
Abstract
Background
Hereditary leiomyomatosis and renal cell carcinoma (HLRCC) is an autosomal dominant tumor susceptibility syndrome, and the disease-related gene has been identified as fumarate hydratase (fumarase, FH). HLRCC-associated kidney cancer is an aggressive tumor characterized by early metastasis to regional lymph nodes and distant organs. Since early diagnosis and provision of definitive therapy is thought to be the best way to reduce the tumor burden, it is widely accepted that germline testing and active surveillance for an at-risk individual from a family with HLRCC is very important. However, it still remains controversial how we should treat HLRCC-associated kidney cancer. We successfully treated the patient with locally advanced HLRCC-associated kidney cancer, who has received active surveillance because of at-risk individual, by radical nephrectomy and extended retroperitoneal lymph node dissection, and examined surgically resected samples from a molecular point of view.
Case presentation
We recommended that 13 at-risk individuals from a family with HLRCC should receive active surveillance for early detection of renal cancer. A 48-year-old woman with a left renal tumor and involvement of multiple regional lymph nodes with high accumulation of fluorine-18-deoxyglucose on positron emission tomography was treated with axitinib as a neoadjuvant therapy. Preoperative axitinib induced the shrinkage of the tumor with decreased fluorine-18-deoxyglucose accumulation. Resected samples showed two thirds tumor tissue necrosis as well as high expression of serine/threonine kinase Akt and low expression of nuclear factor E2-related factor 2 (Nrf2) which activates anti-oxidant response and protects against oxidative stress in viable cancer cells. Targeted next-generation sequencing revealed that FH mutation and loss of the second allele were completely identical between blood and tumor samples, suggesting that FH mutation plays a direct role in FH-deficient RCC. She has remained well after radical operation for over 33 months.
Conclusions
FH mutation plays a role in tumorigenic feature, a metabolic shift to aerobic glycolysis, and increased an anti-oxidant response phenotype in HLRCC-associated kidney cancer.
Similar content being viewed by others


Background
Hereditary leiomyomatosis and renal cell cancer (HLRCC, Online Mendelian Inheritance in Man accession number 605839) is a recently identified autosomal dominant tumor susceptibility syndrome that is characterized by a predisposition to develop benign leiomyomas of the skin and the uterus (fibroids and myomas), as well as aggressive renal cell cancer with papillary type 2 (pRCC2) or collecting duct histology [1–3]. The disease-related gene has been identified as fumarate hydratase (fumarase, FH, Online Mendelian Inheritance in Man accession number 136850) located at 1q43. FH encodes an enzyme that is part of the mitochondrial tricarboxylic acid (TCA) cycle involved in cellular energy metabolism and appears to function as a tumor suppressor since its activity is very low or absent in tumors from individuals with HLRCC. HLRCC-associated kidney cancer has distinctive architectural and morphologic features, is particularly aggressive, and tends to metastasize to regional lymph nodes and distant organs early [4]. Therefore, a high detection rate of mutations in HLRCC families may enable early identification of at-risk individuals and allow early initiation of therapy while their tumors are still small. However, it stills remains controversial how we should treat HLRCC-associated kidney cancer [5]. So far, there have been several case reports regarding HLRCC-associated kidney cancer, however, most of those were reporting the mutation analysis of FH, pathological features, and clinical course. Furthermore, to our knowledge, there have been no case reports of the patients of at-risk of HLRCC-associated with kidney cancer who received active surveillance and were treated successfully, and little is known about the relationship between the clinicopathological features and molecular changes associated with targeting therapy in this disease. In the present study, we successfully treated a patient with locally advanced HLRCC-associated pRCC2 by neoadjuvant administration of axitinib and subsequent radical nephrectomy and extended retroperitoneal lymph node dissection.
FH-deficient RCC is characterized by enhanced aerobic glycolysis and increased anti-oxidant response phenotype [6, 7]. Overactivation of phosphatidylinositol 3‘kinase (PI3K), serine/threonine protein kinase B (Akt), and mammalian target of rapamycin (mTOR) pathway has been reported in RCC. Inhibition of Akt disrupts transcription of glucose transporter protein-1 (GLUT1) and its translocation to the plasma membrane to promote glucose utilization independent of an effect on cell proliferation [8]. Phosphorylation at two sites is required for full activation of Akt, since it is phosphorylated by PI3K-dependent kinase-1 (PDK1) at a threonine residue in the catalytic domain (Thr-308) and by PI3K-dependent kinase-2 (PDK2) at a serine residue (Ser-473) in the carboxy-terminal hydrophobic motif [9]. mTOR has dual rapamycin-sensitive (mTOR-raptor complex: mTORC1) and rapamycin-insensitive (mTOR-rictor complex: mTORC2) functions. mTORC1 is activated by PI3K-Akt and it phosphorylates S6 and eukaryotic translation initiation factor 4E-binding protein 1 (4EBP1), thereby promoting translation and protein synthesis. mTORC2 regulates the actin cytoskeleton and also possesses PDK2 activity that phosphorylates Ser-473 at the carboxy-terminus of Akt, which is essential for activation of Akt [10, 11], and mTORC2-pAkt(Ser-473) signaling affects energy metabolism and cell survival [12]. Activation of Akt may increase cell viability after inhibition of mTORC1 [9]. Hypoxia-inducible factor (HIF)1α expression is dependent on both raptor and rictor, whereas HIF2α expression only depends on rictor, with HIF2α and mTORC2 being more important in RCC [13]. Moreover, phosphorylation of Ser-473 in Akt is considered to be key molecular step in the progression of RCCs and could be a potential target [10, 11, 14]. Furthermore, available reports support HIF-dependent pseudo-hypoxia manner as the mechanism of tumorigenesis in HLRCC [15]. In FH-deficient kidney cancer cells, increased fumarate inactivate prolyl hydroxylases, leading to stabilization of HIF, and increased HIF target genes such as GLUT1, vascular endothelial growth factor (VEGF), platelet-derived growth factor (PDGF), and transforming growth factor (TGF)α, which facilitate tumor growth [7, 16].
On the other hand, HIF-independent manner has been recently reported [17]. FH-deficiency leads to succination of Kelch-like ECH-associated protein 1 (Keap1), stabilization of nuclear factor E2-related factor 2 (Nrf2), and induction of stress-response genes including HMOX1, which is important for the survival of FH-deficient cells. The Keap1-Nrf2 pathway is the major regulator of cytoprotective responses to oxidative and electrophilic stress. Although cell signaling pathways triggered by the transcription factor Nrf2 prevent cancer initiation and progression in normal and premalignant tissues, in fully malignant cells Nrf2 activity provides growth advantage by increasing cancer chemoresistance and enhancing tumor cell growth, and high Nrf2 protein level is associated with poor prognosis in cancer [18]. FH loss results in Keap1 inactivation and Nrf2-dependent activation of anti-oxidant pathways [19, 20].
Axitinib is a potent, selective, second-generation inhibitor of VEGF receptor (VEGFR) 1, 2, and 3 that blocks VEGFRs at sub-nanomolar drug concentrations [21], and relative potency of axitinib is 50–450 times greater than that of the first-generation VEGFR inhibitors like sorafenib or sunitinib [22]. In order to investigate the roles of Akt-mTOR pathway and Nrf2 anti-oxidant response element transcription pathway in HLRCC-associated kidney cancer, we examined the expressions of phosphorylated-Akt (Ser-473) (pAkt(Ser-473), phosphorylated-Akt (Thr-308) (pAkt(Thr-308), phosphorylated-S6 ribosomal protein (Ser-235/236) (pS6), and Nrf2 in surgically resected samples. We also investigated FH mutations by sequencing the coding exons and intron flanking regions in both blood and tumor samples by targeted next-generation sequencing analysis. Such information might be useful to understand the signaling pathway in HLRCC-associated kidney cancer from a molecular point of view.
Case presentation
A 48-year-old woman (III-8, a sister of the proband from this HLRCC family) underwent abdominal ultrasonography annually at a local clinic after 2007, and presented with a left renal mass detected by an ultrasonography and was introduced to our hospital in March 2013 (Additional file 2: Figure S1).
She had undergone enucleation myomectomy for uterine leiomyomatosis at the age of 29 years at another hospital, while hysterectomy had been performed for recurrence large uterine leiomyomatosis at the age of 39 years at other hospital. In 2007 (when she was 40), her sister was diagnosed with HLRCC having a novel FH mutation at 241,671,938 bp (C574T) by direct sequencing of the FH gene from leukocyte DNA. Her sister subsequently died of HLRC-associated advanced renal cancer. In 2007, sequencing of DNA extracted from blood cells of this patient confirmed that she also had the same FH mutation as her sister [23]. After 2007, we recommended that 13 members of this family with the FH mutation should receive active surveillance by annual imaging (abdominal plain computed tomography (CT) or ultrasonography) at a convenient clinic (Fig. 1).

Pedigree. Generations are represented by Roman numerals and individuals are shown by Arabic numerals. The present patient is III-8 (indicated by the arrow) and the proband is III-9. “Mut” shows mutation screening. “Mut +” and “Mut −” indicate mutation-positive and mutation-negative individuals, respectively
Laboratory tests revealed moderate anemia (hemoglobin: 9.3 g/dl) and elevation of serum C-reactive protein (CRP: 3.19, normal < 0.3 mg/dl). Karnofsky performance status (KPS) was 100 %. Plain CT scans obtained at our hospital showed a left renal tumor with a diameter of 7 cm and involvement of multiple regional para-aortic lymph nodes, but no distant metastases (cT3aN1M0) (Fig. 2a). Positron emission tomography (PET) showed fluorine-18-deoxyglucose (FDG) accumulation in the renal tumor and the metastatic lymph node and the maximum standardized uptake value (SUVmax) was 15.3 and 7.5, respectively (Figs. 2b,c).

Positron emission tomography (PET) with [18 F] fluorodeoxyglucose (18 F-FDG PET) / plain computed tomography (CT). Pre: Before treatment with axitinib. Post: After administration of axitinib for 4 weeks. a, d: Plain abdominal CT shows that the primary left renal tumor and enlarged lymph nodes have decreased in size. b, e: SUVmax of the primary tumor decreased from 15.3 to 2.9 after administration of axitinib. c, f: SUVmax of the regional lymph nodes decreased from 7.5 to 2.3 after administration of axitinib
Her risk classification for renal cancer was intermediate risk according to the Memorial Sloan-Kettering Cancer Center (MSKCC) criteria. However, the prognosis of patients with HLRCC-associated renal cancer, in particular those with extrarenal involvement, is extremely poor. Furthermore, her tumors showed a different imaging pattern from that of typical clear cell RCC (Additional file 2: Figure S1), and the histology of the renal cancers in her relatives was non-clear cell RCC (undifferentiated RCC in her mother, pRCC2 in both her sister and maternal cousin). Thus, the tumor of this patient seemed likely to be non-clear cell carcinoma, but we did not perform needle biopsy to avoid dissemination of cancer cells.
In order to decrease the tumor burden and improve the feasibility of surgery, we selected preoperative treatment with a multi-targeted tyrosine kinase inhibitor (TKI). In comparison to first-generation TKIs targeting the VEGFR, axitinib is a potent second-generation inhibitor of VEGFRs with a higher affinity for tyrosine kinase and achieves stronger inhibition of kinase activity with fewer adverse effects such as thrombocytopenia. Additionally, first-generation inhibitors block other targets, such as PDGF receptors (PDGFR), KIT (cluster of differentiation 117: CD117), b-rapidly accelerated fibrosarcoma (RAF), and Fms-like tyrosine kinase 3 (FLT-3), which are not substantially inhibited by axitinib. These off-target activities might contribute to the adverse effects of the first-generation inhibitors, suggesting that more specific inhibitors of VEGFR such as axitinib might have an enhanced therapeutic window. We recently successfully treated a patient who had a large right RCC showing sarcomatoid differentiation that directly invaded the duodenum and inferior vena cava with regional lymph node involvement. In this patient, radical right nephrectomy, cavotomy with thrombectomy, and pancreatoduodenectomy were successfully performed after administration of axitinib as first-line neoadjuvant therapy without severe toxicity [24].
We selected axitinib as preoperative molecular-targeting therapy to decrease the tumor size before surgery with good tolerability. Administration of axitinib starting at 5 mg/day was scheduled for four to six weeks before radical surgery involving left nephrectomy and extended retroperitoneal lymph node dissection (para-aortic and aorto-caval nodes). After 1 week, the dose of axitinib was increased to 14 mg/day. After four weeks of total dose of axitinib of 329 mg (5 mg/day for continuous 7 days and 14 mg/day for following continuous 21 days), there were no apparent adverse events of > grade 3, excluding headache and hypertension (systolic blood pressure > 200 mmHg). Tumor shrinkage and a decrease of SUVmax were observed (Figs. 2d-f). Subsequently, we successfully carried out radical left nephrectomy and extended retroperitoneal lymph node dissection (para-aortic and aorto-caval nodes). Macroscopically, the tumor was an invasive whitish-yellowish mass with partial necrosis. Pathological examination confirmed pRCC2 with Fuhrman grade 3 differentiation (pT3apN1M0). The pathological effect of axitinib was grade 2 (i.e., two-thirds necrosis of the tumor). The patient has been receiving axitinib at 5 mg/day in the manner of one cycle of one week (5 days on - 2 days off) as adjuvant therapy for 33 months, and remains well with no evidence of recurrence at 33 months after the operation.
Materials and methods
Western blotting and Immunohistochemistry
We performed Western blotting using a rabbit anti-human antibody targeting pAkt (Ser-473) (Cell Signaling Technology, Inc; PhosphoPlus Akt (Ser-473) Antibody Kit; # 9270, Danvers, MA), a rabbit anti-human antibody for pAkt (Thr-308) (Cell Signaling Technology, Inc; Phospho-Akt (Thr308) Antibody Kit; # 2965, Danvers, MA), a rabbit anti-human antibody targeting phosphorylated ribosomal protein S6 kinase (pS6) (2 F9, Cell Signaling Technology, Inc; # 4856), as described previously [25].
Immunohistochemical staining was performed with anti-Nrf2 monoclonal antibody (abcam, # ab-62352, Cambrige, UK) using the immunoperoxidase technique and microwave treatment of tissue sections in citrate buffer as described previously [26].
For comparison to the present case, we examined the expression of pAkt (Ser-473), pAkt (Thr-308) and pS6 in surgical specimens of five patients with locally advanced clear cell RCCs with pT3bpN1 or pT4 who received preoperative axitinib as well as the current patient, and of Nrf2 in HLRCC-associated kidney cancer tissues of the proband (III-9) and maternal cousin (III-4) who received no prior treatment.
DNA samples
Germline DNA was extracted from leukocytes according to the standard protocols. Frozen tumor samples were ground to a powder in liquid nitrogen and 30–50 mg of the sample was used for DNA extraction with the AllPrep kit (Qiagen). DNA was quantified and its purity assessed with a NanoDrop ND-1000 spectrophotometer (Labtech).
Next-generation sequencing
We investigated FH mutations by sequencing the coding exons and intron flanking regions in both blood and tumor samples. For targeted next-generation sequencing analysis, the custom primers for FH region were designed using Ampliseq Designer (Life Technologies). Library construction and sequencing were carried out using Ion AmpliSeq Library Kit 2.0, Ion PGM IC 200 kit and Ion PGM (Life Technologies) according to the manufacturer's instructions (Additional file 1).
Data analysis
After a sequencing reaction, the raw signal data were analyzed using Torrent Suite version 4.2.1. The pipeline includes signaling processing, base calling, quality score assignment, adapter trimming, mapping to GRCH37/hg19 reference, detection of mapping quality, and variant calling. After completion of the primary data analysis, a list of detected alleles, sequence variant [single-nucleotide Polymorphisms (SNPs) and the insertion or the deletion (Indels)] were compiled in a variant call file format and presented via the web-based user interface. The results of mapping and variant calling were visualized using Integrative Genome viewer (Broad Institute) (Additional file 1).
Results
Expression of pAkt and pS6
In six patients, five clear cell RCCs and this case, receiving preoperative axitinib treatment, similar findings were observed (shrinkage of the tumor, decreased SUVmax of the tumor, and two thirds tumor tissue necrosis). For the other patients with cT3bN1 or cT4 clear cell RCC, tumor tissues showed heterogeneous changes. Some of tumor tissues showed much lower expression of pAkt (Ser-473), pAkt (Thr-308), and pS6 than other tissues. On the other hand, in our current patient with cT3aN1M0, pRCC2, tumor tissues showed high expression of pAkt (Ser-473) and pAkt (Thr-308), as well as very low expression of pS6 (Fig. 3).

Western blotting. Western blotting for surgically resected tissues (M: marker, N: normal tissue, T1-3: three different parts of tumor tissues). In a patient with cT3bN1M1 clear cell renal cell carcinoma (ccRCC-1) who received preoperative axitinib as well as the current patient, tumor tissues obtained by nephrectomy after axitinib treatment showed heterogeneous changes. Some tumor tissue (T2 and T3) showed much lower expression of pAkt (Ser-473), pAkt (Thr-308), and pS6 than other tissue (T1). Similarly, in the other patients with cTanyN1Many ccRCCs (ccRCC-2 to −4) treated with preoperative axitinib, tumor tissues showed heterogeneous pattern. These findings indicate that some parts of the cancer would show a good response to axitinib but other parts would not. On the other hand, in the present patient with cT3aN1M0, renal cell cancer with papillary type 2 (pRCC2), surgically resected cancer tissues (T1 to T3) showed high expression of pAkt (Ser-473) and pAkt (Thr-308), as well as very low expression of pS6, indicating that the mTORC2-Akt signaling may be more important for molecular targeting than the mTORC1-S6 pathway in HLRCC-associated kidney cancer compared with clear cell RCC
Expression of Nrf2
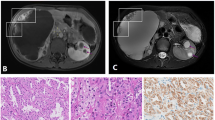
While much of tumor cells showed diffusely strong reaction for anti-Nrf2 antibody in the proband (III-9) and maternal cousin (III-4) (Figs. 4a, 4b), some of viable tumor cells showed weak staining in the present case (III-8) (Fig. 4c). Normal kidney and clear cell RCC tissues showed negative staining (Fig. 4d).

Immunohistochemistry. Immunohistochemical analysis of Nrf2 expression using anti-Nrf2 monoclonal antibody in HLRCC-associated kidney cancer (a-c) (X 200 magnification. Scale bars showed 200 μm). a, b: Much of cancer cells showed diffuse strong brown staining in a membrane and cytoplasm for anti-Nrf2 antibody in the proband (III-9) (a) and maternal cousin (III-4) (b) with non-prior therapy. c: Some of viable cancer cell showed weak reaction in the present case (III-8) with neoadjuvant axitinib therapy. d: Clear cell renal cell carcinoma tissues randomly selected for this study showed negative staining
Molecular genetic analysis
The average Ion PGM™ sequencing output per sample was 150 mega bases with 0.9 million sequencing reads. Of the 16 amplicons in the FH-gene, 100 % achieved a minimum average sequencing depth of 500X and mean depth were 28,419X-34,591X. In samples, the Ion PGM™ detected SNPs and deletions, details of results are shown in Table 1. In the blood and resected kidney cancer tissue samples from this patient and the proband (III-9), common SNPs on exon5 (position; 241,671,938 bp, C574T, codon p. H235Y) was detected, and new alleles were detected at intron regions.
Discussion and conclusions
In the present study, next-generation sequencing revealed that FH mutation and loss of the second allele were completely identical between blood and tissue samples from this patient and her sister (III-9) who died of advanced HLRCC-associated kidney cancer, indicating that FH-deficient RCC is a unique neoplasm that progresses directly by FH mutation.
In FH-deficient RCC, oxidative phosphorylation is impaired and the cells undergo a shift to aerobic glycolysis, consistent with the Warburg effect [6, 7]. The conversion of glucose metabolism from oxidation to glycolysis, the Warburg effect, is one of the representative strategies for generation of adenosine triphosphate (ATP) in cancer cells [27]. Reprogramming of energy metabolism, the conversion of glucose metabolism from oxidation to glycolysis, the Warburg effect, can now be viewed as one of the “hallmarks of cancer” [28]. RCC is characterized by impaired oxidative phosphorylation and a metabolic shift to aerobic glycolysis, a form of metabolic reprogramming. In particular, HLRCC-associated kidney cancer cells have lost the ability to completely cycle through the TCA cycle, due to the loss of FH enzyme activity, and have effectively lost the ability to perform oxidative phosphorylation indicating that these cancers exist in a state of enforced dependence upon glycolysis and represent a notable example of the Warburg effect [7]. Thus, HLRCC-associated kidney cancer might be a clinical model to study energy metabolism deregulation, as well as developing new targeted therapeutic approaches for TCA cycle enzyme-deficient cancers [29]. In this HLRCC-associated pRCC2 case, surgically resected cancer tissue showed high expression of pAkt (Ser-473) and pAkt (Thr-308), as well as very low expression of pS6, indicating that we should study the roles of mTORC2-Akt signaling in HLRCC-associated kidney cancer from the metabolic point of view in more patients in the forthcoming study.
On the other hand, FH-deficient RCC is also characterized by increased oxidative stress and elevated levels of reactive oxygen, thus effective anti-oxidant response is critical for continued growth [6, 7]. In this study, subsequent immunohistochemical staining for Nrf2 protein in the HLRCC-associated pRCC2 also showed intense positive staining (III-9 and −4). At the same time, normal kidney and clear cell RCC tissues showed negative staining. Our findings were consistent with those by previous study [20], indicating that Nrf2 was indeed activated in these FH-deficient RCC tissues. Thus, FH-deficient RCC appeared to be linked to increased expression of anti-oxidant genes with accompanied by the accumulation of Nrf2. In this HLRCC-associated pRCC2 case treated with neoadjuvant axitinib, some of viable cancer cells showed weak reaction for anti-Nrf2 antibodies compared to the tumors of the proband (III-9) and maternal cousin (III-4) who received no prior treatment in which much of cancer cells showed diffusely strong reaction, indicating that axitinib might suppress the Nrf2 pathway by unknown mechanism. Since we do not have preoperative tumor tissues and stored blood samples, we could not compare the VEGF levels between before and after administrating axitinib in the present study. However, in addition to pAkt, pS6, and Nrf2, we should also analyze repeatedly the VEGF, GLUT1 or HIF using tissue and blood samples in order to correspond to dynamic change of the tumor and the general condition which is continuously changed with time in the future.
From a molecular point of view, insight in the cellular pathways involved in pathogenesis of HLRCC might lead to specific options for early diagnosis and targeted therapies. However, since this is only a single case report about our experience with surgery after axitinib treatment for HLRCC-associated kidney cancer, the results should be interpreted with consideration of such limitations and definite conclusions cannot be obtained. While an investigation of the usefulness of axitinib for preoperative or neoadjuvant therapy in patients with locally advanced RCC is now ongoing, availability of axitinib for adjuvant therapy for RCCs has not yet elucidated. Although there was no detailed information regarding histological type of papillary RCC in a previous study using other kinase inhibitors in papillary RCCs, sunitinib seems to be more effective than sorafenib [30]. Furthermore, a phase II trial of bevacizumab and erlotinib in patients with advanced HLRCC-associated pRCC2 as well as sporadic pRCC2 is currently under way (NCT01130519). Therefore, it would be great to conduct in vitro studies using established two HLRCC kidney cancer lines, UOK262 and UOK268 [29, 31].
It is thought that early diagnosis and provision of definitive therapy is the best way to reduce the tumor burden as rapidly as possible. Unlike other hereditary renal cancers, HLRCC-associated kidney cancer is an aggressive tumor characterized by metastasis to regional and distant lymph nodes [4]. A recent report regarding HLRCC-associated kidney cancer recommended that surveillance should preferably be annual abdominal MRI, and that treatment of renal tumors should be prompt and generally involve wide surgical excision with consideration of retroperitoneal lymph node dissection [5]. Thirteen at-risk individuals from this HLRCC family had received active surveillance by annual imaging (abdominal plain CT or ultrasonography) at a convenient clinic, however, as shown in Fig. 2 and Additional file 2: Figure S1, we may overlook the smaller tumors associated with HLRCC in plain CT and/or ultrasonography because of low contrast of the tumors to the normal kidney. Although enhanced CT may be useful, given the radiation exposure and the adverse effect of contrast medium, magnetic resonance imaging (MRI) seems to be suitable for surveillance as recommended [5]. Subsequently, we would ask their attending physicians at a convenient clinic annual MRI imaging study every twelve months.
Currently, surgical intervention is the only therapy available to patients with HLRCCassociated kidney cancers. The patient underwent radical left nephrectomy and extended retroperitoneal lymph node dissection (para-aortic and aorto-caval nodes) after administration of preoperative axitinib. It is difficult issue how we should follow the patient. The patient undergoes imaging examination of chest CT and abdominal MRI at least every three months and PET scan every six months, and remains well with no evidence of recurrence at 33 months after the operation. The patient is receiving axitinib as adjuvant therapy, and we would like to decrease the dose of axitinib gradually. Careful patient selection and meticulous surgical technique are essential in the treatment of patients with HLRCC-associated kidney cancer, and these points should be further emphasized in the era of targeted therapy. Collection of HLRCC-affected family data dedicated to monitoring of patients will provide information on clinical variability and outcome measures that will allow clinicians to adjust diagnostic criteria and management recommendations. It is our hope that more patients with HLRCC-associated kidney cancer will be able to achieve a better outcome.
Ethics approval
The patient and many of individuals in this family signed a consent form that was approved by our institutional Committee on Human Rights in Research for the analysis of germline and somatic DNA. On the other hand, some individuals could not come to our hospital and we could not get approval for DNA analysis, however, all participants in this family give approval for the publication of their clinical and other details in written informed consent. Furthermore, if the participant has died, then consent for publication has been sought from the next of kin of the participant. Thus, we have 'consent to publish' from all the individuals represented in the family tree in Fig. 1. This study was conducted in accordance with the Helsinki Declaration and was approved by the Dokkyo Medical University Hospital ethical review board.
Consent
Written informed consent was obtained from the patient and their relatives to sequence their DNA and for the publication of this case report and any accompanying sequence data or images. A copy of the written consent is available for review by the Editor of this journal.
Abbreviations
- 4EBP1:
-
4E-binding protein 1
- Akt:
-
protein kinase B
- ATP:
-
adenosine triphosphate
- ccRCC:
-
clear cell renal cell carcinoma
- Chrom:
-
chromosome
- CRP:
-
C-reactive protein
- CT:
-
computed tomography
- DNA:
-
deoxyribonucleic acid
- FDG:
-
fluorine-18-deoxyglucose
- FH:
-
fumarate hydratase
- FLT-3:
-
Fms-like tyrosine kinase 3
- GLUT1:
-
glucose transporter protein-1
- HIF:
-
hypoxia-inducible factor
- HLRCC:
-
Hereditary Leiomyomatosis and Renal Cell Cancer
- Indels:
-
the insertion or the deletion
- Keap1:
-
Kelch-like ECH-associated protein 1
- KIT:
-
cluster of differentiation (CD)117
- KPS:
-
Karnofsky performance status
- MRI:
-
magnetic resonance imaging
- MSKCC:
-
Memorial Sloan-Kettering Cancer Center
- mTOR:
-
mammalian target of rapamycin
- mTORC1:
-
mTOR-raptor complex
- mTORC2:
-
mTOR-rictor complex
- Mut:
-
mutation
- Nrf2:
-
nuclear factor E2-related factor 2
- pAkt:
-
phosphorylated-Akt
- PCR:
-
polymerase chain reaction
- PDGF:
-
platelet-derived growth factor
- PDGFR:
-
PDGF receptor
- PDK1:
-
PI3K-dependent kinase-1
- PDK2:
-
PI3K-dependent kinase-2
- PET:
-
positron emission tomography
- PI3K:
-
phosphatidylinositol 3‘kinase
- pRCC2:
-
renal cell cancer with papillary type 2
- pS6:
-
phosphorylated-S6 ribosomal protein
- RAF:
-
rapidly accelerated fibrosarcoma
- RCC:
-
renal cell carcinoma: Ref, references
- Ser:
-
serine
- RNA:
-
ribonucleic acid
- SNPs:
-
single-nucleotide polymorphisms
- SUVmax:
-
maximum standardized uptake value
- TCA:
-
tricarboxylic acid
- TGF:
-
transforming growth factor
- Thr:
-
threonine
- TKI:
-
tyrosine kinase inhibitor
- VEGF:
-
vascular endothelial growth factor
- VEGFR:
-
VEGF receptor
References
Launonen V, Vierimaa O, Kiuru M, Isola J, Roth S, Pukkala E, Sistonen P, Herva R, Aaltonen LA. Inherited susceptibility to uterine leiomyomas and renal cell cancer. Proc Natl Acad Sci U S A. 2001;98:3387–92.
Tomlinson IP, Alam NA, Rowan AJ, Barclay E, Jaeger EE, Kelsell D, Leigh I, Gorman P, Lamlum H, Rahman S, Roylance RR, Olpin S, Bevan S, Barker K, Hearle N, Houlston RS, Kiuru M, Lehtonen R, Karhu A, Vilkki S, Laiho P, Eklund C, Vierimaa O, Aittomaki K, Hietala M, Sistonen P, Paetau A, Salovaara R, Herva R, Launonen V, Aaltonen LA. Germline mutations in FH predispose to dominantly inherited uterine fibroids, skin leiomyomata and papillary renal cell cancer. Nat Genet. 2002;30:406–10.
Alam NA, Rowan AJ, Wortham NC, Pollard PJ, Mitchell M, Tyrer JP, Barclay E, Calonje E, Manek S, Adams SJ, Bowers PW, Burrows NP, Charles-Holmes R, Cook LJ, Daly BM, Ford GP, Fuller LC, Hadfield-Jones SE, Hardwick N, Highet AS, Keefe M, MacDonald-Hull SP, Potts ED, Crone M, Wilkinson S, Camacho-Martinez F, Jablonska S, Ratnavel R, MacDonald A, Mann RJ, Grice K, Guillet G, Lewis-Jones MS, McGrath H, Seukeran DC, Morrison PJ, Fleming S, Rahman S, Kelsell D, Leigh I, Olpin S, Tomlinson IP. Genetic and functional analyses of FH mutations in multiple cutaneous and uterine leiomyomatosis, hereditary leiomyomatosis and renal cancer, and fumarate hydratase deficiency. Hum Mol Genet. 2003;12:1241–52.
Grubb III RL, Franks ME, Toro J, Middelton L, Choyke L, Fowler S, Torres-Cabala C, Glenn GM, Choyke P, Merino MJ, Zbar B, Pinto PA, Srinivasan R, Coleman JA, Linehan WM. Hereditary leiomyomatosis and renal cell cancer: a syndrome associated with an aggressive form of inherited renal cancer. J Urol. 2007;177:2074–9.
Menko FH, Maher ER, Schmidt LS, Middelton LA, Aittomäki K, Tomlinson I, Richard S, Linehan WM. Hereditary leiomyomatosis and renal cell cancer (HLRCC): renal cancer risk, surveillance and treatment. Fam Cancer. 2014;13:637–44.
Srinivaan R, Ricketts CJ, Sourbier C, Linehan WM. New strategies in renal cell carcinoma: Targeting the genetic and metabolic basis of disease. Clin Cancer Res. 2015;21:10–7.
Linehan WM, Rouault TA. Molecular pathways: Fumarate hydratase-deficient kidney cancer--targeting the Warburg effect in cancer. Clin Cancer Res. 2013;19:3345–52.
Ma WW, Jacene H, Song D, Vilardell F, Messersmith WA, Laheru D, Wahl R, Endres C, Jimemno A, Pomper MG, Hidalgo M. [18F]Fluorodeoxyglucose positron emission tomography correlates with Akt pathway activity but is not predictive of clinical outcome during mTOR inhibitor therapy. J Clin Oncol. 2009;27:2697–704.
Hay N. The Akt-mTOR tango and its relevance to cancer. Cancer Cell. 2005;8:179–83.
Sarbassov DD, Guertin DA, Ali SM, Sabatini DM. Phosphorylation and regulation of Akt/PKB by the rictor-mTOR complex. Science. 2005;307:1098–101.
Sarbassov DD, Ali SM, Kim DH, Guertin DA, Latek RR, Erdjument-Bromage H, Tempst P, Sabatini DM. Rictor, a novel binding partner of mTOR, defines a rapamycin-Insensitive and raptor-Independent pathway that regulates the cytoskeleton. Curr Biol. 2004;14:1296–302.
Betz C, Stracka D, Prescianotto-Baschong C, Frieden M, Demaurex N, Hall M. mTOR complex 2-Akt signaling at mitochondria-associated endoplasmic reticulum membranes (MAM) regulates mitochondrial physiology. Proc Natl Acad Sci U S A. 2013;110:12526–34.
Toschi A, Lee E, Gadir N, Ohh M, Foster DA. Differential dependence of hypoxia-inducible factors 1 alpha and 2 alpha on mTORC1 and mTORC2. J Biol Chem. 2008;283:34495–9.
Jonasch E, Corn P, Pagliaro LC, Warneke CL, Johnson MM, Tamboli P, Ng C, Aparicio A, Ashe RG, Wright JJ, Tannir NM. Upfront, randomized, phase 2 trial of sorafenib versus sorafenib and low-dose interferon alfa in patients with advanced renal cell carcinoma: clinical and biomarker analysis. Cancer. 2010;116:57–65.
Sudarshan S, Linehan WM, Neckers L. HIF and fumarate hydratase in renal cancer. Br J Cancer. 2007;96:403–7.
Bratslavsky G, Sudarshan S, Neckers L, Linehan WM. Pseudohypoxic pathways in renal cell carcinoma. Clin Cancer Res. 2007;13:4667–71.
Kinch L, Grishin NV, Brugarolas J. Succination of Keap1 and activation of Nrf2-dependent antioxidant pathways in FH-deficient papillary renal cell carcinoma type 2. Cancer Cell. 2011;20:418–20.
Sporn MB, Liby KT. NRF2 and cancer: the good, the bad and the importance of context. Nat Rev Cancer. 2012;12:564–71.
Ooi A, Wong JC, Petillo D, Roossien D, Perrier-Trudova V, Whitten D, Min BW, Tan MH, Zhang Z, Yang XJ, Zhou M, Gardie B, Molinié V, Richard S, Tan PH, Teh BT, Furge KA. An antioxidant response phenotype shared between hereditary and sporadic type 2 papillary renal cell carcinoma. Cancer Cell. 2011;20:511–23.
Adam J, Hatipoglu E, O'Flaherty L, Ternette N, Sahgal N, Lockstone H, Baban D, Nye E, Stamp GW, Wolhuter K, Stevens M, Fischer R, Carmeliet P, Maxwell PH, Pugh CW, Frizzell N, Soga T, Kessler BM, El-Bahrawy M, Ratcliffe PJ, Pollard PJ. Renal cyst formation in Fh1-deficient mice is independent of the Hif/Phd pathway: roles for fumarate in KEAP1 succination and Nrf2 signaling. Cancer Cell. 2011;20:524–37.
Rixe O, Bukowski RM, Michaelson MD, Wilding G, Hudes GR, Bolte O, Motzer RJ, Bycott P, Liau KF, Freddo J, Trask PC, Kim S, Rini BI. Axitinib treatment in patients with cytokine-refractory metastatic renal-cell cancer: a phase II study. Lancet Oncol. 2007;8:975–84.
Sonpavde G, Hutson TE, Rini BI. Axitinib for renal cell carcinoma. Expert Poin Investig Drugs. 2008;17:741–8.
Kamai T, Tomosugi N, Abe H, Kaji Y, Oyama T, Yoshida K. Protein profiling of blood samples from patients with hereditary leiomyomatosis and renal cell cancer by surface-enhanced laser desorption/ionization time-of-flight mass spectrometry. Int J Mol Sci. 2012;13:14518–32.
Yuki H, Kamai T, Kubota K, Abe H, Nishihara D, Mizuno T, Masuda A, Betsunoh H, Yashi M, Fukabori Y, Yoshida K. Axitinib for preoperative downstaging of renal cell carcinoma with sarcomatoid differentiation and direct invasion of the duodenum and inferior vena cava: A case report. OncoTargets Ther. 2014;7:289–95.
Furuya N, Kamai T, Shirataki H, Yanai Y, Fukuda T, Mizuno T, Kambara T, Nakanishi K, Abe H, Yoshida K-I. Serum interferon alpha receptor 2 mRNA may predict efficacy of interferon alpha with/without low-dose sorafenib for metastatic clear cell renal cell carcinoma. Cancer Immunol Immunother. 2011;60:793–808.
Kamai T, Takagi K, Asami H, Ito Y, Oshima H, Yoshida KI. Decreasing of p27Kip1 and cyclin E protein levels is associated with progression from superficial into invasive bladder cancer. Br J Cancer. 2001;84:1242–51.
Vander Heiden MG, Cantley LC, Thompson CB. Understanding the Warburg effect: the metabolic requirements of cell proliferation. Science. 2009;324:1029–33.
Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144:646–74.
Yang Y, Valera V, Sourbier C, Vocke CD, Wei M, Pike L, Huang Y, Merino MA, Bratslavsky G, Wu M, Ricketts CJ, Linehan WM. A novel fumarate hydratase-deficient HLRCC kidney cancer cell line, UOK268: a model of the Warburg effect in cancer. Cancer Genet. 2012;205:377–90.
Choueiri TK, Plantade A, Elson P, Negrier S, Ravaud A, Oudard S, Zhou M, Rini BI, Bukowski RM, Escudier B. Efficacy of sunitinib and sorafenib in metastatic papillary and chromophobe renal cell carcinoma. J Clin Oncol. 2008;26:127–31.
Yang Y, Valera VA, Padilla-Nash HM, Sourbier C, Vocke CD, Vira MA, Abu-Asab MS, Bratslavsky G, Tsokos M, Merino MJ, Pinto PA, Srinivasan R, Ried T, Neckers L, LInehan WM. UOK 262: fumarate hydratase deficient (FH-/FH-) hereditary leiomyomatosis renal cell carcinoma: in vitro and in vivo model of an aberrant energy metabolic pathway in human cancer. Cancer Genet Cytogenet. 2010;196:45–55.
Acknowledgements
This work was supported in part by Japanese Science Progress Society KAKENHI Grants (26462426) to Takao Kamai. The authors are special grateful to Hitomi Yamazaki for her excellent technique in this study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
Authors’ contributions
TK initiated the study, participated in its design and coordination, carried out the study, performed the statistical analysis, and drafted the manuscript. HA, KA, SM and SS carried out the study. YK and K-IY participated in the design of the study and helped to draft the manuscript. All authors read and approved the final manuscript.
Additional files
Additional file 1:
Supplementary Materials and Methods. (DOCX 270 kb)
Additional file 2: Figure S1.
Imaging of the left renal tumor. a: Ultrasonography, b: Enhanced CT, c: MRI T2W1, d: MRI gadolinium. Lt RCC: left renal cell carcinoma. mLM: metastatic lymph node tumor. These imaging were at pre-treatment with axitinib. (TIFF 1162 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Kamai, T., Abe, H., Arai, K. et al. Radical nephrectomy and regional lymph node dissection for locally advanced type 2 papillary renal cell carcinoma in an at-risk individual from a family with hereditary leiomyomatosis and renal cell cancer: a case report. BMC Cancer 16, 232 (2016). https://doi.org/10.1186/s12885-016-2272-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-016-2272-7