
Abstract
Background
Pilates has captured interest due to its possible advantages during pregnancy and childbirth. Although research indicates that Pilates may reduce labor duration, alleviate pain, and improve satisfaction with the childbirth experience, consensus on these outcomes remains elusive, underscoring the necessity for additional studies.
Aim
This systematic review and meta-analysis aimed to assess the impact of Pilates exercises on labor duration among pregnant women.
Methods
The online database was searched to yield the literature using the terms of ‘Pilates’, ‘childbirth’, and ‘labor duration’, and similar terms including PubMed, Clinical Key, Scopus, Web of Science, Embase, and Cochrane Database of Systematic Reviews up to June 25, 2023. Studies were considered eligible if they were randomized or clinical controlled trials (RCTs/CCTs) published in English, focusing on healthy pregnant women without exercise contraindications. The studies needed to include interventions involving Pilates or exercise movement techniques, a comparison group with no exercise, and outcomes related to labor duration, the period of the active phase, and the second stage of delivery.
Results
Eleven studies, totalling 1239 participants, were included in the analysis. These studies provided high-quality evidence from exercise only RCTs/CCTs. The findings indicated a significant reduction in the active phase of labor (8 RCTs, n = 1195; Mean Difference [MD] = -56.35, 95% Confidence Interval [CI] [-89.46 to -23.25]) and overall labor duration (8 RCTs, n = 898; MD = -93.93, 95% CI [-138.34 to -49.51]) in pregnant women who engaged in Pilates exercises compared to those who did not but doesn’t affect on the duration of the second stage of labor (7 RCTs, n = 1135; MD = -0.11, 95% CI [-7.21 to 6.99]).
Conclusions
While this review primarily addresses the effects of Pilates on healthy and low-risk pregnant women, the findings suggest a potential role for Pilates in shortening labor duration. Therefore, engaging in Pilates or similar physical activities is recommended for pregnant women to potentially facilitate a more efficient labor process.
Similar content being viewed by others

Introduction
Pilates is characterized as a distinct form of resistance and strength training [1], and has been described as a “healing exercise” [2]. The primary objective of Pilates is to establish muscular strength and flexibility by fortifying weaker muscles and augmenting the elasticity, and preparing the body of a pregnant woman for childbirth and postnatal recovery [3,4,5]. Pilates, a form of exercise increasingly popular in health promotion programs worldwide, especially during pregnancy, emerges as a promising activity in this context [6]. Several studies have investigated the impact of Pilates on various aspects of pregnancy and childbirth [3, 7]. Some studies suggest that Pilates may reduce perceived stress during pregnancy, potentially creating mental space for bonding with the unborn child and enhance maternal satisfaction [7,8,9]. This exercise method is recommended as a particularly relevant physical activity for healthy pregnant women, owing to its capacity to enhance postural coordination, flexibility, balance, and overall quality of life [8, 10]. Moreover, the Pilates method has been used by pregnant women to improve the physical and psychological outcomes of pregnancy, potentially reducing pain such as back pain and pain during labor [11, 12]. Additionally, Pilates has been reported to have no negative effects on gestational age, birth weight of infants, and APGAR scores [13]. However, the comparison of the effects of clinical Pilates exercises with and without childbirth training on pregnancy and birth results did not show any negative impact on the APGAR score [14].
Contemporary research posits that sedentary women should commence physical activity during pregnancy to mitigate these risks [15]. At the same time, there has been an increasing focus in recent years on enhancing the childbirth experience and employing techniques to reduce labor duration [16]. Another aspect that is described from previous studies is the established correlation between protracted labor and heightened risks of mortality, as well as maternal and perinatal complications [17,18,19,20]. These complications encompass a range of issues, including increased maternal fatigue, the necessity for induction and cesarean section, instrumental delivery, uterine atony, maternal mortality, elevated fetal distress, hypoxia, low apgar scores, and ultimately, fetal demise [21].
However, the effects of Pilates on childbirth outcomes are still a topic of debate. Some studies have shown that Pilates exercise alone had no significant effect on increasing the rate of natural childbirth in primiparous women [9]. Similarly, there is no consensus on the effects of Pilates methods with voluntary pelvic floor muscle contractions in pregnant women [22].
Research has also demonstrated that Pilates exercises applied during pregnancy could improve women’s core stability and balance levels and reduce their fear of childbirth [23]. While some studies suggest the potential benefits of Pilates on labor duration, there is still a lack of consensus on its overall impact. This systematic review and meta-analysis have been conducted with the objective of elucidating the impact of Pilates exercise on the duration of labor.
Methods
This systematic review has been meticulously conducted in alignment with the established protocols and recommendations outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [24].
Literature search and data collection
This research was conducted through June 2023 using the following search terms: (childbirth OR pregnancy OR pregnant OR labor OR obstetric) AND (Pilates OR physical activity OR exercise OR movement techniques) AND (duration of labor OR length of labor OR length of delivery). The research was carried out using the following databases: PubMed, Clinical Key, Scopus, Web of Science, Embase, and the Cochrane Database of Systematic Reviews. See the supplementary file for detailed search strategies specific to each database.
Studies selection and eligibility criteria
The main inclusion criteria for this systematic review, structured according to the PICOS framework, are as follows:
Population (P): Pregnant women.
Intervention (I): Pilates exercises and physical activity.
Comparison (C): No activity.
Outcomes (O): Duration of labor, active phase duration, second stage duration.
Study Design (S): Randomized Controlled Trials (RCT)/Clinical Controlled Trials (CCT).
Additionally, the studies must be; published in a peer-reviewed journal up to June 2023, and written in the English language.
Two authors (A.H. and H.Z.) initially screened the titles and abstracts of all retrieved records, and subsequently, reviewed the full texts independently. In instances of uncertainty regarding whether studies met the inclusion criteria, a third researcher (F.E.) was consulted, and decisions were made by consensus. We excluded articles not published in peer-reviewed journals, encompassing conference papers, theses, dissertations, books, book chapters, and reports from non-peer-reviewed sources, as well as those in languages other than English. Furthermore, we excluded studies that did not utilize a randomized controlled trial (RCT) or clinical controlled trial design. We included all studies published from the earliest date of consideration up to June 25, 2023, to ensure the relevance and timeliness of the evidence gathered. In cases where multiple reports originated from the same study, the most comprehensive report was selected. If the full text of an article was unavailable, the information provided in the abstract was utilized. However, if the abstract did not furnish sufficient information, the article was excluded from the study. Upon completion of the search, the EndNote program was employed to eliminate duplicates. Relevance checks were performed based on both the titles and abstracts, as well as the full texts. Additionally, the references of the included studies were reviewed to identify any potentially missing relevant papers.
Quality assessment
RCTs were included in the evaluation using the Cochrane Risk of Bias tool (version 1). This tool comprises several domains: selection, performance, detection, attrition, reporting, and other biases. The potential for bias in these assessments can be categorized as high, low, or unclear risk of bias. The quality of all included studies was independently assessed by two investigators, AH and HZ. In cases of disagreement, resolutions were sought through consultation with colleagues FA and DR.
Data extraction
The data were extracted into a sheet (Tables 1 and 2). The extracted data included the following items: summary characteristics such as author (s), year, sample size, study design, age, body weight, BMI, height, education, gestational age at study entry, session characteristics, and duration of labor. Overall labor duration is defined length of the first and second stages of labor. The first stage of labor is the time elapsed from the beginning of contractions to 10 cm of dilation; which includes the latent phase (the beginning of contractions up to 4 cm of dilation) and the active phase (the time elapsed from 4 to 10 cm. of dilation); the second stage is the time elapsed from full dilation (10 cm of dilation) until fetal expulsion [25].
Data analysis
Statistical analysis was conducted using Review Manager (RevMan) version 5.4 and STATA version 17. A significance level was set at a P value of less than 0.05. Overall effects were synthesized through the mean and standard deviation of labor length. Heterogeneity among studies was assessed using the I-squared test (I²). If the I² value exceeded 50%, outlier studies were first removed to homogenize the study sample. When heterogeneity persisted, random-effects models were utilized for the analysis instead of fixed-effect models. Publication bias was assessed using Egger’s test.
Equity, diversity, and inclusion statement
Our research team is dedicated to promoting diversity, equity, and inclusion in clinical practice, research, and training programs. Accordingly, the processes of data extraction, study selection, quality assessment, analysis, and interpretation were conducted independently to ensure results that accurately reflect the most diverse and realistic picture possible. We incorporated data from all primary research worldwide that met the inclusion criteria, without bias towards race, ethnicity, culture, socioeconomic status, or geographical regions.
Result
Study flow
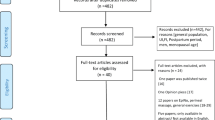
Figure 1 presents a chart detailing the flow of studies through this meta-analysis. In total, 330 records were screened, comprising 316 studies identified through database searches and 14 studies identified through other sources. After the removal of duplicates (24 studies), 290 studies did not meet the inclusion criteria and were subsequently excluded. The remaining 16 articles were retrieved in full for further examination. Of these, eleven studies met the inclusion criteria. The remaining five studies were excluded for the following reasons: two were cohort studies, one was a secondary publication, and two studies did not report the effect size.

PRISMA flow diagram of the screening procedure
The quality assessment (risk of bias)
The authors have meticulously noted and classified the biases associated with the research methodologies into three distinct categories: low risk, high risk, and unclear risk. High Risk: Aktan [14], Ferreira [26], Gehan [27], Perales [28], and Mazzarino [29] were categorized as high risk due to methodological limitations, potential biases, and data reliability issues.
Low Risk
Barakat [30], Bolanthakodi [31] and Haakstad [32] exhibited robust methodology, adequate sample sizes, and clear results, justifying their low-risk categorization.
Unclear risk
Ghandali [9], Rodriguez-Blanque [33] and Price [34] was categorized as uncertain due to ambiguities in its methodology and potential unaddressed confounding factors. This classification adheres to the criteria set forth by the Cochrane Collaboration tool. Detailed insights into this categorization, along with an exhaustive breakdown of the types and instances of bias present in the study methodologies, are comprehensively illustrated in Fig. 2.

Risk of bias graph for studies
Study characteristics
Relevant information from the 11 selected samples is concisely summarized in Table 2. The meta-analytic sample comprised a total of 1239 participants, with 602 in the intervention group and 637 in the control group. The mean age of the studied participants ranged from 23.4 years [31] to 36.8 years [35]. Three studies were conducted in Spain [28, 30, 33], while the remaining were carried out in Turkey [14], Australia [29], Norway [32], Iran [9], Brazil [26], the USA [34], India [31], and Egypt [35]. All study designs were Randomized Control Trials, except for two studies which were Clinical Control Trials [26, 35]. The number of exercise sessions in the studies varied from 7 [31] to 96 [34]. Some studies reported only weight [32], or body mass index (BMI) [9, 26, 28, 30, 34, 35], while others included all of metrics (weight, height, and BMI) [14, 29, 31, 33]. Three studies have presented only the duration of labor [14, 29, 33], while other studies have reported the duration of the active phase, the second stage, and/ or the duration of labor separately [9, 26, 28, 30,31,32, 34, 35] (Tables 1 and 2). No studies reported an increased risk of adverse birth outcomes from Pilates exercises among previously inactive, healthy women.
Quantitative data synthesis
The pooled effect size of Pilates exercises indicates a significant reduction in duration of the active phase (Mean Difference [MD] = -56.35, 95% Confidence Interval [CI] [-89.46 to -23.25], p < 0.001) with a sample size of 1195.
The mean difference in active phase of labour (− 56.35) means that Pilates reduces the duration of active phase of labor by 56.35 min in the intervention group compared to the control group. The analysed data were heterogeneous (I² = 60.96%), hence random-effects models were utilized for the analysis, but the heterogeneity could not be fully resolved (see Fig. 3A).

A; Forest plot of duration of the active phase of labor, B; Forest plot of duration of the second stage of labor, C; Forest plot of duration of labor (sum of active phase and second stage)
The Pilates exercises didn’t decrease the duration of the second stage of labor (MD = -0.11, 95% CI [-7.21 to 6.99], P value = 0.98), in a sample of 1135 pregnant women. The pooled estimate was homogeneous (I² = 71.75%, using a random-effect model) (refer to Fig. 3B).
Eight articles investigated the overall duration of labor (sample size = 898 pregnant women). The data indicated that the Pilates group experienced a shorter duration of labor compared to the control group (MD = -93.93, 95% CI [-138.34 to -49.51], P value = 0.001). The results showed heterogeneity (I² = 61.97%), and this heterogeneity could not be resolved (refer to Fig. 3C).
Assessment of publication bias
We did not observe publication bias for the study in any of the variables studied. The estimated bias coefficient of labor duration was − 0.29 (Egger bias B = − 0.30 (95% CI: − 2.66–2.08) with a standard error of 0.97, giving a p-value of 0.77. Thus, the test provides no evidence for the presence of small-study effect. Thus, the test provides no evidence for the presence of small-study effect. Figure 4 presents the funnel plot result with the 95% confidence limit. The estimated bias coefficient of active phase duration was − 0.85 (Egger bias B = − 0.88 (95% CI: − 3.19–1.50) with a standard error of 0.96, giving a p-value of 0.41 and it was 1.17 (Egger bias B = 0.50 (95% CI: − 4.82–7.16) with a standard error of 2.33 (p-value = 0.64) for second stage of labor.

Presentation of funnel plot
Discussion
The present study aimed to systematically review the literature regarding the efficacy of Pilates in reducing labor length. This meta-analysis was conducted using optimal methods for secondary analysis and included 11 primary studies, all of which were clinical trials. The analytical results indicate that Pilates exercises can significantly shorten the overall duration of labor, including both the active phase and the second stage.
The meta-analysis revealed a notable difference between the Pilates exercise group and control group in the duration of the first stage of labor, despite contradictory findings in the primary studies. The disparity in results from these primary studies could be attributed to variations in sample sizes (ranging from 60 to 325) and the timing of intervention initiation (between 12 and 39 weeks’ gestation). A detailed examination of the primary studies revealed that Pilates exercises were generally more effective in studies characterized by longer durations, higher frequency, and earlier commencement of the intervention [28]. Therefore, under these specific conditions, Pilates appears to strengthen pelvic muscles, increase pelvic diameter, relax muscles, and consequently enhance the condition of the birth canal parts. This, in turn, contributes to the shortening of the active phase of labor [ 29].
The findings of this study demonstrate that Pilates doesn’t affect the duration of the second stage of labor. This conclusion confirm with some earlier studies which indicated no significant difference in second stage’s length between women who practiced Pilates and those who did not [14]. It seems that the length of the second stage of labor, which is defined from the dilatation of the cervix to the expulsion of the fetus, is more influenced by the cephalo-pelvic proportion, birth weight, the strength of the mother’s perineal tissue, and station at complete dilatation [36] as well as differences in obstetric population characteristics and variation in clinical practice [37].
In this study, Pilates was observed to reduce the overall length of labor. Supporting this finding, the outcomes of several meta-analyses have underscored the positive impact of exercise programs on facilitating the childbirth process, particularly in shortening the duration of delivery [38]. However, there exists a divergence of opinion among researchers on this matter. For instance, the findings of two separate meta-analyses suggest no significant association between the regularity, intensity, and duration of exercise and the length of childbirth [39, 40]. This discrepancy may be attributable to the type of exercise. Veisy et al., for example, focused on the influence of aerobic exercise on labor duration [39]. Contrastingly, Pilates, a non-aerobic form of exercise, is primarily recognized for its capacity to enhance physical, mental, and motor functions [15].
This form of exercise encompasses a series of low-impact routines designed to enhance strength and flexibility across the body. Regular participation in these exercises has been demonstrated to fortify the pelvic floor muscles and improve their structural functionality [41]. The enhancement of central and pelvic floor muscle strength, flexibility, and the adoption of proper breathing techniques through Pilates are known to facilitate the birthing process [9, 42]. Additionally, Pilates, initially conceptualized as a body conditioning method termed ‘Contrology’, is founded on six key principles: breath, centering, concentration, control, precision, and flow [43]. Individual investigations into each of these elements have shown that they collectively contribute to a reduction in the duration of childbirth [44, 45].
Notably, the impact of Pilates exercise on labor duration has not been previously analyzed in a systematic review or meta-analysis with a sample size of this scale. The breadth of studies and the substantial number of participants involved in this analysis afford some of the most valid and reliable conclusions that can be drawn on this subject.
Clinical implications
Considering that prolonged labor presents a significant clinical challenge in contemporary midwifery practice, leading to various complications for both mother and child, one effective strategy to enhance labor comfort is the reduction of labor duration, specifically through methods that alleviate the duration of pain. The findings of this review indicate that practicing Pilates during pregnancy serves as a viable approach to decreasing labor length. Pilates, characterized as a discipline that bolsters physical, mental, and motor capacities, comprises a series of low-impact exercises aimed at strengthening and increasing flexibility throughout the body [15]. Analysis of primary studies reveals that Pilates can be reduced labor duration.
To date, there have been no reports of risks associated with moderate-intensity exercise for either the mother or the infant [46]. In light of this, low-risk pregnant women are encouraged to engage in progressive aerobic and resistance exercises before, during, and after childbirth. Nevertheless, it is advisable for pregnant women to undergo clinical evaluation before initiating any exercise program to ensure there are no medical contraindications to continuing with the exercise [47]. Engaging in Pilates exercises of moderate intensity during pregnancy has been shown to facilitate the delivery process.
Our findings endorse the capability of Pilates exercise to reduce the duration of labor in pregnant women. Therefore, Pilates could potentially be incorporated into childbirth preparation classes as a beneficial practice.
Limitations
This study encountered several limitations, both at the level of the individual studies and the review itself. A notable limitation within the primary studies was the lack of reported data on the intensity of the Pilates exercises. Additionally, variations in the initiation timing and duration of exercise sessions may have influenced the results of the analysis. Another limitation at the study level was the heterogeneity of the samples. For instance, while some studies had exercises performed under professional supervision, others involved participants practicing at home without such oversight. Moreover, the participant demographics varied across studies, with many focusing on primiparous women, while others included both multiparous and primiparous participants. This variability, particularly in terms of parity, was not accounted for as a potential confounding factor, potentially contributing to the high heterogeneity observed in the meta-analyses. Consequently, the results of this study should be interpreted with caution.
At the review level, the mean effect size of the active phase period and labour duration was analysed using a random-effects model due to the heterogeneity of the studies. Furthermore, this review was limited to scientific papers published in English, representing another constraint on its scope.
Conclusion
The evidence presented herein underscores that engaging in Pilates exercises during pregnancy is not only safe but also beneficial in optimizing the delivery process and shortening labor duration. Consistent with the guidelines of the American College of Obstetricians and Gynecologists (ACOG), this study reinforces the recommendation that, despite physiological and anatomical changes during pregnancy, women should be encouraged to maintain physical activity. Pilates, as demonstrated, can shorten length of labor. It is recommended that midwives emphasize the use of this exercise in childbirth preparation classes to reduce the duration of childbirth.
Data availability
Data is provided within the manuscript or supplementary information files.
References
Doolan-Roy ED, Reagan K, Modisette M, Mattes LL. Return to Sport following anterior Cruciate Ligament Reconstruction in the Professional Female Ballet Dancer. J Women’s Sports Med. 2022;2:83–94.
Levine B, Kaplanek B, Jaffe WL. Pilates training for Use in Rehabilitation after total hip and knee arthroplasty: a preliminary Report. Clin Orthop Relat Res. 2009;467:1468–75.
Cruz-Ferreira A, Fernandes J, Laranjo L, Bernardo LM, Silva A. A systematic review of the effects of pilates method of exercise in healthy people. Arch Phys Med Rehabil. 2011;92:2071–81.
Navas A, Artigues C, Leiva A, Portells E, Soler A, Cladera A, et al. Effectiveness and safety of moderate-intensity aerobic water exercise during pregnancy for reducing use of epidural analgesia during labor: protocol for a randomized clinical trial. BMC Pregnancy Childbirth. 2018;18:94.
King M, Green Y. Pilates workbook for pregnancy: Illustrated Step-by-step Matwork techniques. Berkerley, Canada: Ulysses; 2002.
Mazzarino M, Kerr D, Wajswelner H, Morris ME. Pilates Method for Women’s Health: systematic review of Randomized controlled trials. Arch Phys Med Rehabil. 2015;96:2231–42.
Cuijlits I, van de Wetering A p., Endendijk Jj, van Baar A l., Potharst E. s., Pop V j. m. Risk and protective factors for pre- and postnatal bonding. Infant Mental Health Journal. 2019;40:768–85.
Hyun A-H, Cho J-Y, Koo J-H. Effect of home-based Tele-Pilates intervention on pregnant women: a pilot study. Healthcare. 2022;10:125.
Ghandali NY, Iravani M, Habibi A, Cheraghian B. The effectiveness of a pilates exercise program during pregnancy on childbirth outcomes: a randomised controlled clinical trial. BMC Pregnancy Childbirth. 2021;21:480.
Aladro-Gonzalvo AR, Machado-Díaz M, Moncada-Jiménez J, Hernández-Elizondo J, Araya-Vargas G. The effect of Pilates exercises on body composition: a systematic review. J Bodyw Mov Ther. 2012;16:109–14.
Feria-Ramírez C, Gonzalez-Sanz JD, Molina-Luque R, Molina-Recio G. The effects of the Pilates Method on pelvic floor injuries during pregnancy and childbirth: a quasi-experimental study. Int J Environ Res Public Health. 2021;18:6995.
Sukmawati S, Mamuroh L, Nurhakim F. Efektivitas Pilates Exercise untuk Mengurangi Nyeri pada Ibu Hamil. Malahayati Nurs J. 2023;5:2351–69.
Yaman S, Tulmaç ÖB, Canarslan B, Hançerli̇oğullari N. Effect of pilates during pregnancy on delivery outcomes. J Health Sci Med / JHSM. 2020;3:442–7.
Aktan B, Kayıkçıoğlu F, Akbayrak T. The comparison of the effects of clinical Pilates exercises with and without childbirth training on pregnancy and birth results. Int J Clin Pract. 2021;75:e14516.
Mazzarino M, Kerr D, Morris ME. Pilates program design and health benefits for pregnant women: A practitioners’ survey. J Bodyw Mov Ther. 2018;22:411–7.
Ghiasi A, Hasani M, Mollaahmadi L, Hashemzadeh M, Haseli A. The effect of aromatherapy on labor Pain relief: a systematic review of clinical trials. Iran J Obstet Gynecol Infertility. 2017;20:89–105.
Ijaiya MA, Adesina KT, Raji HO, Aboyeji AP, Olatinwo AO, Adeniran AS et al. Duration of labour with spontaneous onset at the University of Ilorin Teaching Hospital, Ilorin, Nigeria. Ann Afr Med. 2011;10.
Ijaiya MA, Aboyeji AP, Fakeye OO, Balogun OR, Nwachukwu DC, Abiodun MO. Pattern of cervical dilatation among parturients in Ilorin, Nigeria. Ann Afr Med. 2009;8.
MELAH G, EL-NAFATY A, MASSA A. Obstructed labour: a public health problem in Gombe, Gombe State, Nigeria. J Obstet Gynaecol. 2003;23:369–73.
Piper JM, Bolling DR, Newton ER. The second stage of labor: factors influencing duration. Am J Obstet Gynecol. 1991;165:976–9.
Cheng YW, Hopkins LM, Laros RK, Caughey AB. Duration of the second stage of labor in multiparous women: maternal and neonatal outcomes. American Journal of Obstetrics and Gynecology. 2007;196:585.e1-585.e6.
Dias NT, Ferreira LR, Fernandes MG, Resende APM, Pereira-Baldon VS. A pilates exercise program with pelvic floor muscle contraction: is it effective for pregnant women? A randomized controlled trial. Neurourol Urodyn. 2018;37:379–84.
Bulguroğlu Hİ, Bulguroğlu M, Özkul Ç, Gündüz AG. Investigation of the Effect of Pilates exercises on Postural Stability and fear of birth in pregnancy. Adnan Menderes Üniversitesi Sağlık Bilimleri Fakültesi Dergisi. 2023;7:530–40.
Page MJ, Moher D. Evaluations of the uptake and impact of the Preferred reporting items for systematic reviews and Meta-analyses (PRISMA) Statement and extensions: a scoping review. Syst Reviews. 2017;6:263.
Zhang J, Troendle J, Mikolajczyk R, Sundaram R, Beaver J, Fraser W. The natural history of the Normal First Stage of Labor. Obstet Gynecol. 2010;115:705.
Ferreira CLM, Guerra CML, Silva AITJ, Rosário HRV. do, Pereira MBFL de O. Exercise in Pregnancy: The Impact of an Intervention Program in the Duration of Labor and Mode of Delivery. Rev Bras Ginecol Obstet. 2019;41:68–75.
Gehan A, Khadiga S, Amir G, Eman A. Efficacy of antenatal exercises on maternal and neonatal outcomes in elderly primigravida. 2015;3:109–14.
Perales M, Calabria I, Lopez C, Franco E, Coteron J, Barakat R. Regular Exercise throughout pregnancy is Associated with a shorter first stage of labor. Am J Health Promot. 2016;30:149–57.
Mazzarino M, Kerr D, Morris ME. Feasibility of pilates for pregnant women: a randomised trial. J Bodyw Mov Ther. 2022;32:207–12.
Barakat R, Franco E, Perales M, López C, Mottola MF. Exercise during pregnancy is associated with a shorter duration of labor. A randomized clinical trial. Eur J Obstet Gynecol Reproductive Biology. 2018;224:33–40.
Bolanthakodi C, Raghunandan C, Saili A, Mondal S, Saxena P. Prenatal yoga: effects on Alleviation of Labor Pain and Birth outcomes. J Altern Complement Med. 2018;24:1181–8.
Haakstad LAH, Bø K. The marathon of labour—does regular exercise training influence course of labour and mode of delivery? Secondary analysis from a randomized controlled trial. Eur J Obstet Gynecol Reproductive Biology. 2020;251:8–13.
Rodríguez-Blanque R, Sánchez-García JC, Sánchez-López AM, Aguilar-Cordero MJ. Physical activity during pregnancy and its influence on delivery time: a randomized clinical trial. PeerJ. 2019;7:e6370.
Price BB, Amini SB, Kappeler K. Exercise in pregnancy: effect on fitness and obstetric outcomes-a randomized trial. Med Sci Sports Exerc. 2012;44:2263–9.
Gehan. Efficacy of antenatal exercises on maternal and neonatal outcomes in elderly primigravida. Kasr Al Ainy Med J. 2012;21:109.
Altman MR, Lydon-Rochelle MT. Prolonged second stage of labor and risk of adverse maternal and perinatal outcomes: a systematic review. Birth. 2006;33:315–22.
Cheng YW, Caughey AB. Second stage of labor. Clin Obstet Gynecol. 2015;58:227.
Cancela-Carral JM, Blanco B, López-Rodríguez A. Therapeutic aquatic Exercise in pregnancy: a systematic review and Meta-analysis. J Clin Med. 2022;11:501.
Veisy A, Mohammad Alizadeh Charandabi S, Hematzadeh S, Mirghafourvand M. Effect of prenatal aerobic exercises on maternal and neonatal outcomes: a systematic review and meta-analysis. Nurs Open. 2021;8:2301–17.
Davenport MH, Meah VL, Ruchat S-M, Davies GA, Skow RJ, Barrowman N, et al. Impact of prenatal exercise on neonatal and childhood outcomes: a systematic review and meta-analysis. Br J Sports Med. 2018;52:1386–96.
Torelli L, de Bella J, Rodrigues ZIK, Stüpp CA, Girão L, Sartori MJBC. Effectiveness of adding voluntary pelvic floor muscle contraction to a pilates exercise program: an assessor-masked randomized controlled trial. Int Urogynecol J. 2016;27:1743–52.
Artal R, O’Toole M. Guidelines of the American College of obstetricians and gynecologists for exercise during pregnancy and the postpartum period. Br J Sports Med. 2003;37:6–12.
Pilates JH, Miller WJ. Return to Life through Contrology. Ravenio Books; 1945.
Haseli A, Ghiasi A, Hashemzadeh M. Do breathing techniques enhance the Effect of Massage Therapy in reducing the length of Labor or not? A Randomized Clinical Trial. J Caring Sci. 2019;8:257–63.
Haseli A, Akbari M, Neisani Samani L, Haghani H, Jahdi F. The effect of abdominal massage along with breathing techniques during labor on duration of uterine contractions in primiparous women. Iran J Obstet Gynecol Infertility. 2017;20:1–8.
Davies G, La W, Mf M, C M, My A. Exercise in pregnancy and the postpartum period. J Obstet Gynaecol Can. 2003;25:516–29.
American College of Obstetricians and Gynecologists. Exercise during pregnancy and the postpartum period. Clin Obstet Gynecol. 2003;46:496–9.
Acknowledgements
We acknowledge all authors who contributed to the primary studies. This study is the result of research project No. 4020044, approved by the Student Research Committee at Kermanshah University of Medical Sciences, Kermanshah, Iran. Our gratitude extends to the officials of the Clinical Research Development Center at Motazedi Hospital, Kermanshah University of Medical Sciences, the Department of Midwifery at Kashan University of Medical Sciences, and the School of Health and Welfare at Dalarna University, Sweden, for their invaluable support and contributions.
Funding
The present study was supported by the Student Research Committee, Kermanshah University of Medical Sciences. Kermanshah, Iran (Grant number: 4020044).
Open access funding provided by Dalarna University.
Author information
Authors and Affiliations
Contributions
AH and HZ designed the search strategy and selection criteria. They screened the eligibility of the articles, reviewed them independently, assessed the quality of the articles, and constructed the tables and figures. FE and DR, as the third and fifth co-authors, checked for contradictions and drafted the results and discussion sections. ZK conducted new and updated statistical analyses during the revisions to the journal. AH wrote the first draft of the manuscript, while DR edited and proofread the entire manuscript. Finally, FE also proofread the manuscript and provided comments. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was a research project approved by the Ethics Committee of the Research Deputy at Kermanshah University of Medical Sciences in Kermanshah (approval code: IR. KUMS. REC.1401.583).
Consent for publication
N/A.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Haseli, A., Eghdampour, F., Zarei, H. et al. Optimizing labor duration with pilates: evidence from a systematic review and meta-analysis of randomized controlled trials. BMC Pregnancy Childbirth 24, 573 (2024). https://doi.org/10.1186/s12884-024-06785-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12884-024-06785-5