 99mTc-Sestamibi breast specific gamma imaging versus mammography, ultrasound, and magnetic resonance imaging for the detection of breast cancer in Chinese women. BMC Cancer 16, 450 (2016). https://doi.org/10.1186/s12885-016-2537-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-016-2537-1