
Abstract
Background
Contemporary estimates of diabetes mellitus (DM) rates in pregnancy are lacking in Canada. Accordingly, this study examined trends in the rates of type 1 (T1DM), type 2 (T2DM) and gestational (GDM) DM in Canada over a 15-year period, and selected adverse pregnancy outcomes.
Methods
This study used repeated cross-sectional data from the Canadian Institute of Health Information (CIHI) hospitalization discharge abstract database (DAD). Maternal delivery records were linked to their respective birth records from 2006 to 2019. The prevalence of T1DM, T2DM and GDM were calculated, including relative changes over time, assessed by a Cochrane-Armitage test. Also assessed were differences between provinces and territories in the prevalence of DM.
Results
Over the 15-year study period, comprising 4,320,778 hospital deliveries in Canada, there was a statistically significant increase in the prevalence of GDM and T1DM and T2DM. Compared to pregnancies without DM, all pregnancies with any form of DM had higher rates of hypertension and Caesarian delivery, and also adverse infant outcomes, including major congenital anomalies, preterm birth and large-for-gestational age birthweight.
Conclusion
Among 4.3 million pregnancies in Canada, there has been a rise in the prevalence of DM. T2DM and GDM are expected to increase further as more overweight women conceive in Canada.
Similar content being viewed by others
Background
Diabetes mellitus (DM) during pregnancy is an important health indicator, as it is associated with an increased risk of adverse outcomes for both the birthing parent and their infant(s). Pre-existing type 1 (T1DM) and type 2 (T2DM) DM in pregnancy are known to be associated with an increased risk of adverse perinatal outcomes, such as perinatal mortality, preterm birth, and congenital anomalies [1, 2]. Gestational DM (GDM) is known to increase the risk of macrosomia, intrauterine fetal death, preterm birth, congenital anomalies, and respiratory distress syndrome [3, 4]. Furthermore, a person who develops GDM has an increased risk of developing T2DM or impaired glucose tolerance in the years following pregnancy [5].
Recent estimates show that the prevalence of T2DM and GDM is increasing globally [6, 7]. A rise in T1DM is being documented internationally in younger populations [8,9,10]. Although there are national reports on DM during pregnancy [11, 12], few distinguish between pre-existing DM and GDM. This paper explored the temporal trends of pregnancies with T1DM, T2DM and GDM in Canada using hospital record data over a 15-year period.
Methods
Study design and setting
This retrospective repeated cross-sectional study was conducted using hospitalization data from the Canadian Institute of Health Information (CIHI) acute-care discharge abstract database (DAD) over a 15-year period, from 2005 to 2019. The DAD captures administrative, clinical and demographic information on hospital discharges in Canada [13]. The DAD has been shown to have high sensitivity and specificity on many maternal and infant health variables [14]. Almost all persons in Canada give birth in hospitals (98%); [15] therefore, the CIHI-DAD captures most deliveries in Canada and is the largest Canadian data source for diagnoses of maternal health conditions, such as T1DM and T2DM and/or GDM. Data are received directly from acute care facilities or their respective health/regional authority or ministry/department of health. Facilities in all provinces and territories except Quebec are required to report to CIHI [16].
Participants
Any woman aged 15–54 years who delivered a liveborn or stillborn baby in a Canadian hospital (except in the province of Quebec) between the 2005/2006 to 2019/2020 fiscal years was eligible for inclusion in the study. The DAD was used to identify in maternal records of those who were admitted to hospital to deliver a baby using International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Canadian (ICD-10-CA) codes. Records with an ICD-10-CA code of O10-O16, O21-O29, O30-O37, O40-O46, O48, O60-O75, O85-O92, O95 or O98-O99 with a ‘1’ or ‘2’ coded at the 6th digit, or Z37 coded in any position were used to identify delivery records. Abortive procedures were excluded. The standard maternal population includes persons aged 10–54; however, we excluded persons aged 10–14 years due to small cell counts of 1223 deliveries. The final study sample consisted of 4,320,778 hospital deliveries.
Outcomes
Diabetes during pregnancy was defined using ICD-10-CA codes as follows. For fiscal years 2005/06 and 2006/07 records with ‘O240’ or ‘E10’ were coded as pre-existing T1DM; records with ‘O241’ or ‘E11’ were coded as pre-existing T2DM; and records with ’O244’ were coded as GDM. Due to changes in coding practices, from 2007/08 onwards, records with ‘O245’ or ‘E10’ were coded as T1DM; records with ‘O246’ or ‘E11’ were coded as T2DM; and records with ‘O248’ were coded as GDM. Unspecified DM or DM due to malnutrition were excluded. Supplemental Table 1 has the complete list of ICD-10-CA codes.
Maternal characteristics include age at delivery (grouped by 5-year intervals), pregnancy type (singleton or multiple), rural or urban residence—determined by first three digits of postal code, hypertension during pregnancy, gestational age at birth (< 32 weeks, 32–36 weeks, 37–42 weeks), type of preterm birth (spontaneous or provider-initiated), type of delivery (vaginal, c-section, induction), parity (first time mother or previous delivery) and outcome of delivery (stillbirth or livebirth). Maternal records were linked to birth records to assess if a major congenital anomaly was present as defined by the Canadian Congenital Anomalies Surveillance System [17], if the infant had any birth trauma (using ICD-10-CA codes P10-P15), and to determine birth weight percentiles, expressed as small- (SGA) or large- (LGA) for gestational age birthweight based on Kramer et al.’s methodology [18]. The proportion of missing data was 21% for parity between 2005 and 2015, after which it was < 0.1%, 0.4% for rural/urban residence and 0.6% SGA/LGA (due to missing birthweight). The data were complete for all clinical interventions (type of delivery, preterm birth status), diagnoses and birth outcomes. The study population distribution or the prevalence rates were the same with or without missing data.
Statistical analysis
We calculated the prevalence of DM during pregnancy using deliveries in hospital as the denominator, and any person with a diagnosis of T1DM, T2DM or GDM found on the delivery record as the respective numerators and expressed as a proportion per 1000 deliveries. We calculated temporal trend tests using the Cochrane-Armitage test. We also calculated relative percent changes between 2019 and 2005. Maternal DM rates were also stratified by fiscal year (April 1-March 31).
We described the adverse pregnancy outcomes stratified by DM type and those without DM. Chi-squared tests and p < 0.05 were used to determine if the differences were statistically significant.
We stratified gestational DM by parity to show differences in rates among women who have had a previous pregnancy versus nulliparous mothers. To compensate for the missing parity data between 2005 and 2014, we imputed the missing values using a linear regression approach. We compared the distribution of gestational DM to those with and missing parity information, and as the distribution was similar, it was determined that the data was missing at random [19]. We included maternal age, province of residence, gestational diabetes, mode of delivery and pregnancy type as covariates that may influence the missing values as part of the regression model to minimize bias [19]. The distribution of data were similar in both the imputed and original data. We included the imputed data to populate Tables 1 and 2. All other analysis were done on the original dataset as the slope of change in gestational diabetes remained consistent over time, with or without parity information.
To examine geographic differences, we calculated the prevalence of DM during pregnancy by DM type and province, in five-year intervals. Stratified by DM type, we also calculated prevalence using Ontario as the reference as it contains the largest proportion of deliveries in Canada. In 2011, British Columbia (BC) universally adopted the ‘alternative’ 1 step approach to screen for GDM, which has lower diagnostic thresholds than the ‘preferred’ two-step approach. The preferred approach uses a standardized non-fasting 50-g glucose challenge screening test (GCT) with plasma glucose (PG) measured 1 h later. If the value of the GCT is 7.8–11.0, a 2-hour 75-g oral glucose tolerance test with fasting is performed. GDM is diagnosed if any of the criteria are met: FPG ≥ 5.3 mmol/L, 1-h PG ≥ 10.6 mmol/L or 2-h PG ≥ 9.0 mmol/L. The alternative 1-step approach uses a standardized 2-hour 75-g oral glucose tolerance test with fasting plasma glucose, 1-hour plasma glucose (PG), and 2-hour PG. GDM is diagnosed if any of the criteria are met: FPG ≥ 5.1 mmol/L, 1-h PG ≥ 10.0 mmol/L or 2-h PG ≥ 8.5 mmol/L. This change in practice resulted in a higher number of GDM cases. As BC’s data likely amplifies the national rates due to their testing practices, national estimates are presented with and without BC.
Any estimate with a count < 5 in the numerator was excluded for privacy reasons. Data were analysed using SAS EG version 7.1 and graphs were produced using Microsoft Excel v2016.
Ethics approval was not required as this study was based on anonymized data and conducted under the surveillance mandate of the Public Health Agency of Canada.
Results
The study included 4,320,778 hospital deliveries in Canada over the 15-year study period. Across this period there was a statistically significant increase in T1DM and T2DM (Fig. 1a) as well as GDM (Fig. 1b). The relative increase in T2DM was 189% (2.7 per 1000 deliveries to 7.8 per 1000 deliveries), 25% (2.4 per 1000 deliveries to 3.0 per 1000 deliveries) for T1DM, 162.7% for GDM (36.5 per 1000 deliveries to 95.9 per 1000 deliveries without BC), and 153% (41.2 per 1000 deliveries to 104.3 per 1000 deliveries, including BC).

(a) Annual temporal trends in type 1 and type 2 diabetes mellitus (DM) among hospital deliveries in Canada, 2005–2019. Excluded is the province of Quebec. (b) Annual temporal trends in gestational diabetes mellitus (GDM) among hospital deliveries in Canada, 2005–2019. Excluded is the province of Quebec. Furthermore, the lower dashed line does not include data from the province of British Columbia
The prevalence of adverse pregnancy outcomes varied by DM status. Persons with T1DM and T2DM had a higher prevalence of adverse infant outcomes including major congenital anomalies, preterm birth, LGA and stillbirth compared to those without DM. Persons with GDM had a higher prevalence of preterm birth, caesarean section, induction or LGA compared to those without DM. Persons with GDM also had slightly higher rates of congenital anomalies and birth trauma, but lower rates of stillbirth than those without DM. All persons who had any DM had a higher prevalence of hypertension than those without DM. See Table 1.
The largest increases in both GDM and T1DM and T2DM were found among the youngest population, aged 15–19 years old. For this age group, between 2005 and 2019, there was a relative increase of 260% for GDM (including BC), a relative increase of 291% (without BC) a relative increase of 330% for T2DM, and a relative increase of 92.9% for T1DM (see Table 3).
Mothers who have had a previous pregnancy had an overall higher prevalence of gestational DM compared to first time mothers, however the relative increase in GDM was highest among nulliparous mothers (180%) compared to parous mothers (136%) (see Table 2).
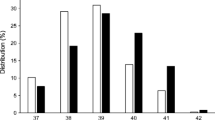
The geographical distribution of DM varied across Canada (Table 4). The highest proportion of GDM cases were found in Western Canada, with British Columbia having the highest rate of 104.3 per 1000 deliveries followed by Alberta with 64.2 per 1000 deliveries. The fewest cases were reported in Nunavut, with a rate of 30.7 per 1000 deliveries. T2DM showed a very different distribution pattern, with the highest reported cases in Manitoba (11.8 per 1000 deliveries), followed by Saskatchewan (6.6 per 1000 deliveries) and the lowest prevalence was seen in Nunavut (1.3 per 1000 deliveries). T1DM was highest in Atlantic Canada, with Newfoundland and Labrador having the highest rate of 4.9 per 1000 deliveries, followed by Prince Edward Island at 4.4 per 1000 deliveries and the lowest prevalence was found in the Territories (2.0 per 1000 deliveries). T1DM and T2DM and GDM increased across all jurisdictions, except Nunavut, where this was only true for GDM. See Figs. 2, 3 and 4.

Prevalence of type 1 diabetes mellitus (DM) by five-year Intervals, by Canadian province, 2005–2019
Excluded is the province of Quebec. Furthermore, as the Yukon Territory and Nunavut each had cell counts < 5, they are not included in this figure
Abbreviations: AB-Alberta, BC- British Columbia, MB-Manitoba, NB-New Brunswick, NL-Newfoundland and Labrador, NS-Nova Scotia, NT-Northwest Territories, ON- Ontario, PE- Prince Edward Island, SK-Saskatchewan

Prevalence of type 2 diabetes mellitus (DM) by five-year Intervals, by Canadian province or territory, 2005–2019
Excluded is the province of Quebec
Yukon Territories and Nunavut had cell counts < 5 and thus, are omitted
Abbreviations: AB-Alberta, BC- British Columbia, MB-Manitoba, NB-New Brunswick, NL-Newfoundland and Labrador, NS-Nova Scotia, NT-Northwest Territories, ON- Ontario, PE- Prince Edward Island, SK-Saskatchewan

Prevalence of gestational diabetes mellitus (GDM) by five-year Intervals, by Canadian province or territory, 2005–2019
Excluded is the province of Quebec
Abbreviations: AB-Alberta, BC- British Columbia, MB-Manitoba, NB-New Brunswick, NL-Newfoundland and Labrador, NS-Nova Scotia, NT-Northwest Territories, NU-Nunavut, ON- Ontario, PE- Prince Edward Island, SK-Saskatchewan, YT-Yukon Territories
Discussion
Over a 15-year period, there has been an increase in T1DM, T2DM and GDM. This is consistent with recent international data [20,21,22]. There was a positive relation between DM and maternal age for both T2DM and GDM, with a higher prevalence seen with each increase in age groups. Despite having the lowest rates of DM overall, the largest increases over the fifteen-year study period were found among persons aged 15–19, for GDM, T2DM and T1DM.
Estimates of the population-level prevalence of T1DM in pregnancies are limited, as most literature reports by combining ‘pre-existing’ DM types or involving smaller clinical study samples. Where data are available, our estimates show comparable results (0.3% had T1DM in our study). Four large studies in Scotland (15-year study period), the UK (16 years), the US (18 years) and Sweden (15 years) found that approximately 0.4%, 0.4%, 0.2% and 0.5% of pregnancies had T1DM at the end of the study period, respectively [20, 22,23,24]. In all studies, an increase in rates was seen over time which is consistent with our study findings. A US study among a cohort of youth less than 18 years of age (non-pregnant population) is projecting a tripling of T1DM and T2DM rates by 2050 [8]. A study in the Pima Indian population over a 30-year period found that increasing weight and increasing frequency of exposure to DM in utero accounted for most of the increase in the DM prevalence in Pima Indian children [25]. The increase in the prevalence of DM in our study is worrying as this increase may have an impact on DM risk among exposed offspring [26].
Established risk factors for developing T2DM or GDM are similar and include pre-pregnancy obesity, advanced maternal age, a positive family history of DM, and non-white ethnicity [2, 5]. Further, women who had GDM in one pregnancy may be at higher risk for GDM in a subsequent pregnancy [27, 28]. As our findings come from administrative data, it was not possible to examine most known individual-level risk factors, thus we cannot establish which risk factor(s) may most explain the increasing trend. We were able to observe a higher prevalence of gestational DM among parous women, though this does not appear to drive the increase over time, as the rate of change over time is consistent with nulliparous mothers. In large part, the increasing trend of an obesity among Canadian adults [29] may explain the increased rates of DM seen in this study. Additionally, increased trends may be due to possible generational epigenetic effects of obesity through maternal in-utero exposure to hyperglycemia [25]. As rates of GDM continue to increase, continued surveillance is important as persons who have GDM have a 35–60% chance of developing T2DM following their pregnancy, have higher risk for GDM in subsequent a pregnancy, and higher risk of adverse infants outcomes [3, 5, 6, 30].
Both Diabetes Canada [5] and the Society of Obstetricians and Gynaecologists of Canada (SOGC) [31] intermittently publish clinical guidelines for GDM screening. The recommendations for GDM screening have varied between iterations of those guidelines, especially following the publication of the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study [32]However, lack of a consensus on which is the optimal screening method continues, resulting in differing estimates of GDM prevalence in Canada. For example, historically British Columbia has had a higher prevalence of GDM than all provinces and territories [33]. In 2011, the province of British Columbia universally adhered to the alternate one-step screening approach for GDM [34], which further increased the prevalence of GDM in that province. Due to the potentially exaggerated increase of cases in British Columbia, national estimates were presented herein that included and excluded data from that province.
Diabetes status was ascertained using ICD-10-CA codes identified in the maternal delivery record. The use of ICD-10-CA coding appears to be a reliable and valid way to identify both T1DM and T2DM, and also GDM. A study comparing ICD-10 coding to medical records for persons who were delivered in hospital between 2016 and 2018 found that for GDM, ICD-10 codes had a high negative predictive value > 99% and a high specificity > 99% [35]. For pre-existing DM, the sensitivity was 85.9% (95% CI 78.8 to 93.0) and the positive predictive value was 91% (95% CI 85 to 97) [35]. Similarly, a validation study conducted in Alberta found that ICD-10 codes for GDM in administrative databases can be used to reliably estimate the burden of the disease at the population level and that delivery record codes are likely more accurate as these codes are included at the end of the hospital stay and have likely been verified [36]. While the diagnostic thresholds for assessing GDM have remained consistent in Canada during the study period [8, 37], there is variation in diagnostic procedures to test for GDM in Canada. As such there is a possibility that jurisdictions or institutions using a one-step approach will show a higher prevalence of GDM than those who opt for the two-step approach. While the ICD-10-CA coding is likely accurate, jurisdictional variations can exist due to testing practices rather than true differences in prevalence.
We noted some striking jurisdictional differences in our data for T1DM and T2DM. The highest prevalence of T1DM was found in Atlantic Canada, with the highest rates seen in Newfoundland and Labrador (1.75 times the Canadian rate). While there is considerable research suggesting that genetics are an established risk factor for the onset of T1, links to obesity, infection and environmental factors are still being explored [38]. Manitoba had over twice the prevalence of T2DM compared to the Canadian rate. It is unknown what may be driving the regional differences, and further research is needed.
There were limitations to this study. Our analyses do not contain Quebec data or data from individuals who choose to deliver at home. Small cell counts in the Northern Territories did not allow us to assess changes in rates over three time periods. No individual-level information such as weight, BMI, ethnicity, smoking status, family history, education or other socio-demographic information is available for analysis. These factors would be important to establish a profile of risk factors to help understand the key drivers among the population or to explore what may be contributing to regional differences.
Our study also has considerable strengths, which include a large population-based dataset, which contains almost all hospital deliveries in Canada excluding Quebec, and includes clinical indicators on the delivery, the health status of the person giving birth and infant outcomes. The data used in this study are of high quality and undergo strict data quality assurance processes. Furthermore, previous studies have shown that using ICD-10-CA codes to identify both T1DM and T2DM and GDM are valid, reliable, and accurate way to measure DM during pregnancy. As such, we expect that our findings represent a true approximation of prevalence in Canada.
Conclusion
These Canadian data showed a steady increase in T1DM, T2DM and GDM among pregnancies in Canada. Continued national surveillance of DM during pregnancy is needed to better inform and guide prevention efforts, as the rates of T1DM and T2DM and GDM are expected to continue to rise due to the increased trend of an older, and more obese maternal population in Canada. Additionally, the increase in DM during pregnancy amongst the younger population warrants particular attention.
Data availability
The data that support the findings of this study were made available from the Canadian Institute for Health Information to fulfil the surveillance mandate of the Public Health Agency of Canada. The datasets analysed during the current study are not publicly available as they were provided by a third party through a data sharing agreement. Applications for accessing the data can be made by completing a request form through the Canadian Institute for Health Information’s website https://www.cihi.ca/en/data-inquiry-form Procedures to obtain data can be made available after making a reasonable request to the corresponding author.
Abbreviations
- DM:
-
Diabetes mellitus
- T1DM:
-
Type 1 diabetes mellitus
- T2DM:
-
Type 2 diabetes mellitus
- GDM:
-
Gestational diabetes mellitus
- CPSS:
-
Canadian Perinatal Surveillance System
- CIHI:
-
Canadian Institute for Health Information
- DAD:
-
Discharge Abstract Database
- LGA:
-
Large for gestational age birthweight
- SGA:
-
Small for gestational age birthweight
- CI:
-
Confidence interval
- SOGC:
-
Society of Obstetricians and Gynaecologists of Canada
References
Wahabi HA, Esmaeil SA, Fayed A, Al-Shaikh G, Alzeidan RA. Pre-existing diabetes mellitus and adverse pregnancy outcomes. 2012;5:496. https://doi.org/10.1186/1756-0500-5-496
Canada. PHA of. Perinatal Health Report. Ottawa, ON: Government of Canada; 2013.
Imperatore G, Boyle JP, Thompson TJ, Case D, Dabelea D, Hamman RF, et al. Projections of type 1 and type 2 diabetes burden in the U.S. population aged < 20 years through 2050: dynamic modeling of incidence, mortality, and population growth. United States. 2012;35:2515–20.
Martin B, Sacks DA. The global burden of hyperglycemia in pregnancy – Trends from studies in the last decade. 2018;145:17–9. https://www.sciencedirect.com/science/article/pii/S016882271830490X
Information CI. for H. Data Quality Documentation, Discharge Abstract database. [cited 2023 Feb 21]; https://www.cihi.ca/sites/default/files/document/dad-data-quality-current-year-information-2020-2021-en.pdf
Health Mof. Diabetes Care - Province of British Columbia [Internet]. Province of British Columbia; [cited 2023 Feb 27]. https://www2.gov.bc.ca/gov/content/health/practitioner-professional-resources/bc-guidelines/diabetes
Stanhope KK, Joseph NT, Platner M, Hutchison C, Wen S, Laboe A, et al. Validation of ICD-10 codes for gestational and pregestational diabetes during pregnancy in a large, Public Hospital. Volume 32. United States: Wolters Kluwer Health, Inc; 2021. pp. 277–81.
Getahun D, Fassett MJ, Jacobsen SJ. Gestational diabetes: risk of recurrence in subsequent pregnancies. 2010;203:467.e1-467.e6. https://www.sciencedirect.com/science/article/pii/S0002937810006757
Canada S. Tables 13-10-0429-01 Live Births and fetal deaths (stillbirths) by place of birth (hospital or non-hospital) [Internet]. 2023. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310042801
Mobasseri M, Shirmohammadi M, Amiri T, Vahed N, Hosseini Fard H, Ghojazadeh M. Prevalence and incidence of type 1 diabetes in the world: a systematic review and meta-analysis. Maad Rayan Publishing Company; 2020. p. 98.
Kramer MS, Platt RW, Wen SW, Joseph KS, Allen A, Abrahamowicz M et al. A new and improved population-based Canadian reference for birth weight for gestational age. 2001;108:E35.
Zhuang W, Lv J, Liang Q, Chen W, Zhang S, Sun X. Adverse effects of gestational diabetes-related risk factors on pregnancy outcomes and intervention measures. Athens: Spandidos Publications; 2020;20:3361–7. https://search.proquest.com/docview/2442166962
Berger H, Gagnon R, Sermer M, Guideline. No 393-Diabetes Pregnancy. 2019;41:1814–25. e1.
Peng TY, Ehrlich SF, Crites Y, Kitzmiller JL, Kuzniewicz MW, Hedderson MM et al. Trends and racial and ethnic disparities in the prevalence of pregestational type 1 and type 2 diabetes in Northern California: 1996–2014. 2017;216:177.e1-177.e8. https://www.sciencedirect.com/science/article/pii/S0002937816308705
Negrato CA, Mattar R, Gomes MB. Adverse pregnancy outcomes in women with diabetes. 2012;4:41. https://doi.org/10.1186/1758-5996-4-41
Diabetes. in Canada [Internet]. [cited 2023 Sep 9]. https://www.diabetes.ca/advocacy---policies/advocacy-reports/national-and-provincial-backgrounders/diabetes-in-canada
Shojaeian A. An overview of the Epidemiology of Type 1 Diabetes Mellitus. 2018.
Dabelea D, Mayer-Davis EJ, Saydah S, Imperatore G, Linder B, Divers J et al. Prevalence of Type 1 and Type 2 Diabetes Among Children and Adolescents From 2001 to 2009. 2014 [cited 2023];311:1778–86. https://doi.org/10.1001/jama.2014.3201
Bancej C, Jayabalasingham B, Wall RW, Rao DP, Do MT, de Groh M, et al. Evidence brief–trends and projections of obesity among canadians. Canada. 2015;35:109–12.
Yeung RO, Savu A, Kinniburgh B, Lee L, Dzakpasu S, Nelson C et al. Prevalence of gestational diabetes among Chinese and South Asians: A Canadian population-based analysis. 2017;31:529–36. https://www.sciencedirect.com/science/article/pii/S1056872716307292
The Hyperglycemia and Adverse Pregnancy Outcome (HAPO). Study - ScienceDirect. [cited 2023 Feb 21]; https://www.sciencedirect.com/science/article/pii/S0020729202000929
Canada PHA. of. Diabetes in Canada [Internet]. 2017 [cited 2023 Aug 10]. https://www.canada.ca/en/public-health/services/publications/diseases-conditions/diabetes-canada-highlights-chronic-disease-surveillance-system.html
Craig ME, Kim KW, Isaacs SR, Penno MA, Hamilton-Williams EE, Couper JJ, et al. Early-life factors contributing to type 1 diabetes. Springer. 2019;62:1823–34.
Coton SJ, Nazareth I, Petersen I. A cohort study of trends in the prevalence of pregestational diabetes in pregnancy recorded in UK general practice between 1995 and 2012. England. 2016;6:e009494–2015.
Berger H, Crane J, Farine D, Armson A, De La Ronde S, Keenan-Lindsay L et al. Screening for gestational diabetes mellitus. 2002;24:894–912.
Russell C, Dodds L, Armson BA, Kephart G, Joseph KS. Diabetes mellitus following gestational diabetes: role of subsequent pregnancy. John Wiley & Sons, Ltd; 2008;115:253–60. https://doi.org/10.1111/j.1471-0528.2007.01459.x
Cho NH, Shaw JE, Karuranga S, Huang Y, da Rocha Fernandes JD, Ohlrogge AW et al. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. 2018;138:271–81. https://www.sciencedirect.com/science/article/pii/S0168822718302031
Mackin ST, Nelson SM, Kerssens JJ, Wood R, Wild S, Colhoun HM et al. Diabetes and pregnancy: national trends over a 15 year period. 2018;61:1081–8. https://doi.org/10.1007/s00125-017-4529-3
Dabelea D, Hanson RL, Bennett PH, Roumain J, Knowler WC, Pettitt DJ. Increasing prevalence of type II diabetes in American Indian children. Germany. 1998;41:904–10.
Organization WH. No title.
Fadl HE, Simmons D. Trends in diabetes in pregnancy in Sweden 1998–2012. 2016;4:e000221. http://drc.bmj.com/content/4/1/e000221.abstract
Canada PHA. of. Congenital Anomalies in Canada [Internet]. 2023 [cited 2023 Sep 9]. https://health-infobase.canada.ca/congenital-anomalies/Index
Committee DCCPGE, Feig DS, Berger H, Donovan L, Godbout A, Kader T et al. Diabetes and Pregnancy. Canada; 2018;S255–82.
Bowker SL, Savu A, Lam NK, Johnson JA, Kaul P. Validation of administrative data case definitions for gestational diabetes mellitus. England: Diabetes UK; 2017;34:51–5.
Jonathan ACS, Ian RW, John BC, Spratt M, Royston P, Michael GK et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. 2009;338:b2393. http://www.bmj.com/content/338/bmj.b2393.abstract
Berger H, Gagnon R, Sermer M. Guideline 393-diabetes in pregnancy. Elsevier. 2019;41:1814–25. e1.
Discharge. Abstract Database metadata (DAD) | CIHI [Internet]. [cited 2023 Feb 21]. https://www.cihi.ca/en/discharge-abstract-database-metadata-dad
Liu S, Joseph KS, Liston RM, Bartholomew S, Walker M, León JA, et al. Incidence, risk factors, and associated complications of eclampsia. LWW. 2011;118:987–94.
Acknowledgements
We would like to thank Dr. Kelsey Vercammen for providing helpful comments on the manuscript.
Funding
None.
Open Access funding provided by Health Canada.
Author information
Authors and Affiliations
Contributions
CN and AM conceived the study and CN carried out the study. CN and SD developed statistical methods and CN performed all statistical analysis. CN drafted and revised the manuscript on the basis of comments from other authors. CN, SD, AM, PM, ED, WE, MVDH, HS, JR contributed to the interpretation of the data, critically reviewed all drafts of the manuscript and approved the final version submitted for publication.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The CIHI data analyzed in this study were collected by the Canadian Institute for Health Information (CIHI) under the authority of jurisdictional privacy or health information legislation and provided to the Public Health Agency of Canada under the Agency’s national health surveillance mandate. Data disclosed to third parties for research, like in this study, is in the form of de-identified record-level data. Data users are required to enter into a non-disclosure/confidentiality agreement with CIHI. CIHI provides PHAC access to de-identified versions of some of their data holdings, including DAD, through a data-sharing agreement signed by both parties in 2017. This agreement furthermore provides guidance on the scope and restrictions associated with PHAC’s secure use of CIHI data. Additionally, as per Article 2.2 of the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans, this research is exempt from IRB review as it relies on de-identified secondary data analysis which is available through a legislated or regulated mechanism and is legally protected by CIHI. All researchers with access to the data were employees of the Public Health Agency of Canada and had therefore obtained at a minimum Reliability Status as outlined in the Policy on Government Security.
Consent for publication
not applicable. Data are anonymized; therefore, consent was not needed for this study.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Nelson, C.R., Dzakpasu, S., Moore, A.M. et al. Diabetes mellitus in pregnancy across Canada. BMC Pregnancy Childbirth 24, 349 (2024). https://doi.org/10.1186/s12884-024-06534-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12884-024-06534-8